
Abstract
Medically unnecessary penile circumcision (MUPC) performed on a non-consenting child has been the subject of increasing critical attention in recent years. This paper provides a behind-the-scenes narrative of the politics of ethical policymaking in the United Kingdom in this area including a discussion about some potential barriers to reform. After a brief overview of ethical guidance for medically unnecessary surgical procedures on children in general and on their genitalia in particular, the paper takes a closer look at three contemporary documents released by UK medical bodies and highlights the unique ethical and safeguarding contradictions in this area. The outcomes of initiatives aimed at engaging constructively with the medical bodies and encouraging wider debate are then described, along with some of the main obstacles to engagement and counter-arguments employed. MUPC is subsequently discussed in a wider societal context, highlighting why serious safeguarding concerns have been raised about what many people believe to be a harmful, preventable practice hiding ‘in plain sight’. The paper ends by calling for UK MUPC guidance to be made consistent with the body of guidance that UK doctors are expected to follow.
Introduction
When it is permissible for doctors to perform medically unnecessary a surgeries on young children at the behest of their parents is a challenging issue. As ongoing debates about infant or new-born penile circumcision, or the appropriate standard of care for children born with intersex traits, for example, illustrates, it is one with which medical societies—and societies at large—are increasingly grappling. 2 More and more, it is recognised that ethical principles and policies regarding especially sensitive surgeries, such as those affecting the genital or sexual anatomy, must be shaped through a process of engagement with relevant stakeholders, including affected persons.
I am a medical doctor who has written and spoken publicly about medically unnecessary penile circumcision (MUPC), b at times drawing on my own experience, having been born and raised within a Jewish family and community where MUPC is widely practised. On the 14 March 2018, I was contacted by a member of the British Medical Association (BMA) ethics committee to provide feedback on a confidential draft of their forthcoming guidelines on MUPC, that is, the removal of the penile prepuce or foreskin in the absence of a pressing medical indication (e.g. to prevent or resolve a serious threat to well-being due to a problematic medical condition). These guidelines have since been published as the ‘NTMC (Non-therapeutic Male Circumcision) toolkit’ 3 released on 14 February 2019.
The toolkit was developed during a period in which MUPC had been drawing increased critical attention from various quarters. For example, the Parliamentary Assembly of the Council of Europe, 4 all the Nordic children's ombudspersons 5 and the combined medical professional bodies of the Netherlands 6 have expressed a variety of concerns in recent years. They argue that MUPC violates boys’ physical integrity rights and risks a range of harmful effects with negligible, if any, net medical benefits when accounting for non-surgical modes of treatment and prevention. The UN Committee on the Rights of the Child has expressed ‘concern about reported short and long-term complications arising from some traditional male circumcision practices’ under the heading ‘Harmful practices’. 7 And in 2019, a large coalition of more than 90 scholars working in law, medical ethics, and related fields published a consensus statement finding that the non-voluntary surgical modification of any person's sexual anatomy is ethically impermissible unless the person is incapable of consenting and the surgery is medically necessary (as defined in the first note). 1
Nevertheless, MUPC of children is still commonly performed—often, but not always, by licensed medical professionals—and many healthcare organisations have been reluctant to pursue substantive reforms. This paper provides a behind-the-scenes narrative of some of the politics of ethical policymaking as they pertain to this controversial subject in the United Kingdom. My aim in doing so is to shed light on the processes of institutional change relating to MUPC from a qualitative, first-person perspective. c By so doing, I hope to help shift policymaking in this area towards a more coherent and consistent application of accepted ethical and Human Rights principles.
In the UK context, MUPC is often characterised as a religious or cultural practice, 11 being predominantly performed on children born into Muslim, Jewish and diasporic North African communities. It is widely acknowledged that communities have a general right to practise their religious or cultural traditions without any undue interference. However, it is equally acknowledged that religious and cultural rights are not entirely unfettered, being limited in the case of practices or actions that infringe upon the rights of others. In line with this, there is growing concern that MUPC represents a breach of a child's human right to physical integrity which undermines his future choice about a psychosexually important part of his body (including choices about whether to have that body part marked with a permanent sign of particular religious beliefs, metaphysical commitments, or identity-related concerns he may not grow up to share).12,13
Contrary to a common misconception, a considerable body of men report feeling harmed 14 by having been circumcised as a healthy child without a medical problem. This feeling of harm may be related to specific surgical risks having manifested for particular men; or it may be due to a sense of body-integrity loss associated with the discovery that one's putatively ‘private’ anatomy was previously modified without one's consent. Specific risks 15 include meatal stenosis, urethro-cutaneous fistula and glanular amputation. Reported psychological harms16–18 include anger, shame, a sense of having been victimised and violated, fear, distrust and grief. Those who have voiced expressions of harm may lack organised representation whether or not they remain within their birth community. Nevertheless, the many thousands of individuals actively engaged in attempted ‘foreskin restoration’ techniques would indicate a significant level of dissatisfaction19,20 amongst circumcised adult males.
Claims of net medical benefit as a reason to perform MUPC in the new-born or early-childhood period have not had wide uptake outside of the United States. d Even in the United States, where routine infant circumcision has been a cultural norm for decades, the medical bodies stop short of active recommendation. 8 Yet even where claims of medical benefit are sometimes made, there are no mainstream scholars or organisations that make the stronger claim that penile circumcision—in physically healthy children—is medically necessary, regardless of the definition used. e Given this, I will show that current MUPC guidance and regulation conflicts with widely accepted medical-ethical principles that are applied in analogous cases.
In particular, I will demonstrate this ethical conflict by examining in more detail the guidance produced by two UK doctors’ organisations. The GMC is the UK medical regulatory and licensing body, and the BMA is the main UK doctors’ professional organisation and trade union. Both organisations produce wide-ranging and detailed guidance documents for doctors. I will argue that GMC and BMA guidance relating to MUPC is anomalous. I will support this by taking a closer look at three contemporary documents,3,24,25 two of which have been generated by the GMC, and one by the BMA. I will highlight the unique ethical and safeguarding contradictions in this area, illustrating how some of the guiding principles are subverted, and moreover how different sections of their guidance become contradictory on this one issue. I will demonstrate that GMC and BMA guidance on patients’ rights to autonomy, on safeguarding principles, on maximising the future choices of patients without capacity, and on respect for patients’ bodily integrity conflicts with GMC and BMA guidance on MUPC.
After a discussion of relevant guidance documents, there follows a description of some initiatives in which I and others have been engaged aiming to encourage wider debate on the ethics of MUPC within these bodies, along with a frank analysis of some of the main apparent obstacles to these initiatives’ success. The paper ends by discussing the MUPC guidance produced by these medical organisations in the wider societal context.
Earlier papers and work have evaluated the institutional processes behind policymaking in this area from a first-person ethnographic perspective, although often with different foci. These have included studies of global health policy decision making 26 concerning adult, ‘Voluntary Medical Male Circumcision’ for HIV prevention in Africa; research and policymaking surrounding female genital cutting27,28; and perceived difficulties in drawing up consensus guidance on MUPC. 29 By contrast, my focus will be on the process of engagement with relevant UK medical organisations in a re-examination of MUPC in the context of current guidance and ethical norms.
Ethical guidance for medically unnecessary surgical procedures on children
The introductory section described how increasing concern is being expressed about the impact of MUPC on children's rights and that claims for net medical benefit are not widely accepted by relevant health authorities. Yet as noted, not even the strongest advocates of MUPC argue that it is medically necessary, whatever health benefits may be claimed for the procedure. Thus, guidance and regulation for MUPC would need to be consistent with the general body of ethical guidance for medically unnecessary surgical procedures on children.
In this section, I will describe the general ethical guidance for medically unnecessary surgical procedures on children and specific guidance regarding medically unnecessary genital surgery on children. In the next section, I will show how guidance from both the GMC and the BMA regarding MUPC is inconsistent with the principles described here.
In the context of medically unnecessary procedures, the GMC has produced guidance for doctors who offer cosmetic f interventions. 30
The focus of paragraphs 32 to 35 of this guidance is on: ‘Treating Children and Young People’. In this section, the GMC advises doctors that:
- ‘[they] must
g
only provide interventions that are in the best interests of the child or young person’; - ‘a parent can consent to an intervention for a child or young person who does not have the capacity to make the decision, but [doctors] should involve the child in the decision as much as possible’; - ‘if [doctors] judge that the child does not want to have the cosmetic intervention, then [they] must not perform it’.
There are some more general principles in the main body of the GMC guidance on cosmetic procedures. Doctors are advised:
- ‘to discuss the procedure directly with the patient to seek their consent’.
And that they must:
- ‘make sure patients are given enough time and information before they decide whether to have an intervention’; - ‘take particular care when considering requests for intervention on children and young people’; - ‘consider [the patient's] vulnerabilities and psychological needs. [They] must satisfy [themselves] that the patient's request for the intervention is voluntary’.
To the best of my knowledge, there is no overarching body of ethical advice relating to medically unnecessary genital surgery on children. Instead, there is sex-specific guidance which largely concerns labiaplasty and circumcision.
Via its website, the NHS provides advice to the public about a variety of health conditions. Regarding labiaplasty, the NHS 31 states that ‘it should not be done on girls younger than 18’. The reason given is ‘because the labia continues to develop beyond puberty and into adulthood’. Regarding circumcision in boys, the NHS 32 states that ‘it is a relatively simple procedure’, and that ‘it is rare for circumcision to be recommended for medical reasons in boys’. There is no indication given that there may be similar concerns about the future growth and development of a male child's genitalia as those described above for children with female genitalia.
The British Society for Paediatric and Adolescent Gynaecology published a position statement 33 about labiaplasty in October 2013 in response to ‘concerns over evidence that such surgery is being performed on girls under 18 years of age’. The statement concluded that ‘labiaplasty does not tackle the cultural and economic factors that are giving rise to vulval appearance distress. There is no scientific evidence to support the practice of labiaplasty and, for girls under the age of 18 years, the risk of harm is even more significant’. And a recent review 34 of cosmetic labiaplasty on minors recommended that: ‘Postponing labiaplasty until adulthood is strongly recommended to help adolescents achieve a well-informed decision regarding an irreversible procedure with possible adverse esthetic and functional outcomes’.
In contrast to medically unnecessary surgical procedures on children, let us now consider a child who has not yet attained the capacity to give his own consent and whose doctors are recommending a medically necessary surgical intervention, such as surgery for suspected testicular torsion which is time-sensitive. In this case, his parents or guardians are given licence to give proxy consent to the recommended treatment on the basis that it is in the child's best interests to do so, because a delay in treatment would most likely cause significant harm that could not reasonably be avoided by less risky measures. In the absence of such qualifying conditions, should anyone—including a child's parents or guardians—seek to breach a child's bodily integrity (i.e. without medical necessity), safeguarding principles apply.
An illustrative model for evaluating the permissibility of genital interventions (e.g. in a medical context), including palpation, cutting or surgery. Figure and abridged text reproduced with permission from Earp BD, Abdulcadir J, Liao L-M. Child genital cutting and surgery across cultures, sex, and gender. Part 2: assessing consent and medical necessity in “endosex” modifications. Int J Impot Res 2023; s41443-023-00698–1.
An illustrative model for evaluating the permissibility of genital interventions (e.g. in a medical context), including palpation, cutting or surgery. Figure and abridged text reproduced with permission from Earp BD, Abdulcadir J, Liao L-M. Child genital cutting and surgery across cultures, sex, and gender. Part 2: assessing consent and medical necessity in “endosex” modifications. Int J Impot Res 2023; s41443-023-00698–1.
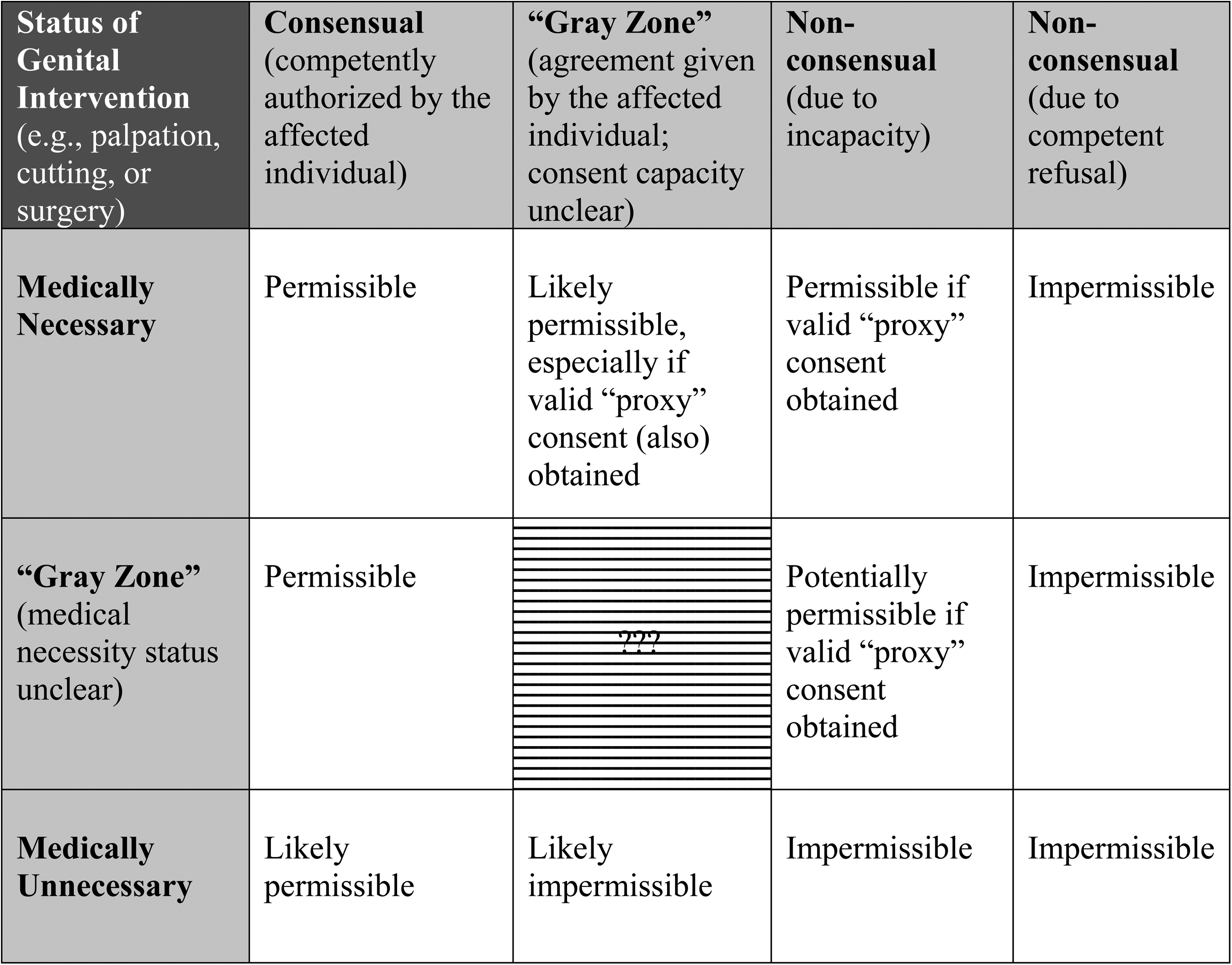
This is not only to protect the child from immediate bodily harm, but also to preserve his future right to make important choices for himself regarding meaningful interventions on his own body once he has gained the capacity to do so (see Box 1 for an illustrative model for evaluating the permissibility of genital interventions). 27
Doctors are required to take steps to protect their patients from avoidable harm. On standard accounts of harm, medically unnecessary damage to, or loss of, healthy, functional tissue is a paradigmatic example. h It might initially seem self-evident therefore, that doctors would take active steps to prevent MUPC, just as they would strive to prevent any other physically invasive, irreversible surgical procedure performed without medical necessity on the body of someone who is unable to consent. This is all the more so given that, in this case, the body part affected is widely seen as being exceptionally personal or private.
Therefore, the apparent inconsistency of MUPC with general ethical and safeguarding principles and guidance for UK doctors and with specific guidance regarding children with biologically female genitalia needs further explanation, particularly as MUPC is widely tolerated and even performed in some cases by UK doctors.
In what follows, I examine how the UK medical community finds ways to tolerate, defend, and even perform a practice that seems to be in tension with its own core ethical principles, and also why medical professionals might choose to do so.
To tease out this apparent contradiction, I will first discuss how recent updated GMC guidance on decision making and consent 24 relates to current guidance on Personal Beliefs and Medical Practice. 25 I will then address the 2019 ‘NTMC toolkit’ 3 produced as a practical guide for doctors by the BMA. In doing so, I will draw from the main findings of a recent paper critiquing the BMA guidance in some detail. 36 I will then explore some potential sociological reasons why this anomalous situation persists.
Recent professional and regulatory guidance
The previous section discussed ethical guidance for medically unnecessary surgical procedures on children in general. For medically unnecessary surgical procedures on children's genitalia, ethical advice differs according to the biological sex of the child. This is the case even though some of the ethical principles described are universal. In this section, I take a closer look at the three aforementioned recent documents and will show why the permissive approach to MUPC appears to contradict doctors’ core ethical principles. These documents are the GMC's 2020 Decision-making and Consent Guidance, 24 the 2013 Personal Beliefs and Medical Practice guidance 25 and the 2019 BMA NTMC toolkit. 3 I will show that the specific guidance on MUPC from both the GMC and the BMA conflicts in several key areas with more general principles and guidance. In the subsequent section, I will describe efforts that I and others have made to engage the two organisations in addressing this conflict, before discussing some possible reasons as to why these attempts have so far proved unsuccessful. I now turn to the three sets of guidance:
In January 2019, I prepared the response 37 from the (UK) National Secular Society i (NSS) to the GMC consultation on the draft consent guidance. 24 This GMC guidance has since been published as ‘Decision Making and Consent’, 24 which came into effect on 20 November 2020. The final version was not substantially different from the draft. The GMC decision-making and consent guidance does not specifically address MUPC; instead, it articulates some general principles intended to cover all branches of medical practice. I will illustrate how some of the guiding principles in this document and in other current GMC guidance documents appear to conflict with GMC guidance on MUPC.
The NSS consultation response commended the GMC decision-making and consent guidance together with the detailed explanatory notes. We supported the emphasis on patient involvement, including the importance of giving patients time to reflect and the need for doctors to be alert to the vulnerable or to a patient under duress or pressure from relatives or carers.
For patients lacking capacity, doctors must take the action, ‘least restrictive of the patient's rights and freedoms including their future choices’ and plan for foreseeable changes in capacity. Also, that ‘if [doctors] don’t have consent or other valid authority on which to carry out a particular intervention, [doctors] must not proceed with it” except in an emergency.
The GMC decision-making and consent guidance is consistent with the GMC's core guidance—Good Medical Practice
38
—which advises registered doctors that they must:
- ‘Make the care of [their] patients [their] first concern’; - ‘Prescribe drugs or treatment … only when… satisfied that this serves the patient's needs’; - ‘Provide effective treatments based on the best available evidence’. - ‘Respect [their] patients’ views about health’; - ‘Ensure that decisions are both informed and voluntary’; - ‘Be aware of other situations in which patients may be particularly vulnerable or susceptible to pressure’.
The updated guidance begins: ‘Shared decision-making and consent are fundamental to good medical practice’. Doctors are required to:
GMC child protection guidance published in 2012 acknowledged the challenges of balancing parental religious freedom with child welfare, stating: ‘In some cases, it may be difficult to identify where parents’ freedom to bring up their children in line with their religious and cultural practices or beliefs becomes a cause for concern about a child's physical or emotional well-being’.
39
This is because, when treating children, a doctor's primary duty of care remains to the patient. According to the GMC,
40
doctors ‘should involve children and young people as much as possible in decisions about their care, even when they are not able to make decisions on their own’.
We can see therefore, that the GMC ordinarily works diligently to support patient autonomy and to protect the rights of children and vulnerable people. Where necessary, the GMC recommends protecting patients even from those most close to them. The GMC, moreover, supports patient autonomy which includes the rights of children to be involved in their own care as much as possible.
Recognising the GMC's detailed attention both to empowering and protecting adults and children, an irreversible traditional surgical practice performed on a child appears to represent a major departure from the usual caution exercised when considering a medical intervention on a child.
The NSS consultation response alerted the GMC to the contradictions between the (then) draft guidance on consent and existing advice to doctors relating to MUPC. Nevertheless, the updated decision-making and consent guidance has failed to resolve these contradictions, elaborated on below.
GMC guidance on ‘personal beliefs and medical practice’, paragraphs 18–23 ‘procedures provided for mainly religious or cultural reasons’
A section on ‘Procedures provided for mainly religious or cultural reasons’ might be expected to focus on culturally or religiously informed choices that competent adults might make with regard to medical procedures that affect themselves.
25
Instead, the section begins: “If patients (or those with parental responsibility for them) ask for a procedure, such as circumcision of male children, for mainly religious or cultural reasons…”
Immediately, it can be seen that the GMC here conflates adult requests for medically unnecessary procedures for themselves, with requests by adults for medically unnecessary procedures on children. Considering the absence of comparable examples, and the care taken to develop GMC guidance, the specific focus of this section on MUPC rather than on wider religious concerns appears to be intentional.
After some standard general advice, the section continues: ‘If the patient is a child, you must proceed on the basis of the best interests of the child and with consent’. How, then, are doctors guided as to the child's best interests? ‘This will include the child's and/or the parents’ cultural, religious or other beliefs and values’.
In other words, when considering MUPC, which is almost exclusively performed on pre-consenting children in the United Kingdom, j doctors are encouraged to substitute parental beliefs as a proxy for the child's presumed later beliefs. However, the presumption of consistency of religious belief between parents and children is increasingly problematic. According to the Pew Foundation, 43 the percentage of non-religious Jews is higher in the younger age groups with 40% of male and female Jews aged 18 to 29 (the youngest cohort quoted) being non-religious.
Although these figures are for the United States, broadly the same picture is likely to apply in the United Kingdom where non-belief is now the majority religious/belief position. 44 It seems likely from the statistics given and the documented trends in UK religious belief that at least 40% of male children born to Jewish parents will be non-religious as adults. Moreover, when considering MUPC for an individual child, it is not possible to know whether that child, as an adult, will be pleased, distressed or indifferent to the MUPC performed on them as an infant. This remains true whether or not they subsequently consider themself to be religious.
Such an approach by the GMC, particularly when considering a medically unnecessary, irreversible operation on a pre-consenting patient's sexual anatomy seems to be in tension with the responsibility on doctors to protect the most vulnerable of patients, and to facilitate patients’ own decision making wherever possible, as elucidated elsewhere by the GMC.
The guidance then states: ‘You should get the child's consent if they have the maturity and understanding to give it’. This statement is consistent with existing GMC guidance on maximising patient autonomy and respecting the rights of children to be involved in decisions about their own care. In the case of a child lacking sufficient maturity and understanding to consent to surgery, however, we have a particularly vulnerable person with temporary incapacity from whom consent can only be obtained by waiting. Given that MUPC is by definition not medically urgent, a recommendation to wait, then, seems the most logical conclusion for a medical guidance to draw.
Instead, the passage continues: ‘If not, you should get consent from all those with parental responsibility’. This seems to prioritise the parents’ sense of religious or cultural urgency over the safeguarding principle that children should be protected from significant intrusions into their bodily integrity – particularly regarding permanent changes to the anatomy of their sexual organs – unless there is a pressing medical indication. Yet, as we have seen, 39 the GMC elsewhere acknowledges that parental freedom to practise their religious and cultural practices may adversely affect a child's physical or emotional well-being. And when parents have disagreed about MUPC, the English courts have ruled in all recent cases 45 that it is in the best interests of a child to defer circumcision until he gains capacity to decide for himself. These legal rulings have not been based solely on the fact of parental disagreement but also on the basis that the child's future beliefs and values are unknowable at such an early age. The legal annexe to this section of GMC guidance was last updated on 7 April 2020 but surprisingly does not include a discussion about these recent rulings.
Therefore, far from mitigating the concern, reducing the advice about a child's best interests to an agreement from ‘all those with parental responsibility’ removes any counterbalance, particularly when the parents themselves may pose a risk to the child's best interests, for the reasons set out below.
Since there is no medically necessary reason to perform MUPC, and since in the vast majority of cases, the child will be too young to express an opinion, doctors following this guidance must necessarily rely on parental arguments that it would be in the best interests of their son to undergo MUPC. Parents with the strongest beliefs are likely more able to persuade a doctor that cutting the child's penis would be in his overall best interests. Thus, younger children, who are born into communities with the strongest beliefs, and whose parents agree with traditional genital cutting practices, seem least likely to be considered in a safeguarding context, when the reverse should be the case.
The final paragraph of this section reiterates the selective focus by the GMC on MUPC. Doctors are instructed to offer parents the opportunity to ‘invite their religious adviser to be present during the [religious circumcision] procedure’. In the absence of any associated discussion of possible child safeguarding considerations, this overtly permissive advice (on MUPC) appears to be in conflict with the official GMC position that it has no ethical position on MUPC.
The 2019 BMA toolkit on NTMC
The subsequent section of this paper examines how this new guidance was produced and what evidence was made available to the BMA to inform the update. 3 Criticisms of the toolkit are summarised below with reference to a more detailed critique contained within a paper I co-authored published in 2022. 36
In our paper, we found the BMA's claim to ethical neutrality regarding MUPC to be misleading. This was because the BMA's guidance, which we consider to be ambiguous and at times contradictory leads to a ‘de facto permissive stance towards the practice underwritten by a perplexing analysis of the child's best interests’. 36
The phrase “best interests” appears over 50 times in the BMA toolkit which states that ‘Doctors must act in a child's best interests’ and that ‘parental preference alone does not constitute sufficient grounds for performing [MUPC] on a child unable to express his own view’. Yet the balancing test recommended by the BMA guidelines to assess a child's best interests in this matter, pits child-centred factors against parental factors. Parental factors regarding MUPC will inevitably relate to the cultural or religious preferences of a child's family. The result is that ‘parental preference alone will have sufficient force to neutralise all other child-centred items on the list’. The BMA's best interests test – a test, moreover, which underpins its whole guidance – is ‘therefore incoherent’. 36
The BMA toolkit states that it is primarily intended to offer ‘practical advice to doctors’ and to highlight some of the debates to illustrate the diversity of views. It asserts that ‘FGM is a wholly separate issue’. This claim is made despite abundant evidence to the contrary (e.g. all known cultural communities that practise FGM also practise MUPC, often for similar reasons, and depending on the community, either the male or female form of cutting may be more physically severe), 46 some of which was referenced in the toolkit itself. The BMA toolkit's MUPC advice therefore demonstrates unjustified sex discrimination.
The 2006 BMA policy document on male circumcision 47 addressed both MUPC and medically necessary circumcision. Regarding the latter, the BMA adopted a coherent standard in line with conventional medical ethics. In our communications with the BMA during the process of policy review, which is discussed later, my colleagues and I endorsed the reasoning in this section; we also highlighted an ethical contradiction. The contradiction is that for someone who has a medical problem but does not absolutely need circumcision to fix it, circumcision would be unethical as it is unnecessarily invasive. Whereas, in the case of a healthy child who has no need for any treatment or surgical intervention, the BMA ‘takes no ethical position’ and is therefore, in effect, recommending less protection.
The 2019 BMA NTMC toolkit introduced two changes (in italics below) into the section on medically necessary circumcision. The BMA continues to regard as unethical, circumcision solely for medically necessary reasons where less invasive approaches are available. However, when a parent desire[s] this (solely medically necessary) surgery for social and cultural reasons the BMA no longer regards this as necessarily unethical. For doctors seeking guidance from the toolkit, interpretation of this section may be difficult if not impossible.
The BMA guidelines assert that: ‘Male infant circumcision does not require a medical professional’. k Here, not only are the usual requirements for safe surgical care omitted, the usual safeguarding concerns are considered neither relevant nor necessary.
The BMA had been made aware of the serious, sometimes life-threatening complications from infant circumcision, occasionally reported in the UK media some of which have only come to light through freedom of information requests. 48 Yet the word ‘safeguarding’ appears only once in the BMA toolkit, specifically in the context of FGM. Doctors unwilling to perform MUPC are instead advised that they may need to conscientiously object.
Engagement with the medical profession
I have argued that current GMC and BMA guidance on MUPC is uniquely discordant with the main body of medical guidance that UK doctors must follow in order to maintain their licence to practice. I have also shown that some of the MUPC guidance is misleading, confusing and fails adequately to address safeguarding concerns. Described below are some of the actions taken to engage the UK medical establishment in addressing the ethical and safeguarding contradictions outlined above with the current permissive attitude to MUPC.
GMC engagement
In 2009, the GMC position on MUPC was: ‘We do not have a position’. But for this statement, the body of GMC guidance in force at that time might reasonably have included MUPC. In fact, but for this statement, any medically unnecessary surgical operation on the genitals of a child would have fallen foul of GMC guidance. Therefore, rather than being a neutral position, this statement can instead be seen to guide doctors to grant exceptional status to MUPC, in effect to be insulated from the rest of GMC guidance. In January 2010, my request for a meeting with the GMC ethics department was granted. A summary of the discussion has previously been published. 49
Drawing on GMC guidance in other relevant areas, I suggested that the GMC would not otherwise condone any form of childhood ritual genital cutting, ordinarily regarded as an assault and battery. 50 I proposed that the GMC remove the six words – ‘We do not have a position’. In so doing they would have reversed the active and singular exclusion of young boys from existing GMC principles and safeguards. Absent these words, doctors would necessarily be guided to treat MUPC as they would any other comparable intervention on children.
Although my interlocutor was sympathetic to the arguments I presented, any suggestion that the exceptional clause should be removed was rejected. The primary reason given, astonishing as it was from a regulatory body with a primary remit to protect patients, was repeated verbatim to colleagues a few years later. We were told: ‘You have no idea how offended the chief rabbi would be…’ were the GMC to change its guidance.
This appears to illustrate GMC priorities in this one area. Ordinarily, the primary focus is on patient autonomy, child safeguarding and maximising future choices. Instead, in the exceptional case of MUPC, the GMC indicated that it had different priorities. The implications for patient care of the GMC's stated preoccupation with the beliefs of parents and the feelings of religious leaders in the context of child safeguarding was a cause for concern.
Consultation responses from the Secular Medical Forum l and the NSS have regularly drawn attention to the incompatibility of the GMC's guidance on MUPC with the rest of its ethical advice. m
Council for Healthcare Regulatory Excellence
I wrote to the Council for Healthcare Regulatory Excellence (CHRE) in 2010 requesting an investigation into the GMC's adherence to its statutory remit of protecting patients. Since the GMC had followed correct ‘procedure’ in drawing up its guidance, the CHRE declared the substantive guidance outside its remit.
During my meeting with the GMC, however, I developed a greater appreciation of the relationship between the GMC and the BMA. The BMA is member-led with a strong professional ethic. Every year, five to six hundred BMA representatives meet, usually over several days, for the Annual Representatives Meeting (ARM). Following democratic debate on motions submitted by members via various BMA divisions, the result of an ARM vote becomes BMA policy.
Politicians and the GMC frequently refer and defer to BMA policy on medical topics. This is despite the BMA having no statutory power (and the oversight that would come in its wake.) During my 2010 meeting with the GMC, the previously referred to BMA's ‘The Law and Ethics of Male Circumcision’ 47 was cited as an authority several times.
BMA engagement
As a BMA representative since 2009, I have attended 15 consecutive ARMs.
Every year since 2010, my local BMA division has submitted a motion to include MUPC for consideration by the BMA's Agenda Committee to be debated at the ARM. In this way, BMA representatives might hear the GMC and the BMA's own arguments about consent, child safeguarding and maximising future choices in this context and would be afforded the opportunity to debate and ultimately to form BMA policy.
None of these motions have been selected for debate. Consequently, despite the BMA's acknowledgement that it is a ‘controversial’ topic, and the fact that a new BMA ‘toolkit’ has been produced in this time, MUPC has not been debated by the BMA's representative body for at least 20 years.
Five motions from the supplementary (motions not selected) agenda with the most representatives’ votes will also be debated. I have informally encouraged fellow representatives to prioritise debate about medically unnecessary genital cutting of children, but this approach has not been successful.
In the absence of dedicated ARM debate on MUPC, it is sometimes necessary to raise this topic through relevant related motions.
Some motions are deemed by the Agenda Committee to be sufficiently non-contentious as to be passed without debate. Unless challenged, these motions will become BMA policy. In 2013, such a motion condemned all forms of FGM. Inevitably, this would have included the most minor forms, such as ritual nicking or pricking, that are less invasive than male circumcision. n Seeing every reason for the BMA to condemn all forms of genital mutilation without caveat, I submitted an amendment to remove the letter ‘F’ from the motion. I was subsequently informed that my controversial proposal had resulted in the fall of this motion, since no ARM time had been allocated for debate.
In 2014, a similar anti-FGM motion was on the main ARM agenda. I was one of two representatives called on 25 June 2014 to speak against this motion. 53 We both asked the BMA's representative body to reconsider a motion that would enshrine into BMA policy an endorsement of discrimination on the basis of sex with regard to the cutting of children's genitalia for no medical reason. In the absence of a specific debated motion to consider MUPC alone or to encompass all forms of medically unnecessary genital cutting of children – which might also include intersex surgery – BMA representatives voted unsurprisingly, in view of its existing illegality, to confirm BMA policy to be wholly against FGM only, thereby maintaining sex discrimination.
We remain the only two representatives to have spoken at the ARM on this subject since 2001. On 23 June 2015, I spoke in favour of a motion which called for ‘doctors to do more to protect all children from all forms of harm’ and ‘to work with communities to protect the children within them’.
Asking representatives to consider first the nature of harm to a child, and supporting BMA commitment to sex non-discrimination without caveat, I asked whether BMA representatives would support a boy who wanted to grow up with his genitals intact. I called on representatives to give their full support to the motion being debated.
Yet before the motion was put to vote, the medical ethics committee chair announced 54 to the meeting: ‘I would like you to disregard Dr Lempert's interesting comments’ – he was alleging that what I had said was not relevant to this motion. When I later asked him why he had spoken out in this way, he replied that some people hadn’t liked what I had said.
The BMA President has a 1-year advisory role. In 2015, the President-elect was the former Commissioner for Children in England, Professor Sir Al Aynsley-Green.
Shortly before his inauguration on 22 June 2015, I informally asked for his thoughts about MUPC in the context of his advocacy for ‘listening to children’. In his reply he alluded to the power of the United States (the only Western, developed country to perform circumcision on a majority of male new-borns for non-religious reasons) and the UK's ‘schizophrenic attitude’. He suggested that I write to him after the ARM which I did.
Some months later, in early 2016, and by way of reply to my letter, I was copied in to a letter from Professor Sir Al Aynsley-Green, by then BMA President. In his letter to the BMA executive, he recommended a policy review of MUPC involving a range of key stakeholders. He wrote that ‘it would not’, in his view, ‘be proper for the Ethics Committee to be involved without the support of BMA members’. He further specified that the issue needed to be handled professionally with transparency, sensitivity and impartiality.
In 2019, the updated MUPC toolkit was issued by the Medical Ethics secretariat without member or representative engagement and without any transparency of process. Since publication of the toolkit, the annual MUPC motions submitted by my BMA division have also been rejected by the agenda committee.
I have regularly had discussions and correspondence with members of the BMA Medical Ethics Committee. In response to my correspondence, the committee chair and ethical advisors assert that BMA policy on MUPC – as on other topics – is made by BMA representatives at the ARM. Contradicting this assertion, the 2019 BMA NTMC toolkit has been published without any involvement of the representative body. o
In 2016, near the beginning of the BMA's revision process of its MUPC guidance, I was invited to a private meeting with the chair and secretariat of the Medical Ethics Committee. With their agreement I was joined by three colleagues – one Jewish – and each an expert on MUPC in their respective fields of medical ethics, law and political science. We have respected the BMA's request not to share details of the meeting. We do not know who else was invited to meet with the BMA during the course of the toolkit preparation.
By invitation, we submitted to the BMA in advance of the meeting a joint, detailed comment on their 2006 guidance with clear recommendations to bring BMA policy into line with current law, ethics, and good medical practice.
At their request, we provided the BMA with further evidence over the following months.
In 2018, we each submitted a response to the draft BMA ‘NTMC toolkit’ which had been shared with us confidentially by the Medical Ethics Committee asking for comment and feedback.
Yet, as detailed above, our recommendations to align BMA policy in this area with existing ethical principles in a coherent and consistent manner were not reflected in the final document. We subsequently co-authored the paper 36 referenced above which used the NTMC toolkit as an exemplar of the current contradictions in law, medical ethics and child safeguarding faced by institutions seeking to draw up guidelines in this area. We detail in the paper how the BMA's NTMC toolkit lacks ethical coherence.
MUPC: A safeguarding concern hidden in plain sight
The GMC and the BMA both advise that doctors act according to a child's best interests with regard to MUPC. Both organisations are seen to place significant weight on making that assessment conditional on sincere adult parental belief. It seems appropriate, therefore, to explore what lies behind those beliefs. Although MUPC is also a Muslim religious rite and performed on some children from the North African diaspora, I will focus here on Jewish beliefs in light of the GMC's repeated comments about the chief rabbi.
The presentation on which this paper is based was first given in April 2019 at the ‘Future Choices’ conference, 55 held at the Faculty of Healthcare Law in Leeds University. As a teenager from the Leeds Jewish community, I studied Judaism and Hebrew, attaining an A level in Classical Hebrew. I consider myself neither religiously nor culturally Jewish, despite the fact that Jewish authorities consider to be Jewish a child born to a Jewish mother (as I myself was), regardless of that person's later beliefs.
Beyond the eponymous Ten Commandments, there are 613 Jewish Mitzvoth, or commandments. Many modern Jewish authorities do not regard them as absolute. Roughly only a third of these commandments are still kept in their original form; for example, prohibitions on the taking of revenge or wronging people in speech. Some commandments remain religiously controversial, such as the prohibition on a man having sexual relations with a man.
Other commandments are no longer accepted by most Jews. Modern society would not accept that a rapist should marry his unwed victim or that the seven Canaanite nations should be destroyed, leaving none to live.
Commandment number 86 decrees that a male child born to Jewish parents should be ‘circumcised on the eighth day of his life’. Nowadays, some Jews instead practise the peaceful, non-cutting Brit Shalom welcoming ceremony for boys and girls.56,57
Perhaps it is because the intention is benign, that MUPC is perceived as something other than harmful, even though it undoubtedly involves deliberate wounding of a child's genitals.
Episodic failures to protect children from significant harm have resulted in serious case reviews and public enquiries. One of the main themes to emerge about the lessons to be learned from such public enquiries is that children have been harmed when caregivers, or those responsible for their protection, have taken the focus off the child and onto other considerations.
In response to the national scandal of children being groomed by gangs of adult men and sexually exploited, the Greater Manchester police chief 58 apologised that the [child safeguarding failures] happened also in Manchester and ‘in plain sight’, yet was not recognised as abusive at the time. The #MeToo movement articulates the regular sexual abuse suffered by women, often in plain sight, and with insufficient action taken – especially against those perceived as powerful. The global Black Lives Matter movement similarly reflects longstanding widespread systemic discrimination. MUPC too is a practice that many people feel deeply harmed by, is entirely preventable, yet which continues to happen ‘in plain sight’.
Some of the reluctance of the UK medical establishment to challenge – or even to debate – MUPC appears to stem from a belief that it is a core religious rite, expressed on behalf of children by his parents. A commendable concern not to offend religious communities should not be a barrier to effective child safeguarding, as indeed it is not in the case of female genital cutting, which remains expressly prohibited regardless of religious justification found, as it is, within some sects of Islam. 59
Conclusion
This personal narrative demonstrates how the UK medical profession's position with regard to MUPC is unique among and in conflict with the rest of its guidance. Doctors are advised that the central premise when deciding how to treat a child must be the child's best interests. Yet for MUPC, the entire question of a child's best interests, as articulated by both the GMC and the BMA, is reduced to the strength or otherwise of parental beliefs. In contrast, very strong parental beliefs that may lead to the wounding of a child are ordinarily regarded as a serious safeguarding concern. Thus, for MUPC, the stronger the parental beliefs the less likely it is that the child will be safeguarded from genital wounding.
I have illustrated how some of the arguments presented by the GMC and the BMA lack coherence. I have further outlined some of the institutional and conceptual barriers faced when addressing the enduring inconsistencies in current medical professional guidance in this one area.
Both organisations concur in selectively directing doctors to depart from the usual medical guidance and safeguards which, if applied consistently and coherently, would otherwise render an invasive, medically unnecessary ritual cutting procedure on a child's genitals unethical. As this redirection actively facilitates a practice that would otherwise be prohibited, claims of neutrality by the GMC and the BMA do not appear credible.
In areas other than MUPC, it is accepted that children's fundamental rights are undermined when those rights become contingent on their parents’ values and beliefs. Yet, the surgical assignation of a child's healthy penis according to his parents’ beliefs, on the highly questionable assumption that he will later adopt those beliefs, is currently tolerated. MUPC is not consistent with a child's right to physical integrity, to form his own adult beliefs, nor is it consistent with guidance to maximise a child's future choices.
In this paper, I have described efforts to engage the UK medical profession constructively to reconsider its guidance in the light of the concerns raised. To date, these efforts have not been successful which is initially difficult to understand when considering the gravity of the safeguarding concerns regarding MUPC.
In trying to understand how recent guidance could have been written so as to except MUPC from the usual safeguards for effective child protection, it seems likely that significant weight has been given to the underlying paradigm of MUPC acceptability. The importance of MUPC to some religions (especially Judaism and Islam) appears to be given priority over manifest Human Rights objections. The barriers described in this paper, including the lack of transparency of process, the avoidance of open debate and the reluctance to challenge religious practice, appear to represent an institutional failure to recognise what many consider a serious safeguarding failure that endures ‘in plain sight’.
While it is not for the medical profession to debate theology or doctrine, it is, however, necessary for it to ensure the protection of all children and that no person and no organisation overrides the primary duty of doctors to care for their patient, to offer that person the treatment that they need and to protect them from unnecessary significant harm. Any undermining of accepted universal safeguarding principles of children just from certain communities is unjustifiably discriminatory.
With this paper, I hope to encourage the GMC, the BMA, regulatory authorities and child safeguarding boards to revisit current guidance on MUPC. Whether or not the GMC and the BMA move to a position similar to that in the Netherlands, Finland and Denmark and recommend that MUPC be discouraged, current guidance must be changed in order to be consistent with the body of GMC guidance that UK doctors are expected to follow. I urge them to make this process inclusive and transparent.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The author chairs the Secular Medical Forum of the National Secular Society, which works to safeguard patients from the harm caused to them by the imposition of other people's religious beliefs and practices on them. The author is a British Medical Association (BMA) representative but does not write in that capacity.
Funding
Funding for the article to be made available via Open Access was provided by the (UK) National Secular Society. The author received no other financial support for the research, authorship, and/or publication of this article.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.