
Abstract
Disputes over life-sustaining treatment between clinicians and patients or their surrogates are common in the intensive care unit and expected to increase in America because of an aging population, shifts in medical training, and trends in popular opinions on end-of-life decisions. Clinicians struggle to effectively communicate the recommendation that withdrawing life-sustaining treatment is appropriate when the burdens of treatment outweigh the benefits. This view seems foreign and unimaginable to surrogates like family members with deeply held values motivate them to insist “everything be done” as long as the patient can be physiologically kept alive. For over three decades now, clinicians and bioethicists have sought preventative ethical and policy solutions to avoid or resolve these treatment disputes, including efforts to improve the communication between medical professionals and surrogates. Looking at the history of proposed solutions shows that giving providers more and better communication and negotiation tools may be inadequate on its own. However, better communication has the potential to unearth the motivations and deeper values of the disagreeing parties so that differing perspectives can be recognized and common ground can be established. The latest emphasize on communication has the potential to succeed where other historical solutions have failed. If bioethics is going to successfully analyze and remedy these disputes, the values motivating these views, even ones outside the bioethical consensus, must be acknowledged and respected. In short, better communication will not avoid or resolve life-sustaining treatment disputes in the intensive care unit unless the deeper ethical convictions of the disagreeing parties are recognized and engaged.
Keywords
Introduction
Disputes over life-sustaining treatment (LST) between medical professionals and patients or their surrogates are not only familiar to those seeking to manage them through ethics consultations, but also to bioethicists and clinicians seeking preventive ethical and policy solutions. The typical case is when a family is requesting to continue invasive mechanical ventilation through the physician advises against it. Physicians, ethics committee members, and even chaplains attempt to explain that from their perspective the most ethical decision is to withdraw LST since the burdens of the treatment outweigh the benefits. However, this perspective coming from medical professionals may be foreign to the patient's family members whose deeply held values are motivating them to insist “everything be done” to keep their loved one alive.
When interviewing nearly 2000 Americans from across the country in 2013, the Pew Research Center found 35% of US adults would want their doctors to “do everything possible to save their lives” if they suffer from “an incurable disease and were suffering a great deal of pain.” 1 This was an uptick from 28% of US adults choosing this option in 1990. 1 This represents the views of thousands of surrogates and family members who may disagree with the physician when making LST decisions for their loved ones in the intensive care unit (ICU) every year.
Several attempts have been made to avoid or resolve this impasse, one approach is improving the communication between medical professionals and surrogates. 2 However, these efforts to give providers more and better communication and negotiation tools seem to be inadequate on their own to address ICU disputes. Better communication has the potential to unearth the motivations and deeper values of the disagreeing parties so that differing perspectives can be recognized and common ground can be established. The problem is that the recent focus on communication does not seek to assist medical practitioners and bioethicists to engage the motivations and ethical principles of the patients or surrogates. Americans who have little interaction with the ICU or medical institutions hold the common position that the paramount goal of medicine and any medical intervention is the prolongation of physiological life. As observed in the history of the discussion of potential solutions, if bioethics is going to successfully analyze and remedy these disputes, the values motivating these views, even ones outside the mainstream bioethical consensus, must be seriously engaged with and respected. In short, better communication will not avoid or resolve LST disputes unless the deeper ethical convictions of the disagreeing parties are recognized and engaged.
Autonomy and surrogates
Patients who possess the capacity ought to make medical decisions about LST without controlling influences. 3 This is the essence of the bioethical principle of respect for autonomy, which Beauchamp describes as acknowledging patient's “right to hold views, to make choices, and to take actions based on their values and beliefs.” 4
When the patient lacks the capacity to make their own medical decisions, a surrogate is recognized as the key decision maker through the patient's own documentation or state laws that grant specific individuals automatic jurisdiction. 3 Clinicians have the legal and ethical duty to identify and inform the surrogate decision maker of the three-tiered standard they should utilize: (1) follow the patient's explicit directives, (2) honor their inferred values, or (3) at the very least seek the patient's best interest. 3 Following the second tier constitutes reflecting on related beliefs and values of the patient to determine how they would assess their current circumstance. For example, deducing the patient would not want to be on LST for an extended amount of time since they hated being a burden to others when they were ill. This is why Beauchamp explains that “the family's role should be primary because it presumed identification with the patient's interests, depth of concern about the patient and intimated knowledge of his or her wishes.” 4 Accordingly, some state laws outline the order of priority that adults related to the patient ought to serve as a surrogate if none was explicitly appointed by the patient. 3 In the cases when the patient's preferences and values are not recorded in a directive or explicit instructions have not been given to the surrogate decision-maker, the surrogate must use substituted judgment relying on their knowledge and experience of the patient's life, values, and beliefs in order to infer what the patient would decide if competent. In the absence of either of these, the third standard of “best interests” must be used, when the surrogate must make medical decisions based on what they believe will be in the patient's best interest “in light of the patient's condition, prognosis, and treatment options.” 3 Sometimes this duty to decide based on the patient's best interest is framed as choosing “what a ‘reasonable person’ would choose if in the patient's circumstance.” 3 Although it is their responsibility ethically and legally, when a surrogate is making medical decisions for a patient based on these third-level criteria, they obviously require the expertise, insight, and even recommendation of the attending medical professionals to properly assess those relevant factors of “best interest” listed above.
Conflicts over LST in the ICU
Decisions about initiating, continuing, withholding, or withdrawing life-sustaining treatment are so fundamental to the well-being and dignity of the patient that disputes among various family members, surrogates, and medical professionals are inevitable. The majority of these disputes in the ICU are between members of the medical team providing care for the patient and the patient's family or surrogate.5–7 One study published in 2013 surveyed over 900 surgeons to examine conflicts in the ICU with patients, surrogates, or other clinicians. The study showed that 70% of the ICU clinicians surveyed reported conflicts within the previous week. 8 Another study surveyed patients showed that out of 650 patients in the ICU, over the third experienced major conflicts about LST specifically. 9
In the last 40 years, these types of conflicts have been rising in number, not declining. Some experts have even referred to these disputes as having reached “epidemic proportions.” 10 Thaddeus Pope argues that these disputes, which he refers to as “medical futility disputes,” are high according to surveys of ethics consultations in US hospitals. 11 However, Pope expects the volume of these disputes to increase due to multiple factors, like an aging population and that “physicians are increasingly more likely to recommend comfort care” instead of LST because of the new emphasis on palliative care in medical training and reimbursement incentives. 11 One contributing factor responsible for this is the growing dominance of the ethical principle of patient autonomy in the late 20th century aided by the “patient's rights” cases such as Quinlan (1976) and Cruzan (1988). These cases not only spurred more academic attention to the topics but also emboldened patients and surrogates to defend their rights to medical self-determination.
According to Jeffrey Burns and Robert Truog, little theoretical or procedural progress has been made in bioethics and medicine after at least 40 years of the practical and ethical wrestling with this issue. 2 This is a problem since although these disagreements are common, they are greatly consequential. As Pope observes, “disputes over life-sustaining medical treatment involve life-and-death stakes.” 12
These disagreements are also important because how they are approached shape the public's perception of health care institutions and professionals more broadly. Thirdly, some have argued that the most pressing reason for finding a solution to these disputes affect medical professionals. As one commentator wrote, this dilemma “represents a true threat to clinicians’ moral integrity,” and our approach and framing of them “may be important in its own right, without necessarily considering consequences for patients.”
History of solutions
Burns and Truog summarize the history of the academic discussion and policy experiments seeking to resolve or avoid these disputes. 2 These efforts evolved through three stages or generations. The first generation, from the 1980s to the mid-1990s, focused on establishing a consensus definition for “medical futility.” A widely accepted standard would provide physicians the clarity and confidence to counter medical requests they believe to be futile or “overtreatment.” Standardization would have strengthened the position of medical professionals in disputes with patients or surrogates over LST, empowering them to refuse treatment that was not within the accepted standard. However, by the early 1990s, the near impossibility of achieving medical consensus became clear.
Mildred Solomon conducted large studies on how health care professionals approach decision-making near the end of life. Through analyzing the transcripts of her in-depth interviews with physicians she reflected on how the term “medically futile,” which is often utilized in these conflicts, “has become a euphemism for an authoritative way to communicate, evaluative judgments based on quality of life considerations, only rarely to designate treatments that were medically inefficacious.” 13 In 2015 multiple medical societies released a statement on the topic, led by the American Thoracic Society. The recommendations included institutional processes to avoid “intractable treatment conflicts,” and replacing the term “futile” with “potentially inappropriate” except when describing physiologically ineffective interventions. They wrote, “the assertion being made by clinicians depends both on technical medical expertise and a value-laden claim, rather than strictly a technical judgment.” 14 This position statement resulted in a shift in terminology. Instead of labeling the treatment in question as “futile” or “medically contraindicated,” such treatment is deemed potentially “medically inappropriate.” 14 One study defines the “perceive[d] inappropriateness of care” as “clashes with [the clinician's] personal beliefs and/or professional knowledge.” Therefore, it is easy to see the difficulty of patients, surrogates, and medical professionals understanding and taking on the other's perspective in these value-laden disagreements. The failure of the first generation to arrive at a consensus was related to the nature of these judgments and disagreements that go beyond physical diagnosis and prognosis.
In the mid-1990s, the second generation of debate and recommendations focused on developing procedural protocols outlining a process, rather than a definition, for physicians and healthcare facilities to follow. While compliance with a protocol to negotiate disagreements could show a good faith effort, it could not shield the medical professionals from protracted value-laden disputes of LST, and potential litigation. At the height of this second generation, a group of hospitals in Houston, Texas developed a city-wide futility policy that became the basis for a groundbreaking state law. The ad hoc task force developing the policy was made up of 18 representatives from 14 hospitals and institutions, mostly representatives from their institutions’ ethics committees.
15
The policy laid out step-by-step requirements for a physician to follow if they hold that a requested medical intervention is medically inappropriate. Provided the steps are followed, the physician is not required to initiate or continue the intervention in question. The group explained that the procedural approach acknowledges there are deeper value-laden disagreements, but seeks to give one set of values the upper hand. Amir Halevy and Baruch Brody wrote that it was, an unfounded value judgment that patient autonomy is inviolate and must always trump other legitimate competing values. The ultimate question is not whether a futility policy is value free, but whether it is based on defensible values.
16
The new “process-based policy” was adopted into Texas state law in 1999 with the substantial addition of legal immunity. 17 The Texas Advance Directives Act (TADA) provided a legal safe harbor for medical professionals to withdraw LST requested by the patient or patient's surrogate they deemed “inappropriate” as long as their process is followed. This model was praised for being the “first such law in the country to provide a process for resolving disputes about end-of-life care, in particular in the area of medical futility.” 18
These efforts realized that at the heart of these LST disputes was the need to fairly balance competing values and ethical perspectives. However, critics like Thaddeus Pope argue that the “most significant fairness problem with TADA” is that this approach gives “decision making power to the hospital's very own internal review committee.” This allowed for one ethical perspective to prevail even if both sides were not fully engaged or recognized. The criticism from bioethicists, legal scholars, and others was that these procedural protocols had no neutral and independent arbiter to help the parties with differing values come to a solution. These criticisms prevented the wide-spread adoption of the second generation's legislative solution to resolve futility disputes. Pope summarizes the significant legal and bioethical criticism concluding that TADA “fails to comply with core ethical and legal notions of fundamental fairness.” 19
Better communication as a solution
Burns and Truog explain that because of these failures with the second-generation solutions, by 2010 experts had begun the third wave of attempts to resolve medical futility disputes with better communication and negotiation. Renewed efforts to improve communication between all parties involved, especially providers and surrogates, turned to negotiation practices and principles from other fields, like business and legal professions, dealing with “highly charged situations” to “mitigate conflicts as they arise before they become intractable.” 2
The value of better communication between medical professionals and patients or surrogates cannot be disputed. This is a far more promising solution than the second generation that allows one party and set of values to trump the other. It is widely acknowledged that miscommunication causes multiple negative outcomes and circumstances in the provider–surrogate relationships. 20 Many have concluded “poor communication” is the main source of LST conflict. 6 Numerous studies and surveys seeking to understand conflicts in the ICU over LST find a breakdown of communication and therefore a deterioration of trust 20 After reviewing many studies examining the affect this has on physician–family relationships, Jenny Way observed, “the needs of relatives of intensive care patients indicate that the most important needs relate to communication and include having questions answered honestly, understanding the diagnosis and prognosis, and having information explained in understandable terms.” 21
The official recommendations by ATS on “Responding to Requests for Potentially Inappropriate Treatments in Intensive Care Units” explained that “clinicians and patients/surrogates should work collaboratively to make treatment decisions and, in the face of disagreement, should first augment efforts to find a negotiated agreement.” 14 The statement focuses on practical tools including “proactive communication strategies” like “listening closely to surrogates,” “discussing the patient's prognosis in clear, jargon-free language,” “explain[ing the] principles of surrogate decision making,” and involving consultants who are “skilled in mediation and conflict resolution.” 14 Furthermore, the statement claimed, “most disagreements in ICUs arise not from intractable value conflicts but from breakdowns in communication that are amenable to communication interventions.” 14
While bioethicists and medical experts need to continue to focus on communication training and the tools to improve these conversations, like relaying medical information to surrogates in a better way, dismissing values motivating a conflict could have negative consequences. Some of the new training and discussion of communication tools that focus on the surface interventions have been criticized as nothing more than manipulation. One qualitative study found through interviews that physicians adopt different negotiation methods to manage disagreements with patients or surrogates including everything from acquiescing to families to “pushing hard, biding time, [and] changing the conversation.” 22 This study found the pitfalls for physicians who come into discussions with families about treatment decisions with a predetermined agenda. 22 The study revealed that often the communication between the two parties was not the exchange of information, discussion of values, working toward an agreement, but instead an effort to bend the family to the medical recommendations or bide one's time until they could be persuaded. 22
Way acknowledges the presence of deeper motivations beneath communication when she concludes, “Conflict can be constructive,” as long as they reveal “differences in values and legitimate concerns that have been inadequately discussed.” However, she then continues, “Improved communication about goals, prognoses, and treatment options will successfully resolve most conflicts and may minimise unrealistic requests by patients or families.” 21
If minimizing unrealistic requests is the true motivation of these methods, “ then one might expect “better communication” to devolve into conflict resolution. This is not truly better communication but arbitrating a disagreement. Michael Hartwick and Gwynne Jones argue, “the health care team must first listen and attempt to understand [the patient or family's] picture before communicating their thoughts on the current diagnosis and prognosis and how this may impact on the patient's life.”
23
They explain that the most effective communication methods start with the exchange of listening and discussion early in the admission or relationship in order to form trust and “a sense of common purpose.”
23
They call for a renewed effort and innovation to be invested in, practical, tangible strategies to equip critical care providers with excellent communication and conflict resolution skills. It is these skills that allow the clinician to weave the humanity and the science of life together. Communication skills that resolve goals of care in a clear, compassionate and transparent fashion, promote good decisions that are congruent with the patient's life.
23
Hartwick and Jones acknowledge that conflict resolution and communication are about more than just pushing hard, biding time, or “minimizing unrealistic requests.” Instead, there must also be the goal to acknowledge the human aspect involved, not just the medical insight or prognosis. Addressing the “goals of care in a clear, compassionate and transparent fashion,” to “promote good decisions that are congruent with the patient's life” is actually getting down to what Burns and Truog call the “underpinnings of conflict” over whether continuing the treatment is inappropriate. 2 If the third generation of approaches to LST disputes is going to be successful it ought to focus on the values of the parties in disagreement, which lie below surface-level communication skills and tools.
Values beneath the communication
When reviewing the history of efforts to avoid or resolve disputes over LST, Burns, and Truog conclude, “the medical profession needs to evolve new strategies to resolving questions of futility.” 2 These “new strategies” should follow “a more nuanced view of the underpinnings of conflicts over medical decision making.” 2 Those “underpinnings” can be found in the values beneath the communication and negotiation between disagreeing parties in the ICU. Ignoring these underpinnings contributed to the failure in the previous generations of attempted solutions.
Ideally, the purpose of better communication is not acquiescence, but to allowing both parties to arrive at a new understanding and appreciate the position and values of those engaged in the disagreement. Sissel Steihaug and colleagues claim that “communication is about sharing and establishing common ground.” 24 Arriving at the common ground is not the same as arriving at an agreement. The ideal functioning of the type of communication they suggest is “recognition” of the other. They explain, “recognition implies/means that the other's inner world of experience is focused and appreciated as relevant just because the other is a human being.” 24 This could be a more expansive explanation of what Hartwick referred to as that weaving of “humanity and the science of life.” 23
Once this recognition is accomplished, Steihaug argues that surface-level disagreement is not damaging to the relationship or likelihood of a resolution. Based on this view, it is possible that disagreement between medical professionals and surrogates in the ICU over LST, is typically damaging because the parties have not recognized one another nor do they see the values or humanity of the other. This is a different type of “communication skill” or “negotiation tool” that does not just try to clearly relay relevant information in an understandable way or try to push hard, but instead seeks to “understand and take the other's perspective.” 24
Multiple “perspectives” are presented in these disputes between surrogates and medical professionals over LST in the ICU that must be recognized. Brody and Halevy describe the values they perceive in play during these LST disputes. They write, “health care professionals and health care institutions have values and principles, as much as a patient and families do.”
16
They point to the surrogate's “value of patient autonomy” which prohibits medical professionals from forcing unwanted treatment on patients, and most importantly, Brody and Halevy point to the physician's value of “professional integrity.” The value of the physician's professional integrity “grounds a prohibition on patients and families from forcing providers and institutions to provide treatments they judge inappropriate.”
16
The American Thoracic Society and other organizations summarized the competing values, writing, Patients have an interest in receiving care consistent with their values and preferences. Clinicians have an interest in not being compelled to act against their best understanding of their professional obligations.
14
Physicians being asked to provide treatment that causes harm without compensating benefit is “unseemly” like multiple amputation, or care that represents a poor stewardship of resources, which could violate their professional integrity. Brody and Halevy seem to identify the values and motivations at the heart of these medical disputes as ethical determinations, not simply questions about the efficacy of an intervention. In these disagreements, there is really a conflict between visions of what is in the best interest of the patient, which transcends the question of whether an intervention is physiologically ineffective. This is the realization that caused the shift in the terminology to “inappropriate care” and away from “futile care,” which clarifies the medical professional's perspective is also ethical in nature.
Though both parties have the patient's best interest in mind, the chasm between the physician's ethical outlook and the surrogate's values and priorities is sizable. A study by Anders Rydvall and Niels Lynöe investigates the similarities and differences of the public and medical professionals on the leading values and reasoning central to decisions about LST The study found significant disagreements between the two groups concerning points as fundamental as the first task of health care and views on the quality of life in critical medical conditions. 25 Rydvall and Lynöe's key finding is that “In order to avoid unnecessary dispute and miscommunication, doctors must better understand the nature of the views held by the general public (and hence those of patients’ relatives), and their expectations and preferences.” 25 Rydvall and Lynöe assert that having a better understanding of the general public's perspective would positively effect the physician–surrogate relationship.
But, Steihaug and others seem to be calling for something more demanding on physicians. They argue that physicians must “understand and take the other's perspective.” When this occurs, disagreement, even attempts to explain their position, does not have to be damaging, when it “is based on solid medical knowledge and with a fundamental respect for the patient's experience perspective.” 24 This is a difficult task for multiple reasons.
As stated by Brody and Halevy and reiterated in the ATS-led statement, the recommendation to withhold or withdraw LST in the ICU is not simply a determination of whether the treatment is no longer effective or physiologically futile. In fact, the dispute arises from the reality that the LST is physiologically effective and the physician expects the treatment to continue prolonging a state of harm for the patient that is not outweighed by the benefits. “Solid medical knowledge” can only determine the extent of the harm and the benefits caused or promised by the treatment. An additional ethical consideration must be made about the relationship of those two factors. This is generally a personal moral choice, determining whether the negative effects or outcomes are worth enduring for the specific positive effect or promised outcome. This is why when commenting on the new process approach to disputes over LST in the ICU (discussed above), the American Medical Association “insists on giving priority to patient or proxy assessments of worthwhile outcome.” 26
Although this is technically the responsibility of the surrogate, especially in cases when there are no explicit directives or information to reflect the patient's values, priorities, and preferences, it is engrained in the nature of the medical staff's profession to develop their own convictions about what is in the patient's best interest For the medical professionals caring for the patient, they have additional duties to follow the other biomedical principles of nonmaleficence and beneficence. 4 Not only are medical professionals’ charges with avoiding causing evil or harm to the patient (like subjecting them to LST that is hastening their death), but also they have the positive duty to prevent harm and promote the good of the patient. 4
Because of the moral nature of these medical decisions and these other value-laden factors of the decisions around LST, the patient's surrogate and the medical professionals could have fundamentally divergent views about what constitutes “best interest,” which commonly is assumed to be most easily ascertained by their surrogates familiar with the patient's values, priorities, and beliefs.
27
The inevitable conflict is that the perspective of medical professionals and the public concerning what course of action regarding LST is “best” for a patient are quite distinct. A qualitative study by Hashim M. Mehter showed that physicians relied on multiple key factors when determining the appropriateness of “aggressively treating” patients in the ICU and thus whether they sought to persuade families otherwise.
22
The leading factors were the physician's perspective on the quality of the surrogate's “substituted judgment and the perception of patient suffering.”
22
Mehter summarizes his study's conclusion that, In the case of conflict, our study suggests that although physicians do take family preferences into account, their approach to decision-making may be driven by the goal of achieving the outcome that the healthcare team believes to be in the patient's best interests—often the withholding or withdrawal of life support or other aggressive treatments when meaningful recovery is unlikely.
22
It is not surprising that these ethical values concerning the patient's best interest motivate physicians “perceived appropriateness” of LST for patients in the ICU. In this sense, both parties do share a common purpose, which better communication could reveal, and help “recognize” and take on the surrogate or family's perspective. Physicians need to be further equipped to see that this value-level communication and respect is a substantial part of their duty to the patient. Otherwise, this disagreement could lead to unjustified decisions by medical professionals since it has been shown that physicians more often than not make inaccurate assumptions about patients’ and surrogates’ preferences and motivating values based on the patient's age and quality of life. 21
So, when analyzing disputes over LST in the ICU, we see both parties have similar goals (best interest of the patient), but one main factor is that medical staff may have a differing perspective on whether the prolongation of life alone is a legitimate benefit of the medical intervention for the patient unlike the attitudes found the general public. 1 Medical professional more readily conclude “that slim chances of life are not always better than dying.” 28 Instead, they hold that “providing comfort, avoiding painful and unhelpful medical treatments” is sometimes “the best that medicine can do, and the only ethical course.” 28 This ethical conclusion could be difficult to understand for those not immersed in the medical community or those that do not see the trauma of the ICU day in and day out. This disconnect between medical professionals and the public could also be caused by how these notions of burdens, benefits, futility, and the prolongation of life have been discussed and development in contemporary bioethics.
Valuing prolonging life in bioethics
The overwhelming consensus of clinicians and ethicists (secular and religious alike) is that the prolongation of life is merely one potential medical benefit among many. In Principles of Biomedical Ethics, Tom Beauchamp and James Childress argue that the core principles of nonmaleficence and beneficence do not automatically “establish a presumption in favor of providing LST for sick and injured patients.”
4
They claim that there is no obligation to always provide or choose treatment like a ventilator or artificially administered nutrition and hydration (AANH). They explain, The use of life-sustaining treatments occasionally violates patients’ interests. For example, pain can be so severe and physical restraints so burdensome that these factors outweigh anticipated benefits, such as a brief prolongation of life. Providing the treatment may then be inhumane or cruel.
4
Beauchamp and Childress see potential medical conditions that are so painful and burdensome that “a brief prolongation of life” as not ethically justified. In fact, choosing life-prolonging treatment could actually be unethical, according to Beauchamp and Childress. This is consistent with the standards of medical care that have been widely accepted for at least two decades. The Hastings Center Guidelines for Decisions on Life-Sustaining Treatment and Care Near the End of Life urges clinicians to assist patients and surrogates to review the relative benefits and burdens of all presented treatment options. In the list of potential benefits that individual patients may consider, the Guidelines include, “the opportunity to live longer, if the quality of prolonged life is acceptable to the individual patient” (see chart). 3
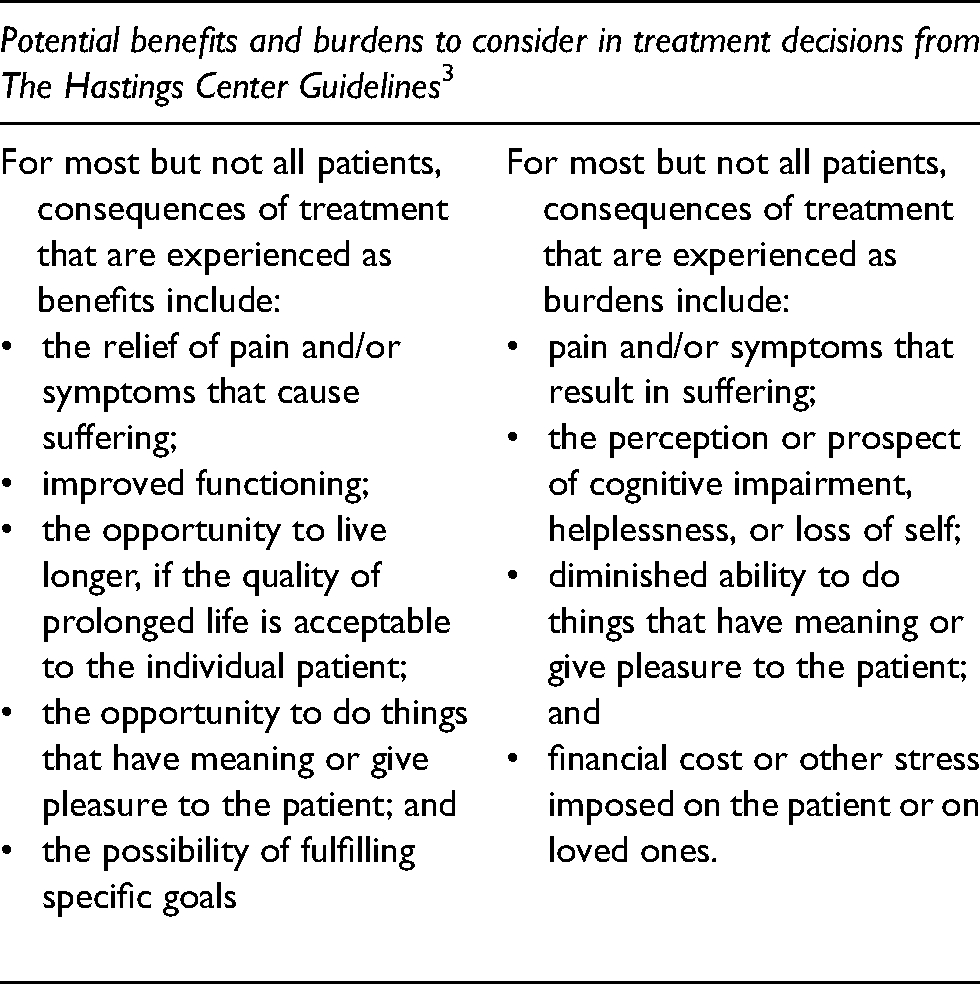
When assessing treatment goals, and the associated potential benefits and burdens, the most lay public would not merely list “the opportunity to live longer” as a singular benefit amongst a series of similarly weighted values. As shown in the study by Rydvall and Lynöe, most in the general public consider the prolongation of life to easily outweigh most, if not all, of the potential burdens of treatment. 1 However, even when listing the benefit of continued life, the Guidelines add the caveat “if the quality of prolonged life is acceptable.” For many, continuing to live, even with “diminished abilities,” “helplessness,” or “pain,” is the paramount “interest.”
In order to seek recognition, to understand, and take on patient and surrogates’ perspectives on the prolongation of life (regardless of the quality), bioethicists ought to explore further potential causes or motivations for these values (for example worldviews that expand the burden and benefit analysis beyond mere physical pain and suffering). In the limited literature engaging these perspectives, bioethicists too often point to religion as the cause of their view that the prolongation of life is the ultimate benefit of medical intervention. In a 2008 article discussing trends of end-of-life decisions in the global west, Robert Truog criticizes “religious fundamentalism and the associated vitalistic view about the sanctity of life.” 29 He warned that a cultural break from “secular humanism that has characterized Western Civilization since the Enlightenment of the seventeenth century” and the reemergence of religious fundamentalism will cause many more medical conflicts over LST Truog argued that the widely-accepted views of Beauchamp, Childress, and the Hastings Center were at odds with certain religious views that are regaining cultural popularity.
Preparing for differing ethical values
Many different types of patients and surrogates, religious and non-religious, are motivated by deeply-held values in these disputes. One of these is the position that the mere prolongation of life is an ethically legitimate benefit of LST in the ICU. These values and the decisions they lead to must be further explored in bioethics and in medical practice to make progress in analyzing and resolving disputes about LST in the ICU. Both bioethicists and medical professionals ought to find alternatives to dismissing this view or seeking to use communication skills to persuade them to change their perspective. Complete agreement on these values or perspectives is not necessary for recognition and respect. Dominic Wilkinson and others challenge the commonly held position that decisions about LST at the end of a patient's life must only be done in the midst of consensus.
28
The authors explore various ethical theories used to support this view and propose a new ethical framework to create space for the difference of opinions in medical professional guidelines and protocols. Practically, they argue that medical teams should be free to discuss multiple options or perspectives with the patient and surrogate, rather than assuming there is only one “medical perspective.” They write, As already noted, there is a range of different values that patients bring to end-of life decisions. These values lead individuals to make different decisions. There is epistemic uncertainty, for example, about the effectiveness of treatment, or the patient's quality of life if they survive, or about what exactly the patient would have wanted in a given circumstance. And there is normative (moral) uncertainty, about which moral rules or principles or frameworks should be applied, and in which way. The important consequence is that we should not seek the single and only right course of action in many cases but rather examine whether there are a range of reasonable courses of action over which patients/families may exercise choice. It is a mistake to think there is always one course, and that a group of clinicians can identify it.
28
Wilkinson concludes that practically, clinicians should be more open-minded and accepting of a different perspective because of uncertainty about a treatments effectiveness and the patient's quality of life. These factors (discussed above) should lead us to examine disputes in the ICU in a new ethical lens that leads to truly “new strategies.” Approaches like Wilkinson's “medical dissensus” and John Rawl's vision for rational deliberation will help us accept and respond to the clash of patient and professional values in LST decisions.
One of the recommendations from the 2015 ATS-led statement is “increased efforts to teach clinicians end-of-life communication skills, including strategies to achieve shared decision making, conflict resolution skills, and skills to emotionally support surrogates facing difficult decisions.” 14 While these surface-level skills are good, cultivating the other type of communication that recognizes the perspective of all parties involved in conflicts, and “promote good decisions that are congruent with the patient's life” may be more beneficial. 23 This will require teaching medical students and clinicians new ways to engage, clearly communicate prognosis, and how to take on other's perspectives. In addition to improved, more deliberate communication and negotiation skills, this training ought to aim to equip clinicians on how to recognize “the other's world of experience” and engage with their values.
While this deeper dive into the other perspective and values could seem too demanding for medical students and our institutions, this type of discernment is typical in a medical professional's common practice. Clinicians oftentimes surmise and evaluate the motives of surrogates in ICUs making LST decisions to protect the interests of the patient. For example, physicians are rightly less likely to agree with a surrogate opting to withdraw LST from a patient if it was clear the surrogate would financially gain from the decision. Part of the physician's duty is to protect patients from potentially bad faith motives or dangerous perspectives that could play into disagreements over the withdrawal or continuation of LST. 30 So, asking a medical student or physician to consider the perspective of the patient and surrogates is not too demanding, but part of responsible medical practice.
Medical and bioethical education may not be able to be expose students to all the diverse values and ethical perspectives outside the medical and bioethical consensus. However, these skills will prepare them to genuinely engage with different motivating values like seeing the prolongation of life as the ultimate goal of medicine and any medical intervention. This type of training should also be extended to ethics consultants. These individuals cannot be left out of this new training since as Pope points out, several leading U.S. medical centers have reported that medical futility disputes comprise a significant percentage of their annual ethics consults: thirteen percent at Memorial Sloan Kettering, twenty-nine percent at the University of Michigan Health System. Stanford's Lucile Packard Children's Hospital and the Mayo Clinic have reported similar percentages.
11
Medical professionals and large percentages of the public may have differing values driving their approach to end-of-life decisions, including views on the exact ethical weight of prolonging life with burdensome medical interventions. However, various perspectives can still be respected and given a room in the ICU and field of bioethics. One promising way forward is to look beneath the surface-level communication skills and seek those deeper goals of recognition and respect beneath the conflicts and arbitration the disputes usually get stuck in.