
Abstract
The current legal status and medical ethics of routine or religious penile circumcision of minors is a matter of ongoing controversy in many countries. We focus on the United Kingdom as an illustrative example, giving a detailed analysis of the most recent British Medical Association guidance from 2019. We argue that the guidance paints a confused and conflicting portrait of the law and ethics of the procedure in the UK context, reflecting deeper, unresolved moral and legal tensions surrounding child genital cutting practices more generally. Of particular note is a lack of clarity around how to apply the “best interests” standard—ordinarily associated with time-sensitive proxy decision making regarding therapeutic options for a medically unwell patient—to a parental request for a medically unnecessary surgery to be carried out on the genitalia of a healthy child. Challenges arise in measuring and assigning weights to intended sociocultural or religious/spiritual benefits, and even to health-related prophylactic benefits, and in balancing these against potential physical, functional, and psychosexual risks or harms. Also of concern are apparently inconsistent safeguarding standards being applied to children based on their birth sex categorization or gender of rearing. We identify and discuss recent trends in British and international medical ethics and law, finding gradual movement toward a more unified standard for evaluating the permissibility of surgically modifying healthy children's genitals before they can meaningfully participate in the decision.
Keywords
Introduction
The law and ethics of medically unnecessary a genital modification of pre-pubescent children are increasingly debated.3–8 On the one hand, it is widely internationally accepted that such modification, brought about by cutting or removing healthy tissue, is both ethically and legally inappropriate in the case of roughly half of all such children: namely, those whose genitalia at the time of birth are deemed to fall within normative standards for “binary” female classification (i.e. non-intersex b females), virtually all of whom will be raised as girls. This international proscription on surgical interference with non-intersex girls’ healthy genitalia applies no matter how slight the intended cut and even when done in a medicalized fashion, that is, with sterile instruments and anesthesia by a skilled practitioner.16–18 In the United Kingdom (UK), the country on which we focus in this paper, such medically unnecessary genital cutting is, in fact, a criminal offence irrespective of the individual's own consent even after the age of 18. c Moreover, in the case of non-intersex girls under the age of 18, parental “proxy” consent or permission for such cutting—based on a sincere assessment of the child's best interests, including interests related to ethnic identification or cultural or religious belonging d —is considered to be categorically invalid.19,22
On the other hand, there is less consensus around children who have certain intersex traits (also called differences of sex development or variations of sex characteristics), regardless of whether they are categorized as male or female at birth.28–31 Some parents and physicians argue that early surgical interventions to “normalize” these children's genitalia so as to bring them into closer alignment with a culturally normative male or female appearance should be allowed. 32 However, a growing number of authors contend that these children, too, should be protected from genital surgeries that are not strictly medically indicated (i.e. to preserve or restore a somatic function that is necessary for physical health, such as the ability to pass urine). This would allow the children to decide, when they are older, whether they endorse the psychosocial or cultural aims of such surgeries, and if so, whether they also accept the particular risks and trade-offs associated with genital surgery as the chosen means of pursuing those ends.13,33–38 In fact, the World Health Organization (WHO) has recently condemned such surgeries, if carried out on children who are too young to consent to them, as human rights violations and as a form of “abuse” 39 (p. 1).
Meanwhile, non-intersex males raised as boys have elicited polarized views with respect to the question of whether it is permissible to perform a medically unnecessary surgical operation on their healthy genitalia in childhood (i.e. prior to the possibility of obtaining their own ethically valid consent). The views are split between those who argue that such children have no moral or legal right to a surgically unmodified penis,40–43 and those who argue that they, no less than children with intersex traits, have the same right to an intact sexual organ as do non-intersex girls.44–49
Many scholars now argue that the current situation, namely, the existence of different ethicolegal standards for medically unnecessary child genital cutting practices depending on the child's sex traits or gender of rearing, is unjust and unsustainable.1,6,26,27,34,50–52 Such scholarship has, however, so far failed to make a significant difference to law or policy. We will illustrate this conundrum with a close analysis of the most recent major UK guidance on non-therapeutic penile circumcision of minors, from the British Medical Association. We intend for our analysis to serve as a constructive critique of this specific policy, but also as a signpost for deeper, unresolved moral and legal tensions surrounding child genital cutting practices in Western countries more generally. 53 In other words, by examining in detail how one influential group of ethicists has sought to reconcile—or in some cases, avoid—these tensions, we can shed light on the kinds of challenges that any such group will face that is charged with issuing coherent legal and moral guidance in this area. Along the way, we provide suggestions for what we see as a more coherent approach going forward.
The British Medical Association guidance on NPC
In February of 2019, the British Medical Association (BMA) released a new set of guidelines entitled “Non-therapeutic male circumcision of children—practical guidance for doctors”. 54 The mention of children in the title is significant, given the distinct legal, ethical, and medical questions that arise when contemplating non-therapeutic interventions into the sexual anatomy of pre-Gillick-competent minors as opposed to older, Gillick-competent minors or adults. 55 For the purposes of this paper, to avoid confusion, we refer exclusively to the law and ethics of non-therapeutic penile circumcision of pre-Gillick-competent minors.
In the UK, Gillick competence—named for the influential court case that established the standard—refers to the legally recognized ability of a minor under the age of 16 to validly consent to a proposed medical procedure on their own behalf. 55 This standard has recently been discussed, most saliently, in the context of ethical debates and legal action surrounding puberty blockers for transgender-identified minors, as in the case of Bell versus Tavistock.56–58 The question at stake in that case was whether an adolescent under the age of 16, who actively seeks a medical remedy for acute distress associated with gender dysphoria, can give their own valid consent to such treatment. 59 The original judgment as to this question, which was later overturned on appeal, was in the negative: the High Court concluded that such a minor was unlikely to have the requisite decision-making competence to authorize puberty blockers for themselves. For the purposes of this paper, we do not take a position on the correctness of either ruling (that is, the original ruling or the ruling on appeal). However, we would note that we are, in general, entirely supportive of transgender and other gender-diverse persons being able to access, without any undue burden, whatever interventions are necessary to secure and promote their health and well-being. And for individuals who are deemed sufficiently autonomous to make relevant healthcare decisions on their own behalf, whether they are Gillick-competent minors or legal adults (transgender or otherwise), we take it as uncontroversial that their decisions should be respected. 60
What, then, should be said about non-therapeutic penile circumcision (NPC), a medicalized intervention that most typically affects minors who are unquestionably pre-Gillick-competent, such as newborns and infants? NPC, which refers to the partial or total removal of an individual's healthy penile prepuce61–63 (see Box 1), raises a distinct set of issues. Indeed, given the logic of the Tavistock case—as controversial as that case proved to be—NPC of children who are categorized as male at birth should, if anything, prompt even greater legal and ethical scrutiny. Tavistock concerned a largely reversible hormonal intervention designed to suspend pubertal development, thereby temporarily preventing certain undesired changes to one's sexual anatomy from taking place. NPC, by contrast, involves the permanent surgical modification of a child's sexual anatomy before they have developed a gender identity or any related attitudes about their body. In other words, unlike an older minor experiencing persistent gender dysphoria, NPC is performed on children who have no physical or mental concerns about their body requiring intervention of any kind. Moreover, and perhaps more importantly, in contrast to the situation of a relatively mature minor who requests an intervention to deal with certain aspects of their sexual anatomy with which they are deeply unhappy—and who can, at least potentially, provide their own valid consent to the requested intervention—NPC is typically performed on children who are not unhappy with their bodies, who have not requested any changes, and who cannot possibly consent to such surgery. How shall we evaluate the legal and ethical status of NPC?
The genital prepuce or foreskin is a shared anatomical feature of both male and female members of all human and non-human primate species. 61 In humans, the penile and clitoral prepuces are undifferentiated in early fetal development, emerging from an ambisexual genital tubercle that is capable either of penile or clitoral development regardless of genotype. 71 Even at birth—and thereafter—the clitoral and penile prepuces may remain effectively indistinguishable in people who have certain intersex traits or differences in sex development.28,72,73 The penile prepuce has a mean reported surface area of between 30 and 50 square centimeters in adults74,75 and is the most sensitive part of the penis, both to light touch stimulation and sensations of warmth.76–78 The clitoral prepuce, while smaller in absolute terms, is continuous with the sexually-sensitive labia minora; it is also an important sensory platform in its own right, and one through which the clitoral glans can be stimulated without direct contact (which can be unpleasant or even painful). 79 Regardless of a person's sex, the prepuce is “a specialized, junctional mucocutaneous tissue which marks the boundary between mucosa and skin [similar to] the eyelids, labia minora, anus and lips … The unique innervation of the prepuce establishes its function as an erogenous tissue” 61 (p. 34). It has been argued that, insofar as one assigns a positive value to the penile or clitoral prepuce, or to the ability to decide for oneself whether such delicate genital tissue should be cut or removed, its non-consensual excision necessarily harms the person to that extent, irrespective of medical risks or complications. 80
The aforementioned guidance from the BMA is significant in that it marks the organization's first substantive update on this question—“The Law and Ethics of Male e Circumcision”—since it published a paper with that title in the Journal of Medical Ethics in 2004 65 (revised in 2006 following criticism from legal experts).66–68 Written by members of the BMA's Human Rights and Ethics Department, the new guidance is presented in the form of a “toolkit” consisting of twelve “cards” to aid physician decision-making. The guidance was an opportunity for the BMA to bring its policy up to speed with more than a decade's worth of scientific, legal, and scholarly developments that had taken place since its previous offering.
We will argue that this opportunity was missed. Apart from some minor improvements in areas such as record-keeping, the bulk of the new guidance does not, we suggest, accurately reflect current ethical, legal, safeguarding, or medical concerns regarding NPC. Addressing these concerns with reference to the BMA guidance will allow us to give an up-to-date account of scholarly developments that we hope will be of use in future guidance preparation.
The authors of the present article are all professionally engaged in academic, legal, and medical fields touching upon the status of genital cutting in the United Kingdom and internationally. As part of the BMA's consultation on the guidance prior to its composition, we were invited to present our concerns about NPC—and the BMA's position on it—both in written submissions and in a face-to-face meeting with BMA ethics representatives in 2016. We also provided detailed comments on a draft of the new guidance in 2018 prior to its release. Here, we identify and discuss several unaddressed or otherwise outstanding areas of concern in the BMA's final guidance.
In the first section, we discuss problems relating to the analysis of medical ethics, including (1) the absence of an explicit stance on the underlying ethical status of NPC, coupled with an implicit permissive stance, (2) an incoherent and impracticable analysis of the child's best interests, (3) unbalanced guidance regarding cultural issues, (4) unbalanced guidance regarding scientific/medical issues, (5) unjustified differential treatment of children of the same sex, (6) unjustified differential treatment of children of different sexes, (7) problems with child safeguarding, and (8) problems with regulation and training. In the second section, we focus on legal issues, including (9) an unjustified presumption of lawfulness of NPC of minors and (10) failure adequately to address recent case law. As we discuss, many of these same concerns will arise in any policymaking context. Further work is therefore needed to address such concerns going forward.
Section 1: Concerns with the BMA’s medical–ethical analysis
Concern 1—Conflicting stance on the underlying ethical status of NPC
Both now and for several decades, the overwhelming question confronting British doctors on this issue has been whether or not the performance of NPC on healthy, non-consenting (because incapable of consenting) minors upon parental request is compatible with contemporary medical ethics and the child's best interests.
In its new guidance, the BMA states that it does not take a position on this issue, but rather adopts a “neutral” stance. As we will argue, this is not an accurate description of the ethical position implied by the guidance, which is in fact permissive. By comparison, other similar bodies, such as the Royal Dutch Medical Association (KNMG), the Danish Medical Association (DMA), and the Finnish Medical Association (FMA), are more forward in their approach, offering a clear medical-ethical stance for consideration. For example, the KNMG states that NPC of minors conflicts with the child's right to physical integrity, and advises doctors to discourage the practice. The KNMG further states that, insofar as there may be health benefits to circumcision—a question we revisit below—“it is reasonable to put off circumcision until the age at which [the] boy himself can decide about the intervention, or can opt for any available alternatives.” 81 The equivalent DMA policy urges that NPC of minors “is ethically unacceptable” and that “circumcision should not be performed until the boy has obtained the [capacity] to independently choose the procedure.” 82 Finally, current FMA guidance holds that parents who request NPC should be counselled about “giving up the procedure or postponing it to a time when the boy is able to decide for himself.” The FMA guidance concludes: “From the point of view of medical ethics, the duties of a doctor should not include performing” the procedure. 83
In failing to articulate an explicit position, the BMA's guidance ends up being ambiguous and at times contradictory. For example, while the guidance declares that parental wishes alone do not constitute sufficient grounds to authorize NPC for a pre-autonomous child, the balancing test it formulates implies that if those wishes happen to fall within certain categories (especially religious or cultural beliefs) this may indeed be sufficient to override all other considerations and proceed with NPC (see Concern 2 below). Moreover, the cautious principles the BMA enunciates for therapeutic (i.e. medically necessary) circumcisions are hard to reconcile with the exceptionally low threshold for authorizing non-therapeutic circumcisions, despite the fact that ethical concerns in the latter case are, if anything, much weightier (see Concern 4 below).
The guidance correctly notes that there is “a wide spectrum of views” within society on NPC and that the issue is “controversial.” It is for this reason, however, that expert guidance is needed. As we discuss next, although the BMA states that it does not take an explicit stance on the ethics of NPC, its analysis suggests a de facto permissive stance toward the practice, underwritten by a perplexing analysis of the child's best interests.
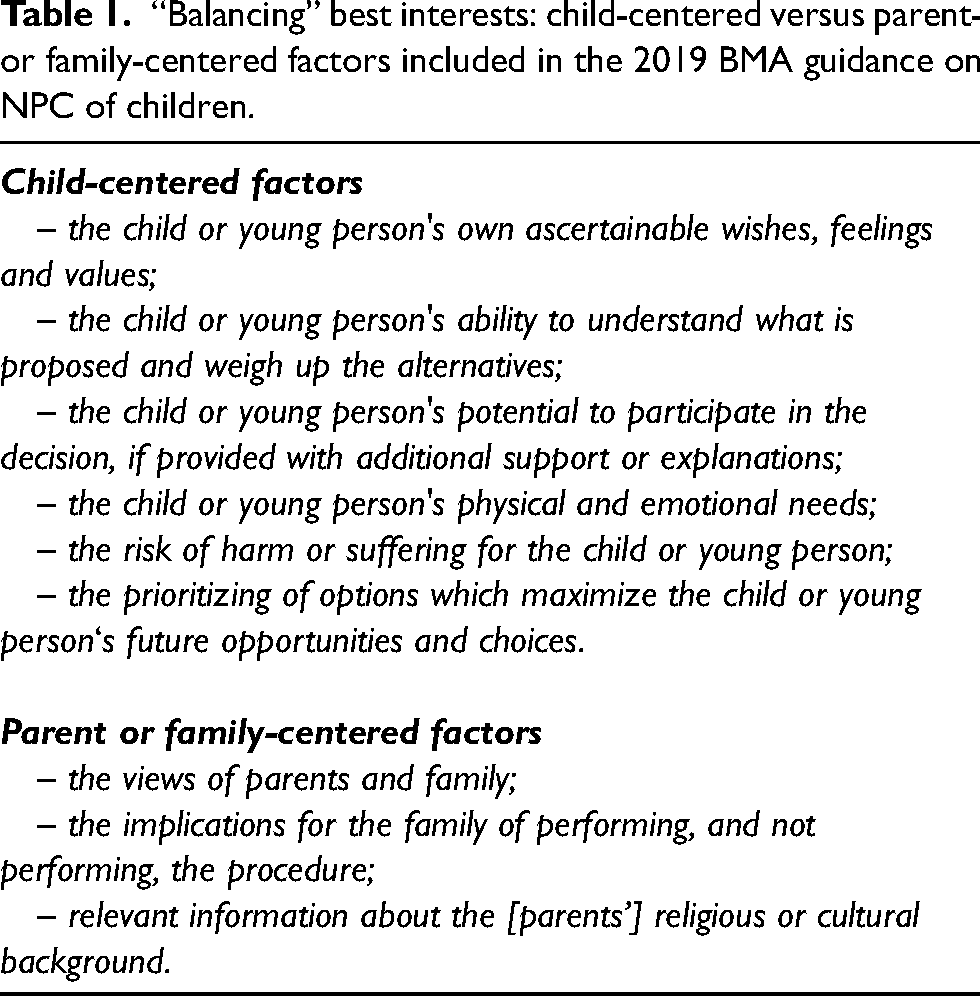
“Balancing” best interests: child-centered versus parent- or family-centered factors included in the 2019 BMA guidance on NPC of children.
Concern 2—Incoherent analysis of best interests
The first of the guidance's “Ten good practice points” states: “Doctors must act in a child's best interests.” The section then clarifies that “parental preference alone does not constitute sufficient grounds for performing [NPC] on a child unable to express his own view.” Such principles are widely accepted. The need to act in a child's best interests, for example, is reflected in law in the Children Act 1989. And it is uncontroversial that parents are not entitled to authorize, for their healthy children, simply whatever surgical procedure they may choose. Yet the force of both statements, we argue, is undermined by the BMA's proposed balancing test for determining what the best interests of the child with respect to NPC actually are. The test includes a set of factors presented all together in a single list; however, each factor can plausibly be identified as either relatively “child-centered” or more “parent/family-centered” and we have organized them accordingly in Table 1 below, under (our) two headings:
The BMA guidance asks the doctor to balance these factors. In effect, therefore, it implicates doctors in a process of weighing up the strength of the child's own input and interests against the strength of those that are more parent-centric. There are, of course, longstanding debates about whether or when a “best interests” standard should even be used in clinical decision-making (albeit typically with regard to scenarios involving a non-competent patient who is currently dealing with a disease or threatened disability, rather than a healthy patient as in the case of NPC).84–89 However, if the best interests standard is to be invoked in connection with proxy decision-making for a child in a medical context, it must be remembered that the very purpose of the standard—in contrast to other proposed standards, such as the “harm principle” 89 or the “zone of parental discretion” 90 —is to center decisions squarely on the child's interests, rather than those of other stakeholders. Thus, despite an expressed adherence to the best interests of the child, the guidance is proposing a test that is not well-suited to that end.
First, the test is not meant to help decide, for example, which of a number of available treatments should be pursued in the case of an unhealthy child, where a decision must be made one way or the other. Rather, it pertains to a decision about whether to perform a non-therapeutic surgery—at the parents’ request—on a healthy child: that is, a child who, medically speaking, needs no intervention whatsoever. Even then, the test does not give clear priority to the child-centered factors it identifies but rather places these factors in competition with other-party interests. Although it acknowledges that parental wishes alone are insufficient to authorize NPC, the BMA—under what we have labeled “parent/family centered factors”—includes two further elements for consideration: the implications for the family of proceeding or not proceeding, and the parents’ religious or cultural background. f
The BMA ostensibly proposes these as independent factors, which might, together with the parents’ views or preferences, provide sufficient grounds to proceed. However, these factors are not truly independent, but rather are—for all intents and purposes—the very same parental preferences re-worded. It is, after all, inevitably the parents who cite their own religious/cultural background as a basis for proceeding (whose background other than the parents’ can ever be at play?); and “implications for the family” will only be communicable by the parents. The medical professional cannot know the child's own wishes and is not entitled to take instructions from the wider family, still less from the child's future cultural community (even if this could be ascertained).
The guidance thus seems to engage in a kind of double-speak: accepting, on the one hand, that parental preferences are not sufficient to authorize NPC, but then allowing for duplicate and even triplicate counting of such preferences under other headings. This gives the impression of a cluster of reasons that could suffice to authorize NPC, when in fact parental preferences are, through various guises, being given potentially determinative weight.
This can be seen by imagining the use of the balancing test in practice. If one takes a neonate or young child, each of the “child-centered factors” is an argument against imposing NPC in childhood and for deferring the decision to the affected individual when sufficiently mature: the child's wishes are not ascertainable; the child cannot understand what is proposed or weigh up the options; the child cannot participate meaningfully in the consent process; the child has no physical need of circumcision and has expressed no preference for losing their penile foreskin; there is identified risk of harm, both physical and psychological, from non-consensual genital surgery; and not circumcising keeps the child's future opportunities and choices open, whereas NPC on a minor shuts down the option of the child to remain genitally intact upon adulthood (see Box 2 for further discussion). As the BMA itself states on Card 6, “the harm of a person not having the opportunity to choose not to be circumcised or choose not to follow the traditions of his parents must also be taken into account, together with the damage that can be done to the individual's relationship with his parents and the medical profession, if he feels harmed by an irreversible non-therapeutic procedure.”
Infant circumcision versus adult circumcision. Arguments adapted from Refs.37,69,91
As noted in the main text, childhood NPC shuts down the option of the child to remain genitally intact upon reaching adulthood. However, one could also argue that a failure to circumcise someone in childhood, in infancy in particular, shuts down the option of the child, once grown, to have previously been circumcised at an age when the procedure is often claimed to be technically simpler and less medically risky than circumcision later on. It might also be emphasized that the infant, in contrast to the adult, will neither prospectively fear the operation nor, once it is over, “remember it.” 92
There are several problems with this argument, both medically and ethically.69 First, it rests on the assumption that if circumcision does not occur in infancy, it will have to be performed later in life anyway. However, in reality, circumcision is rarely required for medical reasons,93,94 and the vast majority of non-circumcised males, certainly in the United Kingdom, choose to retain their foreskins throughout life. Only a small minority of non-circumcised men report “ever” wishing that they “had been” circumcised—even in the United States, where infant circumcision remains a dominant cultural practice.91,95
Second, the argument ignores a key asymmetry in available remedies for resentful members of the classes compared: i.e. those adults who were circumcised non-consensually in infancy, but wish they had not been, and those adults who were not circumcised non-consensually in infancy, but wish they had been. Although members of the latter group, admittedly, cannot travel back in time to undergo an infant circumcision, they do still have the option of circumcision open to them. It will, undoubtedly, involve certain costs and inconveniences, but these are no greater than the costs and inconveniences associated with other voluntary genital modifications that consenting adults may sometimes pursue (e.g. female “cosmetic” labiaplasty; see further discussion below). Moreover, in such cases, there will be no doubt as to whether circumcision is truly desired. By contrast, members of the former group—that is, those adults who resent having had part of their healthy genitals excised before they were capable either of consent or refusal—have no equivalent recourse or remedy: they cannot “undo” their circumcision.
Third, as to medical considerations. Even if one accepts the medical claims advanced by those who defend the “better in infancy” view—notwithstanding that many such claims are scientifically contentious—what the claims suggest is a relative risk reduction for some, but not other, complications associated with infant circumcision compared to “later” circumcision, with the absolute risks, in either case, said to be small and based on potential complications that are (mostly) easily treatable anyway. 92 But if that is the case, the alleged relative risk difference between circumcision in infancy versus "later” is not particularly ethically important. A supposedly trivial risk of likely-treatable complications—divided by any amount—is still trivial.
In any case, “later” in these studies typically means later in childhood—which is not the relevant comparison class in the context of discussions about informed consent. To that end, a direct comparison between infant (i.e. non-consensual) and adult (i.e. consensual) circumcision—controlling for relevant confounds, such as whether the circumcision in question was therapeutic or non-therapeutic—is revealing. According to a recent systematic review, meta-analysis, and meta-regression of all available studies, “while children circumcised at age 2–18 more often experienced complications as compared to those circumcised as infants, there was no significant difference between infants and adults” 96 (p. 32, emphasis added). By contrast, there is a highly significant difference between infants and adults in terms of their respective consent capacity. In other cases, this difference is considered to be perhaps the single most important ethical factor in evaluating the permissibility of proceeding with a non-therapeutic genital surgery.
This last point can be reinforced with an analogy. Suppose, for the sake of argument, that medically unnecessary, so-called “cosmetic” labiaplasty was being contemplated instead of penile circumcision. Further suppose that all of the medical advantages claimed for infant, compared to adult, circumcision by proponents of the “better in infancy” view 92 applied with equal force to “infant labiaplasty” (note: an illegal procedure) compared to labiaplasty carried out in adulthood. Even if the data were unambiguous on this point, the presumable consensus of Western medical ethicists and legal experts would be that such data are irrelevant. 97
For example, the argument that infant labiaplasty would be preferable because “she won't remember it” at that age would not be entertained. The argument that labiaplasties performed in infancy are technically simpler, heal more quickly, or have a slightly decreased (absolute) risk of some, but not other, surgical complications—compared to labiaplasties performed “later on”—would likewise be dismissed as missing the point, even if all such claims were true. Finally, the argument that she might be teased or otherwise socially mistreated for having healthy labia that do not conform to some people's cultural or aesthetic preferences would be seen as misidentifying both the source of, and appropriate solution to, the alleged or potential problem.
Because cosmetic labiaplasties are medically unnecessary, and because they concentrate risk on, and aim to permanently modify, a person's so-called “private” anatomy (that is, a part of the anatomy that people are socialized to regard as being exceptionally personal or intimate), it is wrong, according to this view, to perform such a genital surgery on a healthy individual who cannot consent. In other words, it is wrong as a matter of principle, irrespective of any third party judgments as to the potential balance of benefits and risks of performing the surgery at various ages.
The same analysis, we suggest, applies to all persons raised within societies that regard the genitalia as personal or private, irrespective of the individual's particular sex characteristics. Accordingly, we contend that urgent medical necessity—whereby it is not possible to delay or defer the surgery without putting the person's physical health at significant risk of serious harm—is the only permissible basis for performing genital surgery on someone who is not capable of personally consenting.
Given that (a) parental preference is (as the BMA accepts) insufficient to authorize NPC on a child and (b) as shown above, all additional factors apart from the child-centered ones reflect the same underlying parental preference, the case against proceeding is, according to this analysis, overwhelming. However, rather than acknowledging this implication and urging doctors to counsel against NPC, as some European medical societies have done, or, alternatively, choosing some other test or standard for its guidance that does not pretend to be child-centered, the BMA instead advises doctors to invite the parents to “explain and justify” (Card 6) how their preference for NPC might be in their child's best interests after all. What could be the basis for such an explanation/justification? It seems to us that a decision to proceed with NPC in such circumstances would have to be based on a parental appeal to what the BMA characterizes as potential “psychosocial benefits” that might be attributed to NPC (Card 4).
We will discuss these potential benefits below. In practice, however, by appealing to such uncertain and unmeasurable potential outcomes, parents can—without any plausible pushback from the doctor, who lacks the expertise to evaluate such claims—tilt the results of the balancing test in the direction of genital surgery. Specifically, in a situation where parents want NPC performed on their infant, and where they cite religious reasons or claim that the procedure is in their view in the child's best psychosocial interests (a claim the doctor has no way of assessing, much less rebutting), parental preference alone will indeed have sufficient force to neutralize all other child-centered items on the list. And if the parents do not want NPC performed, then the other items are irrelevant, because the procedure will not be requested in the first place.
Consequently, in reality, the BMA guidance entails that the views of the parents and family, particularly as to their religious or cultural background, will in most cases decide the entire question. All mention of the child participating in the decision, or of the need to maximize the child's future choices, and so on, is thus transformed into window dressing. Problematically, however, such an approach could in principle justify all manner of non-therapeutic procedures on children (e.g. ritual scarring) under the rubric of parental wishes, so long as the procedure is done early enough so as to circumvent the child's own understanding of, or involvement in, the decision. Yet this would run counter to any reasonable understanding of physicians’ child-safeguarding duties, or of maximizing children's (future) bodily autonomy. In other contexts, it has been the subject of legal sanction. g
Concern 3—Unbalanced guidance on cultural issues
In deliberating about the child's best interests, the guidance advises doctors to temper their medical analysis with broader considerations of socio-cultural and even theological factors which are outside the competence of doctors. Given that, as noted below, the BMA is not prepared to take a definitive view as to strictly medical questions (regarding, e.g. health benefits or risks of NPC), it is striking that it does make strong assertions regarding matters of sociology and religion.
For example, the BMA refers to “culture[s] in which circumcision is perceived to be required for all males” as a relevant consideration for doctors asked to perform NPC. It is even prepared to advocate for the “increased acceptance into a family or society that circumcision can confer” as “a strong social or cultural benefit” in favor of proceeding. Of course, precisely the same argument applies to cultures in which ritual female genital cutting is perceived to be required for all females, or in which such cutting is claimed to increase acceptance of the girl-child into a family or society; but this is an argument that the BMA rightly rejects. For males, however, the doctor is asked to stray into the territory of cultural judgments, and in practice to accept at face value whatever parental justification is offered regarding their community's perception of a requirement for NPC (and/or the implications of this perceived requirement for the child's best psychosocial interests).
This is perplexing, given that elsewhere in the guidance the BMA accepts that non-medical cultural/social benefits for NPC are “unquantifiable” and “intangible,” that doctors have “limited understanding” of these matters in any case, and that weighing up such factors against known medical considerations is “challenging” to say the least (Card 6). It is not merely challenging. It is impossible for any doctor not only to make a theological–psychosocial determination but also then to assign a particular weight to that determination, as against medical considerations on the other hand.
Absent from the toolkit is any discussion about the contemporary heterogeneity of religious practices, including in communities such as Judaism98–100 and others within which penile circumcision (and also, in some sects, ritual female genital cutting) has historically been common (e.g. within Islam). It would have been relevant to note that Israel is now home to a support group for Jews declining to practice circumcision, named Kahal, 100 while in the United States, groups such as Beyond the Bris (http://www.beyondthebris.com) have formed (a bris is a Jewish circumcision ceremony). The absence of any reference to increasing UK practice of Brit Shalom, 101 the non-cutting, gender-inclusive welcoming ceremony for children of Jewish parents, 102 means that doctors who rely on the BMA for guidance will be unaware of the variance of opinion within ethno-religious communities as to whether non-consensual childhood circumcision is required for all (male) members. h
Nevertheless, suppose that a particular child's parents do believe that NPC is required. Children do not always grow up to share the religious or metaphysical beliefs, nor the associated cultural values, of their parents. Repeated social attitudes surveys have shown a fall in both belief and affiliation with a faith community, indicating that a growing proportion of adults do not identify with the religion or culture of their birth.104–106 For example, according to the results of a 2013 US Pew Research Center study, 107 “Jewish Millennials, those born after 1980, are the most likely to identify themselves as not religious; 32% say that they would describe themselves as having no particular religion or are agnostic or atheist.” 108 While such data do not entail that NPC is not practiced within this group (an unknown number of non-religious Jews may still circumcise), they do highlight the increasing unreliability of parental religious and/or cultural identification as a predictor of the (adult) child's associated beliefs and values.
By the same token, a recent research synthesis on Muslims and Islam in the United Kingdom finds that non-practicing Muslims may account for 75–80% of all Muslims, with a minority also identifying as ex-Muslim, despite having been raised by Muslim parents. 109 The same report notes that minority religious communities in the United Kingdom are often inappropriately treated as homogeneous. These findings are in tension with the BMA's implied recommendation that doctors rely on the beliefs of a child's parents as an acceptable proxy for the child's future values; they also show the inadequacy of that recommendation vis-à-vis the best interests criterion of “maximizing the child's future opportunities and choices” (Card 6). Put simply, one cannot know what an infant's later cultural or religious attitudes will be, including with respect to NPC. Moreover, the BMA's position ignores standard safeguarding norms whereby the most vulnerable persons are to be protected from strongly-enforced views or actions of more powerful others (as in the notion of a requirement to be non-consensually circumcised) which may not be beneficial to them.
On the question of social inclusion or exclusion claimed to derive from NPC, the BMA guidance relies on hearsay. As one of us has noted elsewhere
69
(p. 658): Advocates of [NPC] do not typically cite any evidence that a [non-circumcised] child will in fact psychologically suffer if they end up being different from their peers in this particular respect. There is also a question about who the relevant peers are, depending on the context. In most Western countries where penile circumcision occurs [including the UK] it is usually limited to a minority sub-group, whereas most individuals in the larger society (of which the circumcised child is ostensibly also a part) are not circumcised. Assuming that the child is not entirely isolated from their non-circumcised peers, then, it could just as easily be predicted that they will be [socially harmed] for being circumcised. In short, the [psychosocial harm] argument only works under an assumption of cultural homogeneity with high rates of circumcision; yet this is not the situation in most multi-cultural Western societies where the ethical debate about [NPC] is primarily taking place.
In any event, it is well understood in other medical contexts that the community is not entitled to hold a child's well-being hostage to an involuntary surgery he or she must undergo (i.e. to deflect the possibility of the child's social exclusion, bullying, or mistreatment for not undergoing the surgery). Rather, and just as in the case of ritual female genital cutting, it is widely appreciated that what must be changed in such cases are the social phenomena that lead to the child's ostracism, not the child's healthy genital anatomy. 37 Otherwise, the “best interests” test would suggest that what is clearly not in the child's best interests can become so because others might act in an even more seriously harmful way towards the child in the future. That is not an accepted position in other comparable contexts.
Concern 4—Unbalanced guidance regarding scientific issues
The toolkit notes that the BMA is not a clinical organization i and that “a more comprehensive review of the literature on this issue from an impartial clinical organisation” would be welcome. Nevertheless, the BMA felt it appropriate to draw some conclusions but not others from the available evidence, with no clear basis as to how this was done. For example, the BMA considers that “the evidence concerning health benefit from NPC is insufficient for this alone to be a justification for boys undergoing circumcision. In addition, some of the anticipated health benefits of male circumcision can be realised by other means - for example, condom use.” These statements are consistent with those of other (e.g. European) medical authorities, such as those we cited above. However, other medical conclusions drawn by the BMA are scientifically inaccurate or misleading.
For example, the BMA states that there is: “good evidence from international studies that male circumcision can reduce the chances of HIV infection in some circumstances, although caution must be taken about how this can be extrapolated to the UK.” Notwithstanding the qualification about extrapolation (i.e. from “international” studies to the United Kingdom), this phrasing implies a potential HIV-related therapeutic benefit from NPC as performed in childhood—the specific topic of the BMA guidance. Yet the evidence being alluded to does not pertain to NPC in infancy or childhood, much less in the United Kingdom. Rather, it pertains only to the rate of female-to-male transmission of HIV to voluntarily circumcised African men, specifically in regions of Africa with high rates of such heterosexual transmission and a low baseline prevalence of penile circumcision.110–112
There is no comparable evidence to support a benefit to female partners of circumcised men, whether in Africa or elsewhere,113–115 nor is there evidence of a reduced risk of transmitting HIV, whether to males or females, following NPC of infants or children anywhere. j The statement from the BMA thus serves to confuse both sexually active with pre-pubertal males and voluntary surgery in adulthood with non-voluntary circumcision in childhood. In a word, the statement serves to distract from the issue under discussion, which is not “male circumcision” in general or as it might be performed at any age, with or without the consent of the affected individual, but rather, non-consensual childhood NPC in particular.
With respect to other health-based claims, the BMA alludes to a medical controversy surrounding childhood NPC (Card 1), implying that there is substantial disagreement about the net health benefits of the procedure among relevant medical bodies: that is, mainstream, non-partisan, national-level professional societies that have formally studied the issue. That is not the case. All such bodies apart from those within a single country—the United States k —have concluded that NPC of children cannot be justified on medical grounds in the sense of conferring a net health benefit. Moreover, even as to that one country, the 2012 policy of the American Academy of Pediatrics (AAP) was met with unprecedented criticism from international experts for falling short of its usual scientific standards and exhibiting strong evidence of cultural bias.123–127 i Despite prominently citing the AAP policy as one of only three examples given, the BMA does not mention this pronounced criticism, nor that the policy was allowed to expire in 2017 without being reaffirmed or renewed.
Finally, the BMA gives minimal attention to potentially positive attributes of the foreskin—the part of the penis removed by NPC. For example, it does not cite evidence that the foreskin is the most sensitive part of the penis to light-touch sensation.76,78,130,131 And yet the penile foreskin, like the female labia or clitoral hood, is a potential source of pleasure in its own right
132
and its unnecessary excision is thus, on some accounts, a harm per se.
91
In other words, if the foreskin itself has any positive value, then its sheer non-consensual removal harms the owner, even if there are no surgical complications or other unintended adverse side-effects. According to the authors of a recent narrative review of the psychosexual implications of NPC
133
(p. 5): Informed decisions [about] penile circumcision, especially when made for infants and children, must be based on an understanding not only of the risks of sexual dysfunction but also of changes in biomechanical possibilities and associated subjective experiences. These changes include a loss of the gliding and rocking of the foreskin over the erect penis in manual stimulation by the person or by a sexual partner, rolling or moving of the foreskin across the glans by tongue in oral sex of the flaccid penis … changes in the need for lubrication, and a potential “rolling” of the skin of the shaft (in masturbation, oral sex, and penetrative vaginal or anal intercourse) where motion on the shaft of the penis pulls the foreskin back and forth across the glans without or in addition to other stimulation of the glans. The irreversible change of anatomical properties, biomechanics, and related sexual activity options that some people and their partners may enjoy is an outcome of circumcision that needs to [be explicitly] incorporated into policy documents and informed consent forms and procedures.
More generally, we find that selective quotes and evidence, where discussed, operate throughout the guidance in the direction of minimizing problems with NPC and downplaying reasons to object to it, while alluding to unproven or intangible (e.g. prophylactic or psychosocial) benefits of the practice.
Concern 5—Unjustified differential treatment of children of the same sex
The toolkit takes an inconsistent approach to three categories of children:
The child who presents with a urological problem but for whom there are less invasive treatments than circumcision; The healthy but unable-to-consent child; and The child who is able to speak/express a view.
As to the first category (children with a urological problem involving their penis/foreskin), Card 3 sets out the standard clinical principle that, “as with other therapeutic procedures … unnecessarily invasive procedures should not be used where alternative, less invasive techniques are equally effective and available,” and that “any decisions to undertake an invasive procedure are based on the best available evidence.” As the 2006 version of the BMA guidance continued: “Therefore to circumcise for therapeutic reasons where medical research has shown other techniques to be at least as effective and less invasive would be unethical.”
The previous guidance thus had an ethical contradiction. How could the BMA take such a strong ethical stance on therapeutic genital surgery while simultaneously ignoring the same standard for healthy children faced with the same genital surgery despite the absence of any medical indication whatever? Rationally, compared to a child who has a medical problem for which a more conservative treatment than circumcision is available—a situation in which circumcision is unethical, according to the 2006 BMA guidance—circumcising a child who has no medical problem at all should be even more objectionable from a medical ethics perspective.
Prior to the new guidelines being produced, we raised this issue directly with the BMA's medical ethics team. Their attempted solution to the problem in the new guidance is more problematic still and lacks internal coherence. Rather than restore the healthy child to at least the level of protection extended to the child with a relevant urological complaint, the BMA has now opted to water down the prior ethical considerations for therapeutic circumcision. The new guidance states that circumcision “solely for therapeutic reasons” would be unethical where there are less invasive treatments available (this is the text of the prior guidance, but with the added qualifier “solely”), but then opens wide the scope for circumcising even in such cases by adding “and there are no relevant social and cultural interests to take into account for that particular child”—a qualifier not previously present.
This creates confusion by introducing:
a non-therapeutic rationale for a “solely” therapeutic procedure; a loophole to circumvent the application of standard clinical principles for therapeutic procedures and; a de facto permissive ethical justification for a procedure about which the BMA claims to have no ethical position.
Indeed, beyond being confusing, this position stretches the credibility of the ethical decision-making process beyond the breaking point. The BMA position now appears to be that a procedure it has deemed “unethical” (circumcision solely for therapeutic reasons where less invasive approaches are available) can become ethical because a parent desires this otherwise unethical surgery for non-medical reasons. Such an approach is without parallel in any field of medical practice, logically incoherent, and cries out for justification.
In our view, the caveat now inserted by the BMA for therapeutic circumcision is there for the sole purpose of defending its position on non-therapeutic circumcision. The BMA's supposed “neutrality” on NPC of children has thus had the staggering consequence of dismantling its own long-held ethical standards as to therapeutic procedures on children as well.
Further contradictions arise from the therapeutic and non-therapeutic comparison. When there is a medical indication for circumcision, the BMA states that it “must only be performed by those who are experienced and competent to carry out the procedure, and in an environment capable of fulfilling guidelines for surgical procedures in children.” By contrast, when the child is healthy and there is no medical indication for NPC, the BMA states that NPC does “not require a medical professional” and makes no mention, for such scenarios, of a safe and suitable surgical environment.
The inconsistency continues with Card 7's treatment of the pre-Gillick-competent child who can nonetheless express a view. In that case, the BMA “cannot envisage a situation where it is ethically acceptable to circumcise a child … who refuses.” By contrast, when it comes to the neonate, who is even more vulnerable than the child who can speak—indeed, who is incapable of refusing in any way—the guidance is unwilling to offer the same ethical judgment.
Contemporary ethical and legal approaches m to age-based competency questions ordinarily dictate that the more vulnerable the person, the more protection they should have against incursions upon their body—especially when it comes to their “private” sexual anatomy—and the more cautious a practitioner should be with respect to their present/future interests. Here the position has been completely reversed: the child whose interests are the least known or predictable is given the least protection, notwithstanding the highly personal, psychosexual significance of the body part in question.
Related to this problem is the BMA's conflicting guidance on following “good clinical practice” (Card 2, point 9). Doctors are instructed to subscribe to good clinical practice when acceding to a parent's request for medically unnecessary genital surgery for their child. Yet a practice cannot reasonably be considered to be “good” (qua clinical practice) when the procedure proposed is, as the BMA acknowledges:
Without medical indication; Performed on a non-consenting patient; Irreversible and at a level of invasiveness which has been ruled equivalent to “significant harm” in UK law (see Section 2 on legal matters below);
53
Not medically urgent and hence deferrable to a time when the patient can personally consent (see Box 2); Performed on a sex-discriminatory criterion (see Concern 6 below).
There is no other procedure in contemporary medicine in which proceeding in the above circumstances would still amount to “good clinical practice.” Recommending that a doctor follow “good clinical practice” as to a procedure ruled out by good clinical practice for the above reasons illustrates the inherent difficulties that the guidance has not solved.
The suggestion that this guidance is in line with the BMA's position on “other procedures involving children who lack the capacity to consent” does not, in our view, align with reality. We are not aware of any non-therapeutic invasive procedures on children involving “significant harm” within the meaning of the Children Act 1989 (see later discussion) that the BMA treats as ethically neutral. It would be preferable to be honest in accepting that the BMA's position on NPC has no parallel in any other area of child care or medicine rather than claim that this policy aligns with any other.
Concern 6—Unjustified differential treatment of children of different sexes
In the previous section, we argued that the BMA guidance, if followed, would result in unjustified differential treatment of children of the same sex who either require or do not require a therapeutic circumcision. In this section, we argue that following the guidance would result in unjustified differential treatment of children of different sexes, namely, non-intersex females and males.
The BMA states that it is committed to non-discrimination in terms of sex. 134 Yet the guidance undermines this commitment by affording differential protection to children on the basis of sex. It states that it “does not cover FGM, which is a separate issue and is a crime in the UK.” The term “FGM” refers to female genital mutilation, which the World Health Organization (WHO) has defined as any medically unnecessary female genital cutting (FGC). 135 The WHO does not make an exception, in its definition, for relatively “minor” forms of FGC, such as ritual nicking or pricking of the clitoral hood (WHO FGM Type IV) which do not remove tissue and are thus markedly less severe than NPC.7,136–138 Nor does it make an exception for religious or cultural commitments—a stance which is similarly reflected in UK law, as per the UK Female Genital Mutilation Act 2003.19,22,139,140 Medical care that rejects the notion of differential treatment on the basis of sex should be committed to offering an equivalent level of protection to all children irrespective of their sex characteristics. In remaining “neutral” on the genital cutting of male infants, the BMA enshrines ongoing sex discrimination in medical treatment.
According to the UK doctors’ regulatory body, the General Medical Council, all doctors have an ethical obligation to protect all children and young people—regardless of their race or ethnicity, parental religion, or the sex characteristics of the child. The BMA is a member-led professional doctors’ organization providing detailed ethical guidance to its members. In this context, the existence of FGM legislation does not remove from doctors their ethical obligation to children not covered by those laws: if anything, the need for ethical, non-discriminatory treatment is even greater for patients who do not enjoy the law's specific protection.
In treating males and females differently in this respect, and siloing the debate on female genital cutting from that on male genital cutting, 141 the BMA ignores the substantial body of scholarship from the past two decades comparing female, male, and intersex forms of medically unnecessary genital cutting. This scholarship highlights significant physical, symbolic, ethical, medical, and legal overlaps shared between the sexes when the full range of cutting practices across cultures is considered and like cases compared with like.51,52,142–164
Concern 7—Child safeguarding
In the United Kingdom and widely elsewhere, the introduction of child safeguarding protocols has been accepted as good practice to protect children from a wide variety of harms, including from within their families. According to the statutory English child safeguarding framework, Working Together to Safeguard Children, a “child centred approach is fundamental to safeguarding.” 165 The child is thus recognized as the primary rights holder in decisions concerning him/her/them, and in need of special protection by virtue of the child's vulnerability, especially in the face of competing claims. Recognizing the potential discord between parental wishes and child safeguarding, GMC guidance on Protecting Children and Young People states: “in cases where the interests and wishes of parents may put the safety of the child or young person at risk, doctors must put the interests of the child or young person first. Failure to act when a child or young person is at risk can have serious consequences for both the child and their family.” 166
The imposition without the child's consent of a medically unnecessary, irreversible surgery of a highly controverted nature is a paradigm case where child safeguarding principles ought to apply. They apply in analagous cases, such as the tattooing of minors (see the Tattooing of Minors Act 1969), where the appropriate safeguarding approach is to defer any such choices to adulthood. The authors can think of no case of surgery in a category equivalent to NPC as to which child safeguarding principles would suggest a “neutral” position.
The guidance is also inconsistent in its application of what safeguarding principles it does uphold. In the context of the safeguards recommended for any (older) child who is more able to give valid consent, the guidance wisely warns in Card 7 that “doctors should be aware that parents can exert great influence on their child's view of a procedure.” It also notes that “the BMA cannot envisage a situation in which it is ethically acceptable to circumcise a child or young person who refuses the procedure.”
It is inconsistent for the BMA to acknowledge the danger of overbearing parental influence on a child who is able to voice consent, while at the same time remaining silent as to the much more extreme danger of the same on neonates and very young children. In the latter case, parental override is total. And while the child as at the time of NPC has no voice at all, he must nevertheless forever live with the consequences of his parents’ decision. 46 If there is a danger in the former position, the danger is exponentially greater in the latter—yet this remains unacknowledged by the BMA guidance.
Concern 8—Problems with regulation and training
The BMA states on Card 1 that: “Male infant circumcision does not require medical expertise.” This statement is unsupported by any evidence. Moreover, it is contradicted by the BMA's own exposition of the numerous clinical, anesthetic, and hygiene standards required of a doctor carrying out a circumcision, whether in a religious capacity or not (Cards 3 and 10). (As an anonymous reviewer of an earlier version of this paper wrote, the statement is “astonishing.”) n
How can such a statement be explained? One possibility is that the BMA is tacitly accepting that the minimal standards of care for non-doctor circumcisers should be lower than the standards of care for doctors. If that is correct, its advice might more accurately be expressed as follows: “Infant penile circumcision is the only surgical procedure in which living, healthy tissue is removed which can in principle be undertaken by anyone at all, and which is not subject to any medical regulation or standard-setting, either over who performs it or how it is undertaken, unless undertaken by a doctor.” o Though the introduction to the guidance states that “our guidance does not cover circumcision by non-doctors,” the BMA fails to explain why standard safeguarding principles are not to be considered in the context of unregulated persons who are not physicians performing non-therapeutic surgery on minors, much less in clinically inadequate environments.
The BMA is evidently aware that the same standards are not being applied in non-medical circumcision contexts: Card 6 acknowledges the risk of “unhygienic or otherwise unsafe conditions.” Indeed, the BMA recommends that doctors take into account the possibility of such an unsafe/unhygienic circumcision—if they themselves refuse to perform it—as a possible reason to perform genital surgery on a healthy child when otherwise they would be unwilling to do so.
As the BMA acknowledges, this is adopting the identical logic previously employed to justify the medical performance of ritual female genital cutting or ritual scarification on minors. That the BMA is prepared to spend a paragraph countenancing such logic for male infants is disturbing, particularly given the BMA's silence on the large incidence of non-professional circumcisions in the United Kingdom. It is also further evidence of how the phenomenon of NPC for ritual purposes in a non-medical context is being allowed by the BMA to influence (indeed, erode) standards of clinical practice.
Section 2: Legal concerns
As to the law, we identify two key problems within the legal elements of the guidance (Card 4 and passim):
Despite accepting that belief in the lawfulness of NPC is an assumption without a specific legal foundation, the Card proceeds nonetheless on the basis that NPC is inherently lawful; and The “recent case law” section fails to put squarely at the forefront the High Court's detailed, repeated, and almost unanimous evaluations—over 20 years and half a dozen cases—that NPC, as in the cases considered, is not in the child's best interests.
Concern 9—Unjustified presumption of lawfulness
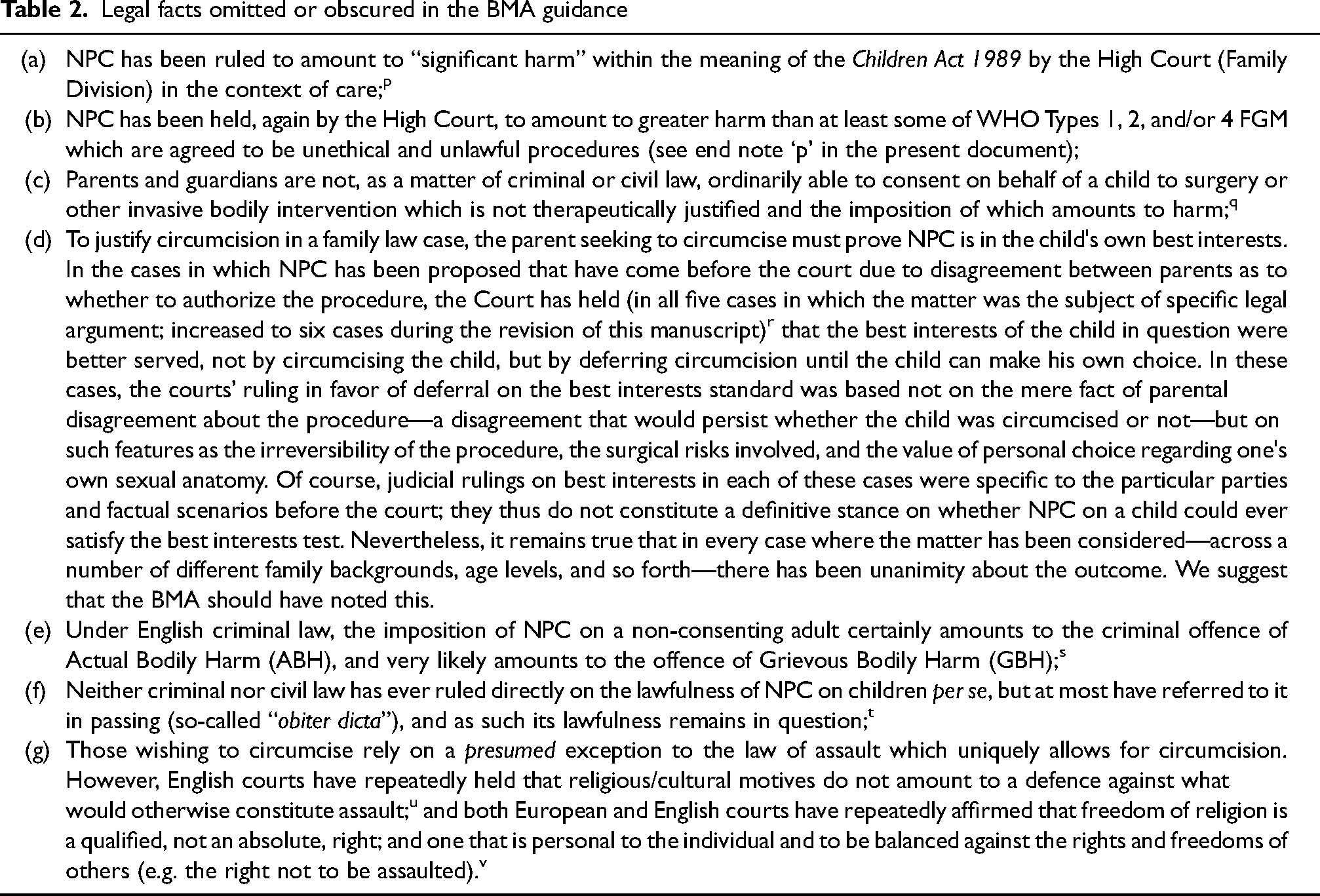
Card 4 asks: “What does the law say about NPC?” However, the card does not then answer this question. Instead, it provides only an “assumption” (i.e. that NPC of children is lawful) while simultaneously accepting that this assumption has no foundation in statute and is controversial. There are a number of facts about what the law does say that should have been included. These are elucidated in Table 2.
That the guidance dedicates an entire paragraph to the now very dated opinion of the Law Commission expressed in 1995 is telling. That opinion is twenty-seven years old—produced well before the High Court's identification of material similarity between NPC and some forms of FGM in terms of significant harm (2015), and even before the six cases on NPC and best interests now delivered by the High Court since 1998. As a document almost three decades behind current legal developments, relying on it is at best unhelpful to doctors; at worst, it amounts to the obfuscation of an emerging legal position that has become increasingly clear.
Concern 10—Failure to address recent case law
The passage “Has there been any recent case law?” also has significant omissions. Responsible guidance answering this question should state that since 1998, of the five (now six) cases to deal directly with disputed NPC, all of them have held that the NPC in question was not in the child's best interests, and that the child's best interests are better served by deferral until the child is older and can make their own decision (see Table 2). The High Court's repeated conclusions clearly favoring deferral of NPC to older adolescence or adulthood should be a key part of this guidance. The current guidance, however, nowhere makes this explicit: instead, this information is deducible only if readers roam carefully through different cards and independently collate the outcomes for themselves. That a major fact about High Court rulings on NPC should be so camouflaged within the guidance undermines the guidance's stated aim of providing practical advice for doctors that equips them with relevant information.
It is also significant that, whereas the BMA is unwilling to express a view on the ethics of childhood NPC, the English courts—applying the same basic test as the BMA w —have been able to reach an outcome as to where the child's best interests lie in each of the six cases considered. That judicial decision-makers have repeatedly reached the conclusion that NPC in those cases should be deferred until the child is capable of consenting to it places the BMA's continued unwillingness to do so in question, and the viability of its “neutral” position under ever-greater strain.
Legal facts omitted or obscured in the BMA guidance
Conclusion
We conclude that the BMA 2019 guidance on NPC of children exhibits serious weaknesses. The authors of the guidance seem to have tried to accommodate, or patch over, the polarized stances on NPC within the wider society—ranging from those who are committed to performing NPC on minors for religious reasons, whatever the law may say, to those who argue that non-consensual NPC, like non-consensual female genital cutting of any kind, is an impermissible bodily assault. Ultimately, such patchwork cannot hold together the inconsistent and contradictory status quo. The “balancing test” the BMA proposes for evaluating the medical ethics of child NPC would, if applied to WHO-defined FGM—especially the subtypes involving “only” the prepuce or labia—yield the conclusion that cutting or removal of these healthy tissues from a non-consenting child's vulva could permissibly be performed if the parents request it for cultural or religious reasons.
For now, the BMA has sought to “bracket” this problem by appealing to the explicit illegality of FGM of every type. Yet this just shifts the inconsistency onto the law, where cracks are beginning to form as well. We propose that, going forward, both in law and medical ethics, children of all sexes and genders will have to be treated equally with respect to parental decision-making about medically unnecessary genital surgeries. Either “minor” forms of FGM will have to be allowed, as prominent defenders of child NPC are increasingly proposing,4,5,25,169–174 or NPC of minors will have to be brought into closer alignment with existing standards applied to other practices. 175 It is our view that a consistent application of widely-accepted medical ethics, safeguarding, legal and human rights principles should result in equal protection for all children from all forms of non-therapeutic genital cutting practices to which they cannot consent.
Footnotes
Acknowledgment
The authors wish to thank John McMillan for helpful feedback on an earlier version of this essay.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The BMA’s main policy-making body is the Annual Representatives Meeting (ARM). Author AL has been a BMA representative since 2009 during which time he has attended each ARM, for which he has requested motions for debate on NPC; in that time there has been no ARM debate around BMA policy on NPC.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.