
Abstract
Modern technology has provided the author with access to a previously unobtainable publication, John Moore’s 1784 work, ‘A Method of Preventing or diminishing Pain in Several Operations of Surgery’. Not only did this allow direct consideration of his technique of nerve compression (which has been described briefly by many others since), but also showed that Moore had very advanced humane views on the need to try and produce pain relief for surgery. It also became possible to obtain far more information on the author, notably that although he worked in London he was born and educated in Glasgow, and did his initial medical training in Edinburgh. He thus is one of a group, all of whom were Scots, who did preliminary work on local anaesthesia before the recognition of the local action of cocaine. His technique was tried, apparently successfully, for a below-knee amputation by John Hunter, and while both the technique and his humane approach were noted by others, the method does not seem to have found wider favour. He continued working as a surgeon in London until he inherited an estate in south-west Scotland, this allowing him to give up clinical practice and focus on writing and campaigning. He wrote the definitive biography of his brother (Sir John Moore of Corunna fame) and was a leading advocate of vaccination, leading the organisation after Jenner’s death. These activities meant that he was well known in his lifetime, but he deserves to be better known today as being the first person to promote the need for pain relief during surgery.
Keywords
Introduction
A previous publication, 1 noted that several Scots (James ‘Young’ Simpson, James Arnott, Alexander Wood, Alexander Hughes Bennett and Benjamin Ward Richardson) made contributions to the development of local anaesthesia before Carl Koller’s definitive recognition of the local action of cocaine in 1884. 2 It is arguable that a century earlier one James Moore was the first to look (using nerve compression) for a form of local anaesthesia, but he and his work are little known. Simpson, the first to use the term ‘local anaesthesia’, 3 describes Moore’s work, but when the author first tried (in the early 1980s) to obtain a copy of his book 4 not one of Edinburgh’s libraries was able to help. To avoid perpetuating errors through being unable to check the original reference the author sought advice on dealing with the problem. The solution proposed, 5 and followed, 6 was to mention Moore’s work without providing a reference, and this policy was followed for subsequent use until 2023 when it was found that modern technology has made available many ancient volumes of interest. A simple ‘Google’ search produced access to an on-line digital copy of the original, 7 and the purchase of a facsimile copy, 8 thus providing access to both Moore’s account of nerve compression and, almost as easily, information on the man himself (Figure 1).
James Carrick Moore (1762–1834). Surgeon and associate of Edward Jenner.
Moore’s early life
Moore was found to be yet another Scot involved in early work leading to the development of local anaesthesia, having been born and educated in Glasgow. His father, John, was a physician and writer, and his mother, Jean, a daughter of John Simpson, Professor of Divinity in Glasgow. He trained in Edinburgh and at St George’s Hospital, London (where he was House Surgeon to John Hunter), and served (1781) as an Army Medical Officer during the American War of Independence. After that he returned to London, became a Member of the Company of Surgeons (predecessor organisation to the Royal College of Surgeons of England) in 1783, went into practice as a surgeon in London, and published his book on nerve compression the following year. 9
Nerve compression
The book (A Method of Preventing or Diminishing Pain in Several Operations of Surgery, 1784) is a slender volume of 50 A5 pages with one illustration (Figure 2). The title and dedication pages (Figure 3) are followed by continuous text, but its sequence is remarkably like the ‘IMRAD’ (Introduction, Methods, Results and Discussion) model for modern scientific papers.
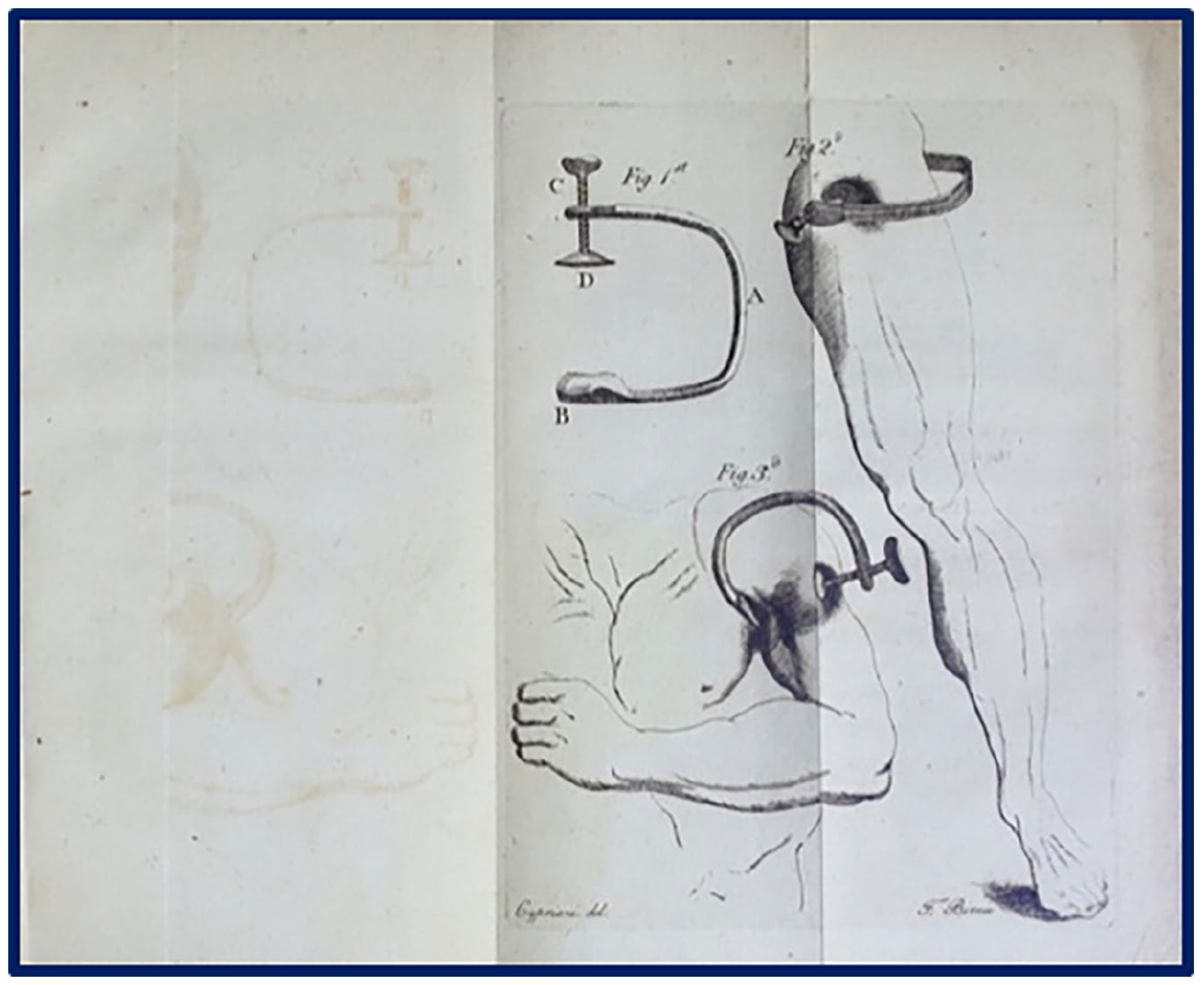
The drawings of Moore’s device in his book.
Title and dedication pages of Moore’s book.
Introduction: To start with he:
Defines the problem – the pain of surgery; Identifies a solution – recognise the pain and treat it; and Proposes a hypothesis – use nerve compression to stop the pain.
This section of the book is the most impressive because his insights, at a time when both surgery and surgeons are looked upon as callous, are well in advance of his time, as a few examples show. He starts by trying to persuade surgeons that they were already practising pain relief:
. . .the earliest efforts in surgery [such as immobilising injuries] had no object beyond that of relieving pain; . . .less painful method of stopping bleeding [than the cautery is now used]; and The same desire of saving pain to their patients has induced modern surgeons to reject use of the scissors [in favour of the scalpel].
Further, he challenged as ‘outdated’ some then current notions:
. . .that a degree of cruelty is requisite to enable a man to perform surgical operations; . . .to prevent or diminish a few minutes of such pain is an object highly desirable; and Some people say, what signifies a few minutes pain:- but it is not those who think themselves under the immediate necessity of undergoing a surgical operation who are apt to hold such language.
Methods: Such reflections led him to seek a solution for the pain of surgery, starting with various ‘anodynes’. He considered morphine ‘highly expedient’ after surgery, but ‘with little or no effect’ during an operation, and thought of nerve section until he recognised that it would, in itself, be ‘painful and dangerous’. However, it was from this that his thoughts turned to nerve compression ‘as in sitting in a particular position – in that state the leg and foot are numbed’. He explored the possibility with self-experimentation, aided by his father, starting with a simple tourniquet, but it produced no numbness and was poorly tolerated. He tried to focus pressure on the sciatic nerve, and this had some effect after half an hour’s application, but (unsurprisingly) below the knee only, and he recognized that femoral nerve compression was needed as well. He also found that pressure on the femoral vessels should be avoided and, with that proviso, found that the combined approach produced a complete effect below the knee. His final device, according to Moore’s illustration (Figure 2), was like a modern ‘G’ clamp with two pads, one with a screw thread to increase the pressure, to be positioned over the femoral nerve, and the other to be placed posteriorly over the sciatic. Armed with his results and arguments he took them to John Hunter who offered Moore the opportunity to try his compressor in a patient about to undergo below-knee amputation at St George’s Hospital.
Results (of clinical trial): The day before the operation (the date is not specified) Moore went to the hospital and had a very successful trial, so
Next morning I began the compression at a quarter before 11 of clock and the numbness of the limbs followed at the usual time.
At a quarter before twelve I gave him one grain of opium, to diminish the smarting of the wound after the operation, when the compression should be taken off.
At the circular incision through the skin, the patient did not cry out, change a muscle of his face, or shew any symptom of pain.
. . .questioned after concerning the pain he had suffered he declared that he had felt hardly any
Discussion
The author believes that this is the first detailed description of an operation performed under any form of anaesthesia, no matter how primitive, with Moore commenting that ‘The trial had all the success I expected’, but indifference seems to sum up the responses he received. The pain relief was dismissed as the effect of the morphine, there was objection to the possibility of circulatory obstruction (in spite of Moore’s efforts to avoid it), and the technique was dismissed as being of use only for operations performed below the knee joint.
Subsequent reaction
There are three, relatively contemporary, references to Moore’s work:
A book review published the same year summarises its content, but makes little comment, ending by referring the reader to the original. 10
James Lucas (a Leeds surgeon) records, in a 1784 review of amputation, 11 that he had tried the method and found it inconsistent, but admitted that it might have been better if he had, like Moore, supplemented it with morphine (many modern practitioners consider that parallel use of ‘sedation’ with nerve block has benefits for more major surgery).
Benjamin Bell, included a section on pain relief in the final (1886) volume of his major work A System of Surgery, 12 described Moore’s technique and commended him for his humane attitude to pain relief. However, he also commented as follows:
It has long been known, that the sensibility of any part may not only be lessened, but even suspended, by compressing the nerves which supply it. And accordingly, in amputating limbs, patients frequently desire the tourniquet to be firmly screwed, from finding that it tends to diminish the pain of the operation.
There are also earlier reports of more specific nerve compression to provide pain relief for surgery, the first known by Ambroise Pare in 1562, 13 but Moore makes no reference to such prior ‘knowledge’, whether through omission or ignorance it is impossible to tell.
Subsequent career
No evidence has yet been found that Moore continued to promote or pursue his ideas or method. Given his insights into the benefits of pain relief this leaves a puzzle behind, but he was a young man busy trying to make his way in the World, and the lack of positive response cannot have been encouraging. He continued in practice in London and seems to have been successful, becoming surgeon to the second Regiment of Life Guards. However, a major change in his life was triggered in 1821 when, Robert Carrick (a Glasgow Merchant Banker) died, and Moore became the owner of the Corsewall Estate in Dumfries and Galloway. Earlier sources(e.g. 9) say that Carrick was related to Moore’s wife, but the estate is still in the ownership of Carrick descendants today, and their website notes that he was Moore’s uncle. 14 Whichever is the case, he added Carrick’s surname to his own, became ‘James Carrick Moore’, gave up surgical practice and (supported by the estate’s income) focussed on being a campaigner and author on matters both medical and military. He was a major supporter of both Edward Jenner and vaccination, leading the campaign after Jenner’s death, and writing, among other volumes, the definitive biography of his brother, Sir John Moore of Corunna fame, work which led to him becoming well known at the time. 9
Legacy
Nerve compression ‘anaesthesia’ is nothing but an interesting footnote in the history of pain relief, but Moore certainly deserves to be better known now, especially in the land of his birth and in the company of the author’s other local anaesthetic ‘heroes’. One of the latter, James Simpson, is well known for his promotion of the use of anaesthesia against objections raised after its introduction in the 1840s, and it might be that his familiarity with Moore’s book,
3
and the humane statements within, informed that activity. Moore, of course, lived in a time towards the end of what is known as ‘The Enlightenment’, and he will have been influenced by many others promoting more humane approaches. However, the book can be said to mark a ‘watershed moment’ when callous attitudes in surgery were first called into question, and humane ones were promoted. To finish, a quote with which there can be no disagreement:
But when people consider the degree of pain given by surgical operations they must agree that to diminish or prevent a few minutes of such pain is an object highly desirable both to the patient and surgeon.
Footnotes
Acknowledgements
The painting of Moore (accession number PG 2731, artist unknown) is used with the permission of the National Galleries of Scotland. I thank Dr Jun Parker for his help in identifying the three contemporary references to Moore’s work.
Article note
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.