
Abstract
Some care home residents with dementia have the capacity, some do not. Staff may need to make decisions about administering care interventions to someone whom they believe lacks the capacity to consent to it, but also resists the intervention. Such intervention can be termed
Keywords
Introduction
It is estimated that 3.2% of people over the age of 65 in the UK reside in care homes 1 and of this population around 69.0% (62.7% for males and 71.2% for females) 2 are living with dementia. Care home residents with dementia have complex care needs in comparison with residents without dementia. 3 One of the main differences relates to lack of capacity and consequent difficulties in consenting to treatments and interventions. The advent of the Mental Capacity Act (MCA) 2005 in England and Wales, with its subsequent guidance and relevant case law, has brought about a step-change in understanding how to approach decision-making for those who lack requisite capacity. However, the implementation of the Act has been roundly criticized, 4 and there is evidence that capacity and lack of capacity are confusing and poorly understood issues for many professionals. 5
Some care home residents with a diagnosis of dementia will have the capacity to make decisions, some will not. If a person does not have the capacity to make a decision, the MCA outlines the process by which decisions must be made in the person's ‘best interests’. Depending on the circumstances, various different people may be called upon to contribute to the process of decision-making for the person who lacks capacity. Generally, for decisions around daily care, the decision-maker will be the carer directly involved. Care staff may make ‘best interests’ decisions for matters relating to personal care (e.g. issues such as washing, dressing and feeding), as well as for healthcare decisions, such as those involving the administration of medications which have been properly prescribed by someone with suitable training. 6
There are times when staff in care homes may have to make decisions about administering such types of care to residents whom they believe to lack the necessary capacity to consent to the intervention, but who also resist it. When care is given in the person's best interests (the person lacking the requisite capacity to decide for or against the intervention) despite his or her refusal to accept such care, it can be termed
Forced care is a type of restraint. 7 Restraint is defined by the MCA as ‘the use or threat of force to help do an act which the person resists, or the restriction of the person's liberty of movement, whether or not they resist’. 7 The Commission for Social Care Inspection (CSCI) defines forced care as the act of ‘restraining a resident so that personal care may be carried out, forced feeding or making people take medications’. 8
The use of restraint in people who lack capacity is considered acceptable, or at least free from the threat of liability, provided that, before applying restraint, less restrictive options have been considered, 9 and that any restraint applied is both necessary to prevent harm and is proportionate. 10
Restraint is frequently used in care homes and is usually carried out by paid, non-medically qualified care staff. 11 According to the Francis Report 12 and to Transforming Care, 13 the evidence suggests that restraint is underreported and not routinely included as part of individual residents’ care plans. The Commission for Social Care Inspection investigations into restraint within care homes concluded that the more impaired the individual, the more likely they were to be the subject of restraint. 14
The work of Sells and Howarth 15 (2014) has highlighted how ‘forced care’ tends not to be considered within the current learning materials provided to train care home staff. In addition, the information given to staff does not seem to lead to improved staff awareness of guidance.
While several areas of the concept of restraint in care have been studied (general attitudes to the patient group, 16 risk factors for restraint, 17 training 18 ), there is a lack of published evidence focusing on staff's understanding and approach to the idea of ‘forced care’, particularly from an ethical perspective. This study aims to explore how care staff understand situations of forced care and the thought processes which underpin their decision making. The study also explores knowledge of the principles of the MCA with a view to suggesting appropriate and targeted education.
Methods
A series of 10 semi-structured interviews were conducted with participants currently working within a care home in the North East of England.
Settings and participants
The participants were sampled from one care home in the North East of England. A single care home was considered appropriate for a preliminary study of this nature.
The frame was criterion based, 19 as selection to the study depended on the characteristics of interest. We targeted care staff working within the home with a mix of genders and lengths of employment to enable collection from as diverse a range as possible. The demographic details of the participants are shown in Table 1.
Demographic details of participants.
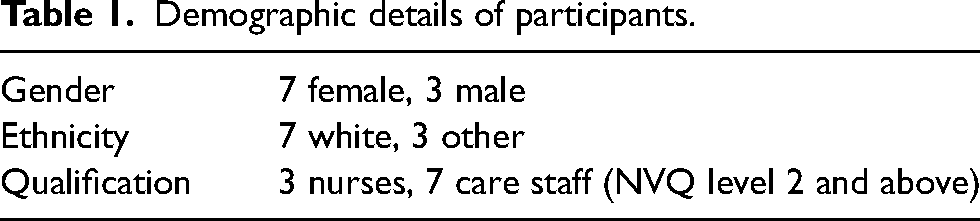
The participants had spent a broad range of time in care, from 4 months to 38 years.
Prior to entering the home for research, permission was sought from the management of the care home to undertake the project. The researcher (AF) advertised the study through posters and flyers as well as verbally to the staff during several visits. Eligible staff were targeted by identifying permanent staff working in the unit for cognitively impaired residents. Participant Information Sheets (PISs) were then distributed to the staff within the care home. This included the purpose of the study, the area of interest, what would be required on the part of the participants (1:1 anonymized, recorded interviews with the researcher). The prospective participants were not provided with a copy of the interview schedule in advance.
Twenty-four hours were given for the staff members to assimilate the information before the researcher made contact for recruitment. It was made clear that there was no obligation to be involved in the study, and that there would be no feedback to the manager if they declined to participate. Written consent was taken before each individual interview. A total of 15 prospective participants were approached and 10 were willing to participate and were included in the study. No one dropped out after recruitment.
As part of the formal ethical application, we also considered the theoretical possibility of any issues arising unexpectedly relating to a participant or resident's safety and outlined a strategy for reporting this, using the local safeguarding vulnerable adults guidance. This was highlighted on the PIS.
While this research did not involve the care home residents as subjects, they were present during the time that the researcher was present within the home. Therefore, residents and relatives were informed of the nature of the study and provided with written information.
Data collection
The interview process was preceded by a short period of observation (2 weeks) in the care home by the researcher. This period allowed staff members to become familiar with the researcher and enabled the researcher to become familiar with the environment and gain a general impression about the types of forced care encounters that were most common in the home.
After this period, the researcher conducted one-to-one semi-structured interviews, using a fictional case study (based on a familiar episode of forced care). They were asked to provide details of (i) how they thought through the particular challenges faced, (ii) their ideas about the term ‘forced care’, (iii) discussion around their reactions to a fictional but familiar case vignette of a situation of forced care, (iv) their rationale for the importance of care giving in dementia and (v) their understanding of concepts of capacity and decision-making in dementia (the principles of the MCA).
The interviews took place within the care home setting and lasted between 30 min and 1 h and were recorded using an encrypted audio recording device. The data was transcribed verbatim and anonymized. Participants were given an opportunity to expand or clarify any points made during their interview both during, and at the end of the interview. Each participant was interviewed once.
After being interviewed, each participant was given a debriefing (verbal and in writing), thanking them for their participation and asking that they did not discuss either the interview questions or their own answers with other staff members until the data collection had been concluded. They were also given contact information for the lead researcher in the event that they later became worried about the issues raised within the study, and also, if they wished to have a copy of the finished piece of research.
Data analysis
Thematic content analysis was used to analyse the data. 19 After initial readings and reflections, themes were identified and sorted according to codes. Interviews continued during this process in order to achieve saturation of data themes. The data set was then analysed as a whole and the content was arranged into broad themes. Coding, analysis and interpretation were reviewed by JH and SW. Reflective notes were taken and reviewed throughout the process.
Results
The themes from the interviews which were most relevant to the participant’s ideas regarding forced care were: (a) rejection of the term itself, (b) need for flexibility of approach in dementia care, (b) need for personal knowledge of the recipients of care, (d) justification for their actions as being rooted in valuing the recipient of care as a person, (e) justification in the need to avoid distress, (f) ideas about these persons having limited autonomy and finally, (g) how assessments of capacity were understood.
Dislike of the term ‘Forced Care’
From the 10 face-to-face interviews undertaken with the participants, there was a general rejection of the term ‘forced care’ when it was used in the interviews. Participants misunderstood the extent of what could be termed forced care, believing that it was physical and either extreme or denoted forms of abuse. Staff tended to reject the use of the term ‘forced care’ on the grounds that it implied to them care that would cause distress. H: I don't like it, its awful … you just do what you can causing them as little distress as possible
F: To me its pushing or like its abuse
A: Forcing them to eat … things like that. Its quite alarming and I didn’t know whether it was appropriate to use the term
A minority identified that care could be covert and did not have to carry ideas of overt force against resistance, but that it was a form of restraint. E: I suppose the nearest we would come is like covert medication, ‘cause that's like restraint’.
After rejecting the term as descriptive of their work, participants described various approaches which they employed in order to gain the compliance of residents.
Methods of bringing about the desired outcome
Flexibility of approach
The participants spoke of the need to afford time and space to situations where providing care was challenging, and spoke of how they would frequently modify both their own expectations of the resident and the actual tasks themselves. C: With everything we have to go with them, we cannot make them do our own routine; we have to change ourselves into their way.
All participants interviewed were asked to address a scenario of forced care, which involved a resident repeatedly refusing a shower (with consequent risks associated with poor hygiene) and so seeming likely to require restraint. Most participants interviewed rejected the need for any overt physical restraint, identifying the need for flexibility, and explained that they would ‘think around the situation’ by practical problem-solving and provide a compromise or more acceptable alternative, such as changing the times of day for washing, getting to know the residents’ bathing preferences and so on. D: I would find out why she doesn’t want a shower, she might prefer a bath, she might not like the person who is bathing her.
Those who volunteered that restraint may be necessary also highlighted the fact that they too would employ a more flexible approach before reaching the decision to restrain (i.e. exhausting other alternatives first). B: So if they are refusing me, we have one resident, she doesn’t really like men at all, she will get agitated, so I just have to get someone else to do it.
Personal knowledge of residents
Participants emphasized the importance of personal knowledge of the person being cared for. A: I think it is very important to know your resident, you can anticipate a lot … they have a whole life of experiences.
C: First of all ask her, if she is not capable of that, you just watch her, by then you should know who she is and what she is about and what she likes
C: I would go through her history, how she was before, and you know we have to look at that
Participants identified care plans and consultation with families as means of gaining this insight. E: It’s important to talk to their families, find out preferred routines … Families can be very helpful – so they can say ‘well Mam always had her baths on Friday nights, you know, after Corrie’*
*‘Corrie’ refers to ‘Coronation Street’, a television soap opera, and care staff used this knowledge to encourage a person to accept care, but by modifying their interventions into the routine she was used to.
They also emphasized the importance of building up a relationship and rapport with the person being cared for (which could not be gained purely by reading about them in a care document), in order to serve their needs best I: You can have conversations about their family … we talk, and they come back to themselves, like we can be like friends
Care staff of all levels of experience made reference to the importance of their interactions with the residents and there being a value in the relationship which could be nurtured and then called upon to reassure a resident who was refusing an intervention.
Justification for actions
The interviews then attempted to focus on deeper issues behind the treatment of residents in specific ways by questioning how staff justified their views. Their justifications tended to group under three headings: the intrinsic worth (value) of the individual; the need to avoid distress; and the ability of residents to retain some decision-making capability (autonomy) despite dementia.
Value as a person
All participants repeatedly voiced beliefs that the residents should not be subject to distress or force, because they had value as ‘fellow persons’. They made links with treating their residents in ways in which they themselves would wish to be treated, or indeed the way that they would wish a loved one to be treated. A: They’ve got their dignity. You know, I wouldn’t like anybody to take me into the shower room and start stripping me
B: I always feel like, ok, this is my grandma
J: Think what you are doing, think, if that was your mam, how would you like your mam to be tret (sic)?
The participants made statements about treating residents as ‘human beings’ or that the residents’ humanity carried an intrinsic worth, which endured despite their illnesses. A: At the end of the day, just because they’ve got dementia, they are people, and you’ve got to respect that.
H: I thought it would be easier caring for somebody who is not related to you, but it isn’t because they are still a person
Some ideas of the worth of the residents were also derived from the residents’ rich history or personal story. A: I think it’s about respect. I think a lot of people with dementia don’t know what they are doing, they don’t know what you are saying to them, but it does matter, they have a whole life of experiences.
Avoidance of harm and distress
Participants gave priority to managing potential harm. Harm was defined as causing distress to a person and was generally considered to be in the form of physical suffering. Once harm was considered likely by the carer, they would then speak about being required to make a decision regarding what was considered to be in the person's best interests. A: You have to make sure that the residents are safe.
In situations where a person was refusing care but was judged to lack capacity then the participants talked of ‘getting the job done’. This variously comprised diversion tactics, avoidance of confrontation and methods of limited/partial information giving, in order to gain compliance. C: Talk to them about their interests and take their mind off the task that you are doing so you do what you need to do really.
E: If its medication I will usually hold it to one side, come back later, try a different approach. Try when they have maybe calmed down, or have been diverted to something different
I: Maybe they don’t like to be toileted, so I’ll ask them to go for a walk … and she will stand up and follow you … then she is going to follow you … before she realizes.
The justification of what is, in effect a form of forced care, but which was considered by care staff as more ‘benign coercion’ or ‘covert care’ techniques was repeatedly brought up as the correct course of action. Staff thought that provided the distress to the resident was minimal it was acceptable and justified as it brought about the desired endpoint (i.e. the care intervention was carried out). C: Sometimes l have to have a different role and change my character in different ways to make them happy. I feel like sometimes I’m one of the family
C: If they don’t know I’m (X) and they are thinking oh, I’m their granddaughter, then I go with the flow
F: Don’t argue because that will irritate them, just change the subject … it calms them down and you can get them ready, ‘cause they let you do it’
Promotion of autonomy
The other factor which was included within the interviews as justification for their actions was the need to allow residents to express their preferences in an attempt to promote some decision-making capacity.
In the context of providing and consenting to care interventions, participants felt that it was important to consider patients’ decision-making capabilities, but within the limits of what they were able to do. This was judged by the care staff themselves. A: They’ve still got choices
Participants made frequent allowances for individual preferences in their work routines by allowing residents to have some say in timings of bathing or getting up and in the expression of preferences. C: Who are we to say you should bath in the morning, everybody's different, so you look at their preferences
G: There's one didn't like to take the dentures out ‘til late, but that's up to him, I would respect whatever decision they make’.
Some participants described how complex care tasks could be broken down into sub-tasks with the possibility that the resident could consent for each component. For example, instead of overwhelming them with the whole issue of washing and grooming, they would explain each part, for example, undressing, and gaining consent, before completing this and moving on to the next stage. F: You just gently take them through the steps one at (a) time, like ‘I’m taking your top off, I’m taking your bottoms off’
Mental capacity
These ideas about autonomy were further explored in relation to the participant's knowledge of the formal assessment of mental capacity under the MCA.
Direct questions relating to the assessment of mental capacity yielded several points. Capacity was often presumed not to be present by virtue of the fact that the person had a dementia diagnosis. H: I think you go by their diagnosis; they’ve got dementia and they don’t understand things
Again, B: If they can understand you, and when they say things to you and it makes sense, I will say, she will have a little bit of capacity
However, during B: If they are refusing care, is it because they don't want it or are they just saying it: do they really know?
E: I suppose each decision you have to look at the capacity – haven’t you?
E: I don’t think she was able to weigh the information to make an informed choice
Participants sought guidance from others, either within the hierarchy in the home, that is, deference to nurses or seniors, or within documentation, for example, care plans. E: Obviously you have capacity assessments that have been done, everybody has an assessment
A: If you can’t get around the situation, I would go to the manager and see what she says and I would take advice.
Discussion
The participants reacted negatively to the term ‘forced care’, and there was a general feeling that it was either not representative of the actual events around caring for those without capacity or that it was a form of abuse and not legal. It was uniformly equated with physical restraint. Participants described their practice as generally avoiding situations where there was overt restraint, opting to take a more flexible approach to situations 20 by either modifying their own behaviour and expectations, or, at times, using covert techniques 21 (which are, of course, also a form of restraint) in order to ensure that their desired outcome was met. Their ability to do this was rooted in their emphasis on the need to have a good knowledge of the recipient of care. 22 Justification for the need to provide care did not typically rely on it being the participant's job, although it was linked with job satisfaction. 23 From the discussions there seemed to be an intuitive morality which shone through the descriptions. The participants’ answers were based on the ideas that the recipients of care should be valued because they had intrinsic worth as fellow human beings. 24
In making the decision about what was the right thing to do in situations of forced care, the participants attempted to put themselves in the position of the recipient of care, or alternatively, think about a beloved relative of a similar age, and hypothesize about what they would want. Naturally, when taking such a position, the staff came to different conclusions – either that the care intervention in question was not completely essential and so forced care was not appropriate, or, that the right course of action was to ensure that the intervention was given. There was also some consideration of a need to balance various ethical principles. First, there was the need to respect the right of self-determination or autonomy 25 of patients by giving them some ability to make choices about receiving care. Secondly, this was weighed against the need to avoid doing harm (non-maleficence 26 ). The avoidance of harm was a rather more nuanced consideration, as there were two perspectives considered. Either staff would see avoiding harm as a matter (1) of administering a much-needed intervention (forced care), so as not to cause suffering by an important omission OR (2) of not providing forced care and so avoiding the distress associated with physical restraint.
Ultimately the right decision, according to the staff, was that the recipient of care remained content and was not distressed. In general, causing distress was equated with, first, a lack of respect for the recipient of care, and secondly harm and mal treatment.
Knowledge about the principles of mental capacity and its assessment (under the MCA) yielded varied and at times uncertain answers. It is a challenging point for many professionals. 27 This study suggests that the basic principles of the assessment of capacity – including presumption of capacity unless otherwise demonstrated, were not necessarily in the minds of care staff. Care staff do not have specific training regarding mental capacity as a matter of routine when entering the private care sector in the UK. Indirect, more practically based questions around capacity yielded better identification of some key points set out in the Act. The level of knowledge seems broadly to be in keeping with the MCA Code of practice, which states that ‘carers do not have to be experts in assessing capacity’. 28 They described taking steps to find out if the person could make decisions, including by reference to care plans. 29 Despite not being in receipt of formal training regarding MCA, they also seemed to be aware of the spirit of the MCA, again outlined in Section 6 of the guidance, by making attempts to ‘get around’ many difficult situations rather than directly applying any form of restraint.
It is worth emphasizing that forced care can be within the spirit of the MCA inasmuch as it aims at the best interests of the residents, where best interests are properly understood, 30 where the least restrictive options have been considered, and where any restraint applied is both necessary to prevent harm and proportionate. The authors have known cases where staff in care homes have refrained from providing necessary care because some form of restraint would be required. Understandable queasiness over the term ‘forced care’ should not obscure the requirement that good care might sometimes involve restraint which inherently involves force. Of course, good behavioural techniques must be considered first as part of seeking to implement the least restrictive means of care. 31
Strengths and limitations
The population of care staff within the UK are a large and diverse group, with extremely varied backgrounds and levels of training. This research attempted to gain as diverse a sample as possible within the research frame, as well as interviewing until saturation of themes was attained. This was considered acceptable for our purposes: a small scale, a preliminary project aimed at generating data concerning the perspectives of care staff on forced care, and potentially informing further work in this area. As a small piece of qualitative research, the study does not carry with it statistical power or generalizability. Involvement of a range of locations and more staff would likely yield a broad and interesting range of backgrounds and levels of training, as well as differing attitudes dependent on location and different care homes each manifesting a different ‘ethos’.
There was the possibility of selection bias – with those with a clearer sense of the ethical issues and ability to reflect or indeed better professional practice coming forward to be interviewed. Despite this, the results showed a broad range of perspectives, and multiple different answers to the research questions. The lack of previous research on this topic has also presented challenges in verifying the data through triangulation. Further work is therefore required. Larger-scale studies may address these limitations and may provide alternative perspectives.
Conclusion
This study has shown lacunae in terms of overtly expressed knowledge of the principles of the MCA that would support the use of forced care under specific circumstances. Equally, it has demonstrated appropriate approaches and nuanced thinking by nurses and care staff about how to deal with residents in a care home who require interventions but who lack the capacity to consent and are inclined to refuse the interventions. Although not always justifying their attitudes in the terms set out in the MCA, many of their behaviours, at least as described and witnessed by the researcher, were in fact in accord with the spirit of the MCA.
With regard to recommendations for future practice, there is a mixed understanding of the concept of forced care, restraint and the MCA. This may be as a result of several possible factors; lack of training, 18 training which is pitched at a level that does not suit the individuals, training given at a time or in a way which does not immediately link with the care staff's experiences ‘on the ground’. Care staff and care homes should be encouraged to have discussions and even local training courses on the principles of MCA and restraint, possibly focusing on specific scenarios or making clear the relevance to their practice. Naturally, we would not want this to result in another addition to an already full list of training requirements, but rather to be of genuine value in their practice.
Footnotes
Acknowledgements
The authors acknowledge and thank all participants and the care home manager who facilitated this research.
Ethical considerations
This study was approved by Newcastle University’s Ethics Committee.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Appendix 1
Please could you have a look at this made-up case. Hopefully it's the kind of situation that you are familiar with. Once you have read through it, I have some questions about how you would think about this type of situation. Nora is 80 years old and is living in a care home. She has had dementia for around 5 years, and now needs full care support for washing, dressing and eating. Over the last few months, she has become less willing to allow the staff to help her wash in the mornings. This used to be part of her usual routine, but she has started to become distressed and physically resist the care staff when they attempt to wash her. The care staff attempted to give Nora a shower, but this required several staff members, as she was verbally and physically aggressive towards them, and distressed during the shower.