
Abstract
The question of whether donors should be able to set conditions on who can receive their tissue has been discussed by bioethicists, but so far there has been little consideration of whether the answer to this question should be different depending on the type of tissue under discussion. In this article, we compare the donation of organs with the donation of reproductive material such as sperm, eggs, and embryos, exploring possible arguments for allowing donors to set conditions in one case but not the other. After considering arguments from procreative liberty, special parental obligations, and donors meeting their genetic offspring, we find that there is no ethically defensible reason to have different policies between these two cases. As a consequence, we conclude that jurisdictions operating with this inconsistency should consider moving their policies into better alignment. We also make some recommendations for the standardisation of the terminology around conditional donation.
Introduction
When people donate human tissue, it is not unusual for them to state preferences over who the eventual recipient(s) of that tissue should be. Placing conditions on donations raises ethical issues that have, in the past, caused significant controversy. Donation systems have policies to determine how conditional donations should be approached, and in the United Kingdom, donation systems for different tissues have different approaches. In this article we consider whether there are sufficient differences between two types of tissue – organs and gametes – to justify these differences in approach to conditional donation. We will outline three putative reasons to support different approaches. First, gametes and reproductive material afford the donor special procreative liberties that do not exist in the context of organs. Second, gamete donation generates special parental obligations that require us to afford donors a greater degree of control over their donated material; and finally, the differing possibilities for donors to meet those brought into existence using their tissue. We will argue that none of these reasons is sufficient to justify treating organs and gametes/embryos differently when it comes to accepting conditions set by donors.
Definitions
Since the arguments above are concerned with gametes that are used to create new people, our interest is specifically in gametes donated for reproductive purposes, for example in the context of treating infertility. Our discussion therefore does not touch on the context of gametes or organs donated for research purposes.
We define conditional donation as any tissue donation that involves a stipulation by the donor regarding who can receive their tissue. True conditional donation occurs when the donation is contingent upon the condition being met. Within this broad definition there are sub-types of conditional donation. Confusingly, distinctions are made in the literature between ‘conditional donation’ and other types of donations that also count as conditional donation. For example, organ donation literature describes ‘conditional’ donation in opposition to ‘directed’ donation, where conditional donation means restricting donations to different types or groups of people (e.g. along racial lines, or lifestyle factors like alcohol consumption), and directed donation means naming a specific individual to whom the organ must go. Looking at Frith and Blyth 1 on embryo donation, the waters are muddied further because they take ‘conditional donation’ to mean ‘those who have frozen embryos ‘specifically selecting’ to whom they will donate their embryo’ (p. 318). They contrast ‘specific selection’ with ‘blanket conditions’ to distinguish conditions identifying a particular individual, and more general conditions. Frith and Blyth's use of ‘conditional’ is therefore distinct from the broader, groups-based meaning of ‘conditional donation’ when used in the context of organ donation.
Another complication is the use of ‘known donation’ in the literature on gamete allocation. This means donating gametes to someone known to the donor, although the extent to which the donor and recipient can be said to know each other varies. This term presumably originated out of a desire to distinguish donations between, say, friends and family members, from donations to strangers on the waiting list. However, given that patients can recruit donors using the internet, newspapers, or television adverts, it is unclear that these should be described as ‘known donor’ situations, given that they raise different ethical issues from situations of donating to friends and family.
Given that the purpose of this article is to consider the concept of conditionality across different kinds of tissue donation, we will use consistent terminology. We therefore propose that ‘conditional donation’ be taken to mean any donation where the donor sets conditions. Following Frith and Blyth, we will ignore the fact that all donations are conditional in the sense that there are always conditions imposed by other parties, such as the clinics where the treatment takes place, higher-level organisations that set eligibility criteria for treatment, and groups that allocate limited funding across various treatments. Relevant legislation, too, might even be regarded as setting conditions on donations.
Since ‘directed donation’ may cause confusion given that donations may be said to be ‘directed’ towards particular groups, we will not use this terminology, as it means essentially the same thing as ‘conditional donation’. Instead, we think that ‘identified donation’ captures the key features of this type of donation: that it involves the identification of a specific requested recipient, whether this is an individual that the donor knows, somebody that they have met through that person's solicitations for tissue (e.g. through social media), or someone picked from a list of possible recipients that is given to the donor. Contrasting with this, conditional donation that involves limiting the donation to certain groups or types of people ought to be referred to as ‘non-identified conditional donation’, to emphasise that while there is no identified individual to whom the donor wishes to donate, the donation is still proposed to be made with conditions attached. In Frith and Blyth's terminology, the difference between conditions that restrict the ‘type’ of person and ones that are directed to particular, identified individuals is the difference between ‘specifically selecting’ a recipient and putting ‘blanket conditions’ 1 on the donation (p. 318).
Background
There has been extensive debate over the permissibility of different kinds of conditional donations,2–4 but the fact that policy on conditional donation varies depending on what kind of human tissue is under discussion has been largely unexplored. There is literature on conditional organ donation, and to a lesser extent on conditional donation of gametes and embryos, but these different tissues are never considered together. Those who believe that conditional donation is always impermissible (e.g. for reasons of equality and non-discrimination) will, by extension, agree with our argument against a difference in policy between these domains. But our purpose here is to argue that irrespective of one's overall view on the permissibility of setting conditions, there is no justification for a difference between setting conditions on organs and setting conditions for gametes.
Given that the UK context is one in which there are differing policies between organs and gametes regarding the permissibility of condition setting, we will use this setting as a starting point for the discussion. However, the argument that follows applies to any jurisdiction in which organ and gamete donation are permitted.
Organ donation and gamete donation operate as two separate systems in the United Kingdom, and are governed by different legislation and organisations. Organs fall under the remit of the Human Tissue Authority (HTA) and the Human Tissue Act (2004) 5 and the Human Tissue (Scotland) Act (2006) 6 (‘HT Acts’) (additional legislative changes have been made in England, Scotland and Wales to incorporate each nation's system of deemed consent). Gametes fall under the Human Fertilisation and Embryology Authority (HFEA) and the Human Fertilisation and Embryology Act (1990) 7 and its 2008 amendments 8 (‘HFE Act’). There are, of course, differences between organs and gametes, in terms of the natures of the donated materials, methods of donation, and that they are governed and regulated by different agencies. The question that we aim to answer is whether these differences can justify different approaches to conditional donation. We will now outline the different stances on conditional donations and will examine some arguments that potentially justify these differences. We will argue that these justifications are unconvincing, and that the differences between the two systems therefore lack sufficient justification.
Conditionality and organ donation
Organ donation comprises two sub-systems: living and deceased donation. Each has a different stance on conditionality.
Deceased organ donation
Most organs are donated by deceased donors, where organs are transplanted from a cadaver to a living individual. Conditional deceased donation of organs was prohibited in the United Kingdom following a case of non-identified conditional donation in 1998 when a donor’s next of kin requested that his organs were only allocated to white people. 9 There had been no specific guidance on conditional donation before this. The organs were accepted and allocated to white people (who, by coincidence, would have received the organs even if restrictions had not been placed), but this decision proved controversial. This controversy prompted a Department of Health investigation, and the subsequent report prohibited all (identified and non-identified) conditional organ donations. The report stated that ‘to attach any condition to a donation is unacceptable, because it offends against the fundamental principle that organs are donated altruistically and should go to patients in the greatest need’. 10 Very similar phrasing was adopted by NHS Blood and Transplant in their organ allocation policy. 11
This general prohibition remained in place until 2010, when further guidance permitted, in exceptional circumstances, consideration of what NHS Blood and Transplant refer to as ‘requests for directed allocation’. 12 This was then incorporated into the NHS Blood and Transplantation allocation policy. 11 Requests for directed allocation can only be considered when they identify a named individual who is a relative or friend of long standing. The guidance also states that the donation cannot be contingent upon the request being granted. If there is a patient on the waiting list with a particularly urgent need, the request for directed allocation may be ignored and the organs allocated to that patient instead.
Living organ donation
Living organ donation in the United Kingdom normally takes the form of healthy people donating an organ (normally a kidney, but sometimes a liver lobe) to family or close friends. In our terminology, these are identified donations, where organs are donated on the understanding that they will be allocated to a specific individual. Unlike deceased organ donation, it is considered acceptable for the donation to be contingent upon the direction being granted, although some donors may agree that if their chosen recipient proves unsuitable at the last minute, then the organ can be allocated to another patient.
Recently, ‘altruistic’ donation has been permitted, and this takes two forms: non-directed and directed. In non-directed altruistic donation, a person donates an organ which is then allocated according to nationally agreed criteria, which increasingly means that they are used to start chains or pairs of donation between otherwise incompatible donor/recipient pairings. 13 In directed altruistic donation (in our terms, identified donation), a person is permitted to donate an organ to a specified individual, but no pre-existing relationship is required. Directed altruistic donation is often facilitated by social media platforms where potential recipients can advertise for willing donors. Although there is potential for donors to identify specific recipients based on the type of person they are, donors may not overtly specify that they only want their donation to be given to a certain type of person.
Conditionality and gamete donation
Gamete donation is not split between living donation and deceased donation like organ donation. (It is also possible to donate embryos, but for simplicity we will refer to gamete and embryo donation together under the umbrella term ‘gamete donation’. There do not appear to be any differences in policy between gametes and embryo donation.) In large part, donated gametes come from living donors, although there have been cases of what could be described as deceased gamete donation: for instance, Diane Blood used sperm from her deceased husband to have children. These cases were ultimately resolved by patients going abroad to have treatment, because deceased gamete donation remains forbidden in the United Kingdom. The question of whether it should be allowed has been discussed elsewhere.14–16
There are, however, still two systems of gamete donation because there are two types of gametes: sperm and ova (eggs). The HFEA does not appear to differentiate between these two types of gametes when it comes to their stipulations on conditionality. For our purposes here, we will consider sperm and eggs together, and take gamete donation as a whole.
Regarding conditions, gamete donation is more permissive than organ donation. The HFEA consent forms for gamete donation include a question asking whether the donor wishes to place any restrictions on their donation.17–19 The question does then go on to suggest ‘e.g. a specified named recipient’, but the donor is still free to place other restrictions if they wish: according to an HFEA Ethics and Law Advisory Committee (ELAC) report on conditional donations, the most common types of restrictions tend to focus on excluding single women, same-sex couples or older women. This report also states that ‘[t]he majority of centres felt that donors should be permitted to place restrictions on the use of their donation’, 20 suggesting that practitioners tend to support this policy.
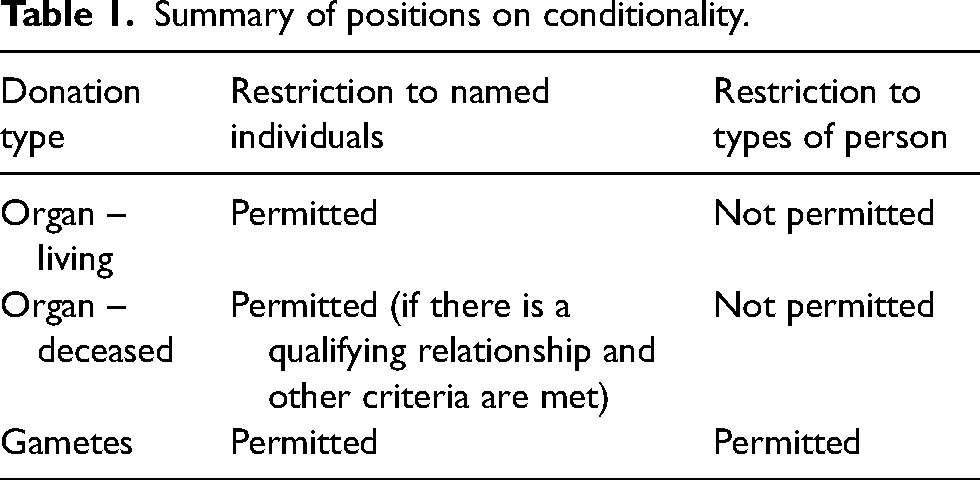
Summary of different positions on conditionality
Table 1 summarises the differing policies on conditions and directions. These policies are the result of legislation that either forbids or allows each practice, and of clinics’ working practices. The table therefore reflects the landscape of choices a UK citizen can expect when considering donating organs or reproductive material. The primary difference is clear: restricting recipients of a donation to certain types of people (non-identified conditional donation) is seemingly considered acceptable for gamete/embryo donation yet completely unacceptable for organ donation.
Summary of positions on conditionality.
Discussion
Ethical arguments for a difference in policy
We will now consider three putative reasons for these differing policies. These have been selected as they relate to the most salient difference between organ and gamete donation: that when one donates organs, one helps somebody who already exists to stay alive, whereas when one donates gametes one helps to bring someone else into existence (as well as helping existing people with their desire to have a child). We do not specifically critique arguments for or against conditional donation in general (e.g. arguments on the basis of altruism, or consideration of the Equality Act, which apply equally to organs and gametes), as we are focussed on whether there should be differences in policy, rather than precisely what the policy should be.
The argument from special procreative liberty
One reason commonly presented in favour of conditional donation is respect for the donor's autonomy.2–4,21,22 Just as respect for autonomy requires allowing people a choice about whether or not to donate, it may also justify giving donors control over other aspects of donation such as choosing recipients.
Procreative liberty is the extension of autonomy considerations into the reproductive domain, and its least controversial tenet is that people have a right to decide whether or not to reproduce. In an effort to cast procreative liberty's net more widely, Robertson claims that ‘some activities seem so closely associated with, or essential to, reproductive decisions that they should be considered part of [procreative liberty] and judged by the same standards’. 23 For Robertson, included in this are decisions about who to reproduce with, or more applicable to conditional donation, decisions about the type of person to reproduce with. It seems likely that the concept of procreative liberty arose in the context of non-assisted reproduction, where people are considered free to choose who they reproduce with. Some of the intuitive appeal of this libertarian position appears to have been straight-forwardly transferred to the realm of assisted reproduction, to make the equivalent claim that parents should similar choice in this setting too.
It is not clear that this translation is legitimate. Procreative liberty, as described by Robertson, is a negative liberty. This means that justification is required for interference with a person's reproductive choices. With regard to the type of person with whom one reproduces, such a negative approach might condemn, say, a policy that prohibits reproducing with someone of a different ethnic origin, as this would interfere with people's choices. The donation of gametes or embryos, on the other hand, brings a third party into the proceedings, and it is no violation of this negative liberty to fail to facilitate choices about the ethnic group with which a person wishes to reproduce. Instead, to say that one must facilitate these choices (as, say, a clinician working in a fertility clinic) is to bring procreative liberty into the realms of the positive.
Even an account of liberty like Shue's, 24 which proposes that negative liberties necessarily have correlative positive elements, would not go this far. Shue argues that all negative liberties have attendant positive social liberties so that, where a duty of non-interference exists, other people have a positive duty to enforce non-interference. In this way, a third party is brought into proceedings even in cases of so-called negative liberty. However, the extent to which the negative duty entails positive duties for third parties is limited, even under Shue's account. In the reproductive case, all this would mean that there is a general social obligation to uphold and protect others’ negative reproductive liberties – for example, to protect people from involuntary sterilisation or pregnancy, or perhaps to uphold and defend laws that allow for reproductive liberty. But it is not clear that a general societal positive duty to defend violations of negative liberty means a general positive duty to facilitate any and all reproductive choices. Importantly, Shue's account is only intended to apply to basic rights – that is to say, rights that, if unfulfilled, preclude the enjoyment of most other things. This includes the right to physical safety, and rights to subsistence. While the frustration of reproductive rights can clearly interfere with a person's wellbeing, there is a necessary connection between safety and subsistence and the enjoyment of other things that is not present in the case of reproductive freedoms. Reproductive freedom is not a basic right under Shue's account, so it may not be a candidate for the kind of negatively derived positive right that he describes.
The idea that negative reproductive rights should entail a general duty on others to facilitate other people's reproductive choices in a clinical context moves beyond the spirit of Robertson's procreative liberty. A person may have the right not to be silenced in voicing their unpleasant and unfair views, but this does not generate a corresponding duty on anyone else to facilitate that person's voicing their views. Whatever one thinks about the putative distinction between acts and omissions generally, the invocation of procreative liberty necessarily generates this distinction, because if positive and negative liberties are not distinguished in some way and are therefore treated as equal, we have no way of negotiating situations in which a person wants to reproduce with someone who does not want to reproduce with them. One person's positive right to reproduce with someone of their choice conflicts with that person's negative right not to reproduce with the first person, and clearly in this case the negative right should win out. We cannot characterise allowing conditional donations as the protection of some negative liberty on the part of the donor, since this generates positive duties on the part of treating clinicians that are unacceptably demanding.
There is no equivalent specific liberty described in the literature for organ donation, possibly because organ donation and transplantation are things that require interference in order to take place. This places them always in the realm of acts rather than omissions in that there must always be some form of clinical or governmental intervention, and therefore in the realm of positive liberty rather than negative. Organ donation and transplantation requires the type of infrastructure, resources, and expertise that, in the United Kingdom at least, make it essentially reliant upon the NHS. Some people have still argued in favour of organ donors having the opportunity to exercise their autonomy, 25 but there is more acceptance that when someone donates an organ, they should relinquish control over allocation.
The argument for conditional gamete/embryo donation on the basis of procreative liberty may fail if we take the distinction between positive and negative liberty seriously. We must at least be suspicious of carrying over intuitions from the domain of negative liberty to that of the positive, and we may have to acknowledge that where third parties are involved, putative parents’ liberty to choose where their gametes go should be further curtailed.
Special Procreative Liberties from the Genetic Connection
Another argument for procreative liberty's enjoying a special status, one that makes it different from liberty in the domain of organ donation, is that specific liberties exist relating to the genetic connection between donor and donor-conceived child. Passing on genes has significance beyond a single generation, whereas with organ donation, no genetic component is passed on to future generations. With gamete and embryo donation there is the possibility that the genetic offspring will themselves reproduce, effecting a chain of events through which the donor's genetic material is propagated for many years into the future. This is not so with donor organs – the organ dies with the recipient, and the genetic connection does not pass on to the recipient's offspring.
There is a strong cultural attraction to genetic reproduction, and some authors have articulated reasons for the value of genetic relatedness in reproduction.26,27 The fertility sector may operate with a somewhat confused and inconsistent framework when it comes to the importance of the genetic connection. Genetic relatedness is prized to the extent that an individual or couple will only use donor gametes if there is a strong reason not to use their own, and there is a general presumption in policy and practice that a person's own gametes are used as a default; but at the same time, no one would want to tell a person or couple using donor gametes that the value of their relationship with the child will be lessened to any extent because of this. The worst example of this might be a case where one member of the couple is using their own gametes and the other is not. These problems lead us to take the Brighouse and Swift view in this context: that the actual goods of parenting lie in the experience of socially rearing a child, rather than merely passing on one's genes. 28
Arguing for the special status of genetic material in the context of fertility treatment may also give rise to undesired motivations for people to become donors, as someone who wishes to donate just to propagate their genes may be considered vain or even as having eugenic motives. Indeed, such motivations would be at odds with the language used by the HFEA in describing gamete donation, as on their website it is described as an ‘amazing, selfless act’ 29 and ‘an extraordinary act of kindness’. 30 While the HFEA's position is not a knock-down argument against conditional gamete/embryo donation, it suggests that there is at least agreement between them and the literature that the genetic connection is not what gives rise to parental rights. The suggestion that parental rights should be transferred from parent to donor is therefore misplaced: parents may have specific liberties regarding the children they rear, but this does not entail that a gamete or embryo donor has such rights. It is our view that, correspondingly, more would need to be done to show that the genetic connection gives rise to rights to set conditions on donations. The social view of the goods of parenting, from Brighouse and Swift, has been described as ‘nearly axiomatic […] in bioethics’. 31 While that description may be an exaggeration, we have shown that at least in this specific context, there are difficulties associated with operating under that view. So, while that view might have given rise to a justification for allowing conditions in the reproductive case, the corollary issues associated with it mean that it must be rejected here.
Does gamete donation generate special parental obligations?
Another potential ethical justification for allowing conditions over gametes but not over organs is that gametes generate special parental obligations, contrasted with parental liberties described above. Here, rather than the mere fact of procreation being what drives a difference, the idea is that there is something special about parenthood that means a person's responsibilities towards their offspring rather than rights over them. This moves the focus of concern away from the parents and their procreative autonomy, and towards the person being created as someone over whom a person must discharge certain duties. These considerations look more consequentialist than the claims discussed in the previous section regarding procreative liberty, as they seem to be grounded at least in part in the welfare of children rather than in the autonomy of parents. One may nevertheless wish to posit deontological-looking considerations at play here regarding the relationships between people and their offspring, so that the consequentialist considerations are constrained by these special relational duties.
Because of these duties, then, it is not just permissible for parents to set conditions, but it is obligatory. There is, however, disagreement about how parents should discharge these obligations. It is in this context of disagreement that variation occurs, and ultimately it is left to the individual parents to decide how exactly they discharge this obligation. The resulting picture, then, is that donors, as prospective parents, have control over where their gametes go, not as a special procreative right, but as part of their general parental obligation to secure a certain type of life or of wellbeing for their offspring, and that there is considerable latitude in how they do this. Conditions may therefore be set in this special case. In the case of organs, which are devoid of the concept of this special obligation, there is no requirement to provide donors with this degree of control, and it is therefore legitimate to curb their ability to set conditions.
In the previous section, we touched on the idea that the goods of parenting lie in child-rearing rather than in child-creating. A case could be made that, if this is so, then the obligations of parenting fall to those who parent the child socially (i.e. raise them), rather than those who causally bring them into existence via donated gametes but have little or no other relationship with the child.
Whether one subscribes to the idea that special obligations arise from parent–child relationships will vary depending on one's theoretical worldview: certainly, one can imagine deontological duties arising from this relationship, or there being virtues pertaining to parenting, and indeed certain agent-relative conceptions of consequentialism may also make room for parenting obligations.
The key feature of these special parental obligations from child-rearing in the context of donor gametes is that they may serve to negate the putative obligations held by the donor. The point is not that the social parents of the child have obligations in addition to the obligations of the genetic parent, the gamete donor. The point is that the mere genetic parent does not have these obligations because they lie solely and exclusively with the social parent(s).
We do not take the view that social parenting obligations serve to totally obviate the obligations of those who donate gametes. We agree with Prusak 32 that a gamete donor must be held at least partly responsible for their decision to donate gametes and what follows from that action. The positive consequences (e.g. to the recipient family) are at least part of what speaks in favour of the action of donating gametes.
Nevertheless, the same is true of organ donors – this action also has consequences, and it is incumbent on potential donors to consider them. Indeed, it is the putative good consequences (saving lives) that drives organ donation and provides the rationale for participating in it, so consequences are clearly relevant. Since the question whether to donate an organ at all is an ethical question insofar as the outcomes of each option differ and therefore matter morally, there may be ethical questions surrounding the manner in which this action is taken. The similarities between organ and gamete donation, then, are greater than normally presumed, insofar as the duties that are derived from consequentialist considerations apply to both domains. An argument needs to be provided for why the relationship between parent and child generates duties – the deontic ones that do not relate to consequences – that would in turn allow for conditions to be set in that domain and not in the organ donation domain.
Therefore, while there may be disagreement on the nature of the obligations befalling potential gamete donors compared to potential social parents, it is still plausible that obligations befall gamete donors and organ donors alike. This similarity casts doubt on the presence of a morally relevant distinction between gamete and organ donors when it comes to setting conditions.
Gamete donors can meet the people created from their donations
The final argument we will consider is that the possibility of a gamete donor's meeting the people who are created by their donation justifies giving gamete donors greater choice. Living organ donors can, and do sometimes, meet their recipients, and those who donate after their death could meet (albeit pre-donation) the eventual recipients of their organs in rare cases of identified conditional deceased donation. It is rarer for gamete donors to meet the recipients of their gametes, perhaps due to a desire to maintain family units that are structured around the idea that the recipients are the definitive parents of the child.
As with the previous arguments, the difference in the gametes case rests on the existence of the third party that is the offspring resulting from treatment. This argument might be considered a special version of either of the two previous arguments, if the possibility of meeting the child generates special obligations or liberties. Given that it could be argued that the possibility of meeting the child is important for either one of these reasons (obligations or liberties), this example deserves its own discussion.
The degree to which it is possible for a donor to meet a child varies between jurisdictions. Where donation of gametes occurs anonymously, such a meeting is unlikely. However, in jurisdictions where anonymous donation is prohibited (such as in the United Kingdom, where donor-conceived children conceived from gametes donated on or after 1 April 2005 will receive information about their donor when they are 18), we can expect meetings to occur. Such a meeting is likely to be fraught with ethical considerations, as donors and donor-conceived children may have a range of ideas about the importance/unimportance of their genetic connection, and differing expectations about their future roles and relationships.
These meetings have the capacity to be sensitive affairs. Our question, however, is about the stronger claim that the possibility of such meetings provides a reason for donors to have greater choice over the recipients of their gametes.
One way to consider the ramifications of these possible meetings is to consider who the stakeholders are. Where the procreative liberties described above are concerned with the rights of the donor, and the procreative obligations were primarily concerned with what the donor must do for the resulting child, the possibility of donors meeting their biological offspring involves a triad of moral stakeholders: the donor, the resulting child or children, and finally, the child's parent or parents: those who receive the gametes and go on to rear the child.
In terms of meeting their biological offspring, what would a donor stand to gain from stipulating who that child's parents can be? They might reason that certain attributes can be vertically transmitted, and wish for their donor child to have those attribute. These attributes might be of central importance to the donor: they could be deeply held values such as a commitment to respecting others, to liberalism, to patriotism, to veganism, or to a particular religion. These values may generate moral prescriptions about how a person should act regarding themselves and to others, including to a god or gods. They may, for the donor, mean the difference between whether the child will be a good or a bad person, or whether that child will go to heaven or hell. Whatever the values are, anyone who has ever imagined having a child has probably thought about the ways they might like that child to be.
There is no guarantee that a child will turn out like their parents, but it is not unreasonable to think that, at least for certain attributes, having parents who are X will increase the chances of their child being X. Given the central importance of these value systems to some donors, it seems there is a prima facie reason to give donors whatever degree of control over the child's value systems is afforded by letting them choose who the recipients will be.
It might be argued that there is in fact something uncomfortable about this values spreading as something that forms part of the value of parenthood. Perhaps it is really none of a person's business what another person's values turn out to be, and having a genetic connection to a person gives me no more right to try to change or set their values than anyone else. This may be particularly so if my connection is exclusively genetic, that is, somebody else will take on the social role(s) of parenting for that child. The argument may be convincing in the case of a person who will actually have a parental role in the child's life but for a donor, the argument is much less convincing. The prospect of meeting one's genetic offspring in this setting mean that we might want to have someone with similar values as our genetic offspring, but the idea that this gives one a right to choose their gamete recipients, particularly as the similarity in values is not really guaranteed, is not convincing.
Let us consider the recipients next. The parents will likely want any meeting between their child and their donor to be as pleasant as possible for everyone, but their primary concern will be their child. They may therefore prefer the presence of shared values between donor and child. This may conflict with their general views on the acceptability of conditionality, but for this discussion we are only concerned with how they will be affected by a meeting between donor and donor-conceived family.
The next stakeholder to consider is the donor-conceived child. Given the possibility of a relationship between the donor and the child and their family (including their social parents, siblings, and any other extended family members), there are similar reasons to those described in the paragraphs above to suggest that donor choice would allow for greater cohesion. After all, if they want a relationship, then there are reasons to ensure the best kind of relationship. If they do not want a relationship, it may matter less whether there is concordance in their views.
Nevertheless, there are reasons why the setting of conditions may be a serious affront to a donor-conceived child. For one, a donor-conceived child may develop an egalitarian worldview leading them to oppose the setting of conditions in such circumstances. Second, and perhaps with the potential for more distress to the donor-conceived child, the child may find that the characteristic(s) against which their genetic parents discriminated represent morally repugnant reasons for discrimination. Further to this, the child may themselves come to have such a characteristic, and in this case the potential for harm and upset to the donor-conceived child is clear.
A good example might be sexual orientation: if a donor is allowed to select out same-sex parents, a donor-conceived child may (a) come to find this discrimination morally repugnant and/or (b) belong to a minority sexual orientation themselves, in which case they may find the affront altogether more personal.
Much of the above rests on speculation about what donors’, recipients’ and donor-conceived children's attitudes might be towards a meeting. As the year 2023 approaches, at which point the first donor-conceived children in the United Kingdom will have reached the age where they can legally find out details about their donors and arrange to meet them, the United Kingdom will likely be a source of rich data on these attitudes. Until then, we must accept a more speculative approach. That being said, we already know that there are donor-conceived people who view the circumstances of their conception as being morally wrong, for reasons relating to senses of personal identity and family relationships. 33 Notwithstanding that some of these arguments are incompatible with some of the suggestions we make in this article, this may give us reason to believe in the plausibility of donor-conceived people's being harmed or caused distress by conditions set by their donor.
One reason that it is problematic for donors to set conditions on who should receive their gametes on the basis of a potential future meeting between parties is that this rests on certain presumptions about the nature of the relationship that will follow. A donor-conceived child, and indeed that child's parents, may have no interest in pursuing a social relationship with their donor. The rationale for removing donor anonymity in the United Kingdom was that a child has a right to information about their genetic history, and to pursue a relationship with their genetic parent(s). 34 Fairness considerations speak in favour of this rationale: most people have ready access to information about who their biological parents are (notwithstanding cases of misattributed paternity), so it seems only fair not to disadvantage donor-conceived children in this way. This line of reasoning may unfortunately be misinterpreted as an endorsement by UK legislators of the importance of a genetic connection (which may be to the detriment of recipient parents and adopted parents), but it would be better interpreted as an acknowledgement that for some people the genetic connection is important, and that UK law does not pass judgement on whether one should value this or not. Their view is likely that, by removing anonymity, the option to find out more about their biological parent(s) is there for donor-conceived children if they wish to take it.
It is important to take note of where this leads us. The spirit of this legislation is clearly derived from fairness or rights-based considerations revolving around the donor-conceived children: giving donor-conceived children the opportunity to get more information both puts them on a level playing field with most other people, and affirms their right to access their own genetic information.
None of this revolves around the donor. The reasons for allowing for the possibility of donor-conceived children and their parents meeting the donor are all grounded in the donor-conceived child themselves. The idea of a donor's being allowed to choose who their recipients are on the basis that this will make the child someone they would be happier to have a relationship with is therefore to place the locus of moral concern on the wrong person. As Calder puts it (summarising Brighouse and Swift): ‘though parenthood carries goods of its own, parental prerogatives are delimited by what is good for children’. 35 The locus of moral concern is therefore the donor-conceived child. The child is the more vulnerable party, standing to suffer the most harm where the relationship goes awry. And crucially, the relationship can be made to go awry not just during a meeting, but when a child learns anything about the donor. The mere revelation to a child that a donor set certain conditions could be harmful to a child. We stated above that parents do not have total control over their children's attributes, so the donor's choice of parents will not fully determine what the child is like. If a child turns out to have an attribute that was selected against by the donor parent (e.g. they are not heterosexual) then the capacity for harm here, we argue, trumps the arguments from giving donors the choice.
The final step in our argument is to outline how these same arguments apply to organ donation just as they do to gamete donation, rendering it illegitimate for there to be different policies between these two spaces. It is straightforward to see how the same concerns apply that would make conditional organ donation illegitimate. Where there is the possibility that organ recipients can meet their donors, there is the potential for fraught relationships. While these are not parental, relationships between donors and donor-conceived children are not parental either, at least not in the most important sense of parenting, that is, the social sense. While the organ case differs from the gamete case in that a new person is not created, and therefore there would not be cases where a direct beneficiary of the transplant was a member of the group being discriminated against (as in the case of gametes donated only to heterosexual people who then go on to have a gay child). Nevertheless, it is plausible that a person would be aggrieved by the notion that their organ donor had selected out people of a certain type, according to principles and criteria that the recipient found morally repugnant.
There is empirical evidence that this harm and outrage would be felt, in the form of the reaction to the British donor's desire to donate an organ only to a white recipient, described above. Normatively, this moral distress seems legitimate, since any person would rightly be aggrieved at the notion that donors had been permitted to make such choices. Even in cases where there is no possibility for an organ donor to meet the recipient, the same worries apply: the mere knowledge of a condition having been set can serve to cause grievous moral harm to an organ recipient.
Conclusion
We have considered putative reasons for allowing donors to set conditions on who can receive their gametes while at the same time refusing to allow organ donors to set conditions on who can receive their organs. The arguments from special procreative liberties, from special parental obligations, and from gamete donors being able to meet their recipients, have all been shown to fail to justify allowing gamete donor conditions and refusing organ donor conditions. Since we have not found, either in our analysis here or existing literature, a good moral reason to have a donation system that allows for setting conditions on one type of tissue but not on the other, any jurisdiction that maintains such a system should review its policies to ensure consistency.
Footnotes
Acknowledgements
We would like to thank Heather Draper, Sue Avery, and Jonathan Ives for their guidance as we did this work.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Work for this article was begun as part of a doctoral project funded by the Arts and Humanities Research Council & Birmingham Women's Hospital NHS Foundation Trust (grant/award number: AH/H034536/1).