
Abstract
The National Health Service (NHS) in the UK is currently facing a significant waiting list backlog following the disruption of the COVID-19 pandemic, with millions of patients waiting for elective surgical procedures. Effective treatment prioritisation has been identified as a key element of addressing this backlog, with NHS England's delivery plan highlighting the importance of ensuring that those with ‘the clinically most urgent conditions are diagnosed and treated most rapidly’. Indeed, we describe how the current clinical guidance on prioritisation issued by The Federation of Surgical Specialty Associations serves this aim. However, whilst there are strong reasons to prioritise elective surgery in accordance with clinical need, we argue that it would be a mistake to assume that prioritisation in accordance with clinical need requires only a clinical or scientific judgement. The understanding of clinical need that we choose to employ in a prioritisation system will be grounded by some key ethical judgements. Moreover, we may also have to make trade-offs between addressing clinical need, safeguarding equality, and achieving other benefits. As the UK faces up to the backlog, it is important that surgical prioritisation guidelines enshrine a broad range of values that we believe ought to determine access to care in non-emergency circumstances. Our analysis suggests that the current approach to prioritisation is not a sufficiently nuanced way of balancing the different moral values that are operative in this context.
TEST CASES
[number in parentheses = Federation of Surgical Specialty Associations priority group classification]
Test Case 1: Elderly Patient Requiring Lower Limb Amputation
An older patient requires surgical intervention following a severe ankle break. However, their functional recovery after surgery may be limited. (P2)
Test Case 2: Elderly Patient Requiring Joint Replacement
An elderly patient is suffering from symptomatic arthritis, which causes them significant pain and motor impairment. The condition is not life-threatening, but it can only be ameliorated with a joint replacement. (P4)
Test Case 3: University Student Requiring ACL Reconstruction
A younger patient has torn their anterior cruciate ligament (ACL). They currently report knee instability and feel that their knee will give way especially when turning, pivoting, or walking down a flight of stairs. They have not been able to return to sport and symptoms have persisted, despite the patient undergoing a suitable period of high quality physiotherapy. As a university student they are able to attend lectures and sit examinations from home. They have been on a waiting list for 4 months. (P4)
Test Case 4: Manual Labourer Requiring Achilles Tendon Reconstruction
A younger patient has presented with worsening heel pain and a limp following an injury several weeks ago. They are now no longer able to function in their professional capacity as a manual labourer. They have been experiencing increasing pain for a number of weeks but they had not previously sought medical advice, partly due to their long working hours. A surgical reconstruction of the Achilles tendon is recommended. They put the patient on the waiting list for a surgical appointment. (P3)
The COVID-19 pandemic has had a considerable deleterious effect on waiting times for elective surgery in the NHS.1,2 Data from NHS England show that there were 6.6 million patients awaiting treatment in May 2022 (up from 4.4 million in January 2020), with roughly 3.13 million awaiting surgery. 3 The government's spending watchdog has warned that waiting lists for elective care in England could reach 12 million by early 2025 without additional staff and bed capacity. 4 Long waiting times are already playing a role in leading large numbers of patients to self-fund treatment privately – the last 3 months of 2021 saw 69,000 patients self-fund treatment, a 39% increase on the same period prior to the pandemic. 5
There are several factors that may have contributed to this predicament, likely including the closure of clinics during the pandemic, the redeployment of surgical staff, and staff absences through illness, amongst others. 1 Whatever its cause, the gravity of the situation is clear.
In response, the government committed £1 billion in the November 2020 spending review to help tackle the elective backlog as part of an additional funding package to support recovery. 4 Furthermore, NHS England recently published a delivery plan for tackling the COVID-19 backlog of elective care (henceforth ‘the delivery plan’). 6 Effective treatment prioritisation is identified as a key element of the delivery plan, which notes the importance of ensuring that those with ‘the clinically most urgent conditions are diagnosed and treated most rapidly’. This aligns with Curtis et al.'s claim that ensuring quickest access for those with greatest need should represent one of the fundamental objectives of a waiting list system for surgery. 7
When appointments for elective surgery are effectively a scarce medical resource, prioritising patients with the greatest need can improve fairness, reduce the waiting times of patients with a more urgent need, and reduce variations between regions.8,9 Nonetheless, level of need has not always been a major determinant of waiting time for some surgical procedures. Indeed, in addition to finding significant differences in waiting time for hip replacement surgery according to social, geographical and health care system factors, Fitzpatrick et al. also found that patients with worse pain and disability at surgery waited longer for an out-patient appointment. 10 There is also some evidence to suggest that patients with greatest need may still not be prioritised even when there is a formal queue management system for elective surgical procedures based on that criterion. 11
Prioritising elective surgery in accordance with clinical need can have clear benefits, but it would be a mistake to assume that prioritisation in accordance with clinical need requires only a clinical or scientific judgement. Prioritisation decisions require us to make trade-offs between competing ethical values; furthermore, the understanding of clinical need that we choose to employ in a prioritisation system will also be grounded by some key ethical judgements. As the delivery plan suggests that prioritisation frameworks for elective surgery are under review, it is timely to reflect on some of the key ethical judgements that will ground a revised framework that gives precedence to clinical need in prioritisation decisions. We will also reflect on some of the other ethical values that may factor into prioritisation decisions.
The initial guidelines
Although clinical need features in many international prioritisation guidelines, the concept is somewhat ‘ill-defined’. 7 This is particularly problematic since transparency, certainty, and scientific validity should all be key elements of an ideal prioritisation system. And so, we argue, should the ethical values that underpin the concept.
Early in the COVID-19 pandemic, in the summer of 2020, The Federation of Surgical Specialty Associations (FSSA) set out a clinical guide to surgical prioritisation in the pandemic, which set out what clinicians view as the relative priorities of different conditions. 12 Crucially, as the introductory notes to the Guide made clear, the Guide ‘began as a short-term expedient to the pandemic and was not intended for long term use’. It set out five priority groups (1a, 1b, 2, 3, 4), with a maximum waiting time stipulated for each group. A given condition or procedure will fall within one of those groups. For instance, aortic stenosis was deemed a priority 2 condition, which should thus be attended to within 1 month, whilst ileoanal pouch surgery was deemed a priority 4 procedure, which maythus be performed within a period exceeding 3 months.
There are two elements of this framework that warrant initial comment. First, the moral reasons to address high clinical need are taken to have lexical priority over other values that might be thought relevant to waiting list management. For instance, although time already spent on a waiting list might serve as a tie-breaker between two patients in the same priority group, a patient in a higher urgency group will have priority over a patient in a lower group who may have been on a waiting list for a longer period.
Need is often the basis for egalitarian approaches to distributive justice: equal treatment for equal need. This is the stated basis of the NHS. Urgency is one key marker of need. However, affording clinical need this lexical priority in resource allocation decisions is not universally accepted, since it might be argued that time already spent on a waiting list has some moral significance. The thought here might be that patients who have spent a long time on a waiting list are owed or deserve some degree of priority, even if others have greater need. One basis for this is an egalitarian approach to justice; queue-based ‘first come first served’ allocation procedures can be one way of operationalising an egalitarian approach that aims to give individuals an equal opportunity to receive a scarce good. 13 Alternatively, time spent waiting may not just be relevant from an egalitarian perspective, it might also be argued that this time is a kind of ‘cost’ that the individual has ‘paid’ for treatment. On this understanding, it might be argued that these patients deserve a certain degree of priority from considerations of desert. In this vein, outside of the pandemic context, Testi et al. have developed a Need-Adjusted-Waiting-Day metric to accommodate both clinical urgency and time spent already waiting into surgical prioritisation decisions. 14
Nonetheless, whilst acknowledging the moral significance of the fact that many patients have been on elective surgical waiting lists for a considerable amount of time, we believe that the initial guidelines were correct to place greater weight on the moral reasons we have to address highest clinical need, particularly given the circumstances of high scarcity at the time of the pandemic.
The second notable feature of the guidelines is that it relies on a conception of clinical need as determined solely by severity of condition, as agreed by the relevant professional community. One benefit of this approach is that it is easy to operationalise, and it gives clinicians straightforward guidance. These are clearly virtues of a system that, as we mentioned above, was developed as an expedient to an emergency situation; moreover, it may be argued that in such circumstances we have particularly strong moral reasons to place particular emphasis on addressing the most pressing clinical need (for reasons we briefly explore below). Yet, it is notable that prioritisation frameworks elsewhere have adopted broader conceptions of clinical need and incorporated other values, as we now go on to describe. As we leave the emergency phase of the pandemic, it is thus appropriate to reconsider the guidelines created for these circumstances, and to consider whether our approach to surgical prioritisation outside of these circumstances should incorporate a broader range of potentially morally relevant features.
Social contributors to need
In other prioritisation frameworks that existed prior to the pandemic, non-clinical factors are understood to contribute to need. For instance, both the clinical priority assessment criteria (CPAC) tool used to assess need for surgery in New Zealand, and the Western Canada Waiting List Project (WCWL) standardised assessment use a range of both clinical and social factors to assess need for surgery. 7 For instance, the CPAC score takes into account whether clinical conditions threaten the patient's ability to work, care for dependants, and live independently. 15
Whether such social factors should contribute to an assessment of clinical need in prioritisation requires us to make various value judgements. One argument for taking these social factors into account is that clinical measures alone may not fully capture the suffering that an individual patient may experience as a result of their condition. Furthermore, it might be argued that social factors are needed to capture the benefit that surgery may have for others beyond the patient herself. A different argument concerns justice; some of the social factors that contribute to a broader conception of need, such as the ability to work, may be attributable to background inequalities. A failure to accommodate these social factors may therefore overlook the insidious role that background injustice can play in obstructing access to health care.
This is particularly important in the current context, as there is some evidence to suggest significant differences in waiting time for surgical procedures by virtue of social, geographical and health-system factors. 10 Moreover, some evidence suggests that demographic features such as ethnicity and gender have some influence on access to surgery,16,17 although evidence regarding the influence of social factors is mixed. 10 In view of this data, we should welcome the fact that the delivery plan calls for resources to be distributed fairly according to clinical need and for systems to analyse waiting list data by relevant characteristics (including age, deprivation, ethnicity, and by specialty) to ensure this. We return to this point below.
Potential to benefit
Other conceptions of clinical need also include criteria that are relevant to a patient's potential to benefit from surgery. Indeed, one of the motivating principles of the CPAC in New Zealand approach is the broadly utilitarian claim that priority should generally be given to patients with the greatest expected benefit from surgery. 15
In contrast, by focussing on severity of condition in determining clinical need, the initial guidelines may be understood to adopt a broadly prioritarian approach to justice. Prioritarianism claims that we should give priority to the worst off in our allocation of a scarce resource. Essentially, the focus of prioritarianism is to maximise the benefits achieved by an allocation, where the benefits to the worst off are given extra weight. 18 This latter point is primarily what distinguishes it from a broadly utilitarian approach, which would simply seek to maximise the overall (non-weighted) benefit of an allocation amongst a population. Notably, in some cases, it may be that prioritising those with the greatest clinical need is also the best way to achieve the maximum benefit in prioritisation. For instance, that may be true in in emergency circumstances in which the capacity to provide care is limited, and there are large numbers of patients with severe clinical need. However, we should not assume that the two approaches will always converge in this way.
Indeed, outside of emergency circumstances, there are legitimate concerns that may be raised about an approach that affords such salience to the severity of condition in prioritisation. First, in implementing such an approach, it is important to be wary of the surreptitious use of prognosis. A deeper concern with focusing only on severity of condition in defining clinical need is that this might mean the prioritisation system will fail to achieve the most overall benefit for patients. One reason for this is that such a system may fail to attend appropriately to those who are likely to develop significant need in the future if left untreated now. Moreover, data also suggest that there can be an important difference between addressing clinical need and actually benefitting patients. For instance, Derret et al. that found no correlations between improvement in health status following surgery and CPAC score prior to surgery. As such, these authors argued that their findings suggest that even greater weight should be afforded to potential to benefit in the CPAC score. 19
A benefit-based approach to prioritisation has to attend to a number of complex empirical matters. First, in order to accurately compare the expected benefit of a given surgical procedure for different patients, we would need to understand the likelihood of the success of the interventions for different sub-groups with the same diagnosis. However, the evidence that might be required to ground such a comparison may not always be compelling. Naturally, this issue is exacerbated when comparing the expected benefit of different surgical procedures with quite different outcomes. Furthermore, an expected benefit approach would also have to accommodate considerations of surgical risk to the patient.
These empirical questions are of considerable significance for a benefit-based approach, but there are also crucial ethical question at the heart of proposals to give expected benefit greater weight in prioritisation decisions: what are the relevant benefits? Should they be defined in a purely clinical sense in terms of the surgical outcome, or should the patient's expected length and/or quality of life be understood to contribute to expected benefit? For instance, these considerations might be used to mount one benefit-based argument in favour of prioritising younger patients. We shall outline another different argument in favour of such prioritisation in the next section.
More broadly, should we understand expected benefit at the level of the individual patient or at the macro level of how much a system of prioritisation will achieve for the patient population as a whole? To illustrate, the latter macro understanding might lend some support to prioritising patients whose surgical requirements can be dealt with in the most time (and staff) efficient manner, if that would free up appointments for more patients on the list, meaning that a greater number could receive treatment.
More contentiously, an even broader consequentialist approach might consider the implications that a prioritisation system could have at a societal level, including for individuals who are not patients. For instance, a prioritisation system could potentially be employed to achieve certain societal or public health goods. One way it might do so is by disincentivising certain undesirable healthy behaviours that result in burdens for the healthcare system; to illustrate, patients could potentially be given a lower ‘expected benefit’ score from surgery if they engage in certain unhealthy behaviours such as smoking. Notably in this regard, there is already evidence suggesting that some clinical commissioning groups in the UK delay or deny routine surgery for patients who smoke, or who are over stipulated BMI limits, contrary to national clinical guidance.20,21 Alternatively, instead of denying treatment for this sort of purpose, a truly utilitarian prioritisation system could instead give greater priority to those in professions with high social utility; indeed, in a similar vein, some countries prioritised certain key occupations for vaccination in the coronavirus pandemic.
Of course, incorporating considerations of societal benefit raise profound concerns about equal moral status and discrimination, as well as the appropriate scope of the medical profession's role in promoting healthy behaviour and other social goods. Yet even beyond this set of contentious issues, decisions about how to understand the ‘benefit’ that prioritisation systems should aim to achieve will raise issues of justice that are familiar from other debates about rationing in healthcare. For instance, incorporating considerations of expectation of benefit may mean that elderly patients will typically be placed at lower priority. This will be so if they are more likely to suffer from co-morbidities that affect surgical outcomes. More broadly, critics have argued that certain measures of expected benefit in healthcare, such as QALYs, can systematically disadvantage certain groups such as older persons and persons with disabilities. 22
Equality, benefit and need
The above remarks indicate that the seemingly straightforward and intuitive suggestion of prioritising surgery in accordance with clinical need obscures a great deal of complexity concerning how we should balance the ethical values of need, benefit and equality.
The initial guidelines placed a premium on addressing clinical need as defined by severity of condition, rather than ensuring equality of access for all patients or achieving the maximum benefits; it thus adopted a broadly prioritarian approach, which identifies the relevantly worst off group as those with greatest clinical need. 23 That is a plausible understanding of prioritarianism in this context, but it is not the only one, as Nielsen highlights in a recent discussion of pandemic prioritiarianism. 24 Social justice prioritiarians might identify those who have faced structural injustice as the worst off group, whilst age-based prioritarians might maintain that the relevantly worst off group in this context are the youngest patients, for the simple reason that they have had fewer life years than others. The latter approach offers a fairness, rather than benefit-based argument in favour of prioritising younger patients, in contrast to the benefit-based argument above.
This is not to deny that the ‘severity’ prioritarian approach implicit in the initial guidelines may be the most appropriate approach. We agree that it is a plausible approach, but it is a way of striking a balance between equality, benefit and need upon which reasonable people can differ; it is therefore crucial that patient groups are included in forthcoming amendments to prioritisation protocols.
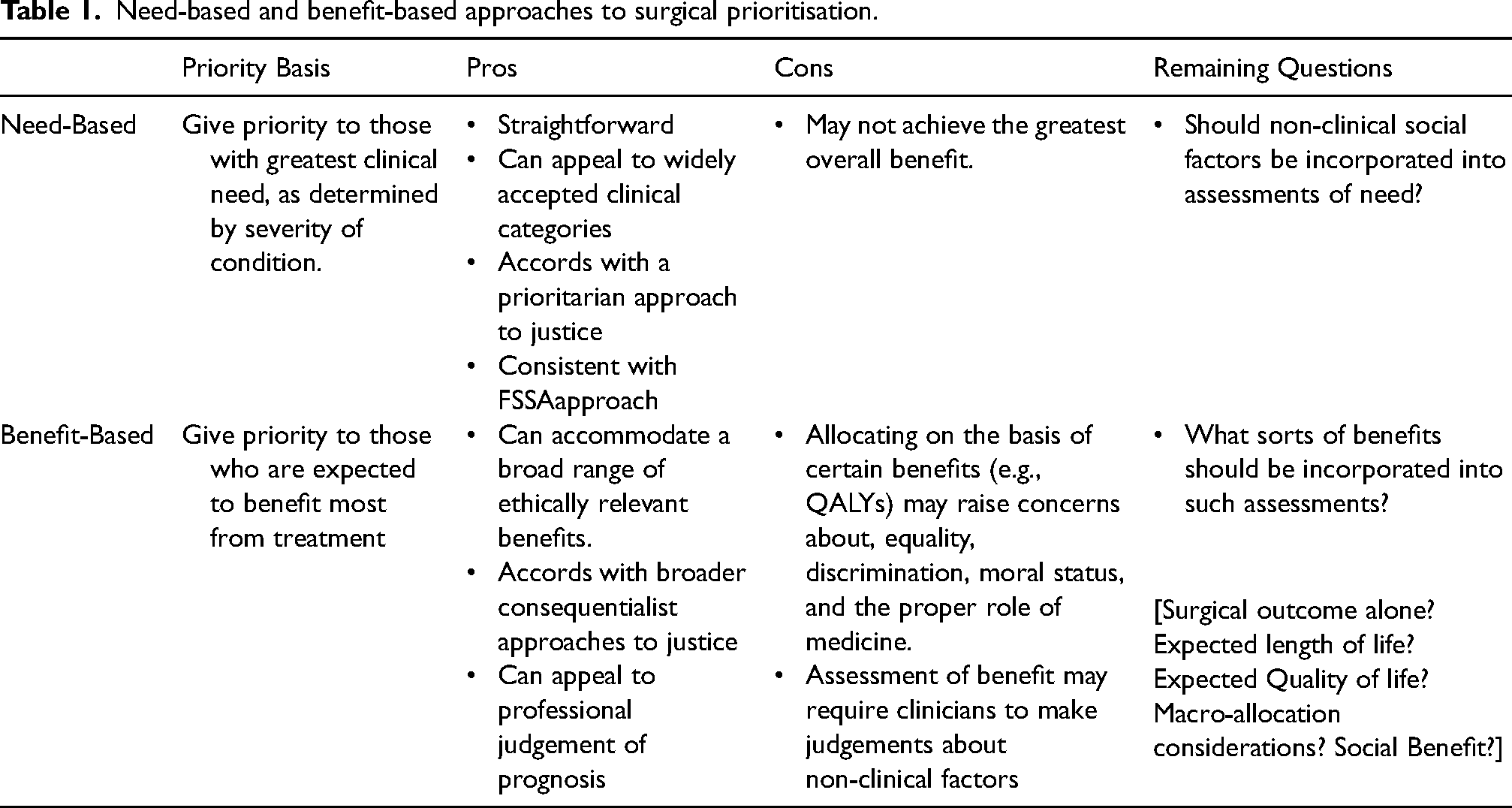
Accordingly, we believe that the first question that policy-makers should answer in outlining a prioritisation system for elective surgery is whether to adopt a primarily need-based or benefit-based approach to classifying different priority groups. We outline the pros and cons of each approach below.
To apply these approaches to our test cases at the beginning of the paper, the needs-based approach would straightforwardly put test case 1 into a higher priority group than cases 2, 3 and 4. In contrast, the benefit-based approach might put test cases 2, 3 and 4 into a higher priority group than 1 if the patient's functional recovery in the latter was sufficiently limited. Furthermore, depending on which benefits one takes into account, test cases 3 and 4 might be prioritised over test case 2.
Of course, one straightforward approach to prioritisation would not use priority groups per se, and could instead rank all individuals on the waiting list in terms of some morally relevant feature (i.e., either benefit or need) that was deemed to be most important for prioritisation. This would serve to ensure that the prioritisation system would either address clinical need or achieve some other benefit in a maximal manner. However, it might be argued that it would be unfair to prioritise on the basis of only small differences in need or benefit, and such an approach would require clinicians to make time-consuming fine-grained assessments and comparisons of every patient's need or likely benefit.
As such, there are good reasons to adopt a priority-group-based approach to allocation. However, once patients have been classified into either a need-based or benefit-based priority category, a second question arises: how to allocate fairly within these groups? An egalitarian approach for allocation within groups would be to allocate in accordance with a lottery procedure – this would be fair in the sense that it would give everyone in the group an equal opportunity to access the resource. However, the lottery approach would fail to acknowledge the fact that some individuals within the priority group may have been waiting for longer than others; accordingly, it might be argued that it would be fairer to allocate within groups on the basis of a queue-based system; this would be fair in an egalitarian sense if all individuals in the group had an equal chance of joining the queue first, and it would also acknowledge reasons of desert to reward those who have waited the longest. However, the queue approach fails to acknowledge other features that might be deemed relevant for fairness. In particular, it fails to acknowledge the fact that some patient's health needs might be attributable to background injustices. Finally, it might be argued that although it would be inappropriate to take certain benefits into account when initially classifying patients into priority groups, it might yet be permissible to consider these benefits in allocating within groups.
We outline the pros and cons of each approach to within group allocation in Table 2.
Need-based and benefit-based approaches to surgical prioritisation.
Approaches to fair allocation within priority groups.
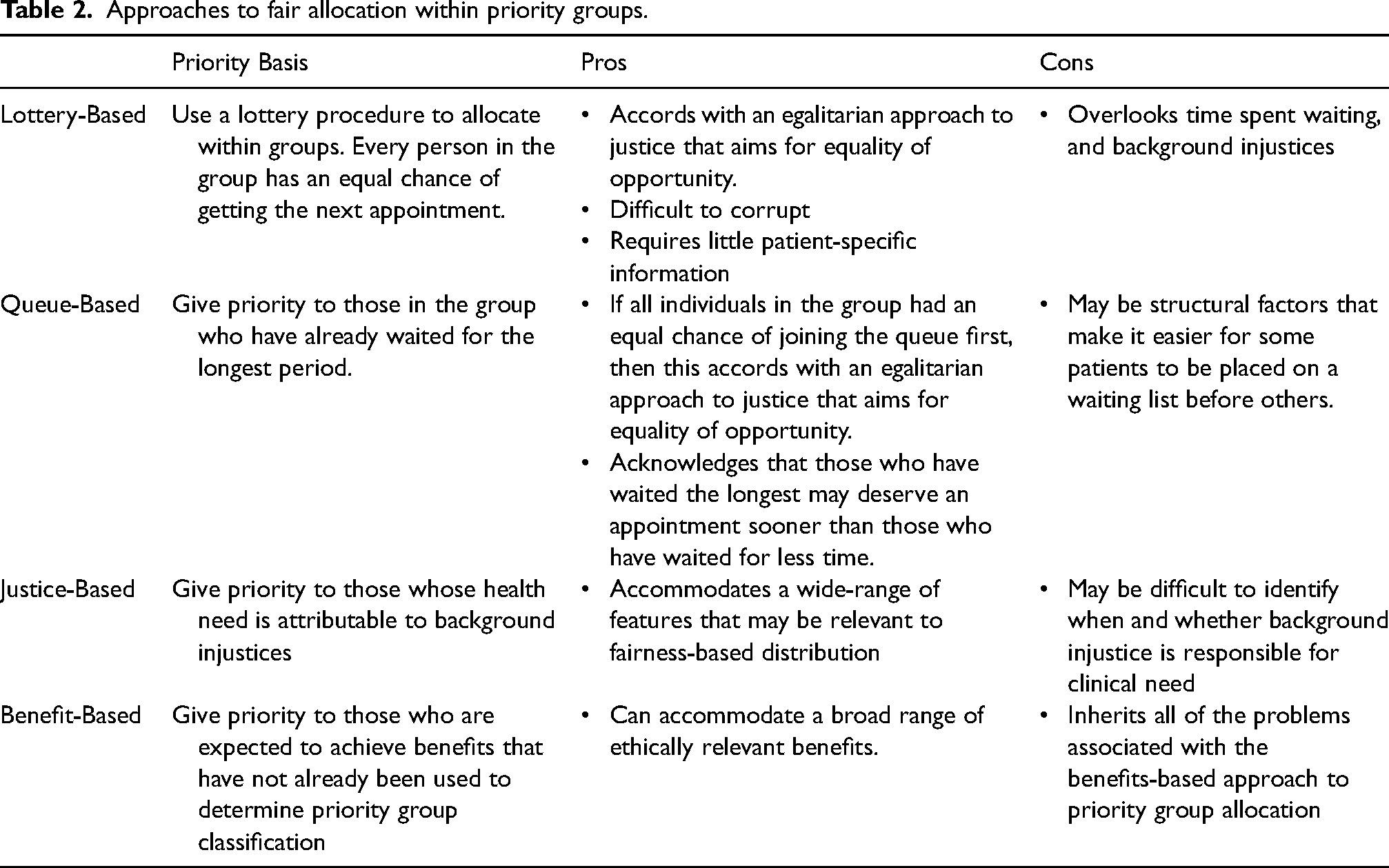
To apply these approaches to our test cases at the beginning of the paper, let us assume that test cases 3 and 4 were placed in the same priority group. The lottery-based approach would essentially flip a coin to decide whether who should get the first appointment between these two cases. The queue-based approach would prioritise the patient in test case 3 over test case 4, whilst the justice-based approach might prioritise test case 4 over test case 3, due to the structural barriers to care that this patient has faced.
Conclusion
The COVID-19 pandemic required healthcare systems to make stark prioritisation decisions in response to severe pressure on healthcare resources. In this context, the FSSA's guidelines for prioritisation provided an important and helpful framework for making prioritisation decisions about surgery in a timely and fair manner. However, we should not lose sight of the fact that these guidelines were developed as an expedient in a time of emergency. As we continue to move beyond the emergency stage of the COVID-19 pandemic, and face up to the daunting backlog before us, it is important that we ensure that surgical prioritisation guidelines enshrine the values that we believe ought to determine access to care in non-emergency circumstances. We believe that our analysis shows that maintaining an approach to prioritisation of elective surgical procedures, based primarily on severity of condition, is not a sufficiently nuanced way of balancing the moral reasons we have to address considerations of need, benefit, and fairness in this context, and all the complexities that involves. The revisions that are made to the existing guidance will ultimately have to be grounded by value judgements about how to strike the correct balance between these considerations; our hope is that our analysis will serve to clarify the ethical dimensions of these value judgements.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JP and JS were funded by the Research and Innovation, Arts and Humanities Research Council, UK Research and Innovation/Arts and Humanities Research Council (AH/V013947/1).