
Abstract
We examine the ethical and legal challenges of continuing inpatient treatment for individuals with longstanding anorexia nervosa (AN), particularly where treatment effectiveness is uncertain. This legally and ethically contentious issue has been explored in a number of cases, which can be divided into two cohorts. We analysed the first cohort in 2017, identifying three key criticisms and offering corresponding recommendations. We assess a second, ongoing set of cases in light of those recommendations, while also considering new issues, including emergent treatment approaches and the debate surrounding the controversial ‘terminal eating disorder’ framework. Although judges in the Court of Protection do not adopt this framework, they do recognise that prolonged, compulsory life-sustaining treatment may – under certain circumstances – conflict with the patient's best interests. We argue that recent approaches to both mental capacity assessments and determination of best interests indicate a meaningful shift towards a more individualised and ethically responsive approach and suggest ways to augment this approach.
Introduction
The judicial approaches to severe and longstanding anorexia nervosa (AN) often navigate complex terrain where patient autonomy, clinical judgement, and the potential for recovery intersect. There is now a significant body of relevant case law which can be divided into two cohorts. We analysed an initial set of five cases 1 in 2017, 2 arguing for a more patient-centred approach and making three recommendations to help bring that about. A brief hiatus followed, where there were no reported cases, but from 2020, a second set of cases ensued. We list the cases involving the determination of capacity and best interests of adults with longstanding eating disorders in Table 1. The second cohort has received little academic attention notwithstanding that they raise and address novel and pressing issues. We seek to address that lacuna in this article. We use our earlier recommendations as a framework by which to analyse the developments and the clinical and judicial commitment to a patient-centred approach. Our analysis situates clinical and jurisprudential developments within broader clinical and ethical controversies – particularly debates around medical futility and the contentious characterisation of certain cases as involving ‘terminal’ anorexia nervosa. We find that there has been measurable progress in addressing each of our prior recommendations, and we suggest ways in which this patient-centred approach could be more fully realised.
Brief description of published cases post 2020 concerning the capacity and best interests of adults with longstanding eating disorders.
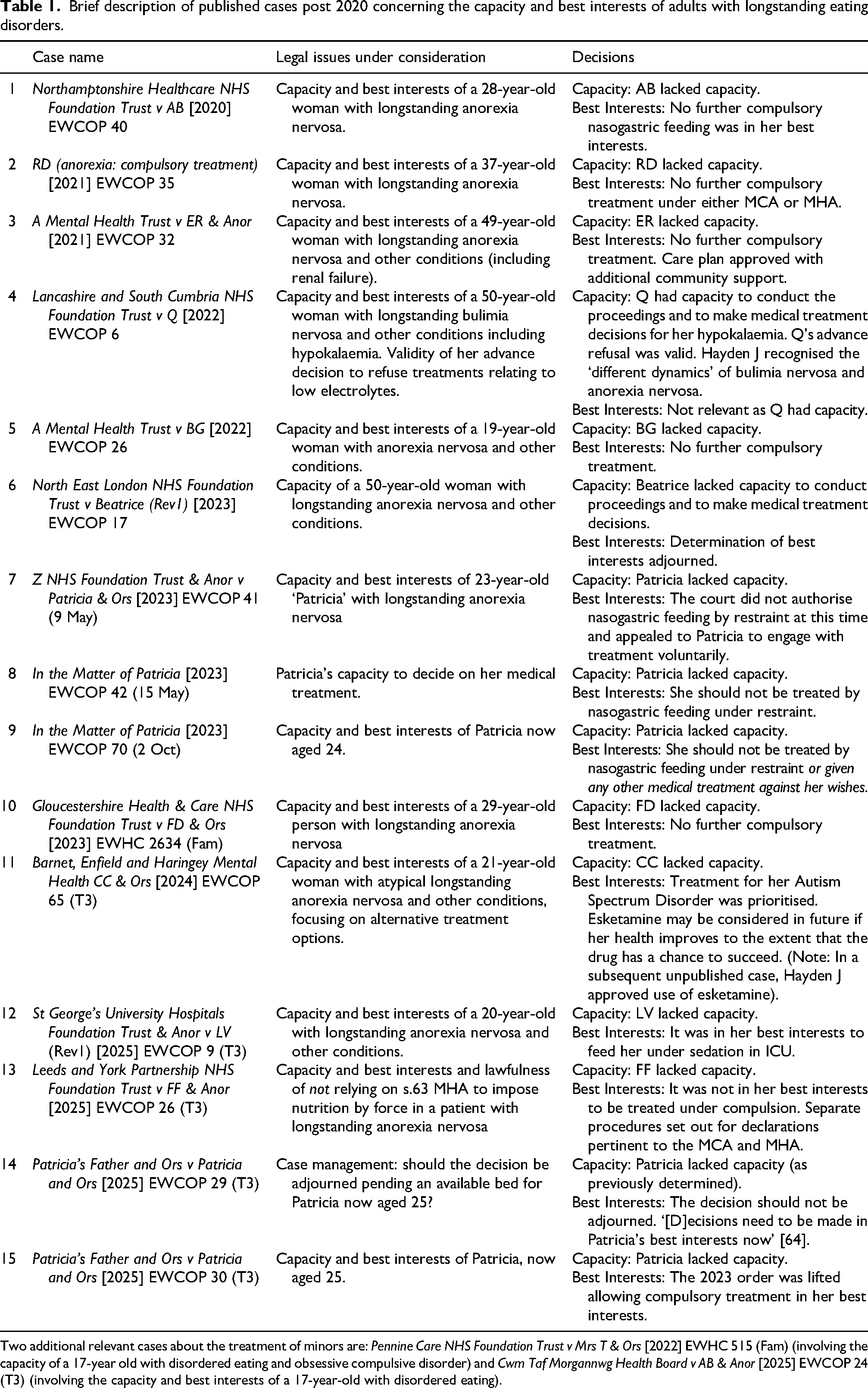
Two additional relevant cases about the treatment of minors are: Pennine Care NHS Foundation Trust v Mrs T & Ors [2022] EWHC 515 (Fam) (involving the capacity of a 17-year old with disordered eating and obsessive compulsive disorder) and Cwm Taf Morgannwg Health Board v AB & Anor [2025] EWCOP 24 (T3) (involving the capacity and best interests of a 17-year-old with disordered eating).
Context
Nutritional restoration of both micronutrients (vitamins and minerals) and macronutrients (to increase body weight and composition) is central to eating disorder treatment. Hospitalisation may be required when intake is inadequate, with nutrition provided through supplements or nasogastric feeding if needed. Where necessary, this can be administered without the patient's consent. 3 Compulsory feeding under restraint is a last resort, used only in medical emergencies when other interventions have failed. 4
Several interrelated factors influence clinical decision-making in this context. A lack of specialist beds often forces patients into general medical or psychiatric settings that may be ill-equipped to provide appropriate care. Co-morbid conditions such as depression, anxiety, autism spectrum disorder or trauma can complicate diagnosis and treatment planning, increasing the risk of harm or retraumatisation when compulsion is used. 5
Emerging treatments such as deep brain stimulation, ketamine, or psychedelic-assisted therapy offer potential new avenues but remain largely untested in this population, creating uncertainty in clinical pathways. 6 Added to this is diagnostic ambiguity: In 2017, we used the label ‘Severe and Enduring Anorexia Nervosa’ (SEAN) to identify cases that persist beyond standard treatment. However, SEAN is a category without clear or consistent criteria, complicating the identification of treatment-refractory cases. 7 Moreover, Lubieniecki et al.'s empirical research suggests the label can be restrictive, reductive and sometimes lead to limitations in care opportunities. 8 They prefer the term ‘longstanding’, which we adopt here.
Further controversy surrounds the concept of ‘terminal anorexia nervosa’. 9 Some clinicians and ethicists support palliative approaches when further active intervention appears futile. Others argue this point is difficult to identify and define, and that current evidence does not allow reliable prognostication at the individual level. They argue that adopting the label of ‘terminal anorexia nervosa’ too readily risks reinforcing the illness narrative and may lead to unjust or premature abandonment of patients and carers. 10
Clinicians initiating nasogastric feeding under restraint must comply with legislation. Two overlapping legislative schemes apply. If the person needs to be detained for treatment of an eating disorder then a treatment order under section 3 of the Mental Health Act 1983 (MHA) is lawful if, broadly, three conditions are satisfied: the patient has a mental disorder, there is a risk to the patient or others, and appropriate medical treatment is available. By virtue of section 63 a detained person may receive treatment for mental disorder without their consent.
Nasogastric feeding under restraint may achieve short-term weight stabilisation needed to maintain life, but it carries both medical and psychological risks and its impact on long-term recovery remains unclear. 11 The appropriateness of medical treatment might reasonably be questioned if it has been tried on a recurring basis and for a prolonged period and is not considered effective. The issue is not just that the legal authority to treat under section 3 is called into question, but that the compulsory treatment engages deeply contested ethical and human rights principles.
The Mental Capacity Act 2005 (MCA) provides a separate framework. According to section 1(2), individuals are presumed to have capacity to make specific decisions unless proven otherwise, in accordance with the two-stage test outlined in sections 2 and 3 of the Act. A person cannot be deemed to lack capacity simply because they make a decision that others view as unwise. 12 Unlike the framework under section 63 of the MHA, the MCA allows a person (P) with capacity to make legally binding decisions about their treatment, including the refusal of interventions such as nasogastric feeding – even where such a decision may lead to a shortened life.
According to section 3 of the MCA, if the person cannot decide because their functioning is impaired, and that impairment can be causally attributed to the individual's underlying anorexia nervosa, thereby meeting the diagnostic criterion in section 2 of the MCA, then P is considered to lack capacity in respect of that decision. Whilst patients with anorexia nervosa will often be able to understand and retain the information and communicate a decision, they are not always able to use or weigh the information under section 3(1)(c) of the functional part of the test. This difficulty may be subtle. It is not always possible for patients whose identity may be distorted by the overwhelming drives of their condition, or who are subject to the emotional dominance of the disorder, or the value placed of losing weight even unto death, to make capacitous decisions. It should be noted this incapacity may be limited to the issue of consent to treatment involving nutritional and weight restoration, which are counter to the drives of the eating disorder. 13 Where capacity is lacking, treatment may be provided based on what is deemed to be in their best interests. 14 Where there is uncertainty regarding capacity or the appropriateness of a treatment, the Court of Protection may issue a declaration as to whether P has capacity and whether a proposed intervention – or which in a range of possible interventions aligns with their best interests. Application to the Court of Protection is required if the decision relates to provision of life-sustaining treatment where the issue is finely balanced, there is a difference of medical opinion or a lack of agreement by those concerned with P's welfare. 15
We note at the outset four features of the relevant Court of Protection judgments: they are fact-specific which makes them highly individualised; they are first-instance decisions, so whilst they may clarify how the relevant legal principles apply in this context, they represent limited doctrinal development; and not all cases are published – there are other relevant cases which are not officially reported and may not be made public at all. 16 Additionally, judgments respond to proposals made – in these particular cases – by clinicians. As such, changes we identify below encompass both clinical decisions as to the framing of the declarations sought and legal decisions about the particular patient's capacity and best interests.
Our 2017 recommendations
Between 2012 and 2017 there were five cases, all of which involved patients who had had anorexia nervosa for more than 14 years. In each, the court found they lacked capacity. However, only in Re E was compulsory nasogastric feeding deemed in the patient's best interests, based on evidence suggesting a year of treatment could offer a 20–30% chance of full recovery.
17
In the other cases, judges reluctantly concluded that no realistic treatment options remained to prolong life.
18
In light of our analysis of these cases, which we do not repeat here in detail, we set out three criticisms and corresponding recommendations:
The courts should consider a patient-centred rather than clinician-centred approach to framing the decision that is subject to a capacity assessment. Because of clinical and ethical uncertainties regarding prognosis and appropriateness of treatment, it is problematic to rely on the same court-appointed independent expert in all cases, and the pool of experts should therefore be widened. Where a patient with longstanding AN lacks capacity, reliance on their stated views about the futility of treatment should be viewed with caution.
In this article, we structure our analysis of the recent case law around these 2017 recommendations, not to suggest these are the sole or definitive lens through which to view the issues, but rather as a useful framework for understanding how clinical and judicial reasoning has subsequently evolved. We take the first two together before turning to the third recommendation on best interests.
The capacity assessment
In 2012, Jackson J said in Re E: I acknowledge that a person with severe anorexia may be in a Catch 22 situation regarding capacity: namely, that by deciding not to eat, she proves that she lacks capacity to decide at all.
19
Pre-2017 cases raised questions about the framing of capacity assessments. If P's decision is framed as refusal of nutrition, the Catch 22 will likely apply. We argued that if, instead, the focus is on P's ability to assess previous and ongoing treatment as futile and harmful to them, then this would shift away from a near assumption of incapacity and adopt a more patient-centred position. This is not to say that the reframing would dramatically change the number of patients found to retain capacity. The impact of the eating disorder combined with the effects of malnutrition on cognition can render P unable to use or weigh the information. Rather it would make clearer the individualised and decision specific nature of the capacity assessment. Our contention was that, notwithstanding the framing of the declaration sought by hospital trusts or assessments of P's capacity by experts, the judge has scope to interrogate and, if necessary, reframe the decision around which capacity is assessed.
In the recent series of cases there has been no case of a patient with longstanding AN where the patient has been found to have capacity. Moreover, the judge will often accept that P lacks capacity if there is agreement between the parties to that effect. 22 As such, one might consider that there has been little change. Nevertheless, we would argue there are three ways in which recent cases move toward the patient-centred capacity assessment we called for in 2017.
Shifting the focus of the capacity assessment
The first progression came in a 2020 case when barristers in Northamptonshire Healthcare NHS Foundation Trust v AB advanced the argument we set out in 2017.
23
AB was 28 and had had anorexia nervosa since the age of 13. She had been treated as an in-patient 11 times. The NHS trust sought declarations that AB lacked capacity and that it was not in her best interests to receive further active treatment. Doctors considered that the only viable option was for AB to undergo feeding through a tube inserted into her stomach. The evidence suggested that AB would resist and be exposed to significant injury. Moreover, even if the treatment was a short-term success, it was considered unlikely that she would engage in the next stage needed to maintain weight. Katie Gollop KC, the respondent's leading counsel, argued that AB had capacity to make a decision about rejecting further feeding under restraint. Roberts J gave considerable attention to this argument saying: [Gollop KC] submits that the issue for the court to determine is: ‘Does AB have capacity to decide whether or not to be tube fed?’ and not ‘Does AB have capacity to make decisions about treatment relating to anorexia nervosa?’. She argues that to frame the question more widely in the second way may be disproportionately restrictive of her personal autonomy. It would, for example, remove her ability or agency to make decisions about whether to undergo therapy or counselling, or admission to hospital for these purposes as opposed to forcible feeding, or whether to accept injections of dextrose or intravenous nutrition or hydration.
Acknowledgement of capacity to refuse life-sustaining treatment
We have already noted that there is no case to date of a person with longstanding AN being found to have capacity to refuse treatment to address low weight. In the post-2020 cases, however, there has been clearer acknowledgement that incapacity is not a foregone conclusion. As Lieven J said in A Mental Health Trust v ER, ‘capacity and autonomy are such important principles, that lack of capacity cannot be assumed for the sake of expediency’. 25 And in Re Patricia in 2023, the court confirmed ‘that judges should not automatically come to the conclusion that those with anorexia nervosa lack capacity’. 26
In Lancashire and South Cumbria NHS Foundation Trust v Q, Q was found to have capacity to refuse treatment. In Q's case, the capacity assessment was for treatment for her hypokalaemia – low potassium levels that resulted from her bulimia nervosa – rather than treatments that might address low weight or her eating disordered behaviours. 27 Hypokalaemia (low potassium) which is often seen in eating disorders (particularly anorexia nervosa and bulimia nervosa) is usually due to vomiting, laxative abuse or other purging behaviours and is an unintended consequence of behaviours which are intended to eliminate or cancel out nutritional intake. Hypokalaemia is medically dangerous as it can cause cardiac events. Treatment tends to be replenishment of potassium levels either orally, or via a medically-supervised intravenous infusion. Potassium levels have no impact on body weight. This means that the assessment of capacity for Lancashire and South Cumbria NHS Foundation Trust v Q was at base about managing her medical comorbidities rather than about treatment countering the drives and values of an eating disorder, or an attempt to help the patient recover. These factors limit the likelihood of comparable findings in longstanding AN cases, but Q's case does demonstrate that there is discussion to be had about the framing of the decision around which capacity is based. This is largely a matter for trusts who frame the terms of the declaration sought, but it is open to the court to interrogate the nature of the decision that P is making and potentially to challenge that framing.
Q was a 50-year-old woman who had been admitted to mental health units at least eight times. Two years previously, Q had made an advance decision to refuse treatment refusing all treatment relating to low electrolytes and to life-saving measures. The trust sought a declaration as to its validity. The advance decision was valid in its format and so the matter turned on Q's capacity, which was taken to ‘stand or fall with the issue of current capacity’. 28 In light of the evidence of her longstanding view that active treatment was not leading to meaningful improvement, and that she was simply ‘sick of it’, notwithstanding her desire to live, and the acknowledged unwiseness of the decision, Hayden J found that Q had the requisite mental capacity. 29
Hayden J recognised that the likely consequence of his decision was that Q's death would be hastened. 30 There are parallels here with the argument that in some cases of longstanding AN, P might be able to form a view on the futility and harm of active treatment even if they could be found to lack capacity to make a decision about weight-maintenance. Q's decision was not framed around her bulimia nervosa and its impact on her decision-making about food. It was framed around her understanding of low potassium levels and the impact this would have on her health, including the consequences of refusing medical treatment for the low levels.
Judicial control of the capacity assessment
Finally, an additional development which moves towards a more patient-centred framing of the capacity assessment is reliance on a wider pool of independent experts (coinciding with one of our three 2017 recommendations) and evidence of greater willingness to question expert views of patient incapacity.
Turning first to the pool of experts, the independent expert in all of the first phase of cases was Dr Glover. We respectfully suggested in 2017 that a broader range of clinical viewpoints is important given the plurality of clinical views on the prognosis and treatment options of patients with longstanding AN. In the second set of cases post 2020, Dr Glover still serves the court, 31 but there are also at least two additional experts involved. 32 In some cases there is no independent expert appointed, and the court instead relies on the health professionals caring for P and pertinent second opinions. 33
There has also been a marked shift away from deference to clinical expert views of a single expert that P lacks capacity. At present, the authors are aware of moves within England to establish a more formal system for seeking second opinions to help resolve disagreements, whilst recognising that finely balanced decisions or those where disagreement cannot be resolved must come before the Court of Protection.
In A Mental Health Trust v ER & Anor, Lieven J made clear that even in the context of anorexia nervosa, capacity is for the court and not medical experts to determine.
34
And in Lancashire and South Cumbria NHS Foundation Trust v Q, the court diverged from advice provided by the independent expert on matters of P's litigation capacity.
35
On decision-making capacity regarding the treatment decision, Dr Glover considered the matter ‘delicately balanced’ but Q's General Practitioner, Dr Gauge who knew Q well, spoke of the steadfast nature of Q's wishes and considered that Q had capacity to make the decision.
36
The court agreed saying: [I]t is difficult to resist the conclusion that [Dr Glover's] instinctive professional desire to save Q's life has, to some degree, obfuscated his focus on the central question of capacity. Jackson J described this as: “to allow the tail of welfare to wag the dog of capacity.” (Heart of England NHS Foundation Trust v JB (supra)). That is an ever-present danger for all the professionals involved in these cases including, if I may say so, the Judge.
37
In conclusion there is evidence that not only are Court of Protection judges carefully considering capacity rather than accepting a catch-22 in which P inevitably lacks capacity, but they are also interrogating the framing of the capacity assessment, albeit without shifting away from the focus on physical weight in any case so far on longstanding AN. Additionally, judges are showing a greater willingness to question medical evidence that capacity is lacking. This – together with the widened pool of independent clinical experts and greater willingness to challenge their capacity assessments – advances toward the patient-centred decision we recommended.
The best interests assessment
Our third recommendation concerned best interests determinations for patients found to lack capacity. In Re E Jackson J admitted that the determination of best interests ‘is not mechanistic but intuitive’. 38 We were concerned that the outcome of the pre-2017 cases combined with clear recognition that best interests should be determined from P's point of view, 39 might lead to assumptions that P's stated view that treatment is futile should be considered central to their best interests, even if it is recognised that the view is not capacitous and not an authentic expression of their will. In other words, recognition that P should have freedom to decide what to eat and how, could fail to give sufficient weight to P's interest (and in many cases, their stated wish) to live.
A defining feature of these cases is the considerable tension inherent in applying a patient-centred interpretation of best interests when the illness impairs P's capacity to express their will and preferences regarding last-resort treatment – interventions that may both provoke resistance and be essential for preserving life. In the recent cohort of cases, the framing of the declarations sought and the Court's responses reflect a commendably individualised approach to determining best interests. We identify and analyse four ongoing tensions: first, differing perspectives on the goal of treatment; second, disagreement over whether and when a ‘hands-off’ approach is appropriate; third, the friction between judicial assessments of best interests and the systemic pressures shaping such decisions; and fourth, procedural tensions arising from the interaction of distinct legal frameworks.
Treatment goals
The clinical approach in England and Wales is guided by the relevant legal framework. In most cases of compulsory treatment of mental disorder, that is the MHA. The Code of Practice to the Act emphasises that the goal of treatment is not necessarily cure and that conditions should not be considered ‘inherently untreatable’: 23.6 Even if particular mental disorders are likely to persist or get worse despite treatment, there may well be a range of interventions which would represent appropriate medical treatment. It should never be assumed that any disorders, or any patients, are inherently or inevitably untreatable. Nor should it be assumed that likely difficulties in achieving long-term and sustainable change in a person's underlying disorder make medical treatment to help manage their condition and the behaviours arising from it either inappropriate or unnecessary.
40
On this basis, medical treatment is not rendered ‘inappropriate’ by virtue of the condition being incurable, or progress being transient. But what of the MCA framework? The best interests assessment will differ depending on whether the goal is management or cure. In relation to a pre-2017 case, John Coggon argued that the notion of a treatment decision requires more careful analysis, suggesting that a narrowly defined purpose of treatment may be inconsistent with Lady Hale's position in Aintree v James 41 that treatment should not be considered futile solely because it offers no realistic chance of cure or palliation. 42 Treatment can be beneficial to P even if it has no effect on the underlying condition, for instance to maintain hope and keep patients alive so quality of life can be addressed. The goal might therefore focus on management even if cure is unlikely or impossible.
This position is reflected in a 2023 judgment concerning a woman anonymised as ‘Patricia’, who at the time was age 23. Moor J distinguished between the chances of full recovery and the chances of maintaining a survivable BMI. The former was as low as 5 per cent. Expert evidence suggested that ‘if she was force-fed and brought back to life, as long as she then eats a certain amount, she may be able to maintain a BMI that is survivable and have a life that is not full but is worth having’. 43 However, the court held in that case that Patricia should not be compelled to accept treatment and that any nasogastric feeding must be undertaken with her consent. It follows that, while the Court of Protection has recognised that cure is not necessarily the objective, a tension persists between the outcomes clinicians, and the courts may each regard as consistent with P's best interests. To understand the reasoning behind the 2023 order in Patricia and its subsequent recission in 2025, we must consider the second tension.
When is a ‘hands-off’ approach justified?
In several cases, having recognised that P lacks capacity to make a decision, and that without forced nasogastric feeding their life is in danger, the court has nevertheless opted to put P in charge of their own destiny. For example, in A Midlands NHS Trust v RD, Moor J said: I am removing any threat of compulsion or compulsory admission to hospital under the Mental Health Act from RD. I am not going to require her to have NG feeds, unless of course she wishes to have them and agrees to such treatment. I do, however, urge her to comply with what the doctors recommend.
44
And in Gloucestershire Health & Care NHS Foundation Trust v FD, Francis J said I … find that it is in FD's best interests for me now to hand FD control over her own destiny, all decisions in relation to nutrition and hydration and any necessary medical treatment. … I do this because I have been persuaded that any further compulsory treatment and force-feeding and/or hydration would be futile, such a process having failed for some 17 years.
45
At first glance this suggests a misplaced reliance on P's will and a focus on long-term goals in place of effective management. This is because P has been found to lack capacity regarding the decision about which they are given control in a situation where it is likely to lead to their death. However, the hopes expressed in several of the cases are that it is P's objection to compulsion that drives their lack of cooperation and, absent the compulsion, that they might accept forms of treatment sufficient to maintain a BMI compatible with maintenance of life. The hope that P will survive is often expressly slim but made in the context of there being no viable alternatives given the assessment that available treatment options will not lead to meaningful improvement and are causing harm.
There is an evidentiary tension as to whether the hope that P will take control is justified. This is an individualised assessment, but the evidence relevant to that assessment is limited and contested. One source might be the impact of the judgments themselves, but whilst the courts do sometimes provide a postscript indicating the outcome for a patient, that is rare in this subset of cases. We might look to expert evidence, but there is division. For example, in the 2023 judgment concerning Patricia, Moor J said of one expert [H]e effectively accepted that his position was that it would never be right to stop and that his view would always be that you should continue to treat and, if necessary, to force-feed. He justified this on the basis that [Patricia] might be right about what gives her the best chance of a good life, but she might also be wrong. She has a partner and her partner is the anorexia which controls the other part of her mind and stops her carrying out her wishes.
46
The concept of futility is highly controversial in anorexia nervosa.
47
Some clinicians consider that returning control to P under the MCA framework, is to abandon them to a treatable mental disorder. Indeed, whilst there is some evidence that this approach can be effective in the short term,
48
the picture is far more clouded for long-term outcomes, with inconsistent findings.
49
Gorrell and colleagues in a comprehensive overview of possible predictive variables conclude that recent findings continue to suggest a consistent negative impact on ED course and outcome associated with low weight (particularly in AN); emerging yet consistent data appear to support the potential relevance of early-life trauma and emotion dysregulation on outcome. Data regarding the effects of illness duration, psychiatric comorbidity, and symptom severity remain conflicting, and research focused on social determinants of health and neurobiological factors remains limited.
50
Patricia's case came back to court in 2025 where Arbuthnot J reconsidered, and ultimately lifted, the 2023 order. The evidence suggested that Patricia's life was in significant danger because of her low weight, but that she wanted to live. Following the 2023 order she had initially gained weight but then progress had stalled. Arbuthnot J considered that ‘There is no doubt now that the hands-off approach, leaving it to Patricia to decide whether to increase her BMI, has not worked’. 51 There was no criticism made of the 2023 decision. The best evidence then was that viable and effective treatment options had run out and returning control to Patricia could result in her engagement with treatment. 52 By contrast, in 2025 an ‘alternative approach’ was on the table, and it was clear that returning control to Patricia was not an effective strategy. Nevertheless, the case may indicate a subtle shift in the emphasis placed on P's will and preferences in light of the clinical implications that can flow from returning control to P.
Systemic pressures
Patricia's case demonstrates that the ‘hands off’ approach can do ‘more harm than good’. 53 It is settled law that the court can do no more for a patient who lacks capacity than it could for one who possesses it; it cannot compel clinicians to provide treatment that conflicts with their professional judgment. 54 In seeking declarations and outlining possible courses of action, trusts indicate the range of treatments they are willing to consider. In some instances, that range is very limited. Where treatment has been repeatedly attempted without success and has caused significant harm, the court may conclude that it is in the patient's best interests not to be treated coercively. In other cases – such as Patricia's in 2025 – clinicians may offer a new or repeated intervention, sometimes novel or experimental in nature, which the court will consider with care. 55
What is clear is that the court's order can have a significant impact on the treatment options available to the patient. In Patricia's case, following the 2023 order, her renewed willingness to engage with treatment was met with reluctance from trusts unwilling to admit her to specialist units unless compulsion remained an option. Constrained to consensual pathways that Patricia was, due to her condition, unable to sustain, she was left without any viable treatment option until the order was lifted in 2025. 56
As noted above, the context in which such decisions are made is systemically inadequate. In 2017, the Parliamentary and Health Service Ombudsman criticised eating disorder services for failing to respond adequately to life-threatening risk. 57 In 2025, McKendrick J delivered a scathing critique of service deficiencies that left 17-year-old AB without appropriate treatment and support. 58 Patricia's case serves as a salutary reminder that the courts may inadvertently worsen these systemic shortcomings by failing to anticipate clinical developments and by unduly constraining medical discretion until a matter is brought back before the court.
Procedural issues
Removing the threat of compulsion also raises a procedural issue. Moor J's 2023 decision in Re Patricia did not formally bind clinicians from detaining and treating Patricia under the MHA, but doing so would conflict with the best interests determination made in accordance with the MCA. The MHA permits compulsion based on risk, without regard to capacity, whereas the MCA requires acting in a person's best interests only if they lack capacity, and respecting their autonomy if they do not. Nonetheless, the Acts are increasingly aligned: the MHA's focus on appropriateness echoes MCA best interest principles, and the Mental Health Bill 59 seeks to strengthen this by emphasising autonomy and consent. In Leeds and York Partnership NHS FT v FF 60 McKendrick J decided that FF lacked capacity and that it was no longer in her best interests to receive food by force. The trust also sought a declaration that they should not rely on section 63 of the MHA 1983 to impose compulsory treatment on FF. McKendrick J recognised that ‘Having concluded it is not in her best interests, I cannot see a proper case for this court to refuse the declaration sought’. 61 The order was made under Civil Procedure Rules rather than section 15 of the MCA, and this is surely good practice going forward.
Futility
We might conclude that our prior concern about when to rely on P's views about the futility and harm associated with compulsion in situations when they lack capacity continues to vex both clinicians and the courts. There is no single or simple solution. Each case will be determined on its particular facts. But there is a sense in which an increasingly nuanced consideration of futility is developing in cases involving patients with anorexia nervosa.
Under the MCA, well-established jurisprudence on the meaning and assessment of futility in decisions about life-sustaining treatment has been adapted to account for the specific context of anorexia nervosa. The MCA Code of Practice envisages that treatment may not be in P's best interests if it is futile and burdensome to the patient: 5.31 All reasonable steps which are in the person's best interests should be taken to prolong their life. There will be a limited number of cases where treatment is futile, overly burdensome to the patient or where there is no prospect of recovery. … 5.33 Importantly, … doctors are [not] under an obligation to provide, or to continue to provide, life-sustaining treatment where that treatment is not in the best interests of the person, even where the person's death is foreseen. …
62
Under the MCA, acts in connection with the treatment of P who lacks capacity are only lawful if they are done in P's best interests. 63 Active treatments for anorexia nervosa should not be considered futile merely because the evidence suggests they cannot effect a cure. But they might be considered futile if the evidence suggests they cannot sustain short-term health or management of the condition so that it will bring about an acceptable quality of life. It bears repeating that consideration of futility is part of the best interests assessment and not a standalone test. And it is essential to understand that where life is at stake and questions around capacity or best interests are finely balanced or disputed, the Court of Protection should be approached to make a declaration of P's best interests. 64
Futility can be physiological if treatment will not bring about management of the condition, and it can have a qualitative element if managing the condition will have a serious impact on P's quality of life. Once the case comes to court, the assessment of futility is made by the judge, in light of evidence from clinical experts. The judge does so not as a standalone test, but as part of their assessment of the patient's best interests, where a patient is found to lack capacity.
There is another aspect of the notion of ‘futility’ that runs through these cases, namely that of hope and meaning. In a time of controversy and polarisation of views, there is a place for compassionate, person-centred and patient-led care, using collaborative approaches which neither abandon patients as futile and not worth treating further, nor perpetuate escalation of coercion and restrictive practice. 65 The National Eating Disorder Collaboration in Australia, for example, in its Holding Hope Guidance, provides a rights-based, autonomy-respecting approach which supports shared decision-making. 66
Embedded in the concept of futility is the notion that ‘all hope is gone’ and recovery is impossible. However, even when they are dying and recovery is impossible, people with life-limiting illnesses can be supported to have a quality of life and find meaning in what remains in their lives – this is the core tenet of palliative care. 67 In the cases which have come to the Court of Protection, as well as in the wider societal controversy over the concept of ‘terminal anorexia’, there is a risk of overlooking how the person's wishes and values as well as their meaningful relationships can be heard and supported. This respectful discussion of both the issues at stake and the person's wishes and values can enable them to find meaning and hope, which may mean that they are able to accept support and even re-engage in treatment, as expressed by the judges in Re Patricia [2023] and Re FD, discussed above.
Conclusion
In this article, we have revisited our 2017 critique of a series of five Court of Protection cases in light of a more extensive series of cases that started in 2020 and continue to date (see Table 1). We have used our three recommendations as a framework to assess the development of case law in light of new treatment possibilities and tensions around controversial suggestions that anorexia nervosa might in some cases be considered ‘terminal’. We suggest in this article that the concerns we identified in 2017 are shared by, and to some extent addressed in, subsequent judgments.
The first 2017 recommendation was that courts adopt a patient-centred, rather than clinician-dominated approach when framing the decision around which capacity is assessed. We are encouraged by the Court of Protection's clear affirmation that incapacity should not be presumed solely on the basis of diagnosis. Recent judgments demonstrate a consistent willingness to closely examine P's capacity to litigate and also to make decisions that diverge from clinical advice, reflecting a rigorous and individualised approach.
The second concern was the over-reliance on a single independent expert, as seen in all five of the pre-2017 cases, which risked limiting the court's perspective. We welcome the subsequent broadening of the pool of experts and the increased use of second opinions, enhancing the diversity and robustness of clinical input.
Finally, we argued in 2017 that when a person with longstanding AN is found to lack capacity, focus on P's will and preferences in the determination of their best interests should take into consideration the impact of their condition on their preferences. This becomes especially problematic if P's (potentially unauthentic) perception of futility aligns with a judicial evaluation that measures the appropriateness of treatment primarily against the goal of cure rather than ongoing management of the disorder. We have found that whilst the judges in the post-2020 cases do sometimes return the matter to P's control, this is because both the long-term chances of cure and the short-term effectiveness of highly burdensome treatment in managing the condition are so low that continued compulsory treatment is considered futile.
We have recognised that the assessment of futility is but part of the best interests assessment, which also looks to other factors, including P's preferences. However, there may be room for a distinction to be drawn between two types of futility: the futility of repetition of the same treatment already shown to be ineffective or alternatively ever more escalation of compulsion and restriction; and a more global, holistic concept of futility in terms of the chances of ever being able to live a good quality of life or even to recover. We can with some confidence determine when the first type of futility exists; however, evidence does not enable us to be sure when the latter type of futility applies.
We have articulated differences between the mental health and mental capacity legal regimes that are impacting practical treatment options for patients and the ethical norms that guide them.
Finally, just as science is advancing and changing in terms of whether we can predict outcomes on an individual basis, there is also ongoing research on novel treatments for longstanding severe eating disorders. Both of these may result in more clarity and more hope in the future.
Footnotes
Acknowledgements
We would like to thank the anonymous reviewers for their helpful comments. Thanks also to the Law and Ethics of Anorexia Nervosa – Values in Practice Network for providing a stimulating environment for discussions that helped shape the ideas in this article. Special thanks to Jess Griffiths, Rachel Jenkins, Nikola Kern and Alex Ruck Keene for their generous and insightful comments on earlier drafts.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.