
Abstract
Introduction: Non-violent resistance, carried out by healthcare workers, has been a common phenomenon. Despite this and despite the issues this type of action raises, we know little about the healthcare workers who engage in this action and their perspectives about its justification. This exploratory study sought to address this gap, examining these fundamental questions amongst a sample of healthcare workers who have engaged in acts of resistance, exploring their understanding of non-violent resistance, its justification and the barriers they faced in engaging in such action. Methods: Participants were recruited through Medact's (https://www.medact.org/) member database and directed to an online survey hosted on Qualtrics. While participants were unlikely to be representative of the broader UK healthcare community, participants were in an advantageous position to comment on non-violent resistance. Descriptive quantitative analysis and a content analysis were conducted. Results: The majority of participants felt that non-violent resistance could be justified dependent on its cause and/or the action in question. Within this, most felt that if action were non-violent, that if it didn't harm patients and that if the issue in question had to do with health being compromised, action was often justified. A number of others framed their justification as being a right or duty to engage in non-violent resistance. In relation to barriers to engaging in non-violent resistance, these fell into three categories: personal, professional and broader concerns related to society or the general culture found in healthcare. Within these, time and concerns about registration or the consequences of engaging in action were cited as the greatest barriers. Conclusions: These results suggest that healthcare workers who regularly engage in non-violent action carefully thought through their actions, acknowledging the diversity of actions and issues that could be challenged, for many patient care remained a primary concern. There is a need for clarity from regulatory bodies and in particular the need for dialogue between healthcare bodies and healthcare workers who continue to engage in acts of non-violent resistance.
Background
Resistance as carried out by healthcare workers has been a common but largely overlooked phenomenon. We can find mention of agitation and advocacy for hygiene and sanitation throughout Europe as early as the 1800s. 1 Today, we can find numerous examples. Strike action has arguably been the most commonly discussed form of action in the literature and elsewhere,2,3 however, we can also find many examples of healthcare workers engaging in marches, vigils, open letters, hunger strikes, resignations, whistleblowing and civil disobedience. 4 Beyond these actions, the risks, context and stakes are vastly different. In the United States for example, healthcare workers petitioned against a Burger King that had been operating in a New Jersey hospital for 25 years. The store was subsequently closed in early 2021. 5 A few months later, a doctor published an open letter reporting that he had performed an abortion in defiance of a recent law passed in Texas that legislated a near-total ban. 6 Healthcare workers in Myanmar were amongst the first to take to the streets after the military seized power in a coup in early 2021. Concerned about working for the unelected government, many left their jobs and set up clinics out of sight from the authorities. 7 Such actions came with significant risk. By December 2021, it was estimated that over 10 months in Myanmar, there had been 355 acts of violence or obstruction against healthcare workers. This included 284 arrests, 113 raids of hospitals and 31 deaths. 8 In Sudan, again after increasing violence following a military coup, healthcare workers took to the street to protest against violence carried out by security forces, including attacks on hospitals and patients. 9 While we needn't look far for headlines of healthcare workers engaging in non-violent resistance, limiting our discussion to such acts is likely an underestimation of its prevalence. Often overlooked are the everyday acts of subversive behaviour, for example, a doctor providing care for undocumented migrants or a nurse who breaks the law to provide abortion care. 10 Such acts, while more difficult to quantify, are likely to be just as frequent, if not more so than public acts of resistance.
Despite its frequency and diversity, and the range of questions it raises – conceptual, normative, regulatory and perhaps more generally about the role of healthcare workers in society – with the exception of strike action, 11 resistance has received relatively little scholarly attention. As well as a dearth of literature, one consequence of this is that relatively little guidance for healthcare workers who engage in such action exists. For example, in the UK, the General Medical Council (GMC – the UK's regulatory body for doctors) has offered little clarity on whether healthcare workers could face disciplinary action for engaging in various forms of non-violent resistance. During the junior doctor strikes in 2016, the GMC made several veiled threats about doctors being potentially struck off if participating in the strike. 12 More recently and following the arrest of several doctors during a civil disobedience campaign to protest the lack of action on climate change, the GMC stated that in all cases they would ‘… make our decision based on the specific facts of the case’. 13
To date, these issues have not been explored with healthcare workers more generally and those who have engaged in acts of resistance. This exploratory study sought to address this gap with a sample of healthcare workers who have engaged in acts of resistance, specifically exploring their justifications for such action and the barriers they faced in engaging in such action.
Methods
Procedure and participants
Participants were recruited through Medact's (https://www.medact.org/) member database which contains the details of approximately 7000 healthcare workers and academics, both presently employed and retired who are largely based in the UK and Europe. Participants were directed to an online survey. Medact was formed in 1992 and is an organisation that seeks to ‘…work together towards a world in which everyone can truly achieve and exercise their human right to health’. 14 Medact has an active membership involved in the production of research and campaigning, mostly in relation to its four campaign areas which focus on peace and security, climate and health, economic justice and health and human rights.
While we have and will continue to refer to our participants as healthcare workers, we do not in any way want to imply this sample is representative of the broader healthcare community. Medact is an organisation that campaigns on political issues that impact health. While we did not ask about political views, it is likely that our sample were far more politically engaged and held more progressive views than the majority of UK health workers. 15 It is also likely that they engaged in protest actions far more regularly than others in the UK health community. In saying this however, given the nature of this sample, they were in an advantageous position to provide insight in relation to our research questions, namely in exploring the justifications for and barriers to engaging in non-violent resistance. As this survey was exploratory, we did not set a limit on the number of people who could participate, however from past engagement, we expected to get at between one and two hundred responses.
Survey and data collection
An online survey was hosted on Qualtrics and included participant demographics and several closed and open questions, including involvement in non-violent resistance. The results reported here focus on a series of questions related to healthcare workers’ justifications for non-violent resistance, and the barriers they faced in engaging in it. The survey was developed in an iterative fashion by the researchers over several months. We utilised the terminology of non-violent resistance/action in the survey as opposed to the more general term ‘resistance’. 16 We felt non-violent resistance would be better understood by participants and because of the fact that there are simply very few examples of healthcare workers engaging in violent acts of resistance.
Analysis
Descriptive quantitative analysis for the closed questions was conducted using SPSS 27. 17 Open questions were analysed using content analysis. This method counts the number of times a comment or theme arises and presents results using descriptive statistics supported by narrative from the data. The steps involved in qualitative content analysis, as described by White and Marsh 18 ; formulating a research question followed by coding and analysis. Coding involved reading through all responses to identify key phrases and segments of text, noting places of convergence and divergence. This continued iteratively until categories and sub-categories emerged. Initial coding was carried out by RE which resulted in a draft coding scheme. Secondary coding then involved all authors who revised this scheme, again employing an iterative approach until all authors agreed upon categories and sub-categories. While content analysis is often reported noting how many times a theme or issue was raised, given we are not making claims about generalisability we have opted to omit the precise number of responses for each theme or issue below.
Ethical approval
Ethical approval for this study was granted by the University of Greenwich University Research Ethics Committee (UREC/20.5.6.11)
Results
Sample characteristics and engagement in non-violent resistance
Overall, there were 148 responses to the survey. Age was relatively spread, however, the majority of participants were over the age of 65 (n = 45, 30.4%). Seventy-eight (52.7%) participants were identified as women, 46 (31.1%) as men and 4 (2.7%) as non-binary. The vast majority of participants indicated they were from a white background (n = 104, 83.9%), 12 (9.7%) participants indicated they were from an Asian, African, Caribbean or mixed background, while 8 (6.4%) participants indicated they were from other ethnic backgrounds. Professionally, the majority of participants were doctors (n = 77, 52%), nurses (n = 13, 8.8%) and healthcare academics (n = 8, 5.4%). Most indicated they held a senior position (n = 63, 42.6%) either now or prior to retirement. Thirty-three (22.3%) and 28 (18.9%) participants indicated they held a mid-level or junior role respectively. Fifty-five (37.2%) participants were retired.
An overwhelming majority of the sample had engaged in non-violent resistance, with 128 (86.5%) indicating they had engaged in some form of action (only 3 participants said no, while 17 skipped this question). Over 60% of participants (n = 81) indicated they engaged in non-violent resistance at least a few times a year. Participants were also asked about the types of activities they engaged in. Most participants participated in marches (n = 118, 79.7%), online activities (n = 104, 70.3%), lobbying (n = 80, 54.1%) and flyering/leafleting (n = 70, 47.3%). The activities least engaged in including whistleblowing (n = 25, 16.9%) and sit-ins (n = 34, 23%). Results are summarised in Figure 1.
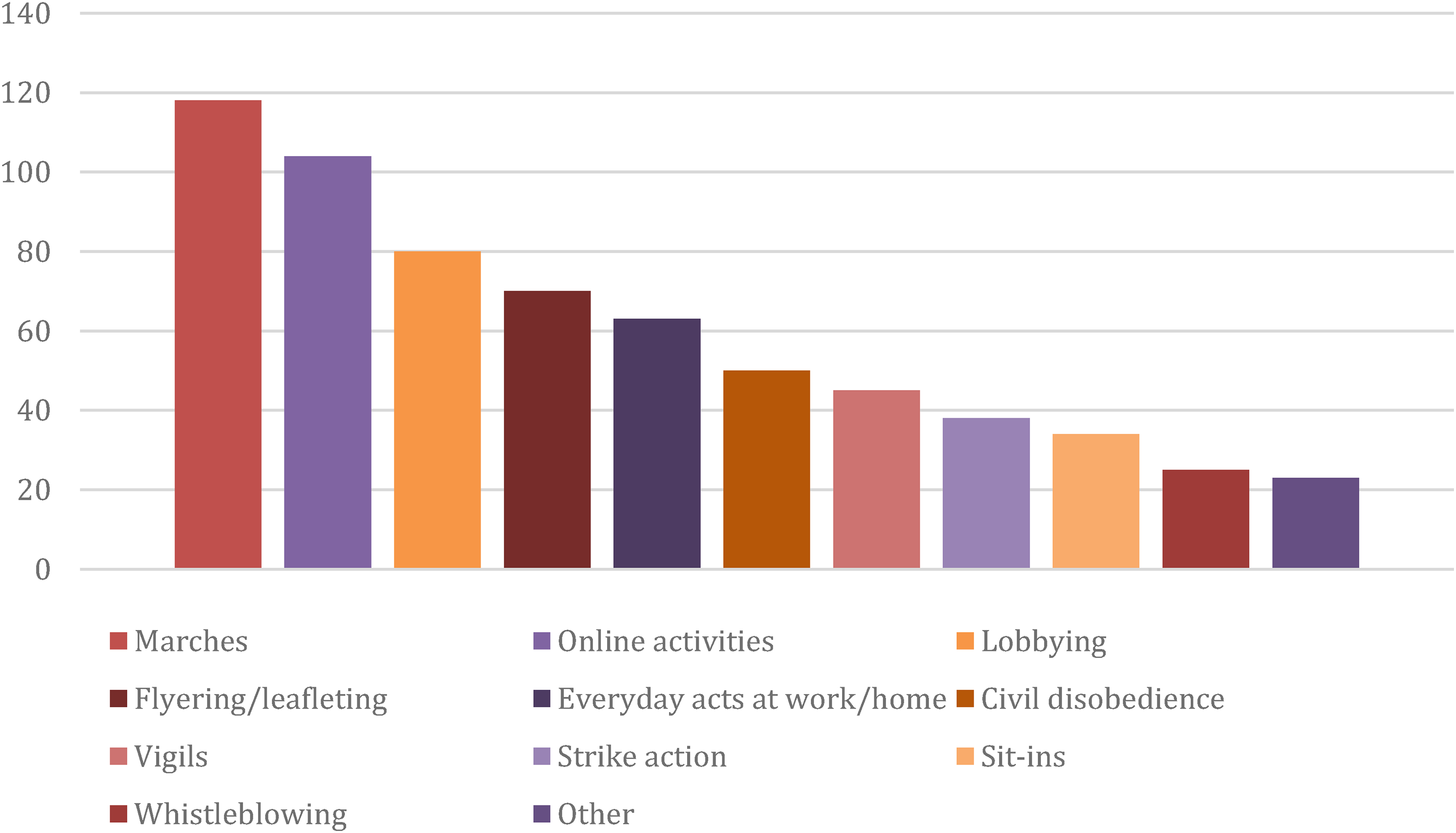
Number of participants and types of non-violent resistance that had been utilised.
Justifying non-violent resistance
Participants were asked if they felt non-violent resistance, when carried out by healthcare workers, was justified. Thirty-six (24.3%) participants thought it was always justified, 60 (40.5%) participants thought it was justified very often, 41 (27.7%) participants thought it was sometimes justified, while only 1 participant thought it was rarely justified. No participants felt that non-violent resistance was ‘never’ justified. Participants were then asked to elaborate on this question. Seventy six participants provided a response. Responses again fell into four main categories: (1) the right or duty to participate in non-violent resistance, (2) dependent on the cause or matter being resisted, (3) dependent on the action in question and (4) that healthcare workers were no different to others in relation to the justification of non-violent resistance. A summary of these results is included in Figure 2.
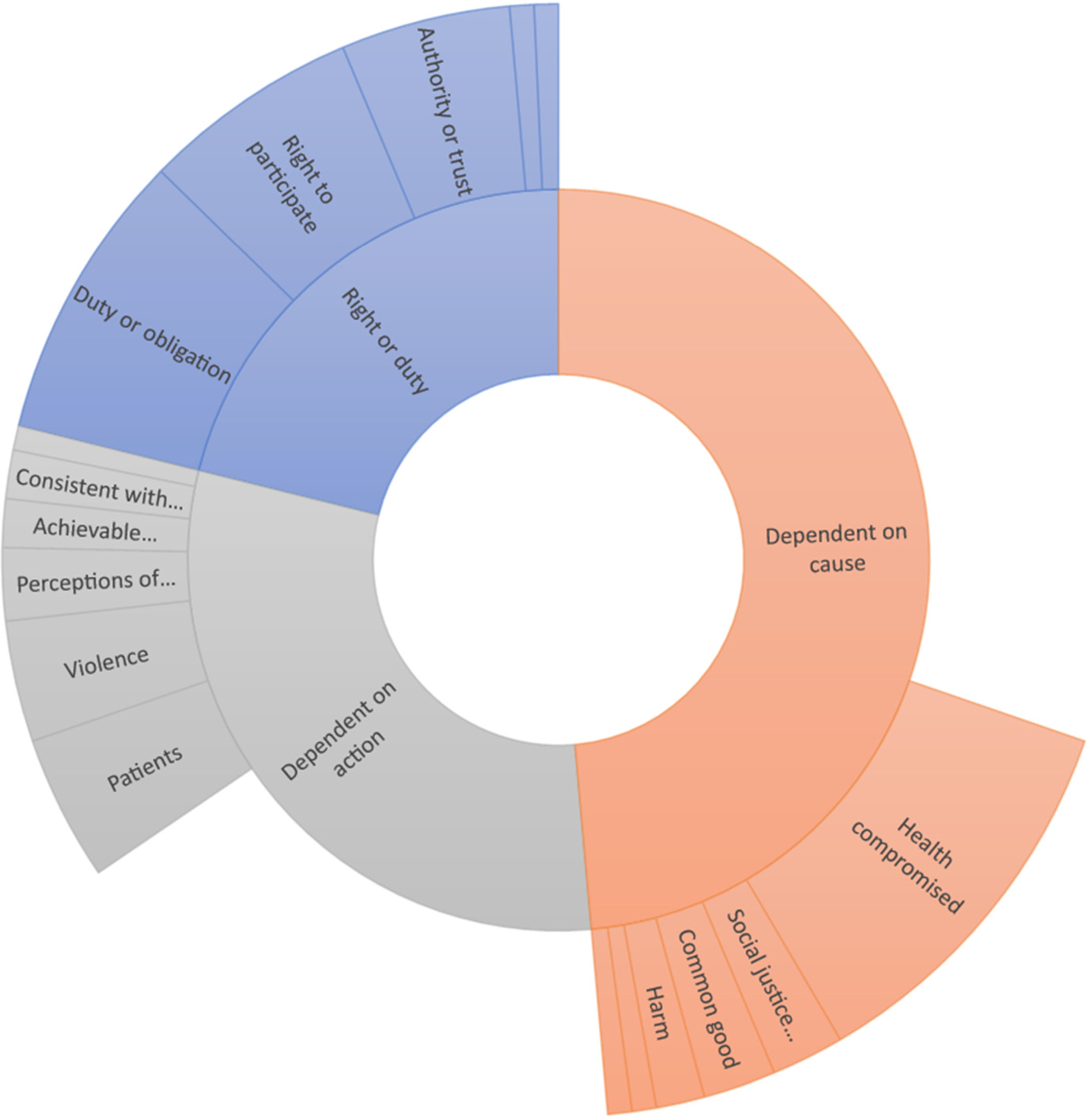
Sunburst chart of responses when asked about the justification of non-violent resistance.
The right or duty to participate in non-violent resistance
A substantial number of participants asserted that healthcare workers were either allowed or had a right to participate in non-violent resistance, however, not only felt that such action was permissible, but a duty or obligation. One participant noted that such action had support from figures in healthcare leadership roles, while one noted that such action could be justified on conscience. We all have a right, so far at least, to protest against poor/bad decisions and treatment. That healthcare staff should be denied this right, or deny themselves this right, simply plays into the hands of those who exploit them and their sense of vocation/service (Participant 20).
The cause or issue being resisted
Over half of the participants identified that the cause was important in assessing the justifiability of action. A number of participants offered more specific answers on this point, identifying causes where health or healthcare is compromised instances of more general harm to people or the environment and causes related to social justice or oppression. Militarisation and causes that were not motivated by self-interest were each noted by one participant respectively. Well it depends on the issue. people may resist or act for completely invalid reasons (Participant 147).
The stronger the link back to the health of people the more justified it is to carry out an action as health workers. e.g., the Climate emergency has enormous health implications and so HCP [health care professional] involvement is very appropriate; whereas an action to support an increase in the power of the richest 1% by HCPs would not be justified at all and would I’d suggest be a betrayal of trust (Participant 63).
The action
A substantial number of participants also identified the action itself as being important when considering the justification of non-violent resistance. More specifically participants identified that action should not harm patients, should not resort to violence or harm, should consider the perceptions of the public, should be a last resort, should have, to some extent, achievable outcomes, and should be consistent with healthcare ethics, while one participant felt the justifiability of action was at least somewhat dependent on the action's impact on others: I feel this depends on the context in which it is taken and the mode of non-violent action. Some actions may be seen as ‘too extreme’ in the eyes of the general public and therefore risk bringing the professions into disrepute if undertaken on a large scale. Similarly even small but overly conspicuous actions may have the same effect – if the actions of a select few are widely broadcast in the media for example. This could possibly undermine what I believe to be advantages of healthcare workers taking part in direct action (Participant 97).
Differences in justifying non-violent resistance
The final theme related to a series of responses that felt there was no or little difference in justifying non-violent resistance when compared to others. Several participants felt this was the case in some way. Health care workers are responsible for the health of their patients and it is their duty to take any action they feel necessary to protect them. They are also citizens in addition to being health care workers and have a right to protest peacefully about any issue that they feel strongly about (Participant 132).
Barriers to engagement in non-violent resistance
Participants were asked whether they felt that engaging in non-violent resistance was consistent with their professional codes, guidelines and regulations that guide professional behaviour. Twenty-six (17.6%) participants felt it was always consistent, 47 (31.8%) felt it was ‘very often’ consistent, 45 (30.4%) felt it was ‘sometimes’ consistent, while 11 (7.4%) felt it was rarely consistent. No participants felt that it was never consistent. Participants were also asked about how concerned they were about their professional registration if engaging in non-violent resistance. Seventeen (11.5%) participants indicated they were very concerned, 33 (22.3%) indicated they were moderately concerned, 37 (25%) indicated they were slightly concerned, while 43 (29.1%) indicated they were not at all concerned. A summary of these results is included in Figure 3.
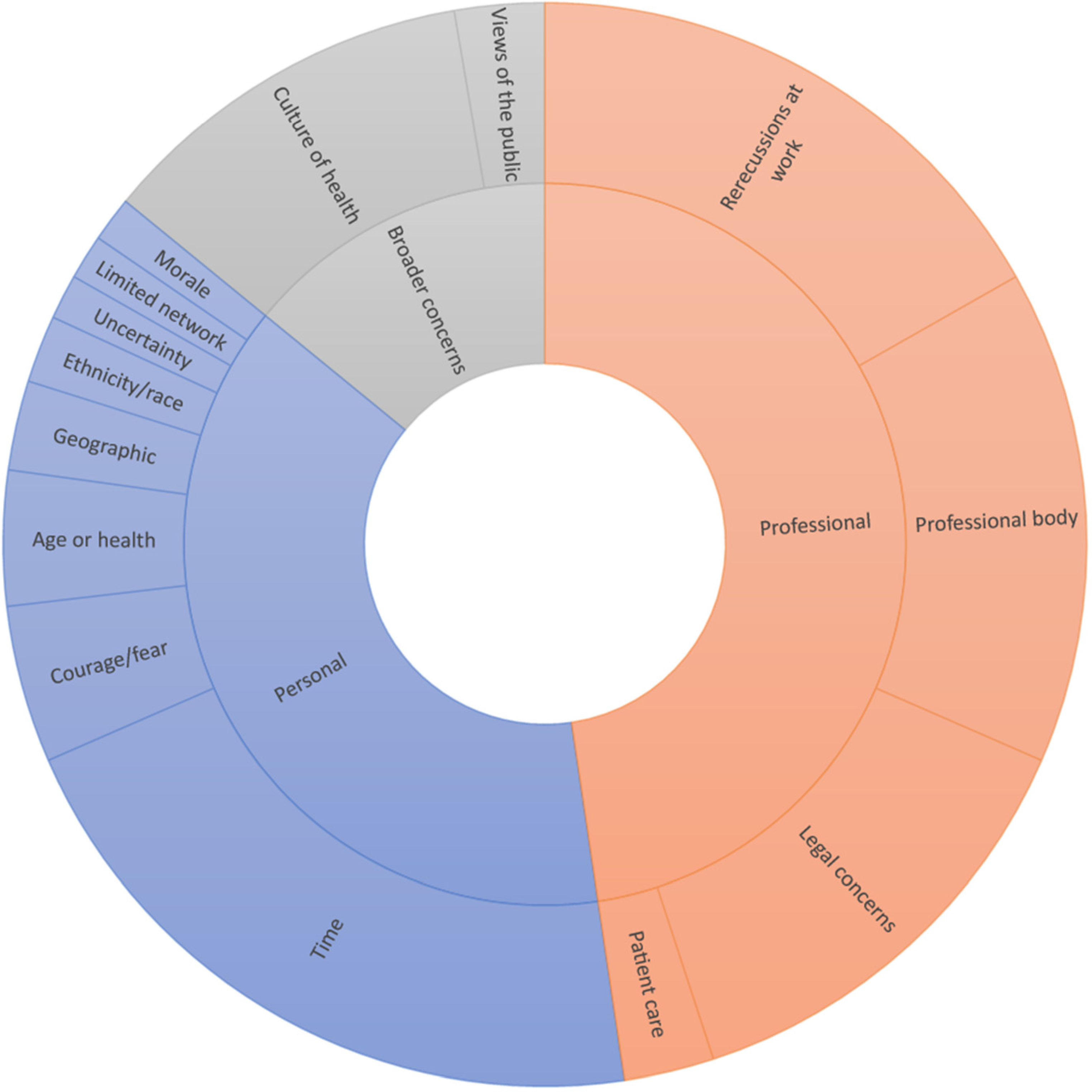
Sunburst chart of responses when asked about the barrier to engaging in non-violent resistance.
Following up on the above two questions, participants were asked to elaborate on what barriers they experienced in relation to engaging in non-violent resistance. Eighty-nine participants responded to this question and their responses fell into three categories: (1) personal reasons, (2) professional or work-related reasons and (3) broader concerns about how non-violent resistance is perceived.
Personal barriers
When it came to personal barriers, a substantial number of participants indicated that time was the greatest barrier to engaging in non-violent resistance. Fear about the consequences of such action, health or caring-related concerns, geographic limitations (i.e. an inability to travel to actions), ethnicity or race, morale, lack of a network to carry out actions and uncertainty about how to help or what to do were also cited as barriers. Race, as a black woman. I’d rather lay low than put myself at risk of any trouble that could jeopardise my further career (Participant 138).
I am also very concerned about the differential effect of race. A middle aged, white, middle class woman may not go to prison for a protest, a black young male may (Participant 43).
A lot of my colleagues don't have the time or capacity to engage in such endeavours – they’re just trying to live and feed their families. The system thrives off of this (Participant 112).
Professional or workplace barriers
The most cited concern related to professional or work-related barriers to non-violent resistance was the potential for repercussions at work, this included concerns about management not understanding such acts and possible detrimental impacts on career progression. A number of participants cited concerns about their registration or the fact that their professional body had not made their position clear on non-violent resistance as a barrier, while several others cited legal concerns, in relation to actions which might involve breaking the law or being arrested. While for some participants these legal concerns were framed as a personal barrier, the majority of participants framed this as a professional issue, potentially impacting on their registration and/or having repercussions at work. A smaller number of participants raised concerns about how non-violent resistance may impact patient care or relationships. Attitudes taken by local health service employers/NHS management may be inconsistent with the supposed freedoms of citizenship, for example more drastic limitations on free speech and behaviour are imposed on NHS employees during times of pre-election purdah (Participant 110).
I have engaged in the majority of non violence resistance whilst I was a medical student and now I am employed I have definitely felt a lot more reluctant to engage in protests that may have certain risks i.e., arrest/ police presence/ televised. I do have real concerns that if I was arrested this could threaten my medical career, and I think this is often a greater concern for junior doctors as we have a lot more of our career ahead of us (Participant 103).
The GMC is a significant barrier for myself and other doctors wishing to engage in non violent resistance. The further criminalisation of protest in the new [Police, Crime, Sentencing and Courts]bill will make it even easier for the GMC to suspend doctors who engage in non violent resistance. Although there is a strong argument for doctors acting in the best interests of the broader population by participating in protest and resistance (e.g., for climate change or access of refugees and undocumented migrants to the NHS) it is unclear whether this would stand up in the GMC and I fear that we will see healthcare workers silenced through fear of losing their jobs. I think it is a significant barrier to doctors organising and I hope that there is a path to some kind of agreement with the GMC in the future regarding this but I am unsure this is realistic (Participant 85).
How non-violent resistance is perceived more broadly
Several raised concerns about how non-violent resistance was perceived in healthcare more generally, with most noting that non-violent resistance was not understood by many of their colleagues, nor was it present in the culture found in healthcare more generally. A smaller number of participants raised concerns about the views of the public. Inability to predict how senior colleagues/management would respond and possible impact this would have on employment. E.g. possible response could be from support to indirect threat of disciplinary action, and even if you could successfully argue against this, it can be very stressful to be in an environment of colleagues who don't care/understand and would not back you up (Participant 141).
A lack of political education amongst HCWs [health care workers] is a serious barrier, often HCWs are encouraged to be ‘neutral’ ‘objective’ ‘apolitical’ by institutions and regulatory bodies and this discourages likelihood to engage with non-violent resistance (Participant 107).
Aside from concerns about registration I am also concerned about the disapproval of, or alienation from, colleagues. I have been involved in protest and civil disobedience but do not tend to talk about this at work to colleagues. I have colleagues who agree with various protest movements but do not think there is a role for healthcare professionals to play in these. Additionally I would be concerned about my patients finding out (Participant 98).
However, it does feel like the emphasis on the public's view of HCPs is sometimes used to silence HCPs from speaking out in defence of vulnerable patients/groups to on other important issues, but also generally engaging in protest action as a separate thing to their profession (Participant 15).
Discussion
There has been limited work that considers the justification of non-violent resistance amongst healthcare workers, and with little guidance on the topic, it remains a divisive issue. Some may agree that climate change is a pressing issue, yet disagree with civil disobedience as a tactic. Many will disagree with those protesting against vaccination and other public health measures, but agree that marches (in most cases) are a relatively contained form of protest that causes minimal disruption. We are unaware of any study that has explored the attitudes of healthcare workers in regards to the justifiability of non-violent resistance. The above results begin to address some of these questions.
On this point, it is worthwhile to first consider the literature on the justifiability of non-violent resistance, a literature which is somewhat limited. Childress 19 was one of the first to consider illegal actions in healthcare and specifically civil disobedience. Several questions are posed related to the ends of the action, whether it is a last resort, the possible consequences of the action (including its likelihood of success and the risks involved), and finally different types of ‘disobedience’, for example, violent and non-violent acts and so on. This framework has been applied elsewhere to consider civil disobedience in response to inaction on climate change 20 and illegal actions during the COVID-19 pandemic. 21 There has also been some discussion about the justifiability of strike action in healthcare, arguably the form of action that has been most commonly discussed and debated in the literature and elsewhere. Selemogo 22 for example, outlines several similar criteria to consider in strike action, including whether a strike demands are just, whether such action is a last resort and whether its risks are proportionate to its demands. In some ways, it is difficult to compare our findings as participants were asked a far broader question, whether non-violent resistance, more generally, was justified. There were, however, a number of notable similarities that could be seen in our data, regardless of the specific actions or issues that participants spoke about. For example, a number of participants spoke about action being a last resort, carefully assessing the risks in undertaking such action and one of the issues that have arguably been most pressing in the literature focused on healthcare strikes, 11 the impact of the action on patients and broader health and well-being.
Perhaps unsurprisingly, our sample felt that non-violent resistance was justifiable under many circumstances with a number of participants suggesting they felt that healthcare workers had a right or duty to engage in such action. In line with the above literature, a substantial number of participants felt that it was first necessary to look at the ends of the action, and some specified this may be most justifiable in circumstances where health or healthcare is compromised, there is harm to people or the environment or in addressing oppression or injustice. This focus on the ends of action, its demands or what its aims are is important. While many would agree with the examples of non-violent resistance provided to this point, there are a small number of examples where non-violent acts that have been carried out by healthcare workers that had questionable or completely unjustified ends. For example, doctors in Canada in 1934 went on strike when a Jewish doctor was hired. 23 More recently, healthcare workers have been involved in protests against public health measures, such as vaccines, lockdowns and face coverings. 24 While we can see behaviour that is completely unjustified in these actions, some intersect with a range of other discussions that remain pressing, such as the extent to which, or if health workers should be regulated on social media at all. 25 Beyond considering the ends of the action, a number of participants also identified the action itself as being an important consideration. A number said that the action should not harm patients and not resort to violence. Finally, some also noted that healthcare workers were also citizens, so felt there was little or no difference in the actions that healthcare workers could engage in when compared to other groups. This issue is something that has been raised elsewhere in the literature 26 (although has received not nearly enough attention), notably balancing the right of healthcare workers to protest as citizens and what they might owe patients and society as clinicians, such debates have been had in relation to strike action, where action has the potential to impact patients and more disruptive forms of action, such as civil disobedience. 27
Related to the question of justification, we also asked participants their views about the barriers to engaging in non-violent resistance. While related to the above questions, this question dealt more closely with the practical issues of professional registration. As we discussed above, in the UK regulatory bodies have long been reluctant to provide clear advice on whether such action may impact professional registration. 13 Most broadly, participants identified personal, professional and broader social concerns about their involvement in non-violent resistance. Time was by far the greatest personal barrier, followed by concerns about the consequences of the action, health limitations or personal caring responsibilities and even race, with a number of participants raising concerns about the differential impact that protest may have on those from minority ethnic backgrounds. These concerns have parallels elsewhere, for example. it has been well documented that in the UK doctors from ethnic minority backgrounds are far more likely to face disciplinary hearings. 28 Participants also had substantial concerns about the potential impact of such action in the workplace and on their career. A number raised concerns that the professional registration bodies in the UK (such as the GMC and Royal College of Nursing) had not made their position clear and were thus worried about being deregistered if engaging in such action. A substantial number also raised concerns about the legality of such action, notably breaking the law or being arrested. When participants raised legal concerns they were often closely related to their professional regulation and career progression, rather than opposition to law-breaking, per se. These concerns are well founded, while in the UK there have been no doctors who have lost their registration after being involved in civil disobedience demanding greater action on climate change, 29 there remains little clarity from regulatory bodies about their position on such action. Interestingly a large number of participants also raised concerns about how such action may be perceived more generally by colleagues or the public, suggesting that such action was not the norm and that more generally there was a lack of awareness about such action in healthcare. It also suggests that a number of participants felt somewhat isolated in relation to this type of action, not having colleagues who would understand or support their actions. Given the nature of our sample and what is known about the broader political attitudes of NHS workers, this is perhaps unsurprising. 15
In saying all of this, some caution is warranted in interpreting our results and a number of limitations are worth noting. First and foremost our sample cannot be considered representative of all healthcare workers. Our sample was primarily based in the UK, were recruited through Medact, a campaign organisation and most were engaged in some type of non-violent resistance. These participants offered a depth of knowledge and experience that other healthcare workers may not have had in relation to non-violent resistance, this however does limit the generalisability of our findings. That is, our findings represent the views of what are likely a small group of healthcare workers who are generally politically progressive and politically active, including many who regularly engaged in various forms of protest. While we feel these results are valuable in beginning to explain the views of healthcare workers who engage in this type of action, care is therefore needed if seeking to apply these results elsewhere. In addition to this, a substantial number of people in our sample were retired. This may have impacted perceptions about barriers and justifications for action. Finally, the way the questions were framed in our survey was quite general. Clearly, a strike raises different normative issues than a sit-in, for example. We did not ask about specific acts of resistance, however, this is something that should be considered in future studies. On this point, it is worth noting that there is already an existing body of work that details the health workers attitudes towards strike action, 30 we are not aware of any other work that has attempted to explore more specific forms of resistance amongst healthcare workers.
These results suggest that amongst a sample of healthcare workers who regularly engage in non-violent action, these acts are often carefully thought out; very few in this sample indicated that non-violent resistance could be justified in all circumstances acknowledging the diversity of actions and issues that could be challenged, for many patient care remained a primary concern when considering such action. These results speak to the need for clarity from regulatory bodies and in particular the need for dialogue between healthcare bodies and healthcare workers who continue to engage in acts of non-violent resistance. Given the long history and frequency of such action in healthcare, the important causes it has championed and its relative effectiveness in achieving health and social gains, 4 it is surprising that these conversations are yet to be had.
Supplemental Material
sj-docx-1-cet-10.1177_14777509231156050 - Supplemental material for Justifying non-violent resistance: The perspectives of healthcare workers
Supplemental material, sj-docx-1-cet-10.1177_14777509231156050 for Justifying non-violent resistance: The perspectives of healthcare workers by Ryan Essex, Hil Aked, Rebecca Daniels, Paul Newton and Sharon M. Weldon in Clinical Ethics
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.