
Abstract
Given the costs of litigation high-profile court cases about withdrawing life-sustaining medical treatment for seriously ill children in England & Wales tend to be followed by discussion about how to avoid similar cases in future. Whilst two proposals, mediation and replacing the best interests standard with a harm threshold, have received broad attention, a proposal to replace the court by a specialist review committee has not been further investigated. This article analyses the effects of a putative replacement of the courts by a specialist review committee using the process enacted by the futility clauses in the Texas Advance Directives Act (TADA) as a model. Under TADA life-sustaining treatment may legally be withdrawn when a review committee deems it futile and no alternative healthcare provider can be identified. The investigation finds that installing a national review committee with the power to decide whether life-sustaining treatment is futile would have reduced the number of court cases about withdrawal thereof in England & Wales to a handful over the last 3 decades. In addition to shorter procedures and costs savings, a national review committee modelled after TADA would have advantages for both clinicians and parents. Advantages for clinicians are more limited exposure to delivery of clinical care that may cause moral distress and less exposure to adverse press and social media content. Advantages for parents are that the process would establish them as ethical decision makers and offer the possibility of a transfer of the care of the child provided an alternative healthcare provider can be found. As such decisions taken by a specialist review committee may be more acceptable for parents than those of the courts.
Keywords
Introduction
High profile cases in which withdrawal of life-sustaining medical treatment for seriously ill children is litigated in England & Wales tend to be followed by discussions on how to avoid similar cases in the future.1,2 Some proposed solutions, i.e. the introduction of a harm threshold3,4 and improved conflict resolution through alternative dispute resolution methods such as mediation 4 have been extensively debated but lack evidence they prevent litigation.5,6 However, another proposal, namely to replace the courts by a specialist review committee,7–9 has not been further investigated. This is somewhat surprising as review committees are already operating successfully elsewhere. In this paper I aim to address this gap by investigating the effects of a putative implementation of a review process similar of that currently operating in Texas, USA.
In 1999 the state of Texas, USA enacted the Texas Advance Directives Act (TADA). 10 The futility clauses 11 within TADA empower local review committees to arbitrate in disputes about life-sustaining treatment for incapacitated patients on request of the treating clinician. Should the reviewing committee decide that continuing life-sustaining medical treatment for a particular patient is futile the treatment can be withdrawn if, after a period of time defined in the Act, an alternative health provider cannot be found. Following the procedure set out in TADA protects clinicians from civil, criminal and regulatory challenges should they withdraw life-sustaining medical treatment without consent.
Implementing a process similar to TADA in England & Wales would entail 2 important changes; first it replaces the court with a specialist review committee and second it replaces best interests of the child as decision-making standard with futility.
Replacing the courts
Given the plurality of values in current society, it is reasonable to assume that intractable conflicts about withdrawing life-sustaining medical treatment for a child are inevitable 12 and thus for some cases arbitration will remain necessary. Whilst a court decision (ultimately) will end the conflict, the process in itself is adversarial, lengthy, and costly. Moreover, it can be argued that parents and wider society are now less accepting of the courts making these decisions. Whilst many parents still say they will abide by the court's ruling also if that goes against their sincerely held beliefs,13,14 on a number of occasions parents have resisted either the judgement or the court procedure. For example, families have left the country to avoid complying with the judgement 15 or court procedure. 16 Others moved the care for their child to another NHS Trust once proceedings were started 17 or simply refused to engage.18–20 In addition, families have tried to frustrate the court procedure, i.e. by parting company with their legal team just before the start of a hearing in an attempt to cause a delay.21,22 More recently, a family arranged for transfer of the medical care of their child after exhausting the legal process thus sparking a new round of court cases. 23 In addition, in the last few years, protests and demonstrations24–26 as well as financial support for families involved in court proceedings might be taken as an indication of a broader societal rejection of the role of the court in medical treatment decisions for seriously ill children.
Tied to the above, there is a lively discussion in British society as well as in academia about the question who should have the ultimate say about the medical treatment of seriously ill children; parents or clinicians. In academic literature, Bridgeman
27
for example speaks about treatment contrary to professional conscience and argues that clinicians should not be compelled to deliver treatment that is, in their view, futile whereas Auckland and Goold
28
argue that because these decisions are value-laden parents should have the final say. Both views are however compatible with a transfer of the child to able healthcare providers who are willing to deliver the contested treatment. It is not unusual for parents to have the final say when healthcare professionals disagree. Indeed, this is compatible with judicial thinking in England & Wales as expressed by Hedley J: ‘[W]here a clinician concludes that a requested treatment is inimical to the best interests of the patient, and that his professional conscience, intuition or hunch, confirms that view he may refuse to act and cannot be compelled to do so, though he should not prevent another from so acting, should that clinician feel able so to do.’
29
(emphasis added)
A transfer of care to a capable and willing healthcare provider as enacted in TADA should be able to resolve some of the intractable conflicts currently reaching the courts.
Futility
Deciding that withdrawal of treatment is in the best interests of a child implies a preceding decision that the medical treatment under discussion is judged not to deliver enough benefit. For example, explaining his decision to allow withdrawal of life-sustaining treatment from Charlie Gard, a child with a lethal metabolic condition, Mr Justice Francis said about the experimental treatment available in the USA: ‘The prospect of the nucleoside treatment having any benefit is as close to zero as makes no difference. In other words, as I have already said, it is futile.’
30
The futility of the nucleotide treatment and the absence of other treatment options determined that providing life-sustaining treatment was not in Charlie's best interests.
Futility does have a somewhat tarnished reputation as concept for decision-making mostly because it lacks precise definition.31,32 The main reason the concept of futility is indeterminate is because it contains value judgements, a characteristic it shares with other concepts such as ‘best interests’. 33 In defining futility Schneiderman et al.34,35 differentiate between a judgement about the probability that medical treatment will be effective and judgements about the quality of the resulting life. A similar approach is taken in guidance of the Royal College of Paediatrics and Child Health (RCPCH) about limiting life-sustaining treatment for children. The guideline has inter alia the categories ‘life limited in quantity’ and ‘life limited in quality’. 36 In both definitions the former is a technical medical decision, the latter a value judgment. Proponents of the use of the concept of futility thus rightly point out that in clinical decision making futility remains an important concept given the ultimate powerlessness of medical science in the face of human mortality.35,37 Moreover, medical futility is dependent on the goal of treatment. 38 Whilst for physicians a return to relative health or at least independence from intensive care is the goal, for some parents the goal is to sustain life as long as possible or until ‘a natural death’ occurs. 39 Value judgements about what constitutes a ‘good death’ in addition to value judgements about what constitutes a ‘good life’ are both part of disputes whether life-sustaining treatment for this particular child is futile.
The duality implied in the term ‘futile treatment’ or ‘futility’ in Schneiderman's definition described above has led to calls to use different terminology. TADA itself uses the term ‘medically inappropriate treatment’. More recently the term ‘potentially inappropriate treatment’ has been advocated for to ‘describe treatments that have at least some chance of accomplishing the effect sought by the patient, but clinicians believe that competing ethical considerations justify not providing them.’ 40 Below I will use the term ‘potentially inappropriate treatment’ in the sense described above. The term ‘futile’ treatment is reserved for treatments that cannot achieve the physiological goals and for that reason should not be provided. In this terminology an example of futile medical treatment would be providing ventilatory support to a child no longer alive, e.g. a brain dead child. Whilst conflicts about futile treatment in this sense are rare the question has been litigated in the courts of England & Wales albeit as a request for a declaration of death rather than as a best interests decision. 41
I will however continue to speak of ‘futility clauses’ to refer to the clauses in TADA that regulate the withdrawing of life-sustaining treatment without consent as the term is broadly used in the literature about TADA.
To investigate how an implementation of a review committee similar to those enacted by TADA would affect the resolution of intractable conflicts about withdrawal of medical treatment for children in England & Wales, I proceed as follows. In Section 1 I describe the process of dispute resolution regulated by the futility clauses in TADA as well as reported experience with the procedure and criticisms thereof so to be able to outline the characteristics of a specialist review committee suitable for England & Wales. In Section 2 I investigate the expected advantages and pitfalls of implementing a specialist review committee. In Section 3 I investigate how a specialist review committee deciding on potentially inappropriate medical treatment would serve the interests of clinicians and parents respectively. Lastly, in Section 4 I describe how the landscape of conflict resolution would change should a specialist review committee replace the courts in England & Wales.
Based on the investigation I conclude that replacing the current court system by a procedure modelled after TADA would avoid most but not all court applications. Those that currently reach the court because there is nobody with sufficient parental responsibility available or when parents disagree with one another will continue to require a court decision. However, replacement of the court by a specialist committee should lead to shorter procedures and therefore limit costs whilst still providing legal certainty for clinicians. Moreover, replacing the court by a specialist review committee deciding on potentially inappropriate treatment might be attractive for both clinicians and parents. Using such a standard for decision making in combination with the possibility of a transfer of care for the child respects both the ethical decision making of clinicians and parents.
Section 1: About TADA
Whilst TADA regulates several aspects of end-of-life care, here I will only review the process enacted by its futility clauses. 11 The procedure is as follows; a treating physician who feels that life-sustaining treatment for an incapacitated patient is potentially inappropriate or futile but cannot reach agreement with the surrogate decision-maker a or the patient (by advance directive) about its withdrawal, can refer the case to a local hospital review committee. TADA empowers these committees to decide whether a particular life-sustaining treatment should be continued. Should the committee find the treatment is beneficial it will be continued. When considered inappropriate, the hospital, working with the family, must try to arrange transfer to another provider who is willing and able to continue the treatment. If after a period of time defined in the Act b no such provider can be found, the physician may legally withdraw the disputed treatment.
The rights of the patient and family are protected by clauses determining that prior to the committee's review the family is informed about the local process, given notice of and be invited to participate in the review committee's meeting. To participate in the review process, for both the clinician and patient legal representation is permitted but not obligatory. The review committee must provide the family with a written report about their findings. The decision of the committee itself cannot be appealed thus the process after a committee's finding that continuing life-sustaining treatment is inappropriate is time-limited. Whilst the committee's decision cannot be appealed, the family can appeal to the state court for an extension of the time in which to find an alternative health care provider. An extension can only be granted if there is a reasonable likelihood of finding a willing provider.
The futility clauses in TADA have been in place since 1999 and have undergone several changes. Relevant changes are the inclusion of paediatric cases in 2003, 42 the exclusion of withdrawal of artificially administered hydration and nutrition in 2015 43 and an extension of the time periods for notification to the family of the review process as well as the time allotted to find an alternative healthcare provider in 2023. 44
Implementing a model similar to TADA in England & Wales would thus require a marked movement in ethical thinking towards more discretion for parents in deciding about life-sustaining treatment for their child. Whilst in the TADA model the parents are still restricted to medical treatment that clinicians are prepared to provide, the offered treatment elsewhere may be considered not to be in the best interests of the child by their original clinical team.
Reported experience with TADA
Because TADA does neither enact mandatory data collection nor publication of committee's decisions the reported experience with its procedure is limited to a handful of academic papers describing experiences in the first decade after enactment.45–48
The first paper, written by authors who were involved in writing the futility clauses in TADA, describes the experience of a single institution in the first 2 years after TADA's enactment. An increase in ethics consultations about the potential inappropriateness of life-sustaining treatment which resolved most disagreements (37/47) lead the authors to conclude that TADA's existence improves communication between families and clinicians. 46 The committee found treatment to be inappropriate in all 6 cases that it reviewed. All families subsequently agreed to its withdrawal.
The second paper reports the findings of a survey covering the first 5 years after TADA's enactment. The survey shows that use of the TADA procedure is limited to larger, urban and teaching hospitals. 48 In 178/256 (70%) cases reviewed the committee considered the treatment should be discontinued. Of the 178 patients 78 died before treatment could lawfully be withdrawn, 71 families agreed to withdrawal of treatment, 30 patients were transferred and 8 patients improved to the extent that treatment was considered beneficial by their clinical team. c Treatment was withdrawn in less than half (33/78) of the remaining patients.
Authors from three hospitals have reported 12 cases of children for whom the TADA procedure was invoked.45,46,49 The children were diagnosed with a variety of life-limiting disorders. In 2 cases the family agreed to withdrawal of treatment after being informed about the local TADA procedure but before their case was referred. The committees decided that continuing treatment was inappropriate in 8/10 cases. Two children were transferred to another healthcare provider, for 5 children the treatment was withdrawn and one child died before treatment could lawfully be withdrawn.
Two additional children are described in an article based on publicly available data. 50 In both cases the local committee found that continuing treatment was inappropriate. One family was successful in obtaining an extension of the time period for transfer but the child died before the final ruling. In the other case the hospital sought court involvement after having gone through the TADA procedure due to concerns about parental capacity which led to some months delay before life-sustaining treatment was withdrawn.
Criticisms of TADA relevant for specialist committees in England & Wales
Having been in place for over 20 years the process enacted by TADA has received a fair amount of critique. Below I discuss how the critique can be addressed in the setting of England & Wales. Surprisingly little criticism addresses futility as the decision-making standard. Those authors that do point to the indeterminacy of the concept 51 and the resulting subjectivity of any judgements, both of referring clinicians and the review committee. 52 Solutions tend to be sought in improving the procedure rather than changing the decision-making standard.
Communication prior to referral
Concerns have been raised about the lack of standards for communication about the potential inappropriateness of the life-sustaining treatment with the family prior to referral.53,54 Whilst the courts in England & Wales also do not set standards, reported cases contain extensive evidence of previous discussions, second opinions, input of ethics committees and sometimes mediation. However, the amount of communication prior to court application may reflect a preference to avoid litigation. 55 It is possible that clinicians might refer cases at an earlier stage to a specialist review committee. To ensure sufficient communication with the family prior to referral it may be useful to set some standards about prior communication before a referral can be accepted.
Potential for bias
TADA empowers a physician to unilaterally decide which cases to refer for review. 52 This decision-making power has led to concerns about a potential for bias, in particular with regards to race.52,56 There is indeed some evidence that families from ethnic minorities are more often involved in the TADA procedure. 52 Whilst explanations other than discrimination, i.e. a higher preference of intensive care at the end of life for some minority groups 57 are available, even suspected bias in the referral of cases seriously undermines the credibility of the process. The concerns about bias highlights a long recognised oversight in TADA; the lack of statutory data collection and publication.37,58 Due to the lack of data, concerns about bias can neither be substantiated nor addressed. In addition, without a body of previous committee decisions both clinicians and families lack guidance. 59
In England & Wales, NHS Trusts and its physicians also unilaterally decide whether to apply to court; professional guidance and section 11(2)(a) of the Children Act 2004 sets out circumstances in which an application to the court could be considered not when they should be made. Similar to Texas, reliable data about the ethnicity of families involved in litigation in England & Wales is not available. However, because court decisions are generally reported transparency about the court's decision-making has been achieved. The current transparency should be maintained and indeed could be improved upon by compelling specialist review committees to collect and report a minimum set of data in addition to all anonymised decisions.
Standards for committee membership
TADA does not give guidance with regards to the background, qualifications or experience of the committee members. The lack of standards in combination with the lack of appeal53,60,61 has raised concerns that the committee is too powerful, may be biased in favour of their clinician colleagues53,61 and that their decisions may be an unacknowledged rationing decision d rather than a decision about the (in)appropriateness of the medical treatment. 52
For England & Wales some of these concerns can be avoided by implementing a national specialist review committee. The 37 reported cases about withdrawing medical treatment for children litigated between 1990 and December 2023 e suggests the number of cases potentially referred to a specialist review committee will be small enough to allow review by one committee. A national review committee would go some way in eliminating concerns about favouritism towards close colleagues. Moreover, a national review committee could set standards for prospective members. In addition to fair representation of ethnic minorities, the committee could include clinicians, ethicists and lay members to ensure a wider variety of views. A more representative committee might also be more acceptable to both parents and the wider public.
Parental position
Procedural concerns raised in TADA have been about the period of notification prior to the committee hearing 62 and the availability of medical notes. Similar concerns have been raised in England & Wales. The Nuffield Council for Bioethics recently recommended a notification period of at least 3 days prior to a court hearing 63 and a similar period could be used prior to review by a specialist review committee. Equally, the implementation of a specialist review committee should not affect their recommendation to provide parents with their child's clinical notes within 7 days of the request. 63
Guidance for committees
TADA does not set out guidance with regards to how the review committees should make their decisions.52,53 The question whether guidance should be issued to guide the committee's decisions in England & Wales is complex and I do not aim to resolve it here. It should be noted however that currently whilst judges refrain from ethical analysis 8 they generally do adopt the RCPCH guidance on withholding and withdrawing life-sustaining treatment. 64
Emergency reviews
Sometimes a NHS Trust makes an emergency application for withdrawal of life-sustaining treatment.65–67 In the three cases reported since 1990 the reason for the emergency hearing was that the child suffered untreatable pain. For such instances a national specialist review committee should have an emergency procedure that ensures cases can be heard within days.
Funding
Currently in the UK ethics committees in NHS hospitals receive no or minimal funding. A national specialist review committee would require a significant investment to be able to fulfill all the tasks detailed below.
What should a procedure by a specialist committee in England & Wales look like?
Taking into account the experiences and critique of TADA a specialist review committee and their procedure should have the following characteristics:
a national review committee of which the members represent a variety of skills, qualifications and experience statutory data collection and reporting minimum standards with regards to communication about withdrawal of life-sustaining treatment with the parents prior to referral standards protecting parental involvement; i.e. disclosure of medical notes, opportunity for arranging a second opinion prior to referral, invitation to attend and participate in the meeting reasonable periods to notify the family and between review committee decision and time of withdrawal of treatment transparency is ensured through reporting of anonymised decisions retained possibility to hear urgent applications within days
Section 2: Pitfalls and advantages of a National Specialist Committee modelled after TADA
I now turn to potential pitfalls and advantages that the implementation of a national specialist review committee modelled after the committees empowered by TADA would entail.
Transferring patient care
A main advantage of implementing a specialist review committee in England & Wales modelled after TADA is that it offers two solutions to an otherwise intractable conflict about withdrawal of life-sustaining treatment. These two solutions both respect the clinician's ethical objections to providing potentially inappropriate life-sustaining treatment as well as parental ethical decision-making in relation to their child.
As such it is vital that a transfer of the medical care of child is a real possibility. However, in England & Wales it is unlikely that a child whose treatment is judged to be potentially inappropriate by clinicians in one NHS hospital will be accepted by another. Indeed, for Isaiah Haastrup, a child who suffered catastrophic brain damage due to deficiencies in obstetric care 68 and who was at the centre of a high-profile case when the Trust applied to withdraw his life-sustaining treatment, several London hospitals declined a transfer into their care. 69 Any transfer of care would thus most likely involve a healthcare provider abroad. Apart from practicalities, i.e. visa applications, an important question that families will face is how to fund the treatment. Absent personal resources families will have to resort to crowdfunding. However, research shows that crowdfunding for medical treatment does not reach it stated target in 90% of cases. 70 The family of Tafida Rafeeq for example for whom the court did allow a transfer of her care to an Italian hospital, 71 raised only 17% of their goal. 72 Moreover, Figure 1 depicts a more recent fundraising effort for Indi Gregory, 73 a child with a life-limiting disorder involved in litigation about withdrawal of life-sustaining treatment, showing that donations are closely related to the publicity generated by court procedures. Publicity is likely to be less should repeated public court procedures be replaced by a single more private procedure by a national specialist review committee. For parents to raise sufficient funds for treatment will thus be even more challenging. Should a specialist review committee modelled after TADA be implemented in England & Wales difficult questions about the period of time given to parents to raise sufficient funds before life-sustaining treatment can be legally withdrawn will need to be answered. A transfer of care may only be achievable for a select group of (wealthy) parents.
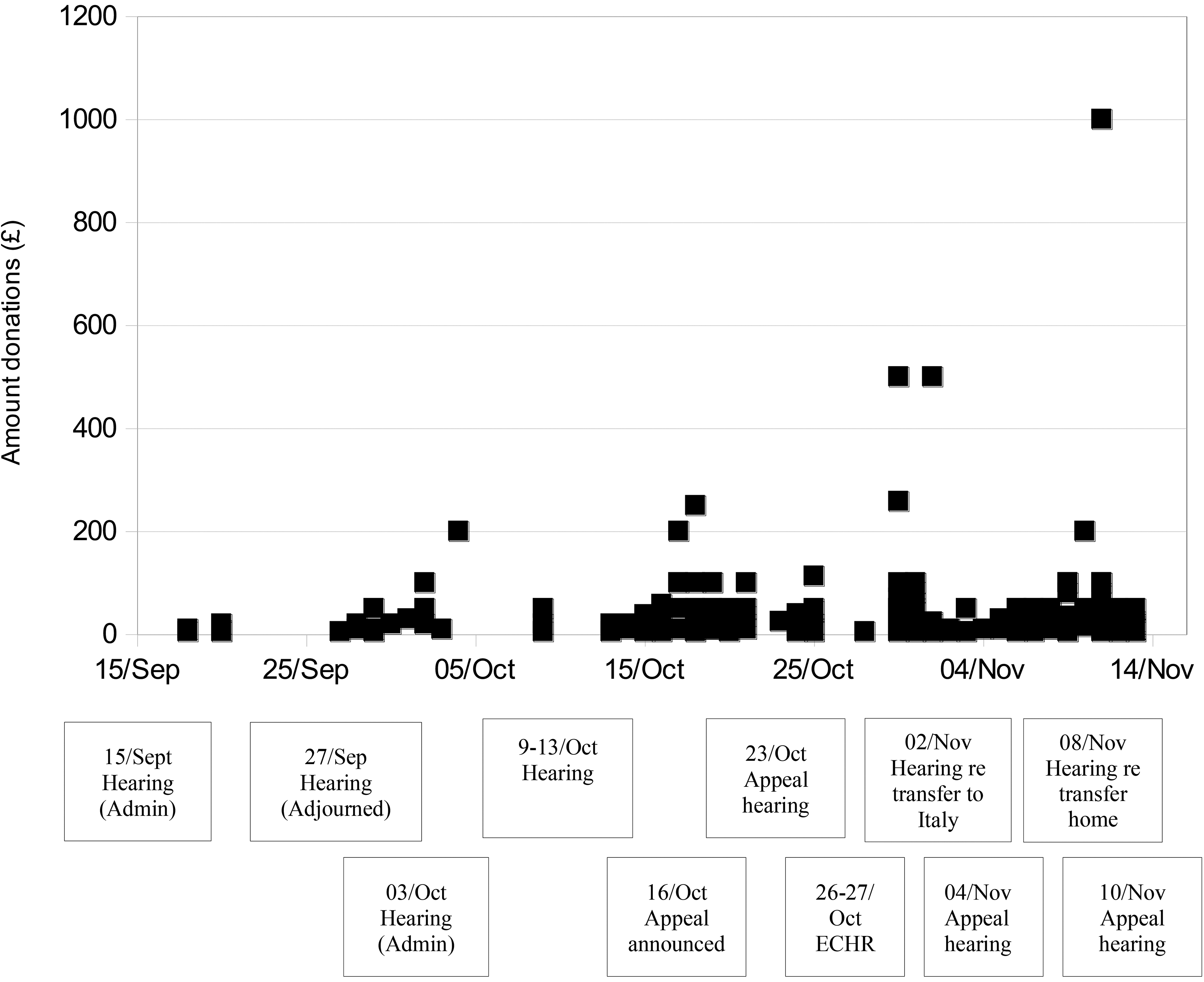
Graph showing close relationship between court dates and donations as reported on the GoFundMe page for Indi Gregory’s treatment and appeal (https://www.gofundme.com/f/the-right-to-stay-alive-and-fight-the-courts). Data collected between 15/09/2023 and 13/10/2023.
Temporal boundaries
An important advantage of a national specialist review committee modelled after TADA is that it provides clear temporal boundaries mostly because the committee's decision cannot be appealed. Whilst that may seem radical it should be noted that in the 35/37 reported cases since 1990 in which the applying Trust gained permission to withdraw life-sustaining treatment all appeals have failed to reverse the first decision of the High Court. The average length of the judiciary process based on data in reported cases is summarised in Table 2 in the Supplementary Data. Excluding urgent applications, the average time between application and first High Court decision for cases in which withdrawal of life-sustaining treatment is litigated is 3.6 months (range 1–9 months) whereas appeals add on average 7.5 weeks (range 3–14 weeks). It seems reasonable to assume that a single review by a national specialist review committee will result in a shorter procedure.
However, in some reported cases parents return to court when they cannot reach agreement about other aspects of care. For example, parents have contested the place where life-sustaining treatment is to be withdrawn. 74 Litigation about disputes about other aspects of care when care cannot be transferred would still be possible after an implementation of a national specialist review committee and may lead to an extension of the temporal boundaries. To maintain the boundaries as much as possible it would be important that the courts of England & Wales would treat any applications about aspects of care after the national specialist review committee has decided that continuing life-sustaining treatment is not appropriate as urgent.
Costs
The example of TADA demonstrates that it is possible to engage in end-of-life arbitration without the involvement of lawyers. How much the NHS currently spends on costs of litigation is not known. In 2015 Halliday et al. 75 estimated the costs of legal representation when parties agreed to withdrawal of artificial nutrition in adult patients at £53.000. However, in disputed cases, for example those of Charlie Gard and Alfie Evans, the NHS has spend £420.000 combined. 76 Beside a decrease in the cost of litigation, there may be some additional cost-savings due to transfer or earlier withdrawal of life-sustaining treatment. Whilst costs involved in the setting up and running of a national specialist review committee for which NHS Trusts may be (partly) responsible, may still be substantial it is likely that future costs per case will be considerably less compared to those of a court application.
Section 3: Interests of clinicians and parents
In this section I discuss how the interests of both clinicians and parents in intractable conflicts would be served by a national specialist review committee deciding on (in)appropriateness of life-sustaining medical treatment.
Clinician's interests
Whilst not usually directly addressed in court, clinicians have an interest for themselves in court cases about withdrawal of life-sustaining treatment. It is known that delivering potentially inappropriate or futile medical treatment can cause moral distress in healthcare professionals. Moral distress, defined as a situation in which ‘one knows the right thing to do but constraints make it nearly impossible to pursue the right course of action’ 77 is known to contribute to burn out and post-traumatic stress 78 and to affect patient care in paediatric intensive care environments. 79 Both clinicians and their NHS Trusts have an interest in avoiding delivering medical treatment they deem to be inappropriate.
When the decision whether or not to withdraw life-sustaining medical treatment is left to an arbiter referring clinicians risk that the arbiter finds the treatment should be continued. In court applications this risk seems particularly low. In only 2 reported cases71,80 (6%) since 1990 the court did not consent to the proposed withdrawal of life-sustaining treatment and in one case only the existing clinical team was expected to continue the treatment they in court had described as ‘cruel’. Whether a specialist review committee would more often disagree with clinicians is an open question. In Texas, review committees disagree with the referring clinician in about 20–30% of cases.45,46,48,49 Whilst the experience with TADA cannot be simply be extrapolated to England & Wales a more diverse committee can be expected to make a different analysis and decision. For clinicians the advantage of shorter procedures and clear(er) temporal boundaries may be counterbalanced by a more frequent requirement to continue life-sustaining treatment they deem inappropriate.
In some high-profile cases healthcare staff involved in the care of the child have been the target of public criticism and anger. 81 There are indications that moral distress, combined with the publicity and public anger around high-profile cases cause staff resignations 82 or at least cause some healthcare professionals to reconsider their future career. 83 Moreover, paediatricians feel that press and social media involvement ‘fan the flames’ of conflicts with the parents making it more difficult to resolve the conflict in a private setting. 63 An advantage of the establishment of a specialist review committee could be that it results in a single hearing rather than several court cases exposing healthcare staff to less negative publicity.
Parental interests
Parental decision making tends to be characterised by judges as largely emotional rather than a parental attempt to make a decision in the best interests of the child. Judges have inferred parental decisions as being ‘coloured by their own emotion or sentiment’
84
or parents to be ‘unable to relinquish hope’.
85
Whilst in many judgements the parents are praised for their care and commitment to their child, parents are complimented about their decision-making only in cases when they agree to the proposed withdrawal of treatment. For example, in a case in which the withdrawal of life-sustaining treatment for a severely brain-damaged newborn was litigated, Hayden J said: ‘It is, in my judgment, a great tribute to them, that they perceive an emerging conflict, between the preservation of Danny's dignity, and their understandable wish for him to live. Each of them, and perhaps for different reasons and beliefs, has come to the conclusion that the approach recommended by the Trust is the right one for Danny. It is obvious that each family member is putting his best interests at the centre of this challenging decision.’
86
This judicial position is at odds with how parents see their own role in medical treatment decisions. Research shows that many parents feel they should be the main decision maker about limiting or withdrawing life-sustaining treatment. 87 Several studies highlight that parents see their decision making in the context of trying to be a ‘good parent’.88–90 Whilst moral distress in parents91,92 has not received much attention in academic literature, certainly in intractable conflicts parents are constrained in obtaining what they see as the right treatment for their child and can thus be expected to experience moral distress.
Evidence from TADA shows approximately a third of surrogate decision makers agree to withdraw the treatment when the specialist review committee agrees with their clinician that treatment should be discontinued.46,48 A much smaller group is able to transfer the care of their child or family member. However, the largest group is not able to find an alternative healthcare provider willing to take over the care for the patient.
Thus, whilst, the implementation of a specialist review committee modelled after TADA in England & Wales will empower parents to attempt to transfer the care for their child, an actual transfer will depend on finding an alternative healthcare provider. Some of the parents unsuccessful in transferring their child's care may experience more moral distress compared to the current court procedure when they fail to secure an alternative healthcare provider. Other parents may feel less conflicted once they understand that their wished for care is not provided by healthcare providers anywhere.
Parents have described the court environment, due to its rules and regulations, as daunting and intimidating. 63 Participating in a less formal hearing of a specialist review committee should be less daunting and indeed efforts can be made to make it so for parents. In the absence of a requirement for legal representation, an additional advantage for parents may be that, should they so wish, they can directly participate in the proceedings and will have more of a ‘voice’ than currently in court.
In summary, whilst replacing the courts with a specialists review committee modelled after TADA offers both clinicians and parents advantages compared to the current court system, some aspects of the interests of individual parents and clinicians may be less protected compared to the current court procedure.
Section 4: The changing landscape of dispute resolution
In this section I will investigate what the effect of an implementation of a national review committee modelled after TADA would be on the landscape of dispute resolution and the type of cases that would still reach the courts.
Cases to be decided by the courts
In three types of cases the courts would remain the final arbiter. As discussed above, in cases in which further conflicts arise after a decision on withdrawal of life-sustaining treatment has been taken, the courts would still be the appropriate authority to decide on these additional conflicts.
In addition, a small minority of cases reach the courts because there is no one with sufficient parental responsibility available. Examples include children cared for by a local authority93,94 and children of whom the parent does not have sufficient capacity. 19 Whilst a specialist review committee may decide on the (in)appropriateness of the provided life-sustaining treatment they cannot replace parental consent. There will therefore remain a role for the courts in these cases to decide in the best interests of the child.
Another special circumstance is when parents disagree amongst themselves.95,96 Whilst in England & Wales the consent of one parents is sufficient to give or withdraw medical treatment, when parents disagree about important decisions it is considered good practice for the NHS Trusts rather than the parents to apply to the courts. Whilst in case of a parental dispute a referral to the specialist review committee could still be made in order to reach a decision whether treatment ought to be continued, should their decision not result in agreement between parents an application to the court will remain the final pathway for settlement of the parental conflict.
However, referral to the specialist review committee would prevent court applications when there is no disagreement between clinicians and parents but the NHS Trust applies to the court for a declaration of lawfulness nonetheless. 75 The legal protection provided to the clinician by a review of the specialist committee should be sufficient hence court involvement in these cases would be superfluous.
The implementation of a specialist review committee modelled after TADA would also prevent litigation when parents have already arranged for continued medical treatment elsewhere.21,71,97 Indeed, parents would have the right to arrange a transfer before a referral to the specialist review committee has been made. However, safeguards should be in place to prevent a transfer to a provider of ill repute or who proposes harmful medical treatment, by access to existing child protection procedures.
To maintain comparability with TADA, this investigation did not include cases in which withholding future life-sustaining treatment was the topic of litigation. There is no reason why a specialist review committee could not also review the futility of future life-sustaining treatment. It is however foreseeable that the health status of some children will evolve and questions will arise whether the case should be reviewed again. Currently, in such cases both the parents and NHS Trusts can apply to the court for a review and it deserves consideration whether parents should also be able to apply to the specialist review committee.
The focus of this investigation is the effects of a replacement of the current court procedure by a specialist review committee procedure. How such a specialist review committee should be implemented in England & Wales is outside the scope of this article albeit that it is recognised that an important challenge will be to prevent the courts from scrutinising their decisions. I refer to others for a proposal how a national specialist review committee might fit into the legal landscape in England & Wales. 98
In summary, this investigation shows that replacing the courts in England & Wales in conflicts between clinicians and parents about the withdrawal of life-sustaining treatment with a specialist review committee modelled after TADA would limit court involvement to cases in which no one holds sufficient parental authority for the decision, when parents disagree amongst themselves and where there are child protection concerns. Compared to the 37 reported cases between January 1990 and December 2023, implementation of a national specialist review committee would have reduced the number of cases heard in court to just 7. f
Conclusion
Installation of a national specialist review committee with the power to decide whether continuing life-sustaining treatment for a particular child is appropriate can be expected to reduce the number of cases reaching the courts in England & Wales to just a handful.
Referral to a national specialist review committee rather than the courts would have several advantages for all participants. An advantage for clinicians and their Trusts is that the procedures can be expected to be shorter and less costly. Moreover, the review can be expected to be more private, so that there may be less exposure to negative content in the press and on social media. For the parents the main advantage would be that they are provided with an opportunity to transfer their child to a different healthcare provider when agreement cannot be reached. A disadvantage for clinicians may be that a specialist committee may decide more often that life-sustaining treatment should be continued, a disadvantage for parents may be that they will not be able to secure an alternative healthcare provider willing to take over the care for their child. However, given its advantages the installation of a national review committee as a way to avoid lengthy and costly court procedures deserves to be further investigated.
Supplemental Material
sj-docx-1-cet-10.1177_14777509241289742 - Supplemental material for Limiting court involvement in end-of-life treatment decisions for children in England & Wales: Advantages and limitations of a specialist committee deciding on futility
Supplemental material, sj-docx-1-cet-10.1177_14777509241289742 for Limiting court involvement in end-of-life treatment decisions for children in England & Wales: Advantages and limitations of a specialist committee deciding on futility by Veronica ME Neefjes in Clinical Ethics
Footnotes
Acknowledgements
The author would like to thank Nicola Glover-Thomas, Søren Holm and the anonymous reviewer for their helpful comments on earlier versions of this paper.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.