
Abstract
Background:
The presence of sleep-disordered breathing (SDB) in congestive heart failure (CHF) is associated with poor prognosis and is underdiagnosed despite advances in CHF management. The prevalence of SDB in CHF remains understudied in South East Asia.
Methods:
A prospective, observational single-centre study was conducted where 116 consecutive patients in a specialised heart failure clinic underwent level 1, attended polysomnography (PSG).
Results:
The prevalence of SDB was 78% using the apnoea-hypopnea index (AHI), AHI ⩾ 5/h threshold, and 59% with the AHI ⩾ 15/h threshold. Obstructive sleep apnoea (OSA) was the predominant type of SDB and was associated with increased body mass index and neck circumference. STOP-BANG was predictive of SDB, especially in men. Central sleep apnoea (CSA) patients had worse sleep indexes and lower awake arterial carbon dioxide. SDB was also homogenously present in preserved ejection fraction (EF) CHF.
Conclusion:
Most of the CHF patients were found to have SDB with the utility of PSG. Local CHF guidelines should include sleep testing for all patients with CHF.
The study is registered on ClinicalTrials.gov (NCT05332223) as ‘The Epidemiological Characteristics of SDB in Patients with Reduced or Preserved EF CHF’.
Keywords
Introduction
Congestive heart failure (CHF) is a common condition affecting 1–2% of the adult population. 1 It remains a leading cause of hospitalisation and mortality worldwide. Despite advances in treatment modalities, the associated 5-year mortality rate approaches 50% and has remained static for decades. 2 Complementary strategies need to be developed to target and address factors that are associated with disease progression and prognostic impairment.
Sleep-disordered breathing (SDB) is increasingly recognised as a common comorbidity of CHF due to improvement in access to sleep diagnostic studies.3,4 Nevertheless, it is a potential contributor to the morbidity of CHF as it remains underdiagnosed and undertreated. 5 SDBs may manifest as obstructive sleep apnoea (OSA) or central sleep apnoea (CSA), and the proportion of these two entities in CHF patients are highly variable in various study populations.6,7 The utility of screening questionnaires such as the Epworth Sleepiness Scale (ESS) to detect SDB in CHF patients is not reliable as these patients lack the hallmark features of SDB. 8
We sought to examine the epidemiological characteristics and the frequency as well as the types of SDB in CHF outpatients from a specialised heart failure clinic in a community hospital setting in Malaysia. We also evaluated the epidemiology of SDB in preserved ejection fraction (EF) CHF patients.
Methods
Patients
In this prospective, observational, single-centre study,116 consecutive patients aged 18 years and older under follow-up in Heart Failure Clinic, Hospital Taiping, Malaysia were enrolled from 1 April 2022 until 31 December 2023. All participants who were able to understand study information and give informed consent regardless of EF, and the presence or absence of symptoms of SDB were included. Only patients who had been diagnosed with SDB or treated with any form of positive airway pressure therapy prior to this were excluded. During recruitment, a total of 118 patients with CHF were screened. Two patients had a sleep study performed before and were already diagnosed with SDB. These patients were not included in this study. We believe the study cohort is representative of the centre’s CHF burden as none of the patients declined consent.
The study’s protocol was approved by the Medical Research and Ethics Committee of the Ministry of Health Malaysia (MOH Malaysia), and it was conducted under The Declaration of Helsinki and current national guidelines for clinical trials. Written informed consent was obtained from all individuals.
Demographic information was documented. Clinical characteristics such as aetiology of CHF and medications used to treat CHF were captured. Anthropometric measurements such as weight and height to derive body mass index (BMI) as well as neck circumference measurements were obtained. The ESS to estimate subjective daytime sleepiness and the STOP-BANG assessment (Toronto Western Hospital, University Health Network University of Toronto) were performed at baseline. Six-minute walking test was performed to assess functional capacity. Information on heart failure severity, such as New York Heart Association (NYHA) functional class and echocardiographic variables, were recorded.
Sample size calculation
The sample size calculation is done using the single proportion formula. The prevalence of OSA in patients with CHF among Asian Indians was 50.6% as reported by a study done by Bhalla et al. 9 With estimated 10% precision, we required at least 97 cases to be included in this study. After considering 20% dropout rate, we decided to include 116 cases.
Polysomnography (PSG)
An attended overnight in-laboratory PSG using Alice version 6 system (Respironics, Pittsburgh, PA, USA) for at least 6 h was scheduled. The following variables were monitored and captured. Sleep staging using electroencephalogram, electrooculogram, and electromyogram. Respiratory effort using inductive plethysmograph sensors to detect thoracoabdominal movements. Oro-nasal airflow using pressure flow transducer and thermistor. Oxygen saturation using pulse oximetry and cardiac rhythm using electrocardiography. Other parameters that were monitored included body position, presence of snoring and end-tidal CO2 (EtCO2) measurement to detect hypercapnia. An awake arterial blood gas (ABG) sampling was done within 30 min to 1 h of termination of PSG and awakening.
Apnoea is defined as a cessation of inspiratory airflow for 10 s, and hypopnea is defined as a reduction of airflow (>50%) or thoracoabdominal effort lasting 10 s resulting in a 4% drop in oxygen saturation. Obstructive apnoea is diagnosed if respiratory effort is present and central apnoea when no respiratory effort is detected. Hypopneas is categorised as obstructive when snoring, flattening of the nasal pressure inspiratory signal, or paradoxical thoracic and abdominal movement signals occur during the event. Central hypopnea is scored when all of these features are absent.
The apnoea-hypopnea index (AHI) is defined as the number of apnoea or hypopnea episodes per hour of sleep. The oxygen desaturation index (ODI) is defined as the number of oxygen desaturations of 4% or more per hour of sleep. The number of arousals per hour of sleep is calculated as the arousal index (AI).
AHI, ODI and AI were accurately determined. OSA was diagnosed when obstructive AHI is more than 5/h and more than 50% of events are obstructive apnoeas. Likewise, CSA is diagnosed when central AHI is more than 5/h and more than 50% of events are central apnoeas. All PSGs were performed and scored based on international guidelines for sleep studies.10,11 Patients were stratified into three groups based on sleep variables: (1) No SDB (AHI <5 h), (2) SDB (AHI ⩾ 5/h), and (3) Moderate to Severe SDB (AHI ⩾ 15/h), respectively.
Data analysis
The statistical analysis was performed using IBM Statistical Package for the Social Sciences for Windows, version 21.0. Armonk, NY, USA. Descriptive statistics, including patient demographics and clinical and physiological variables, were presented using mean (standard deviation) for normally distributed variables and frequency (percentage) for categorical variables. Frequency comparisons were conducted via Pearson’s Chi-square test or Fisher’s exact test for categorical variables and an independent t-test for continuous variables. Correlation analysis was performed using Pearson correlation method. The results were considered significant if the p-value was less than 0.05.
Results
Patient characteristics
A total of 116 patients were enrolled and underwent nocturnal PSG in the present study.
Majority of patients had coronary artery disease, 65%, and were on β-blockers, 90%. (Table 1). The overall prevalence of SDB was 78% using the AHI ⩾ 5/h threshold and 59% using the AHI ⩾ 15/h threshold. Patients with SDB regardless of the AHI thresholds were predominantly men and had significantly higher body weight, BMI, neck circumference and STOP-BANG score. PSG showed that patients with SDB had significantly higher ODI, lower lowest oxygen saturation and poorer sleep quality, as reflected by the significantly higher AI. Patients with SDB also had significantly lower awake arterial oxygen (PO2). We also discovered that there is strong positive correlation between AHI and ODI in CHF patients (R2 = 0.932, p < 0.001) in this present study (Figure 1).
Baseline characteristics of heart failure patients classified according to the different thresholds of apnoea-hypopnea Index.
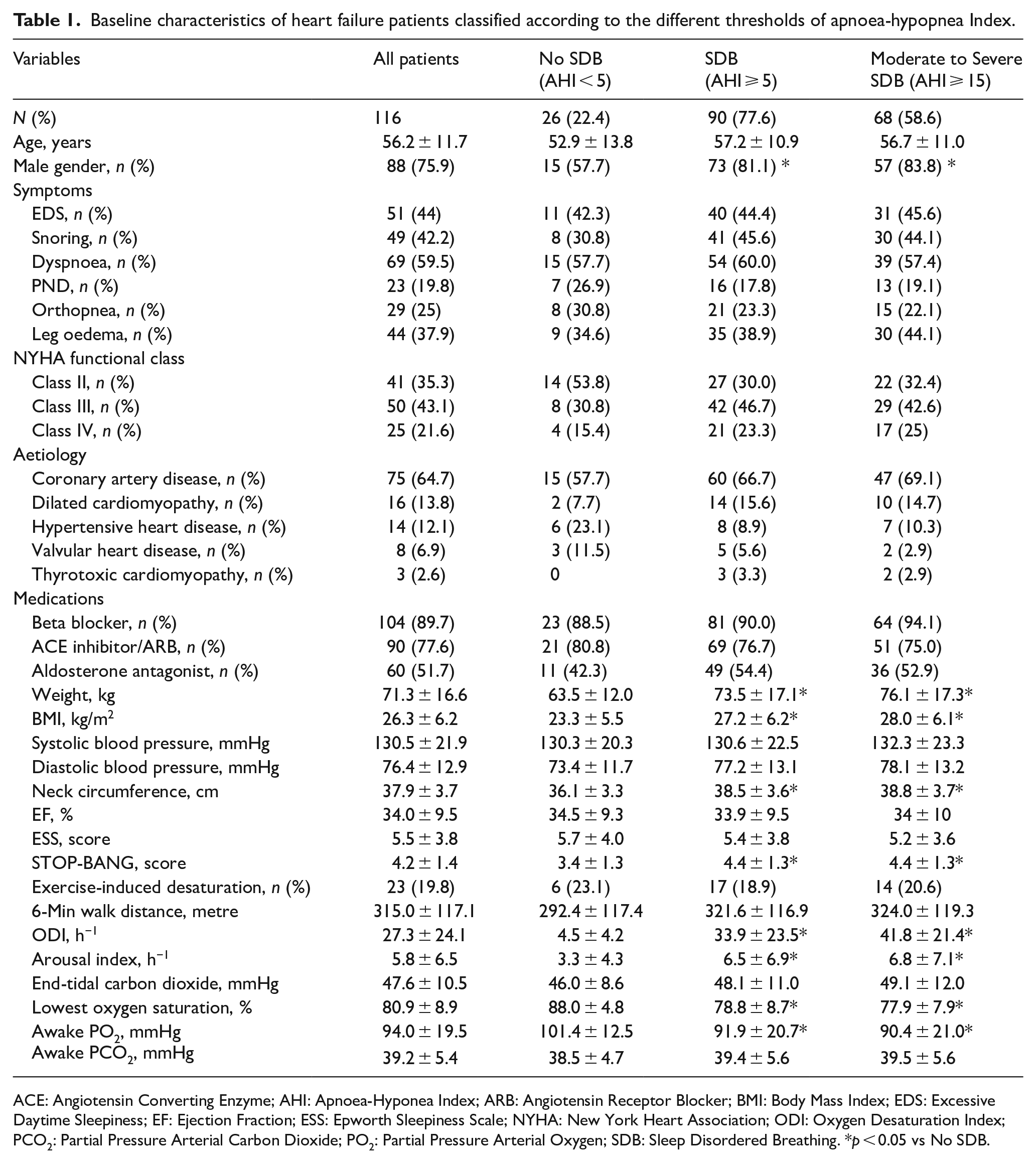
ACE: Angiotensin Converting Enzyme; AHI: Apnoea-Hyponea Index; ARB: Angiotensin Receptor Blocker; BMI: Body Mass Index; EDS: Excessive Daytime Sleepiness; EF: Ejection Fraction; ESS: Epworth Sleepiness Scale; NYHA: New York Heart Association; ODI: Oxygen Desaturation Index; PCO2: Partial Pressure Arterial Carbon Dioxide; PO2: Partial Pressure Arterial Oxygen; SDB: Sleep Disordered Breathing. *p < 0.05 vs No SDB.
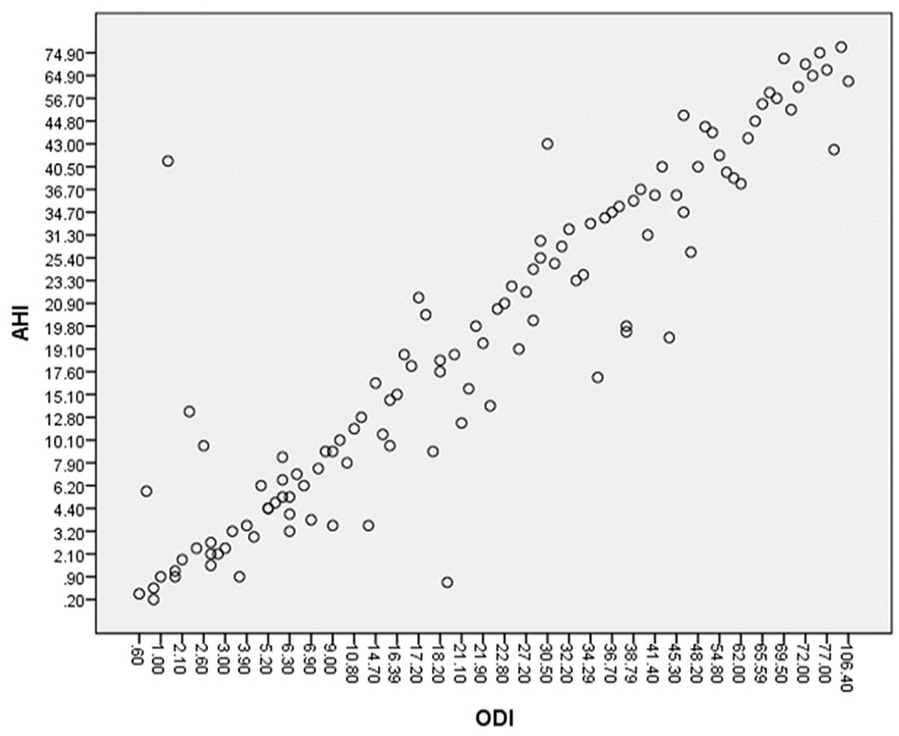
Correlation analysis between AHI and ODI in 116 patients with Heart Failure. (R2 = 0.932, p < 0.001). AHI: Apnoea–Hypopnea Index; ODI: Oxygen Desaturation Index.
Influence of gender
Majority of our SDB patients were male, 81%. (Table 2). Male patients with SDB had significantly higher rates of coronary artery disease as the aetiology of CHF, higher neck circumference and STOP-BANG score as well as sleep fragmentation.
Demographic, clinical and polysomnographic characteristics of patients with SDB and heart failure according to gender.
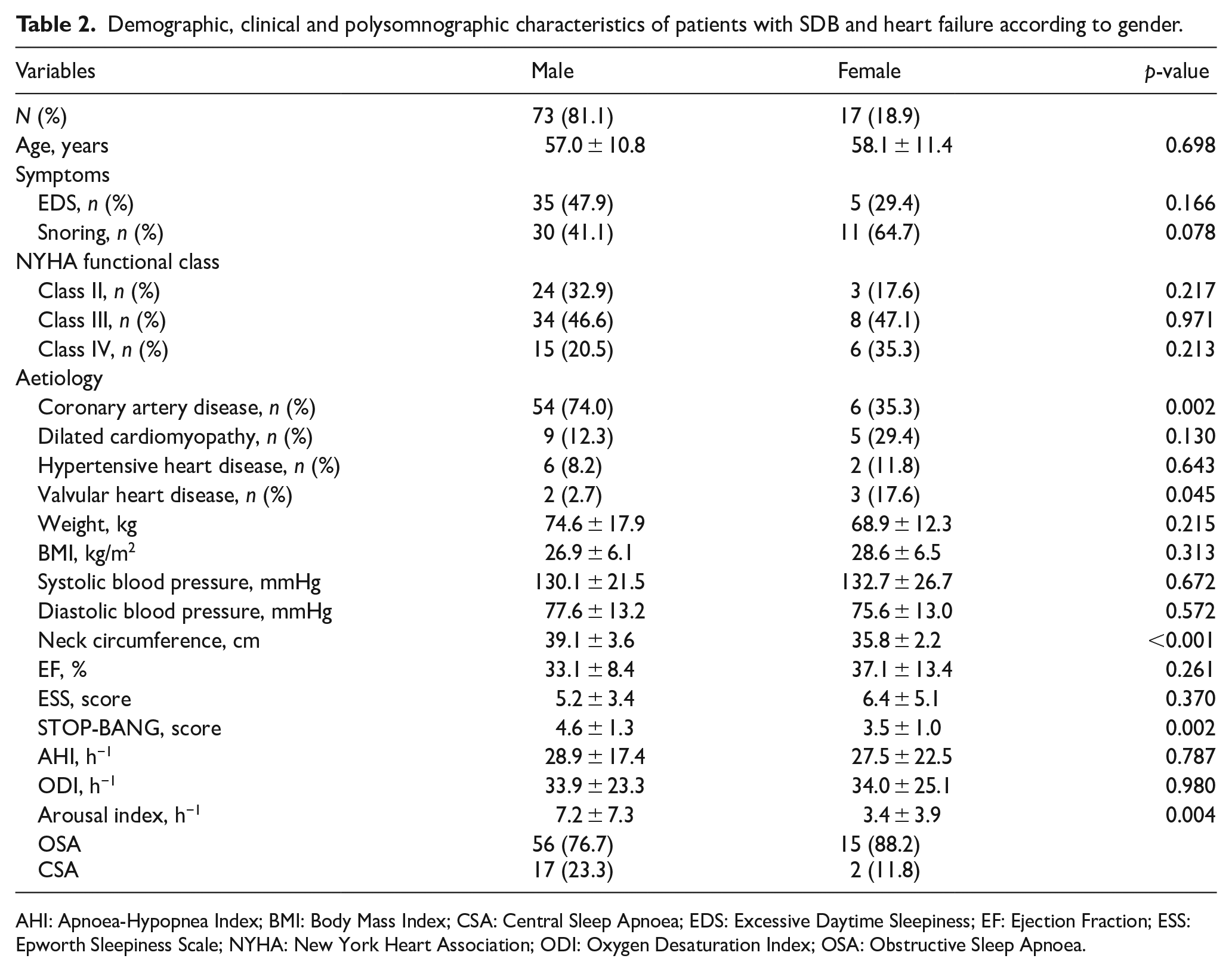
AHI: Apnoea-Hypopnea Index; BMI: Body Mass Index; CSA: Central Sleep Apnoea; EDS: Excessive Daytime Sleepiness; EF: Ejection Fraction; ESS: Epworth Sleepiness Scale; NYHA: New York Heart Association; ODI: Oxygen Desaturation Index; OSA: Obstructive Sleep Apnoea.
Prevalence of types of SDB
PSG revealed OSA in 61% of patients (Table 3). OSA patients were significantly older compared to patients with CSA. CSA patients were more symptomatic and had poorer NYHA functional class as well as EF, but the differences did not achieve statistical significance. AHI and ODI were significantly higher for CSA patients who also had significantly lower awake arterial carbon dioxide (PCO2).
Comparison of demographic, clinical and polysomnographic characteristics between OSA and CSA.
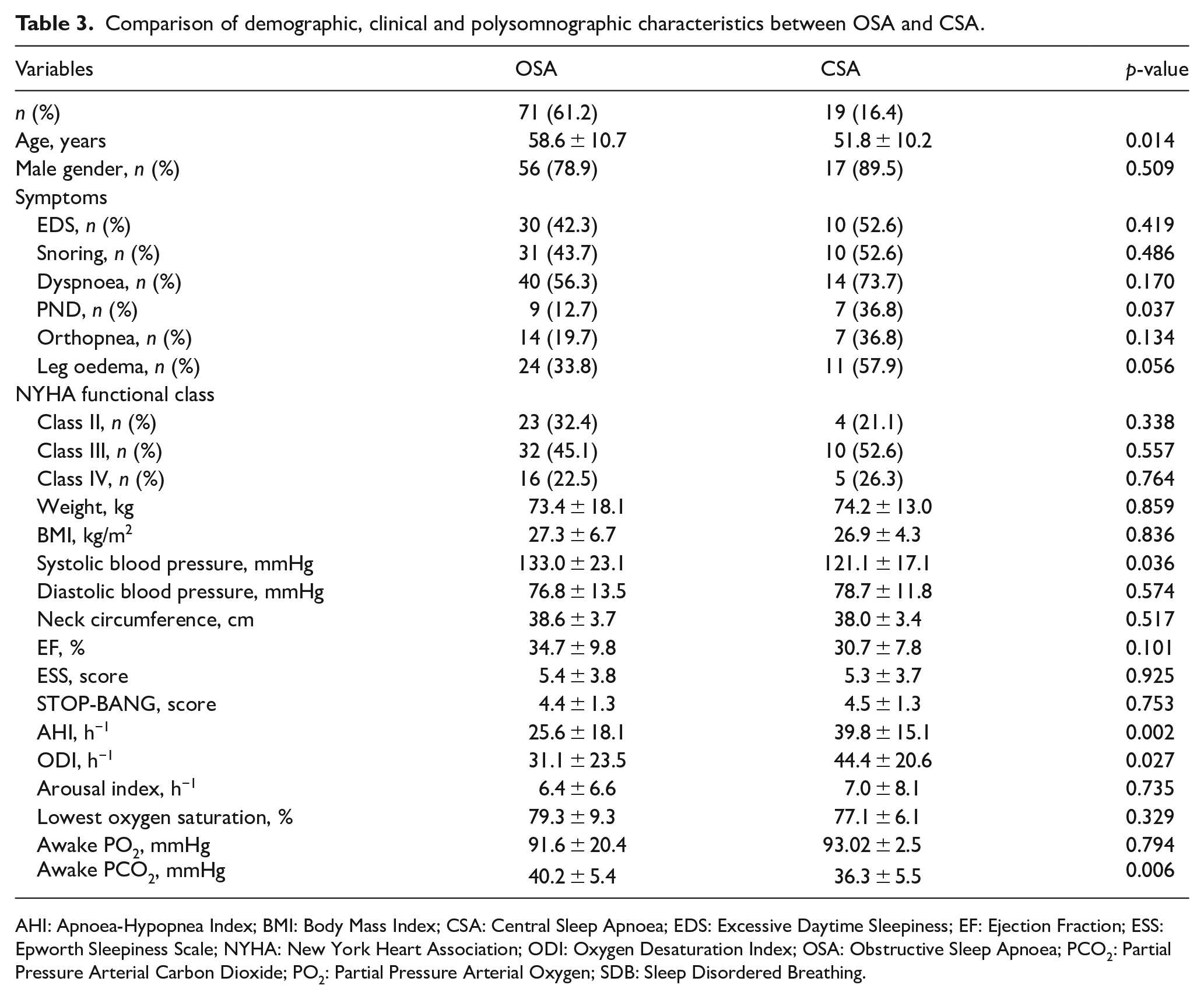
AHI: Apnoea-Hypopnea Index; BMI: Body Mass Index; CSA: Central Sleep Apnoea; EDS: Excessive Daytime Sleepiness; EF: Ejection Fraction; ESS: Epworth Sleepiness Scale; NYHA: New York Heart Association; ODI: Oxygen Desaturation Index; OSA: Obstructive Sleep Apnoea; PCO2: Partial Pressure Arterial Carbon Dioxide; PO2: Partial Pressure Arterial Oxygen; SDB: Sleep Disordered Breathing.
SDB in preserved EF CHF
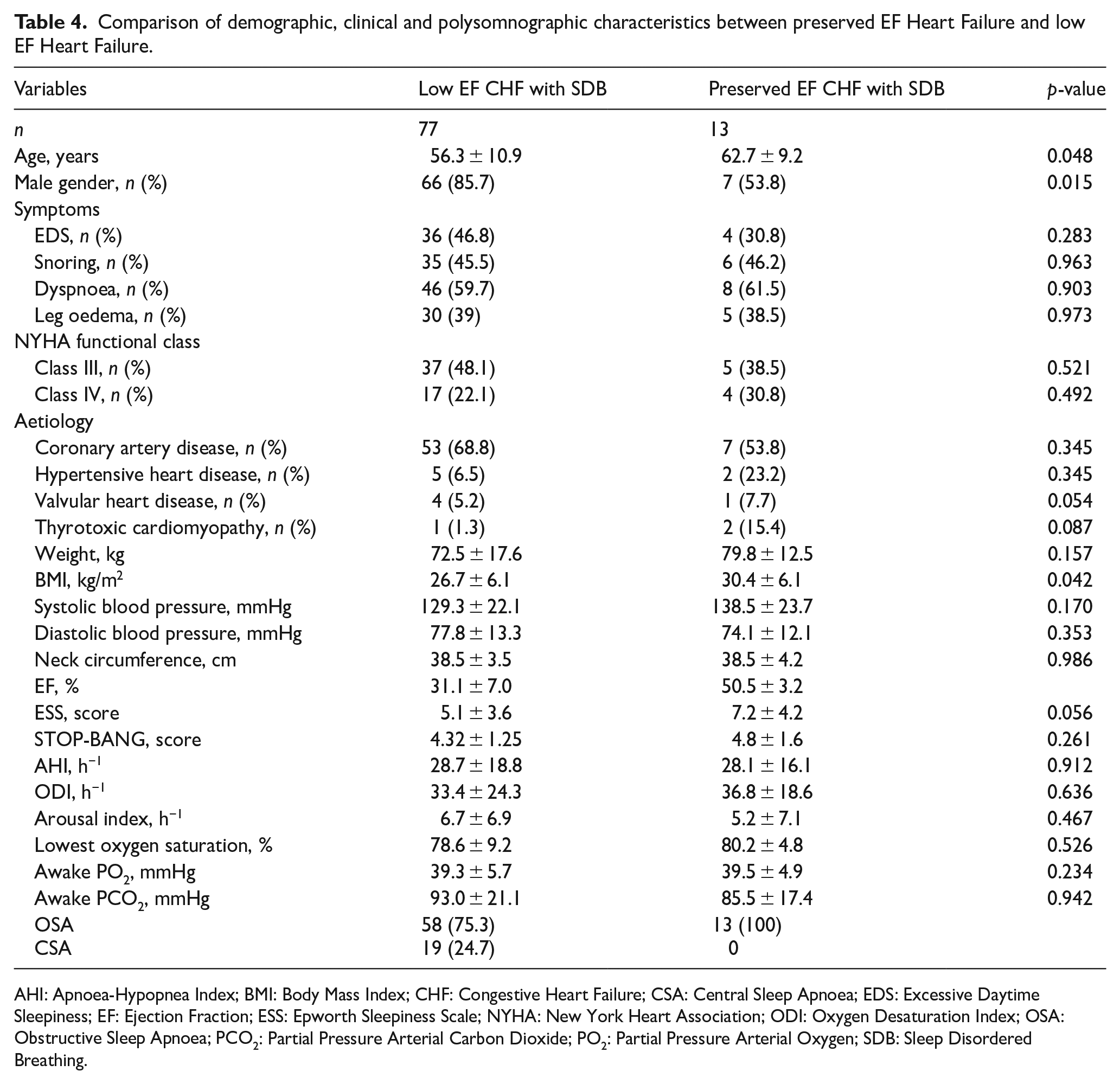
Only 16 patients with preserved EF CHF were included in this present study. Thirteen patients (81%) were found to have SDB, and all of them had OSA (Table 4). These patients were predominantly women, significantly older and had a higher BMI compared to patients with low EF CHF. There were no differences identified in terms of symptoms, aetiology of CHF, NYHA functional class, STOP-BANG score, PSG indexes and awake ABG measurements between the groups.
Comparison of demographic, clinical and polysomnographic characteristics between preserved EF Heart Failure and low EF Heart Failure.
AHI: Apnoea-Hypopnea Index; BMI: Body Mass Index; CHF: Congestive Heart Failure; CSA: Central Sleep Apnoea; EDS: Excessive Daytime Sleepiness; EF: Ejection Fraction; ESS: Epworth Sleepiness Scale; NYHA: New York Heart Association; ODI: Oxygen Desaturation Index; OSA: Obstructive Sleep Apnoea; PCO2: Partial Pressure Arterial Carbon Dioxide; PO2: Partial Pressure Arterial Oxygen; SDB: Sleep Disordered Breathing.
Discussion
To the best of our knowledge, the epidemiology of SDB in CHF has not been studied in the South East Asian population. This study is one the first studies to comprehensively evaluate the epidemiological characteristics of SDB in patients with CHF in a centre in Malaysia, satisfying all of the following: (i) a prospective design; (ii) data involving more than 100 consecutive patients; and (iii) a comprehensive evaluation using level 1, attended PSG. Consistent with previous studies, we report a high prevalence of SDB in 78% of patients using an AHI threshold of more than 5/h and 59% of patients using an AHI threshold of more than 15/h. This prevalence is marginally higher than what was reported in previous studies where SDB was present in 47% to 76% of cases.4,6,7,12,13 This wide variation of prevalence can be attributed to the different thresholds of AHI used to define SDB in various trials. However, we believe this is not the sole reason that explains the difference between the prevalence observed in our study compared to previous observations.
The results from studies conducted in USA and Europe on the prevalence of SDB in CHF may not be applicable to our patients for various reasons. Firstly, a diverse and multi-ethnic population in Southeast Asia may have an impact on the occurrence of SDB due to varying craniofacial morphological appearances, differences in levels of obesity and respiratory chemosensitivity. Additionally, the disparity in health services and the socio-economic differences between developed countries in the West and a developing nation in Southeast Asia may have an impact on pharmacotherapy of CHF affecting the frequency and severity of SDB.
Furthermore, large population studies were retrospective and utilised unattended portable sleep testing (PST), as access to PSG is limited and costly.4,13 Unattended PST may underestimate AHI and underdiagnose SDB as the number of apnoeas and hypopneas are reported in relation to ‘total recording time’ with PST compared with ‘total sleep time’ with PSG. Several studies also reported an overall prevalence of SDB as it was not possible to distinguish between OSA and CSA.7,9,14 PST is not recommended by the American Academy of Sleep Medicine (AASM) for the diagnosis of CSA. 15 In the present study, we discovered strong correlation between AHI and ODI in patients with CHF. PST measures airflow, respiratory effort and oxygen saturation and hence ODI can be quantitatively deduced. PST can be used as a screening tool to detect SDB, but substantial false negative rates, when compared with PSG, certainly suggest more evidence is needed regarding its accuracy and reliability. 16
Similar to previous studies, women are also under-represented in this current study.4,6,7,12,13 Due to the recruitment of consecutive patients, we had no control over the gender of our participants. Despite similarities between age, BMI, EF and AHI between the two groups, women had a lower frequency of SDB and significantly better sleep quality. There were significant variations by gender with CSA found to be two times more likely to occur in men; meanwhile, OSA was more common in women. The reasons for these gender differences are poorly understood. Comparison with previous studies is less feasible as some of these studies only included male subjects.3,13 Little is also known about the risk factors for the development of SDB in women with CHF.
SDBs can present as OSA, CSA or as a combination of these two abnormal breathing patterns. However, all patients in the present study had either predominant OSA or CSA. The prevalence of OSA and CSA in CHF is higher than in the general population and ranges from 12% to 43% and 21% to 40%, respectively, according to varying studies.17,18 In contrast, we report a higher prevalence of OSA, 61% and significantly lower prevalence of CSA, 16% in our study population. The high prevalence of OSA is explained by the presence of traditional risk factors, which include increased neck circumference and BMI in our multi-ethnic study population. The lower prevalence of CSA is because almost 90% of our patients were treated with beta-blockers. The suppression of CSA by beta-blockers has also been documented in two preceding studies.19,20
As OSA was the predominant type of SDB in our patients, the presence of SDB was associated with increased BMI and neck circumference. The severity of SDB when assessed using AHI, ODI and lowest oxygen saturation was worse in CSA compared to OSA. This corresponds to the observation made by Solin et al. 21 We also discovered that awake arterial carbon dioxide was predictive of CSA. This is an expected finding as patients with CSA have hyperventilation during wakefulness and sleep due to unstable ventilation regulatory mechanisms. Only few studies reported independent predictors of SDB using multivariate analysis. They report only BMI was a predictor of OSA; meanwhile, male gender, advancing age, atrial fibrillation and low awake arterial carbon dioxide were independently associated with CSA.4,7,22
Another point to consider is that a significant number of CHF patients have reported daytime sleepiness regardless of the presence or the absence of SDB. The ESS score seen in this study was also not remarkably different between these two groups. Patients with CHF have daytime sleepiness due to nocturnal CHF symptoms. 23 Other studies reported patients with CHF have less subjective sleepiness presumably due to pre-existing sympathetic overactivity at baseline that may mask its detection.9,24 On the other hand, we found STOP-BANG to be predictive of SDB, especially in men. STOP-BANG has been shown to be predictive of SDB in the general population but inadequately assessed in CHF patients. 25 Hence, we agree that screening with ESS may not be reliable in predicting SDB in CHF, but our findings show that there is a role for STOP-BANG in selecting patients for PSG.
Many previous studies have shown a high prevalence of SDB in low EF CHF.3,4,26 Nevertheless, patients with preserved EF CHF may also suffer from SDB, but it remains understudied globally. Bitter et al. reported a prevalence of 48% for SDB in preserved EF CHF patients. As the study used PST for diagnosis, the AHI may have been underestimated because actual sleeping time may have been shorter than the recorded time. 27 Another study which used PSG reported a prevalence of 55% but had a small sample size. 28 The current study extends these findings by showing that SDB is homogenously prevalent in CHF patients regardless of EF. All of our preserved EF CHF patients with SDB had OSA and were predominantly women with significantly higher BMI. The sample size (n = 16) was small as this was a study of unselected stable CHF outpatients.
The present study has several major strengths. It is a pioneer prospective research on the epidemiology of SDB among CHF patients in a South East Asian population. We report a high prevalence of SDB in this cohort, and it is unlikely this prevalence is overestimated. This is because all patients were enrolled in a consecutive and unselected manner. They also had undergone Level 1 PSG, which is the gold standard for the diagnosis of SDB. Studies which sampled highly selected CHF patients may have overestimated the prevalence; meanwhile, the utility of PST for diagnostics may have underestimated the prevalence of SDB. Furthermore, almost 90% of patients were treated with beta-blockers, which shows that our CHF patients were treated according to international guidelines. 29 The results of this study are applicable to CHF patients regardless of EF, as data from preserved EF CHF patients were also included in the analysis. Finally, the sleep studies were scored by a single scorer. This could have eliminated possible bias induced by potential interobserver variability between patients.
We acknowledge that the present study has some limitations. The present study was conducted in a single institution and the inclusion of diverse multi-ethnic patients may render the results not applicable to patients outside this region. As this was a systematic study of unselected stable CHF outpatients, the sample sizes of women, patients with CSA and preserved EF CHF were small and multivariate analysis could not be performed. This study was not intended to identify the independent predictors of SDB.
In conclusion, most of our CHF patients were found to have SDB. The presence of OSA or CSA has been associated with poor prognosis in CHF. SDB presents as a potential therapeutic target in CHF as nocturnal ventilation universally improves quality of life, left ventricular systolic function and physiological outcomes. Although survival benefits have been reported in OSA patients adherent to nocturnal continuous positive airway pressure (CPAP), this is only seen in a fraction of CSA patients who are termed as responders.30,31 Therefore, recognising CHF patients with SDB have important clinical implications. We suggest that revisions be made to local CHF guidelines to include sleep testing in the form of PSG in all patients with CHF. In limited resource settings, performing PST as a screening test in patients with high STOP-BANG scores is reasonable.
Footnotes
Acknowledgements
The authors would like to thank the Director General of Health Malaysia for permission to publish this paper. The authors also thank Muhammad Ridzuan Fadzil (Respiratory Unit, Hospital Taiping) for his contributions in performing and interpreting the sleep studies.
Data availability statement
Data are available on request from the authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.