
Abstract

A 69-year-old female presented with a 2-month history of diarrhoea and abdominal pain. She had a medical history of well-controlled type 2 diabetes. All laboratory investigations performed during the initial evaluation were within normal limits, including haemoglobin, c-reactive protein and serum albumin. Stool routine and calprotectin levels were normal. Due to her age, she was scheduled for a screening colonoscopy for colorectal cancer. Bowel preparation was initiated with a split-dose regimen of polyethylene glycol.
The following day, after taking the second dose of the preparation solution, she developed severe abdominal pain and distension within an hour. On examination, she was tachycardic and appeared distressed due to the pain. Abdominal examination revealed gaseous distension with tenderness and guarding. Blood tests, including serum electrolytes, were normal. In view of her acute abdominal symptoms, an emergency computed tomography scan of the abdomen was performed to assess for bowel obstruction. The imaging revealed marked dilation of all colonic segments, from the cecum to the sigmoid colon, with a maximum diameter of 6.2 cm and no transition point (Figure 1(A)–(C)). These findings were consistent with colonic pseudo-obstruction.
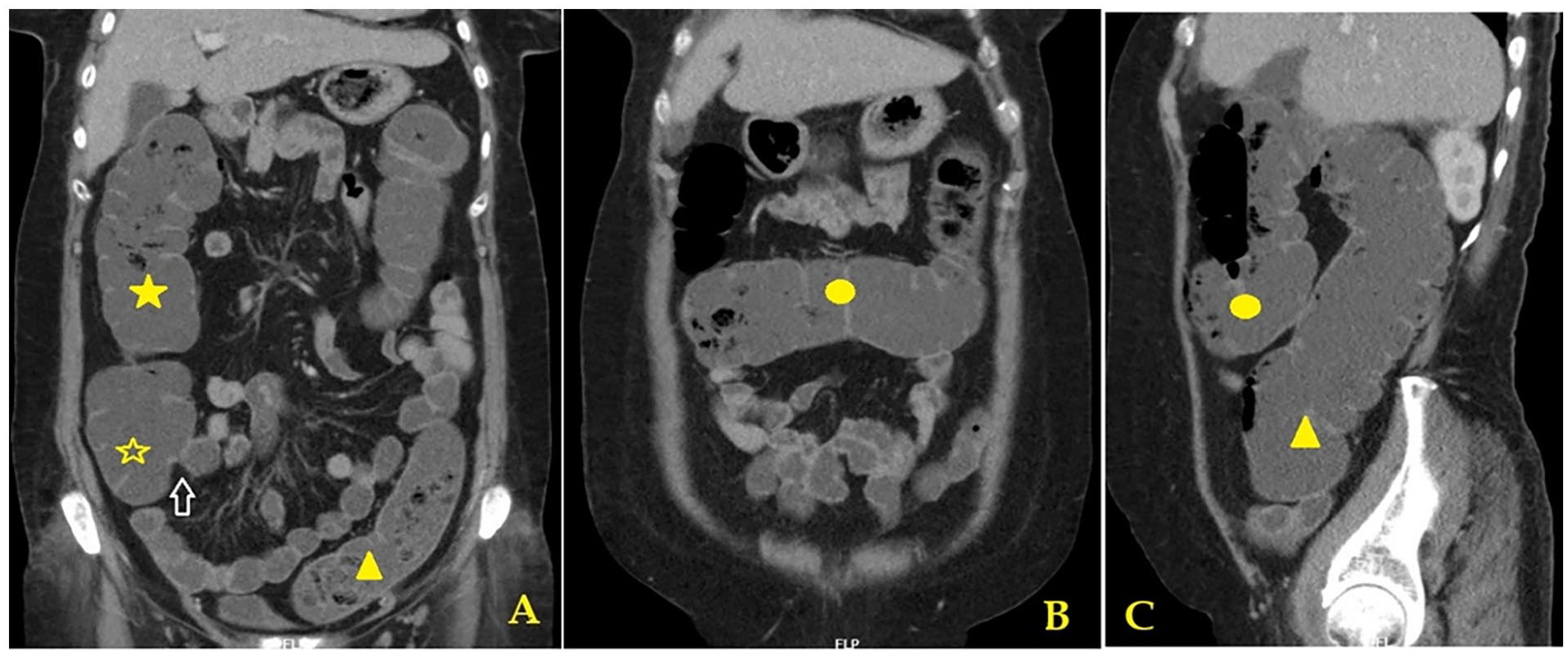
Contrast enhanced computed tomography abdomen depicting coronal view (A, B) and sagittal view (C) showing normal ileocaecal valve (white arrow) and marked dilatation of cecum (yellow hollow star), ascending colon (yellow solid star), transverse colon (yellow solid circle) and sigmoid colon (yellow triangle) without any transition point.
The patient was managed conservatively with bowel rest and intravenous fluids. She showed improvement within 12 h and was discharged the following day. One month later, her symptoms had marginally improved, and she was admitted again for bowel preparation and colonoscopy, which was performed without complications. Colonoscopy revealed a normal study. She was diagnosed as possible post-infectious irritable bowel syndrome and was treated with anti-spasmodics and a neuromodulator, and she remained symptom-free during a 7-month follow-up.
We present a rare case of acute colonic pseudo-obstruction (ACPO) that occurred during the bowel preparation phase of colonoscopy. Colonoscopy is considered the gold standard for evaluating and treating ileocolonic pathologies and is generally well tolerated with a low risk of complications. The complication rates range from 0.28% to 0.5%, with higher rates observed in procedures involving therapeutic interventions, such as polypectomy.1,2 Proper bowel cleansing is essential for an adequate colonoscopy. The most common adverse events during the bowel cleansing period are nausea, vomiting, dizziness or altered sensorium, typically resulting from electrolyte imbalances. Bowel obstruction has been reported in approximately 0.26% of colonoscopy procedures, with common causes including obstructive lesions such as malignancy or strictures. 3
ACPO is characterised by massive colonic dilation in the absence of mechanical obstruction. Several predisposing factors may contribute to its development, including prior abdominal surgery, trauma, neurological disorders, cardiorespiratory disorders, electrolyte imbalances, hypothyroidism, viral infections and certain medications. 4 A significant precipitating factor during the bowel cleansing phase of colonoscopy could be the water and electrolyte disturbances induced by the preparation solutions, such as sodium phosphate or polyethylene glycol. Known electrolyte imbalances associated with bowel preparation include hyponatraemia (3.3%), hyperphosphatemia (0.65%), hypocalcaemia (8.07%) and hypokalaemia (4.83%). 5
The most serious complications of ACPO include ischaemia and perforation, particularly, in cases with caecal diameters >10–12 cm or when the condition persists for more than 6 days. In patients with uncomplicated ACPO (i.e., no ischaemia, peritonitis, caecal diameter >12 cm or significant abdominal pain), conservative management remains the first-line treatment, with success rates ranging from 77% to 96%. 4
This case highlights a rare and potentially life-threatening complication that can occur during the bowel cleansing phase of colonoscopy. It is, to our knowledge, the first such case reported in the literature. Clinicians and healthcare providers involved in patient education about bowel cleansing and colonoscopy should be aware of this rare complication. Early detection and prompt intervention are critical to prevent serious outcomes associated with ACPO.
Footnotes
Acknowledgements
None.
Author contributions
RSNR had written the draft and obtained images. BM and SS revised the draft. All the authors approved the final manuscript.
Consent for publication
Obtained from the patient.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.