
Abstract
Adolescent pregnancy results from the complex interaction between various internal and external vulnerabilities. These vulnerabilities persist after the infant's birth when the adolescent becomes a parent. Adolescent parents are unfairly stereotyped as unmotivated and incompetent. Some legislations prohibit adolescents from giving consent on the grounds of incompetency. Despite being different, “competency” is frequently used interchangeably with “capacity”; thus, incompetent individuals are often mistaken to lack capacity. Consequently, legally incompetent adolescents who became parents are frequently disregarded during their infant's decision-making process. This article discusses the distinction between the competence and capacity of adolescent parents, the various vulnerabilities that contribute to an adolescent's incompetency, and advocates respect for the adolescent's capacity in making decisions for her infant. We propose a workflow for obtaining informed consent for infants born to adolescents ethically guided by the respect for individuals principle while staying within the country's legal framework.
Introduction
The World Health Organisation (WHO) defined adolescents as individuals from 10 years to 19 years old.1,2 The adolescence period is said to be the second most dynamic events of human brain growth and development. This period is the transition between childhood and adulthood, which explores the issues of independence, identity, and sexuality. 3
Adolescent pregnancy is not uncommon. Based on the WHO, an estimated 21 million adolescent girls become pregnant every year in developing regions. 4 In Malaysia, the prevalence of adolescent pregnancy is 2.8%, but this figure is likely an underestimate as there are many unreported cases, particularly in less developed rural areas. 5 Adolescent pregnancies are frequently attributed to their excessive risk-taking behaviour and peer-influences on their evolving capacity.6,7 However, this attribution does not paint a complete picture, as adolescents are vulnerable to various external factors which are frequently beyond their control. For instance, lack of access to contraception, low education level and low socio-economic status are risk factors for adolescent pregnancy. 8 This list is not exhaustive, as an adolescent's predisposition to pregnancy is intricately related to other familial, cultural and social factors. 9 The interplay of these factors, which are often synergistic, can amplify the adolescent's vulnerability. This is reflected in a study from Malaysia, where a majority of adolescent pregnancies are from low-income urban families and are school drop-outs. 10 Additionally, most of the adolescents in the study turned to their peers and other unreliable resources for contraceptive information rather than referring to trustworthy sources, as contraception is a sensitive subject to be discussed in the society. 10 Although 63% of adolescent pregnancies in this study are reported to stem from consensual sexual activity, 10 the circumstances surrounding their consent were not explored. Thus, it remains uncertain whether these minors were deceived into sexual activity. This notion is reflected in this study, where a fifth of the respondents reported being coerced into sexual intercourse. 9 In short, adolescent pregnancy is a consequence of the vulnerability arising from a complex interaction between various personal and socio-cultural factors and not solely a result of their evolving mental capacity.
In Malaysia, adolescent pregnancy is taboo due to traditional and religious values prohibiting premarital sex.10,11 Adolescent mothers are frequently stigmatised, especially in a conservative society where having an illegitimate child is perceived as bringing shame to the family. There were cases where adolescent mothers get disowned by their own family, often leaving the adolescent mother with no choice but to abandon her infant. 11 Moreover, adolescent parents are stereotyped as unmotivated, irresponsible and incompetent in caring for their child. 12 Govender et al. reported that healthcare workers perceived that adolescent mothers are difficult and less receptive to advice, 13 although this rebellious behaviour exhibited by the adolescents may simply be a reaction to the discriminatory attitudes towards them. Such biased and negative perceptions and reactions could explain why adolescent mothers face discriminatory attitudes and disrespect in healthcare settings. 14 Furthermore, regulations in some countries seem to undermine the adolescent's capacity to decide. An example of this is that individuals below the age of majority (18 years old in Malaysia) are legally disqualified from giving informed consent for medical procedures. 1 From the utilitarian view, the ultimate aim that justifies this regulation is to protect the minor's right to sound decisions and perhaps to spare the minor from the task of making difficult decisions. However, the dilemma arises when medical consent is needed for the child of adolescent parents, in which both the child and parents are minors. Without a clear guide, practices differ from one centre to another even within the same country but in most instances, the adolescent is left out from the consent process. From our experience, the medical consent for children of adolescent mothers is frequently obtained not from the adolescent but from other adults related to the adolescent, like their parents. A state-appointed Child Protector may assume surrogacy if a legally-acceptable adult surrogate cannot be identified. Although this practice may lead to adolescent parents feeling left out, disrespected and discriminated, 14 it is common because the healthcare workers are obliged to work within the local regulatory framework.
This case illustrates the ethical conundrums of obtaining medical informed consent for an infant born to an adolescent. We discuss and propose an approach to navigate through these ethical challenges.
Case
A baby was born prematurely at 30 weeks of gestation to a 15-year-old mother at a specialist referral hospital in a developing country. Due to complications of prematurity, the baby was admitted to the neonatal intensive care unit (NICU) for respiratory and nutritional support. At 23 days of life, the baby became anaemic and required blood transfusion. As per standard protocol, informed consent for transfusion of blood products should be obtained. For minor patients, the parents normally give informed consent.
The mother has a complex social background. Besides being an adolescent parent, she has no documentation of citizenship and is under the care of her biological mother (the baby's maternal grandmother) who is a single parent herself. The adolescent and her 16-year-old sexual partner have no formal education, are illiterate, and unemployed. They planned to get married traditionally, which is permitted under the local customary law.
In this situation, the issue of who can act as a surrogate decision maker for the baby comes into question. As the baby's mother is a minor, she is not a legally competent surrogate for her child. Therefore, in practice, the maternal grandmother is the most suitable person to act as the legal surrogate for both the baby and the adolescent mother. However, although the adolescent and her mother appear to share a family bond, their relationship could not be verified due to absent documents, which is an important legal requirement. Thus, clinicians were in a dilemma regarding whom consent should be obtained.
Discussion
Our case illustrated several issues arising from informed consent for infants of adolescent parents. We present our arguments to respect a minor's capacity as a parent within a legal context where minors are considered incompetent.
Is an adolescent competent to make medical decisions for her infant?
Decision-making competence is the ability to follow normative rational principles in decision-making. 15 A competent decision-maker must be able to comprehend the issue at hand, understand the options available, identify alternatives, recognise and weigh the risks and benefits of each option, summarise the information and evaluate the outcome of a decision. 16 The recognition of the consequences of a decision, credibility of the information and correctness of choice are also important qualities of a competent and autonomous decision maker. 16
Individuals in Malaysia are legally allowed to give medical consent when they reach the age of majority, which is 18 years old.1,17 The justification is that minors are presumed to be legally incompetent. 18 In practice, the term “competence” is often used interchangeably with “capacity”.1,19 Consequently, it is often misconstrued that an incompetent individual also lacks capacity.
It is essential to understand that the two terms are related yet different. The simplified relationship between competence and capacity is illustrated in Figure 1. Competence refers to a legal concept that allows a person to provide an opinion or make an autonomous decision. 18 A decision is considered autonomous if the person has received sufficient information, has adequate capacity, and does so voluntarily. 20 On the other hand, capacity is an individual's psychological ability to understand information, reason and reflect on them to make a decision. 18 Thus, capacity, along with voluntariness, are components of an individual's autonomy which constitutes the individual's competency. A person's competence is determined by his capacity and voluntariness; a person can have full capacity yet be considered incompetent if his decisions are not voluntary due to coercion, exploitation or manipulation.
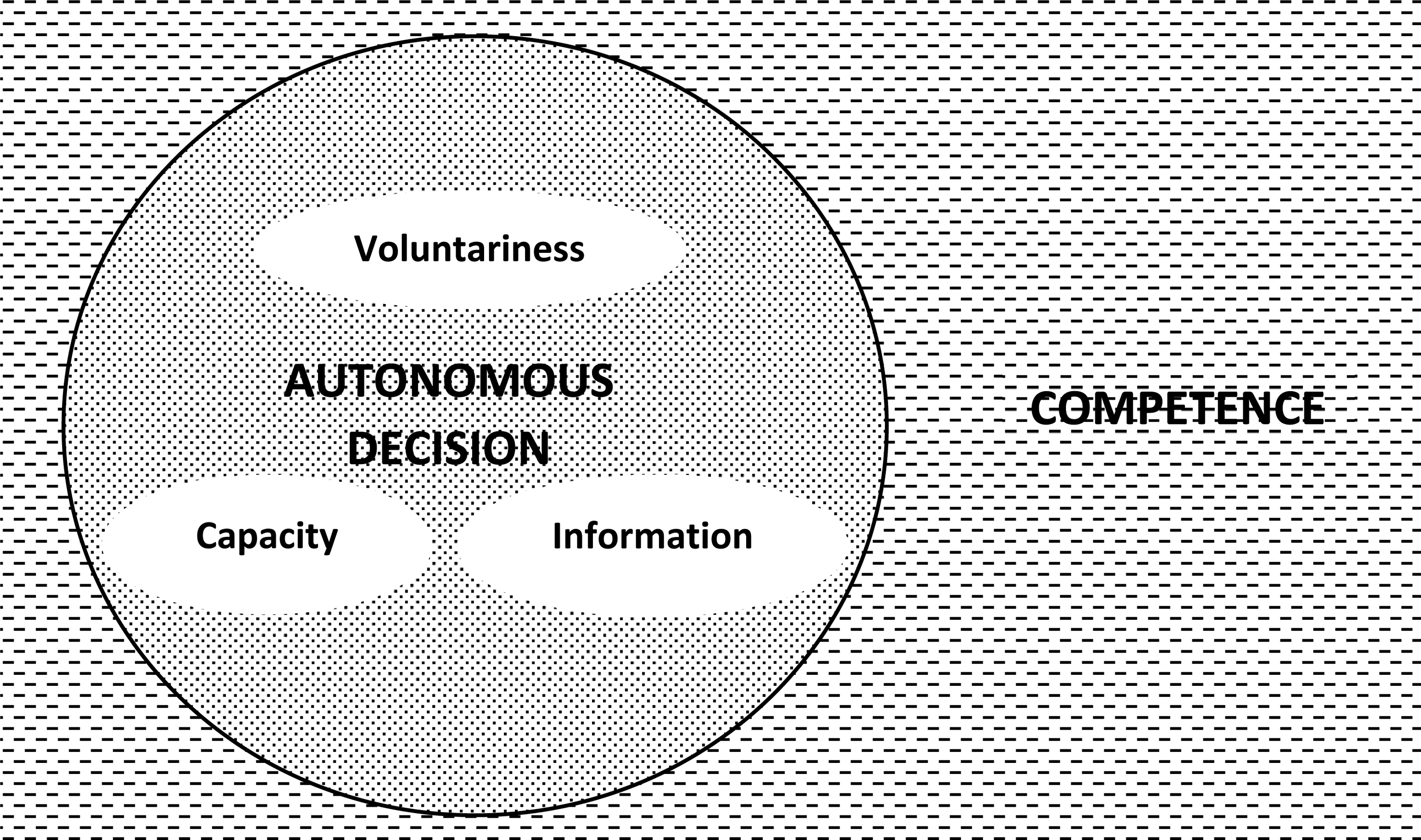
The relationship between competence and capacity. Competence is the ability to make autonomous decision, which depends on capacity to understand information and voluntariness.
In the context of minors, incompetence is attributed to the lack of capacity, 1 but this is not always the case. For instance, studies have shown that when given the same situation, adolescents as young as 14 years old could make sound treatment decisions as adults.21,22 Although these studies involve hypothetical scenarios, it demonstrated that minors have a certain capacity to make reasonable treatment decisions. Arain et al. reported that the pre-frontal cortex, an area of the brain with executive functions (including decision-making) evolves and only matures fully at 25 years old, 23 which is beyond the age of majority in most countries. This biological process is postulated as a reason why adolescents are more likely to engage in high-risk activities compared to adults. 23 This may be true to a certain extent, but it does not imply that the brain's executive function maturity affects capacity. If anything, the study findings supported our view that the age of majority is an inaccurate representation of capacity. For instance, if brain immaturity is the justification to consider a 17-year-old as lacking capacity and thus incompetent, the same could apply to a 23-year-old based on the study results, which is not the case. Furthermore, the definition of the age of majority differs between countries, ranging from 18 to 21 years. 24 This variance reflects our notion that the age of majority does not reflect capacity. For example, consider a 19-year-old from country A, where the age of majority is 18 years, who migrates to country B where the age of majority is 21 years. If we define capacity based on the age of majority, it makes no sense that the 19-year-old loses his capacity simply due to migration. Thus, it is an oversimplification to assume that every minor is incompetent due to lacking capacity, as capacity level differs between individuals and situations. While evolving capacity may contribute to their incompetency, labelling all minors as lacking capacity is an unjust supposition.
In minors who have adequate capacity, what else can affect their competence? To answer this, we need to be well-versed in the circumstances which compel a minor to be vulnerable. They are vulnerable to external pressures of being dependent on adults for material (money, food, shelter), emotional (care, support, love) and social (guidance in difficult situations, absence of role models) assistance. 25 In addition, other risk factors that contribute to a minor's vulnerability includes poverty, problematic families and health issues. 25 Even if the minors have adequate capacity, these vulnerabilities may affect their voluntariness, which in turn affects their autonomy. This is particularly significant if the minor is not emancipated. For example, an adolescent may refuse a lump-removal surgery, but this may not be due to his lack of understanding of the significance. As an adolescent, he is financially dependent or may not have anyone to support him post-surgery. In this example, his voluntariness is affected by his social vulnerabilities as a minor rather than the lack of capacity to understand the procedure. It is, therefore, important to recognise and address these vulnerabilities when working with minors, and provide appropriate support and guidance in decision-making.
In clinical settings, some precedents allow minors to make treatment decisions.26,27 The case of Gillick versus West Norfolk and Wisbech Area Health Authority [1986] AC 112 is the most famous example where the presiding judge ruled that a child under 16 years old can give consent if they have sufficient understanding of the proposed treatment including the procedure, the risk and benefits and availability of other options. 28 However, the application of the Gillick competence test when deciding a minor's competence is not undisputable. 29 The timing of capacity assessment, the interpretation of Gillick competence to agree or refuse treatment, the vague definition of competence, and the ambiguity of the relationship between competence and authority are the arguments against Gillick's. 29 There are suggestions to supplement the Gillick competency test with parts of the Mental Capacity Act, which have a more comprehensive definition of capacity, to provide clinicians with a more robust definition of capacity. 29 These suggestions are yet to be tested, and arguments on the best approach are ongoing, which is beyond the scope of this article. Nevertheless, from an ethical viewpoint, these arguments reflect the growing appreciation of the minor's decisional capacity within the legal fraternity. This positive development upholds the principle of respect for a person's capacity.
In short, we have ascertained that a minor's incompetence should not be assumed to stem from a lack of capacity. A minor's competence is more likely to be influenced by various external vulnerabilities, affecting their voluntariness. Therefore, it is unfair to blanketly exclude minors from the consent process. Instead, each minor should be involved, guided and supported in decision-making to the best of their capacity.
We have argued that a minor's capacity to decide treatment should be respected. However, our previous discussion is focused on the capacity of minors to decide their treatment. The next question is whether a minor has the same capacity to decide for other individuals. In our case, can the adolescent mother make medical decisions for her infant? Due to the paucity of literature and precedence, there is no definite answer. From the legal standpoint, some places in the United States allowed 15-year-olds to be the sole surrogate decision-maker for their infants as a way to advocate rights to parental authority, although this is not absolute. 30 Opponents argued that by allowing adolescents to be the surrogate to their infants, the infants are denied the right to a competent, adult surrogate decision maker. 30 It is not our expertise, nor is it our intention to decide which legalities are appropriate. Instead, we considered the ethical viewpoint, where respect for individuals should prevail. In our case, respect for individuals is not only about respecting her parental rights; it also comprises respecting her choices. That includes her choice to determine the surrogates for her infant, especially if it concerns complex medical decisions.
Before we discuss this further, it is important to appreciate that making medical decisions can be overwhelming, even for adults. 31 The complexity of medical decisions comes in a spectrum, from decisions for a minor procedure to decisions for end-of-life care. It is even harder to make a surrogate decision, especially if the decision significantly affects the person's life. Iverson et al. reported that adult surrogate decision-makers in critical care settings expressed the difficulty of committing to a decision, where they felt pressured with limited or no alternatives. 32 Thus, it does not do justice to expect a minor to make decisions that even adults find difficult in the name of respecting her capacity. Instead, she should have the choice not to make that decision. In other words, just because a minor is capable of deciding for her infant does not mean she must.
A proposed approach for Informed consent of infants born to adolescents
In Malaysia, the law disqualifies those below the age of majority from giving informed consent. 1 Consequently, minor parents are legally disqualified from being their children's surrogates. A typical informed consent process involving adolescent parents is illustrated in Figure 2, although practice may vary between institutions. As an alternative, we propose an approach (Figure 3) to obtain informed consent from adolescent parents while still working within the confines of the law. This shared decision-making approach primarily upholds the principle of respect for the minor and differs from the typical approach in three ways. First, the adolescent mother is more involved in decision-making for her infant, yet the responsibility does not lie solely on her. Considering the stressful circumstances an adolescent might face during the post-partum period, this may spare her the pressure of making difficult decisions alone. Second, the adolescent mother's choice of surrogacy for her infant is respected. As illustrated in Figure 2, typically, the adult who is a next-of-kin of the adolescent mother (e.g., her parent) is the legally-acceptable surrogate by default in the current setting. This may be tricky if the relationship between the adolescent and her parent is problematic. In context, the adolescent's pregnancy may not be well received by her family, especially in conservative communities where out-of-wedlock pregnancy is shunned and even criminalised.33,34 Thus, our proposed approach addresses this problem by identifying surrogates based on the level of trust rather than by hierarchy of kinship. Lastly, the clinicians play a more significant role as the adolescent's advocate by providing guidance and support throughout the informed consent process.
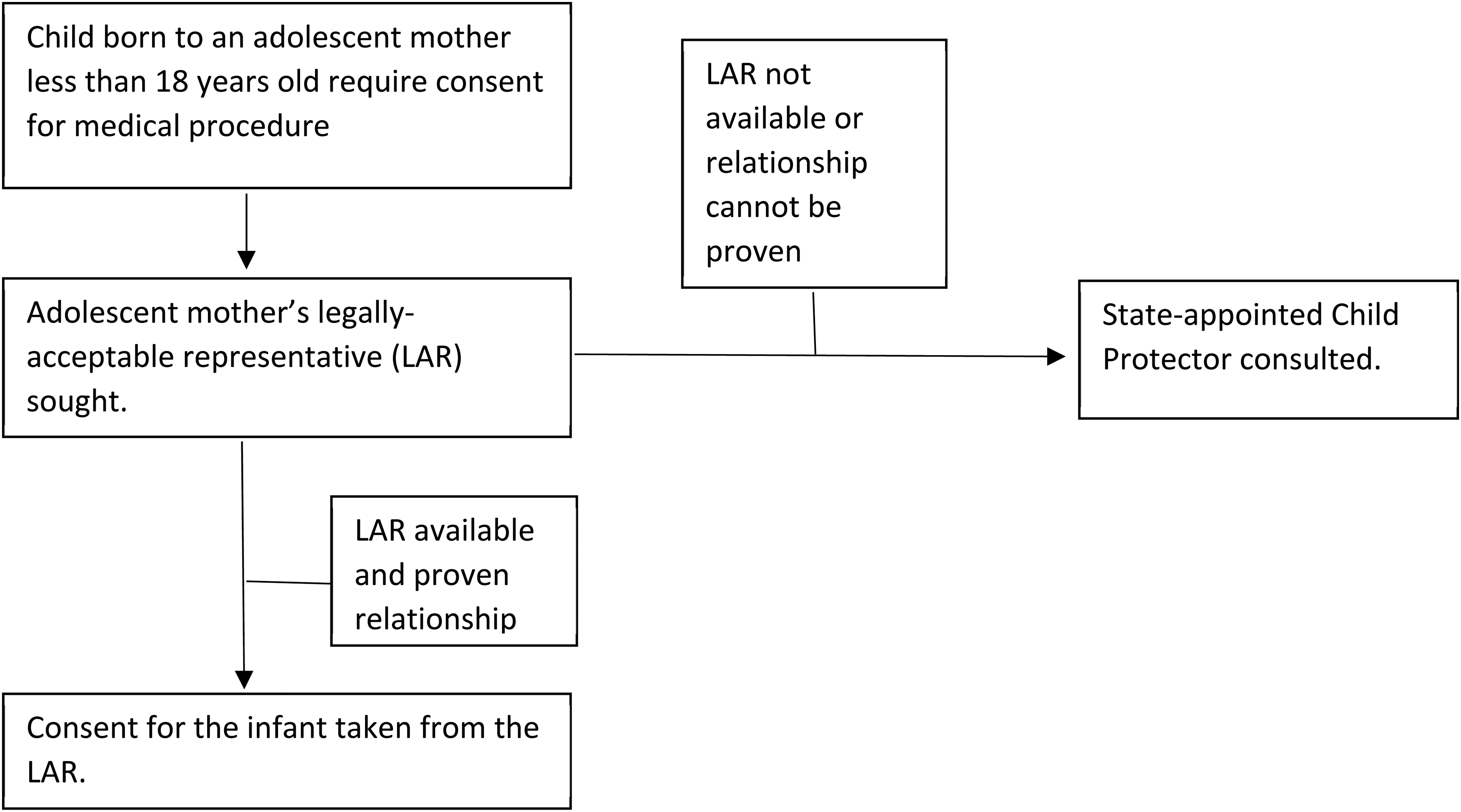
A typical informed consent process for a child of an adolescent. Practice may vary between different hospitals.
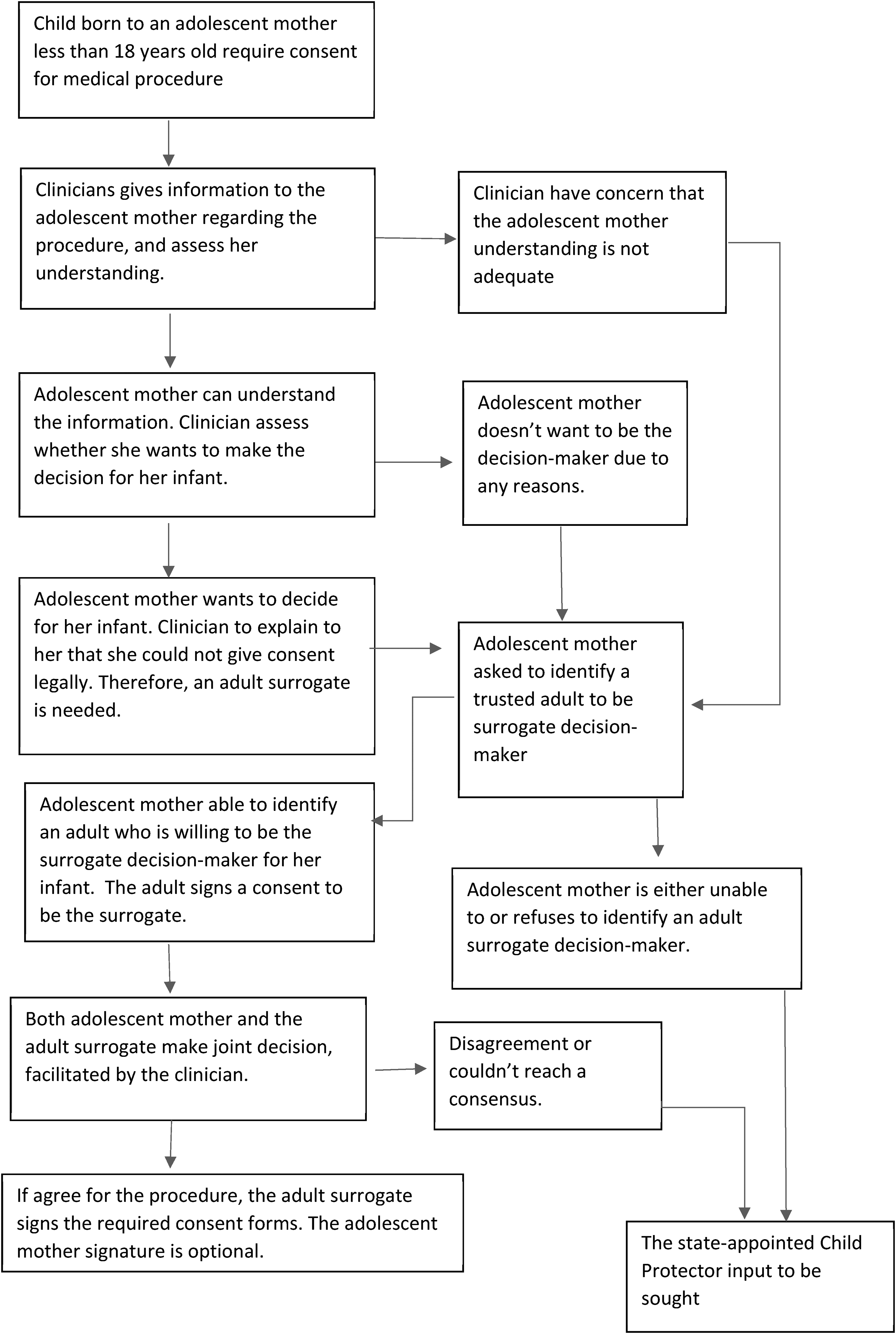
Suggested approach to obtaining informed consent for the child of an adolescent.
As an approach based on the shared decision-making (SDM) model, our proposed model shares the limitations of SDM. 35 In particular, clinicians may find our proposed approach time-consuming and unsuitable for life-threatening emergency conditions, which are common in the NICU. However, we argue otherwise. In life-threatening conditions, we acknowledge that the timing of informed consent may be delayed, but clinicians are still obliged to explain and get informed consent afterwards, during which our proposed approach is applicable. However, we do recognise that other factors like the clinician's lack of SDM practice and exposure, competing priorities with other patients, workload and unsuitable ward environment may be more significant limitations towards the implementation of our proposed approach. 35 Nevertheless, these limitations should by no means be the reasons for disregarding adolescent's choice. Instead, these are challenges that everyone should seek to overcome to uphold the principle of respect for individuals. These challenges are difficult to surmount as it requires unequivocal commitment from all stakeholders, but it is a worthy cause to champion.
Finally, the involvement of the state-appointed Child Protector as the last resort in our proposed approach seem to endorse paternalistic medicine, where the surrogate's decision is overridden by a third person. 36 We beg to differ for two reasons. Firstly, the actual patient in our case is the infant who lacks autonomy; thus, any decisions should be made by a competent surrogate, whomever they may be. In this context, the Child Protector simply assumes surrogacy after the initial surrogates fail to decide. Secondly, the involvement of the Child Protector in our case does not fit the definition of paternalism. Our proposed approach does not involve the Child Protector overriding the surrogate's decision; the Child Protector is invoked only if the surrogates fail to decide. This step is important to safeguard the infant's health, particularly in settings where the surrogates are undecided on conditions that are not immediately life-threatening but have catastrophic outcomes if the treatment is delayed, for example, to consent for peritoneal dialysis in a uraemic infant.
Conclusion
Obtaining consent for the infant of an adolescent parent is ethically and legally challenging. We propose an approach that respects the adolescent's capacity and choice in all aspects of the informed consent process while allowing clinicians to work within the country's legal framework. The proposed approach is not meant as a legal guide, but aims to promote further discussions on navigating through similar scenarios. We do not claim to have the best approach. Instead, we merely illustrated how such a scenario could be addressed guided by the ethical principle of respect for individuals. Lastly, we hope our case study generates awareness among the medical, legal and ethical fraternities of the urgent need to address this not-so-uncommon ethical conundrum in this part of the world.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This case study is registered in the Malaysian National Medical Research Registry (NMRR ID-23-00434-FUU). As per local regulations, ethics committee review for case studies are waived.