
Abstract
Restrictive visitation policies produce inequities in healthcare that have meaningful consequences for patients’ health and well-being. There is a surplus of existing literature exploring the consequences of reduced visitation in the setting of pediatric patients lacking decision-making capacity, but relatively little scholarship addressing visitation restriction for less vulnerable adults possessing capacity. Here, we present the case of a patient who suffered serious complications of childbirth, during the delivery of her healthy newborn, leading to prolonged hospitalization. During her treatment course, she was subsequently denied visitation with her newborn, who had been discharged from the hospital, and this had detrimental effects on her recovery. Hospital policies restricting visitation during the COVID-19 pandemic were intended to reduce the risk of disease exposure for both patients and staff, despite conflicting evidence demonstrating this benefit. In contrast, they often have negative effects on patient stress, mood, and physical recovery. The sequelae of this US-based case study argue the need for more holistic hospital visitation policies, placing a specific lens on adult patients receiving a visitation from their newborn children.
Introduction
The lack of uniformity in visitation policy and the resultant inequity in healthcare has been previously described. 1 Reduced visitation can impact the psychosocial, decisional, and logistical aspects of patient care. Existing literature demonstrates the consequences reduced visitation has on dependent pediatrics patients in addition to others lacking legal decision-making capacity (DMC).2,3 Existing visitation policies regarding vulnerable populations, strongly emphasize logistical considerations, such as assistance with bedside care and informed consent, when granting exemptions because these factors have a beneficial impact that outweighs the underlying intent of reduced visitation (i.e. to limit the spread of disease).2,3
Less attention has been paid, among providers, to the effects restricted visitation has on hospitalized parents possessing DMC receiving visits from their minor children. The case described below involves a patient who suffered severe complications related to childbirth, requiring prolonged hospitalization in the United States, and who was subsequently denied visitation with her newborn. This case further supports the need for more holistic, compassionate, and conscientious hospital visitation policies among adult patients receiving visits from their newborn children by expanding upon previous ethical analyses. It provides an example illustrating that restricted visitation can have detrimental effects on the well-being and treatment of adult patients (with DMC) which outweigh the benefits of restricted visitation to patients and staff. It then draws parallels for this population to the logistical considerations underlying previously existing exemptions to visitation restriction regarding the contrast of beneficence and nonmaleficence.
Case
Jennifer was a 39-year-old cisgender woman who experienced life-threatening complications following the birth of her healthy fourth child ultimately resulting in cardiovascular arrest in the Fall of 2021. Following successful cardiopulmonary resuscitation (CPR), Jennifer was transferred to the surgical intensive care unit (ICU) for higher level of care. After a massive transfusion, she stabilized and was brought to the operating room for definitive surgical treatment of internal injuries related to childbirth and subsequent CPR.
Jennifer's recovery required a prolonged stay on an ICU floor given that she was intubated for a period of days, had various physiological parameters mandating this (i.e. tachycardia) and numerous complications related to her recent childbirth, and subsequent surgeries. While intubated, Jennifer was put in restraints to prevent her from pulling drains and tubing out, but at the time was unsure of the reason for the restraints. Further, given the gravity of events during her childbirth, the heavy sedation she was under, and the appearance of her abdomen after several surgeries, initially she was unsure of her newborn's health and status or if she had even delivered yet at all.
Jennifer had never seen her baby in person, and given the traumatic nature of the delivery, she did not even remember giving birth. This confusion and uncertainty regarding her newborn and the restraints she was placed in, were understandably distressing and a great source of anxiety to Jennifer. Once able to communicate, following extubation, Jennifer expressed concern regarding her healthy newborn, who she learned had actually been discharged with family, and frustration that she was not permitted visitation with her newborn, due to hospital policy, an altered version of which (modified to ensure anonymity and protect patient privacy) is displayed in Figure 1. The hospital policy at the time, depicted in Figure 1, had restricted visitation due to COVID-19 and mandated that patients 18 years and older on an ICU floor be limited to one designated visitor, who also had to be at least 18 years of age. This restriction was based on local institutional interpretation of state department of health (DOH) guidelines which set age requirements for visitation and available Centers for Disease Control (CDC) recommendations to “allow only visitors essential to providing patient care” such as individuals to “help provide patient care and/or care for pediatric patients.”4–6 The length of Jennifer's hospitalization, therefore, resulted in prolonged separation from her newborn during a period that is typically regarded as critical for bonding. This can in turn lead to increased levels of maternal stress and anxiety as well as numerous health detriments to baby.7–11 This had a detrimental effect on Jennifer's mood, which hindered her participation in occupational, physical, and speech therapy, and in her medical team's opinion significantly delayed her physical recovery. Consequently, her medical team began to feel that they were providing inadequate treatment and caring for their patient with insufficient compassion.
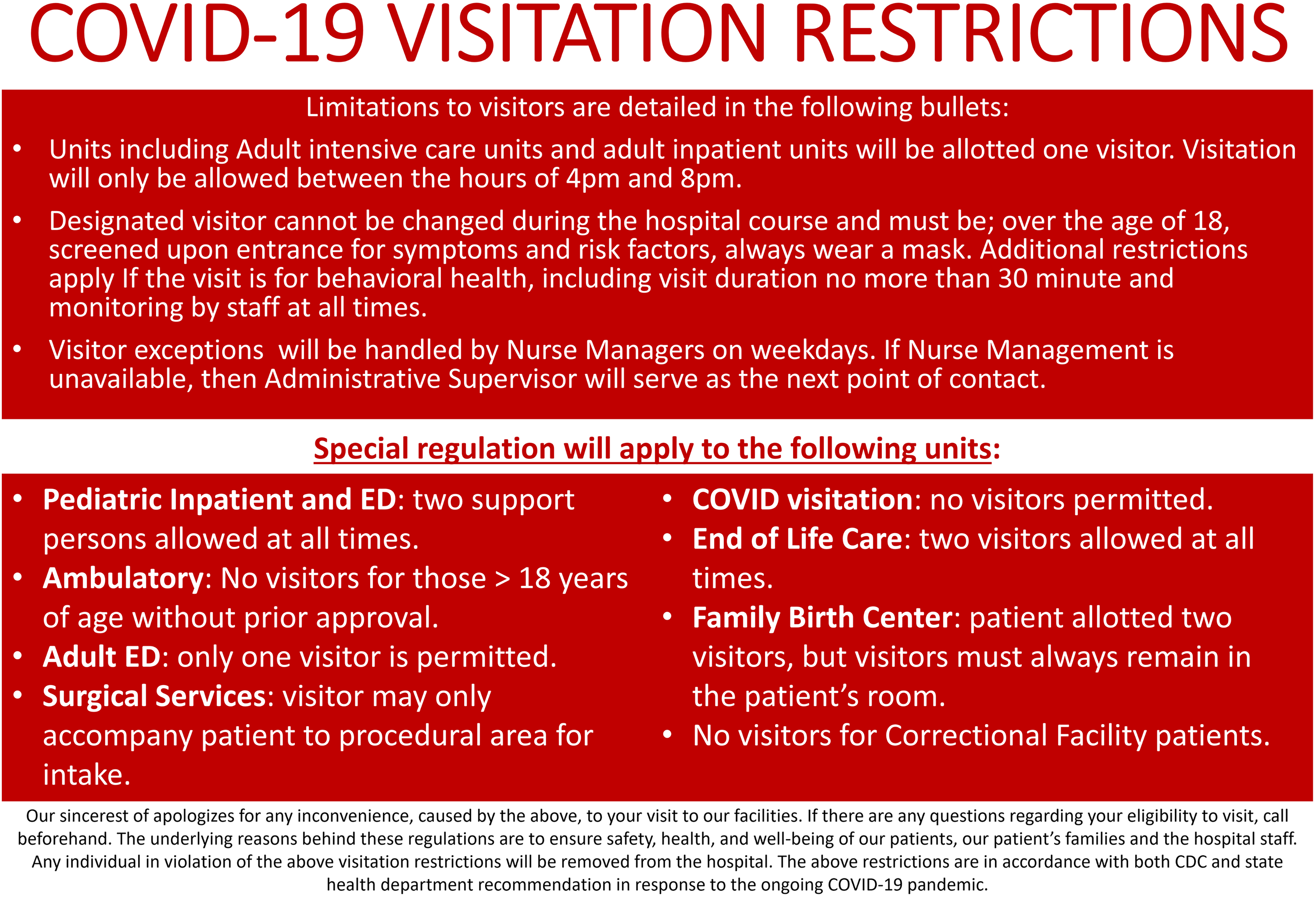
Example of restricted visitation policy. This figure was modeled after restricted hospital visitation policies available online and modified for deidentification.
Jennifer requested to visit with her newborn multiple times over several consecutive days. Both the nursing staff, and her team of physicians spoke with hospital administration to express Jennifer's circumstances and her desire to be with her newborn and request she be granted visitation, but this request was denied given the newborn's age, and existing hospital policy (Figure 1). As such Jennifer was repeatedly told this was prohibited by the hospital's policy and when senior members of her treatment team finally informed her that this was an absolute prohibition, she was overwhelmed with anguish and despair. The contrast between Jennifer's affect and appearance preceding and following receipt of this information was immediately evident. Soon after, she experienced a decline in her physical health, with a reversal of previous clinical improvements. Given this, her team pursued various avenues to allow for an exception to permit visitation.
After lengthy and repeated conversions with multiple hospital departments and administrators, on the part of attending physicians, nursing, and case management, Jennifer was eventually granted visitation with her newborn. Over the following days, her mood greatly improved, along with her appetite and her ability to participate in physical and occupational therapy, which accelerated her recovery and eventual discharge. This case was based on true events. The patient's name and demographic information were fictionalized and the specific complications of birth as well as conditions complicating recovery were masked to protect the identity of the patient.
Discussion
The risks and benefits of restricted and liberal visitation policies
Hospital policy associated with COVID-19 was preventing Jennifer from fulfilling her need, as a parent, to be with and care for her newborn, though it was consistent with WHO, CDC, and NYS DOH guidance, available at that time, regarding visitation restriction related to age and assistance with care.4–6,12 The policy was implemented with the intent to keep Jennifer, her newborn, staff, and other patients safe. Jennifer was suffering from a number of problems that could have put her at increased risk of complications from COVID-19 infection, such as her recent surgeries. 13 Guided by the principle of nonmaleficence, it is the health professional's responsibility to mitigate risks, such as disease transmission. 14 Visitation restriction is a well-established practice for decreasing transmission of traditional viruses such as influenza or respiratory syncytial virus.3,15–21
Hospital policies should both remove harm and add intervention to promote patient welfare. 14 Jennifer was on an ICU floor with other critically ill patients more susceptible to complication from infection and severe COVID-19 and the circumstances of her newborn visitation would have been different had she been on peripartum unit. As mentioned, restricted visitation has efficacy with other viral diseases, in reduced disease transmission;3,15–21 however, the policy preventing Jennifer from visiting with her newborn was specifically related to COVID-19 and not these other infections. Several studies and reviews, prior to this case, had demonstrated conflicting and unclear evidence at best for the efficacy and benefits of visitation restriction in the context of COVID-1915,16,18,20,22 and further systematic reviews expanding upon this lack of clarity have been published since then. 3 Furthermore, household members may carry a similar risk of exposure and increased co-infectivity.15,23 Consequently, restricting visitation to a single family member (Jennifer's family member), while not allowing others from the same household (Jennifer's newborn) is unlikely to reduce harm in the context of COVID-19. On top of all this, Jennifer was negative for COVID-19 throughout her stay, and there was and continues to be scant evidence for limiting parental visitation with newborns among those who are asymptomatic or negative.3,24
In contrast to reducing harm, available literature has demonstrated that reduced visitation can lead to increased stated pain and stress, decreased medical staff responsiveness, and increased fall and sepsis rates.16,22,25 The consequences of restricted visitation are especially evident when considering the lack of skin-to-skin contact (SSC) contact allotted to peripartum mothers such as Jennifer. SSC leads to higher per day newborn weight gain, and cardiorespiratory stability, lowered maternal stress and anxiety, and increased breastfeeding success.7–11 Mood, anxiety, and stress in turn correlate with recovery time.26–28 These benefits are well recognized within the scientific community and supported by laws such as the Newborns’ and Mothers’ Health Protection Act. 29 Specifically under the lens of COVID-19, evidence has since come out that parental separation from newborns is associated with increased postnatal depression, suicidal ideation, and decreased breastfeeding success. 30 Breastfeeding in turn leads to decreased postpartum blood loss and reduction in all-cause newborn mortality. 31
Restricted visitation policies with indeterminate evidence for benefit3,15–19,22 and clear evidence of harm violate the principles of nonmaleficence and respect for autonomy. This is particularly troubling in the context of newborns visiting their parents as exemplified by Jennifer and her newborn given the clear benefits to visitation on patient recovery time, and satisfaction with hospital experience.32–34 Furthermore, Hospital policy in the context of COVID-19 should be continually revisited and revised as new evidence continues to be published. In Jennifer's case, instead of fostering an environment conducive to healing, the visitation policy actively harmed her, physically and mentally.
Patient autonomy and visitation policy
Despite the fact that the purported benefits of hospital visitation policies are universal, existing literature demonstrates certain subsets of vulnerable patients (such as children) are more likely to be granted exemptions.3,32,35 The risk to the rest of the hospital, however, is similar whether a parent is visiting a child or that same child is visiting the parent in the hospital. Evidence regarding the increased spread of infection from children visitors to the hospital is conflicting36–39 and in fact, as the pandemic continues, available evidence has demonstrated children are less frequently the source of transmission in the spread of COVID-19.40,41 Furthermore, the risk of COVID-19 is similar among household members,15,23 so allowing Jennifer's newborn to visit, accompanied by the already visiting caretaker, would likely not increase the infant's risk of infection. There is contradictory evidence and unclear benefit to the rest of the hospital population regarding decreased spread of COVID-19 by preventing child visitors, or by preventing children from accompanying other visitors from the same household. In contrast, there are clear benefits, detailed in the preceding paragraphs for allowing newborn children to visit with their parents such as lowered maternal stress and anxiety, and decreased recovery time. Unlike young children, there were no questions regarding Jennifer's DMC and there were clear benefits to Jennifer from visitation which outweighed the unclear and likely minimal risks to the rest of the hospital population from her newborn visiting. Thus, the denial of the right to assess the risks and benefits of visitation for herself and her child was a clear infringement on her autonomy, with no clear benefit to the rest of the hospital.
Visitation policy and exemption
Hospital policy should be guided by the cost-effective management of limited clinical resources to maximize benefits and minimize harm 42 and be applied in a just and equitable manner across all patients. 35 A universal approach to visitation policy fails to incorporate the unique needs of individual patients, families, and clinicians in the widely varying clinical settings of the hospital. 3 The lack of directive from state guidance recommending a minimum age for visitation “except in rare exceptions as determined by the hospital” 4 and the ambiguity in CDC guidance limiting visitation to “only those essential for the patient's physical or emotional well-being and care” 6 has the potential to exacerbate inequity. This is further complicated by the lack of consistency among various health care providers when implementing and dissenting from said hospital policies and procedures.43–46 In Jenifer's specific case, the lack of clarity from this guidance in regard to “emotional well-being” and no provision for examples of “rare exceptions” that hospitals could base their decisions on result in policies that limit emotional support to only those over 18 (Figure 1) and prevented Jennifer from receiving needed time with her newborn. If a patient's health allows, hospital visitation policy should not separate or deny visitation between parents and their newborns.
The real question regarding an exemption to policy is: does the benefit of an exemption for patients outweigh the potential risks to other patients and staff? Restricted visitation is not novel, however, the data prior to this case and thus far in the pandemic has failed to sufficiently demonstrate its efficacy in reducing the spread of COVID-19.3,15–19,22 Yet available literature demonstrates that age restrictions for COVID-19 visitation policies are not unique to Jennifer's case, are prevalent in many other institutions, 47 and have similar effects on patient health and emotional status. 48 Therefore, these policies in the context of COVID-19 are not based on evidence and should continually be reviewed and revised. Research has not shown a significant risk of vertical transmission between asymptomatic mothers with their newborns.3,24 In fact, the passage of antibodies to COVID-19 through breastmilk may be beneficial to infants.49–52 As noted above, Jennifer's sole permitted visitor was a caretaker of the newborn; infection brought to the hospital by the infant was likely to be shared by the caretaker.15,23,38 Limiting visitation to just one family member, in certain scenarios, has the potential to negatively impact patient well-being without demonstrating a clear reduction in disease transmission.
Conclusion
The COVID-19 pandemic has been ongoing for over two years now and is likely to be a continued facet of healthcare provision. At the beginning of the pandemic, when these restricted visitation policies were implemented, there was little the citizen could do to mitigate risk besides social distance; however, the advent of safe and efficacious, and widely available vaccines, has provided individuals with other avenues to reduce their risk of severe infection. 53 Despite the evolution of the pandemic and our response to it, many institutions have maintained their restricted visitation policies, even in the absence of supporting evidence and in the face of existing evidence such as that children may transmit COVID-19 to a lesser degree. In cases like Jennifer's, adherence to hospital policy actively harms patients and families and violates their autonomy. Hospitals should consider modifying existing visitation policies to permit peripartum patients to visit with their newborns. Such approaches to visitation facilitate patients’ recovery, while also benefitting children's socioemotional development and well-being.
Current policies also lack point of contacts for exception and processes for evaluating policy impact and performing revision in the face of new evidence. 1 Often times, this leads to confusion regarding how to go about getting an exception to policy, both for patient and providers, increased wait times for a decision, and rejections of policy exemption even when the benefits clearly outweigh the risks. After much resistance from hospital oversight, the care team was able to unite Jennifer with her newborn and her status, mood, and participation in recovery incomparably improved. It is past time for hospitals to take steps to prevent similar cases from occurring within the context of COVID-19 and among any new disease outbreaks which inevitably will occur in the future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.