
Abstract
During a pandemic, demand for intensive care often exceeds availability. Experts agree that allocation should maximize benefits and must not be based on whether patients could have taken preventive measures. However, intensive care units (ICUs) are often overburdened by individuals with severe COVID-19 who have chosen not to be vaccinated to prevent the disease. This article reports an experiment that investigated the German public's prioritization preferences during the fourth wave of the coronavirus pandemic (N = 1014). In a series of scenarios, participants were asked to decide on ICU admission for patients who differed in terms of health condition, expected treatment benefits, and vaccination status. The results reveal an in-group bias, as vaccinated individuals preferred to allocate more resources to the vaccinated than to the unvaccinated. Participants also favored admitting a heart attack patient rather than a COVID-19 patient with the same likelihood of benefiting from ICU admission, indicating a preference for maintaining regular ICU services rather than treating those with severe COVID-19. Finally, participants were more likely to admit a patient to intensive care when this meant withholding rather than withdrawing care from another patient. The results indicate that lay prioritizations violate established allocation principles, presaging potential conflicts between those in need of intensive care and those who provide and allocate it. It is therefore recommended that allocation principles should be explained to enhance public understanding. Additionally, vaccination rates should be increased to relieve ICUs and reduce the need for such triage decisions.
Introduction
When COVID-19 began to spread in 2020, intensive care units (ICUs) filled rapidly, and there were images of crowded hospitals across the world turning away severely infected patients. 1 The approval and rollout of vaccines was perceived as a turning point. As vaccination reduces the chances of critical infection and transmission of the disease, 2 experts called on governments to vaccinate at least 85% of the population.3,4 To date, vaccination rates in most countries have failed to reach this target; for instance, despite extensive efforts to ease, promote, and incentivize vaccination, rates in the United States were below 60% in November 2020. 5 Similarly, vaccination rates in Germany have settled at around 70%, which was not enough to prevent a fourth drastic surge of infections and deaths. 6 As ICUs filled again and hospitals had to turn away patients with severe conditions like intracerebral hemorrhage, 7 discussion turned to the allocation of intensive care beds. Should unvaccinated patients with severe COVID-19 be deprioritized for admission when there are too few ICU beds for all of those in need?
As the provision of intensive care requires significant resources, ICU capacity is necessarily limited, and ICU beds are generally reserved for patients whose recovery depends on this high level of care. Typically, patients who are expected to recover outside ICU and those who are expected to die regardless of medical intervention are not admitted.
8
However, despite this emphasis on specific prognoses, ICU capacity may be insufficient from time to time, and when demand for intensive care exceeds the available capacity, triage is required. Persad et al.
9
identified four basic principles for allocating scarce medical resources.
Maximizing benefits (utilitarianism): According to this principle, intensive care should be allocated to those who are most likely to benefit. Maximizing benefits can be understood as saving the greatest number of individual lives or preserving the most life years by prioritizing those who are expected to survive longest and with reasonable quality of life following treatment. Clearly, this latter decision depends on information about patient age as well as prior medical conditions and comorbidities. Favoring the worst off (prioritarianism): This principle favors the allocation of scarce resources to patients with the worst prospects if left untreated, disregarding post-treatment prognoses. Although this typically means prioritizing the sickest, it can also mean favoring younger patients, who are considered to be in greater need because they will potentially lose more life years. Treating people equally (egalitarianism): On this principle, all patients should have equal access to intensive care. This can be achieved by implementing a first-come-first-served rule or a lottery system that randomly assigns ICU capacity in conditions of scarcity. Promoting and rewarding instrumental value (instrumentalism): This principle prioritizes certain patients in order to maintain critical infrastructures. For instance, healthcare workers may be privileged because they may save others in the future.
As no single principle can adequately incorporate all of the morally relevant considerations, allocation systems typically invoke multiple principles. However, approaches to selecting, weighting, and operationalizing principles vary across interventions.10,11 In the case of ICU admission, scholars agree that the most important concern is to maximize benefits.8,12,13 Given the constraints on time and information during a pandemic, it is reasonable to maximize the number of patients likely to survive treatment with a reasonable life expectancy by prioritizing younger individuals with fewer coexisting conditions for admission to intensive care. Similarly, it seems reasonable to prioritize healthcare professionals and other key workers over other occupational groups.
12
Patients with similar prognoses (and similar instrumental value) should be treated equally by implementing random allocation. In other words, triage decisions should not be influenced by a patient's wealth or social status or by any personal relationship with medical staff.
8
As triage systems do not typically take into account of whether patients are to blame for their condition, allocation of intensive care should be no different for patients with COVID-19 and those with other severe conditions like heart failure, stroke, or cancer. 12 Although there would have been significantly fewer hospitalizations during the COVID-19 pandemic if everyone was vaccinated against the disease, unvaccinated patients with severe COVID-19 are nevertheless entitled to intensive care. Imagine, for example, that two comparable persons are competing for an ICU bed: one with COVID-19 and one who has suffered a heart attack. According to the above principles, there should be no clear preference, as both are equally sick and would benefit to a comparable extent from intensive care. In this case, random selection is justified. However, some laypeople might disagree with this recommendation. In countries where vaccination against COVID-19 is readily accessible and available to everyone, high incidence of severe infection and the need for triage could easily be avoided. Previous research has shown that people are blamed for their own health problems when perceived as irresponsible. 14 In the above example, one might expect vaccinated individuals to prioritize a heart attack patient over an unvaccinated person with severe COVID-19.
Allocation preferences may also be driven by perceived prosociality. Vaccinated individuals typically perceive those who are not vaccinated against infectious diseases as antisocial and favor penalties for this free-riding behavior. 15 In this view, vaccinated patients would be prioritized, irrespective of diagnosis. If laypeople assign different priorities on the basis of vaccination status, one question that arises is whether they would apply these criteria for patients with differing prognoses. For instance, if an unvaccinated patient with COVID-19 is more likely to benefit from intensive care than a vaccinated heart attack patient (perhaps because he is younger), the principle of maximum benefit implies that the COVID-19 patient should be prioritized. However, on the grounds of reciprocity and responsibility discussed above, some laypeople might disagree, especially if they are themselves vaccinated.
As public support is vital for the successful implementation of any approach to resource allocation, 16 we conducted a survey-based experiment to examine the German public's preferences regarding admission to intensive care. In a series of scenarios, participants were asked repeatedly to decide between patients who differed in terms of health condition, expected treatment benefits, and vaccination status. We further investigated whether those decisions varied when patients were to be prioritized for available versus depleted resources. In general, experts agree that it is ethically permissible to reallocate critical care to someone who is more likely to benefit.17,18 Although there is no medical or moral difference between withholding and withdrawing intensive care, the latter often incurs a higher emotional tax. 19 Consequently, allocation preferences of the public could be biased against the withdrawal of medical resources too. Our study was designed to identify any such bias among the German public. In exploring lay preferences in the context of medical ethical dilemmas, it was not our intention to criticize or propose any revision of well-founded principles for resource allocation. Instead, we hope the results will inform communication strategies to explain and justify triage procedures, thereby increasing public understanding and support.
Method
Participants and research design
The experiment was conducted in Germany during the fourth wave of the coronavirus pandemic (November 16–17, 2021) as part of the COVID-19 Snapshot Monitoring (COSMO) cross-sectional study series. 20 Participants were recruited from a non-probabilistic sample (N = 1014), which was quota-representative for age × gender and federal state. Participants ranged in age from 18 to 74 years (M = 44.69, SD = 15.49) and included 497 males and 517 females. A large majority (87%, n = 878) had already been vaccinated against COVID-19. Participants were randomly assigned to one of two experimental conditions: equal versus unequal likelihood of benefit from intensive care for patients with COVID-19 and heart failure.
Procedure and materials
After assessing the relevant information about demographics and vaccination status, participants were asked to complete a series of allocation decisions in two distinct scenarios and to evaluate the extent of different patients’ own responsibility for requiring intensive care.
Scenario 1: allocation of intensive care
In the first scenario, all participants were told that many intensive care units were reaching their capacity limit because of the high incidence of coronavirus cases. They were asked to imagine that two patients needed the only available ICU bed, which meant that intensive care would be withheld from one of them. Participants in the equal likelihood of benefit group were told that the two patients were similar, that their chances of survival without intensive care were comparably low, and that both would benefit equally from an ICU bed. In the unequal likelihood of benefit group, participants were told that the two patients were similar but that their chances of survival without intensive treatment might differ. They were further asked to imagine that intensive care was expected to stabilize all patients equally well—that is, all would have the same probability of survival with intensive treatment.
After reading the relevant information, participants in both groups were asked to make a series of six consecutive decisions prioritizing one of two patients for intensive care. In total, there were four patients competing against each other: a vaccinated and unvaccinated patient with COVID-19 and a vaccinated and unvaccinated heart attack patient. In the equal likelihood of benefit condition, participants were told only the patients’ diagnosis and vaccination status. In the unequal likelihood of benefit group, participants were also told that the COVID-19 patients had a 25% probability of survival without intensive care while the heart attack patients had a 50% chance. In each case, the order of presentation of decisions and patients was randomized.
Scenario 2: reallocation of intensive care
In the second scenario, participants were asked to imagine that all beds in an ICU were occupied by unvaccinated patients with COVID-19 and that a vaccinated heart attack patient had shown up. As in scenario 1, participants in the equal likelihood of benefit condition were told that the chances of survival without intensive care were comparably low for all patients and that all patients would benefit equally from being admitted to the ICU. Accordingly, participants in the unequal likelihood of benefit condition were asked to imagine that the COVID-19 patients had a 25% probability of survival without intensive care while the heart attack patients had a 50% chance. Again, they were asked to imagine that all patients would have the same probability of survival if admitted to the ICU, indicating a higher likelihood of benefit for the COVID-19 patients. After reading the relevant information, all participants were asked to decide whether the vaccinated heart attack patient should be admitted to intensive care, which would mean reallocating resources withdrawn from one of the unvaccinated COVID-19 patients. Again, the order of the two options (admitting vs. not admitting the heart attack patient) was randomized.
Blaming patients
Participants were also asked to assess the extent of four patients’ responsibility for their poor state of health and their need for admission to the ICU. As in scenario 1, the question related to a vaccinated and unvaccinated patient with COVID-19 and a vaccinated and unvaccinated heart attack patient. Participants were asked to respond on Likert-type scales ranging from 1 (not to blame at all) to 5 (very much to blame).
Results
Allocation decisions
A log-linear Bradley–Terry model 21 was used to estimate average patient priority from the six pairwise comparisons for vaccinated and unvaccinated participants in the two experimental conditions in scenario 1. Figure 1 shows how patients were prioritized—equally, higher, or lower than the baseline of the vaccinated patient with COVID-19 (second row). On average, vaccinated participants in the equal likelihood of benefit condition (left side, black) prioritized vaccinated heart attack patients (first row) above this baseline. Unvaccinated patients with heart attack (third row) and vaccinated patients with COVID-19 were similarly prioritized, and unvaccinated patients with COVID-19 (fourth row) were deprioritized as compared to all other patients. In the unequal likelihood of benefit condition, vaccinated participants (left side, red) assigned lower priority to heart attack patients; that is, heart attack patients who were less likely to benefit from ICU treatment were prioritized at the same level as COVID-19 patients. In this case, priority depended on vaccination status alone, with vaccinated patients prioritized over unvaccinated patients.
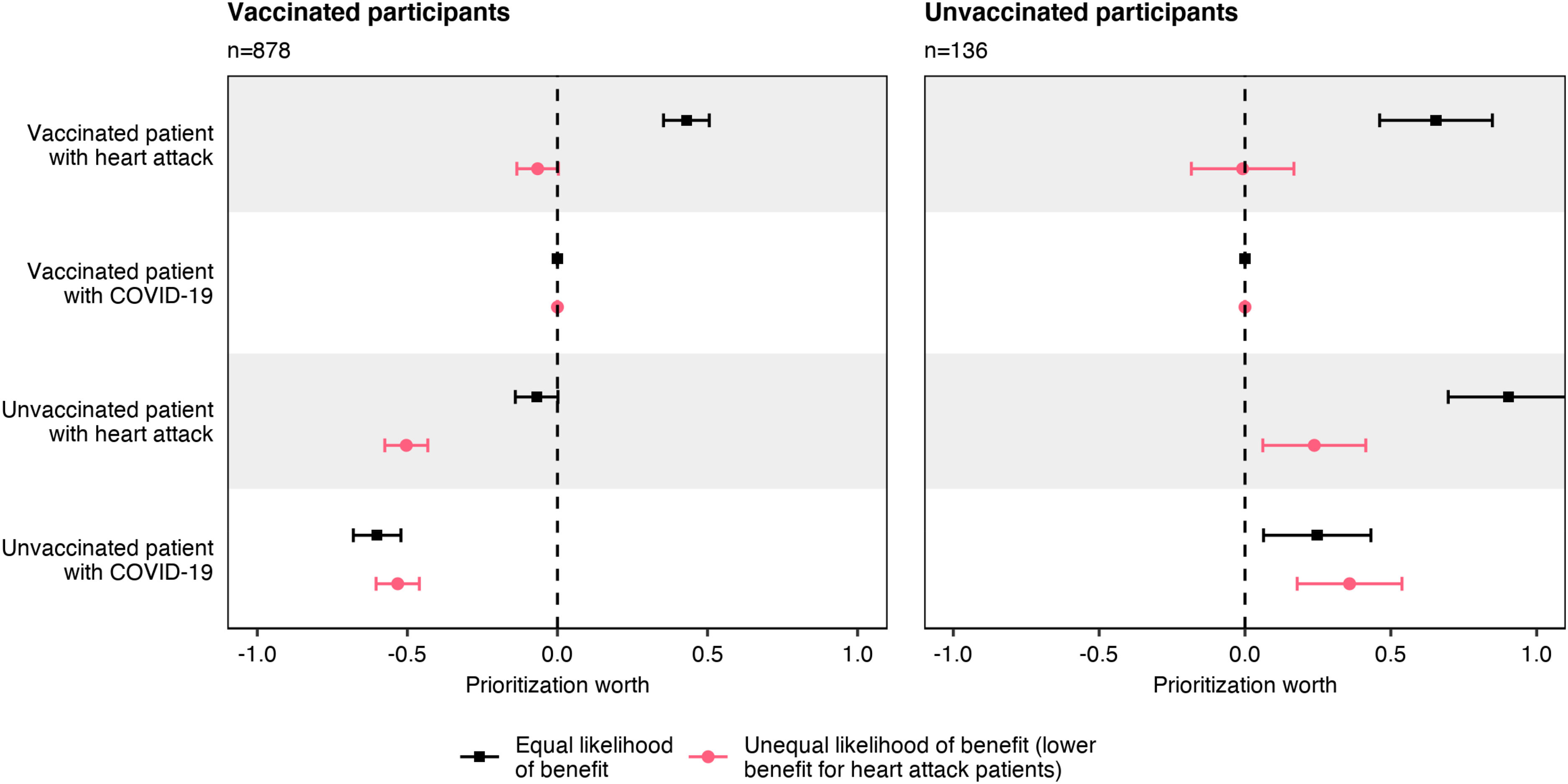
Prioritization for intensive care.
Unvaccinated participants responded differently. In the equal likelihood of benefit condition (right side, black), heart attack patients and unvaccinated patients with COVID-19 were prioritized over vaccinated patients with COVID-19. In the unequal likelihood of benefit condition (right side, red), the assigned priorities differed by vaccination status rather than diagnosis, as unvaccinated patients were prioritized over vaccinated individuals.
Withholding versus withdrawing intensive care
Figure 2 shows how participants decided when intensive care should be allocated to a vaccinated heart attack patient or to an unvaccinated COVID-19 patient. A majority of vaccinated participants (left) prioritized the vaccinated heart attack patient over the unvaccinated patient with COVID-19, regardless of experimental condition or scenario. For unvaccinated participants (right), the vaccinated heart attack patient was assigned above-chance treatment priority in the equal likelihood of benefit condition when care was to be withheld (scenario 1) and below-chance probability in the unequal likelihood of benefit condition when care was to be withdrawn (scenario 2).
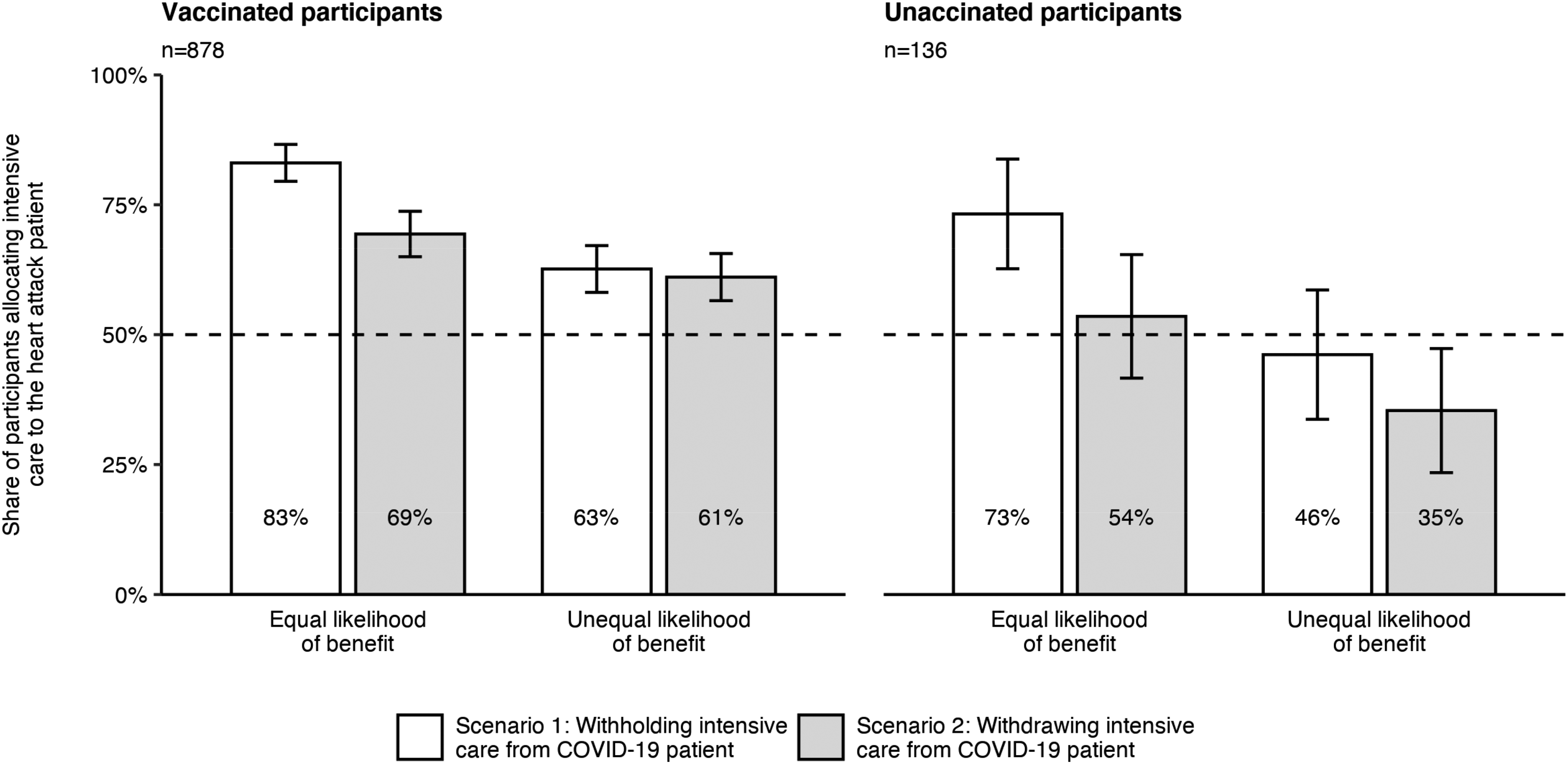
Prioritization of a vaccinated heart attack patient over an unvaccinated patient with COVID-19.
A mixed effects logistic regression was performed to examine differences across participants, experimental conditions, and scenarios. As shown in Table 1, the probability of treating a vaccinated heart attack patient in preference to an unvaccinated patient with COVID-19 increased when participants were vaccinated, when both patients had an equal likelihood of benefit, and when treating the vaccinated heart attack patient meant withholding rather than withdrawing intensive care from an unvaccinated patient with COVID-19.
Predictors of prioritization of a vaccinated heart attack patient over an unvaccinated COVID-19 patient.
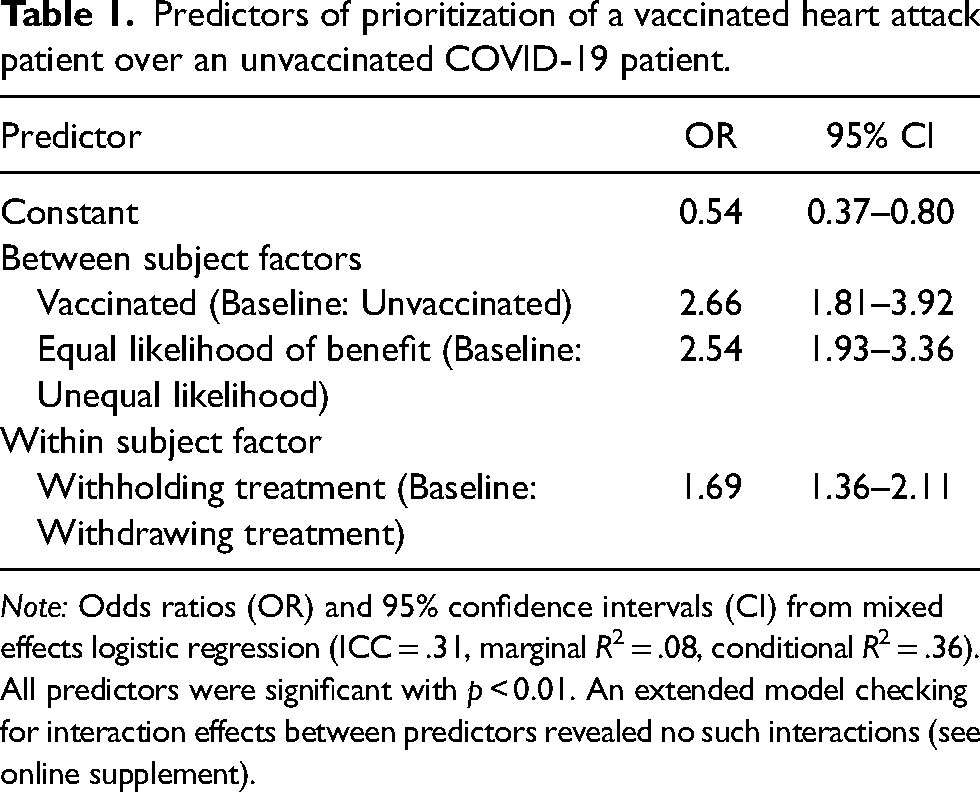
Note: Odds ratios (OR) and 95% confidence intervals (CI) from mixed effects logistic regression (ICC = .31, marginal R2 = .08, conditional R2 = .36). All predictors were significant with p < 0.01. An extended model checking for interaction effects between predictors revealed no such interactions (see online supplement).
Blaming patients for their poor health
Figure 3 shows average blame ratings for the four patient types by diagnosis and vaccination status. Pairwise comparisons of vaccinated and unvaccinated participants’ ratings revealed significant differences regarding unvaccinated patients with COVID-19, t(183.57) = 16.80, p < 0.001, and heart attack, t(205.09) = 4.54, p < 0.001. Although both vaccinated and unvaccinated participants tended not to blame vaccinated patients for their poor health, vaccinated participants were more likely to blame unvaccinated patients, especially those with COVID-19.
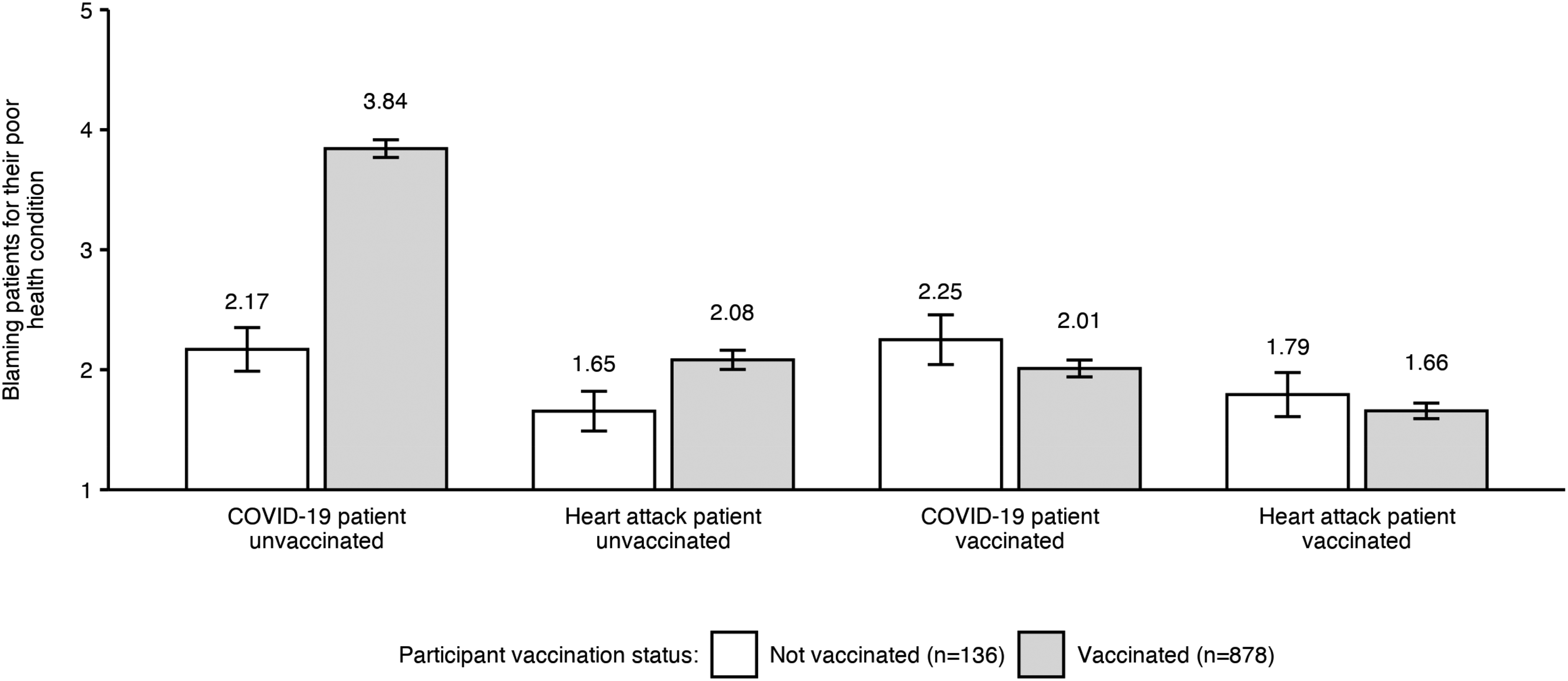
Blame of patients for their poor health.
Discussion
When medical resources are scarce, there is a need to define and implement allocation procedures. In the case of intensive care, experts agree that allocation should be based on the principle of maximizing benefits,8,12 prioritizing patients who would benefit more from ICU admission. This approach is ethically permissible even if it means that intensive care must be withdrawn from another patient.17,18 However, when two patients with a comparable likelihood of benefit compete for intensive care, random selection is often recommended. 9 Although other factors like instrumental value may be taken into account, ethicists agree that patient wealth or social status should not inform decision-making. 8 Assigning blame is also considered unacceptable; that is, patients who are responsible for their own disease must not be deprioritized. 22 It follows that patients should be treated equally regardless of their vaccination status. 12 When an unvaccinated patient with COVID-19 and a vaccinated heart attack patient are equally likely to benefit from intensive care, both should have the same chance for treatment.
However, our data indicate that laypeople may adopt other perspectives, depending on their own vaccination status. Vaccinated participants disagreed with the prevailing professional view by deprioritizing unvaccinated patients with COVID-19 and blaming them for their poor health. Non-vaccination was seen as violating a social contract, 15 and deprioritization can be understood as an act of punishment. Interestingly, when the equal likelihood of benefit was assumed, similar mid-level priority was assigned to the unvaccinated heart attack patient and the vaccinated patient with COVID-19, while the vaccinated heart attack patient was assigned superior priority. Consequently, both vaccination status and diagnosis influenced allocation preference, with heart attack prioritized over COVID-19.
When COVID-19 patients are expected to benefit more than heart attack patients from intensive care, they should be prioritized. In this case, however, participants’ decisions took no account of the diagnosis, confirming discrimination against COVID-19 patients across conditions. A possible explanation is that vaccinated people may prefer to maintain normal ICU services (i.e. for conditions other than COVID-19), distributing only the remaining capacity (if any) to those with COVID-19. In this regard, heart attack is a common cause of ICU admission in nonpandemic times and represents perhaps the central case of emergency admission.
In contrast, unvaccinated participants tended not to blame patients for their health status. However, their prioritization preferences were not driven by benefit considerations alone, as unvaccinated patients with COVID-19 or heart attack were prioritized over vaccinated patients with COVID-19 in both the equal and unequal likelihood of benefit conditions. Overall, the results indicate an in-group bias, 23 as both vaccinated and unvaccinated participants tended to allocate resources according to their own status beyond established allocation principles.
On average, participants preferred withholding rather than withdrawing treatment. Although this approach diverges from ethical considerations,17,18 it aligns with previous evidence regarding the high emotional burden experienced by healthcare workers in withdrawing resources from patients in need. 19 Laypeople are also likely to experience this burden, which would explain the preference for treating a vaccinated heart attack patient when this meant withholding (rather than withdrawing) ICU resources from an unvaccinated COVID-19 patient.
Although our results highlight important differences between lay decision-making and medical ethics regarding intensive care allocation, we must acknowledge some limitations of the present study. First, the allocation decisions were fictitious, and preferences may differ when real lives are at stake. Second, our findings relate to a specific time and context: a German sample surveyed at a time when infection rates and ICU admissions from the delta variant were rising quickly. Future research should investigate prioritization preferences in other countries and cultural contexts, as well as timelines (i.e. during vs. after the current pandemic). Third, our results may have been biased because responsibility indicators were provided for COVID-19 patients but not for heart attack patients. Future research should explore whether lay preferences diverge when taking into account of patients’ vaccination status and other health-related behaviors (e.g. diet, exercise). Fourth, the allocation tasks forced participants to prioritize one patient over another, but research from other domains shows that people often prefer not to participate in clinical decision-making. 24 As there was no option to refrain from allocation or to assign equal priorities, participants who had no preference were obliged to select one patient at random, which means that some answers may not perfectly reflect individual preferences. However, as rankings were analyzed across participants, the results can be considered a reliable representation of allocation preferences among German adults aged less than 75 years.
The discrepancy between allocation recommendations based on a set of established ethical principles and lay preferences suggests some potential for social conflict. To mitigate any such tensions, it seems important to address the underlying problem of low vaccination rates that leads to overburdened ICUs. This can be achieved by (1) communication strategies that persuade unvaccinated people to get vaccinated (e.g. by informing them about the severe effects of infection and potential or actual overburdening of ICUs) and (2) policies that limit the contacts of unvaccinated people or mandate vaccination. However, when new virus strains emerge and the available vaccines prove less effective, the burden on ICUs may remain high even when large parts of the population are vaccinated. Therefore, procedures and principles for allocating intensive care need to be well-documented and clearly communicated to the public. Education campaigns could explain how professional triage decisions are made. They may be complemented with easily accessible information, for example, on hospital websites. Triage may also be addressed in entertainment formats such as medical dramas or documentaries. Efforts should address the discrepancy between established processes and lay preferences by informing the public about the potential disadvantages of including vaccination information in triage decisions. First, this information is not always available and given the constraints on time and information, assessing the vaccination status before admitting severely infected persons to intensive care may not be practicable. Second, including vaccination information in triage decisions means withdrawing resources from patients who are to blame for their bad health. If this principle was applied to other conditions, heart attack patients should be less likely to be admitted to an ICU, too, for example, when they are obese as this could also be considered an avoidable risk factor. 25 In this regard, it may become difficult to justify allocation decisions that focus on vaccination records but do not include other information about patients’ (ir)responsible health behaviors. Explaining these peculiarities to the public may increase support for established triage procedures. Besides large-scale campaigns, individual triage decisions should always be explained to patients and their relatives when seeking care. As this can be an emotionally demanding task, medical personnel should be supported. Clear documentation of allocation procedures and offering conversational trainings may help to decrease the psychological burden.
Footnotes
Acknowledgements
The study was conducted as part of Germany's COVID-19 Snapshot Monitoring (COSMO), a joint project of the University of Erfurt, the Robert Koch Institute, the Federal Centre for Health Education, the Leibniz Institute of Psychology, the Science Media Center, the Bernhard Nocht Institute for Tropical Medicine, and the Yale Institute for Global Health. The authors are grateful to Dr Philipp Felgendreff for the fruitful discussions that inspired this research.
Authors’ note
PS, LK, LF, SE and CB designed the research; PS and LK performed the research; PS planned and performed data analysis; PS wrote the initial draft, which was revised and approved by all authors. Our research obtained ethical clearance from the University of Erfurt's IRB (#20200302/20200501) and all participants provided informed consent prior to data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Klaus Tschira Stiftung, Leibniz Institute for Psychology, Deutsche Forschungsgemeinschaft, Universität Erfurt, Thüringer Staatskanzlei, Robert Koch Institute, Thüringer Ministerium für Wirtschaft, Wissenschaft und Digitale Gesellschaft, Bundeszentrale für gesundheitliche Aufklärung, (grant number no grant/award number, BE3970/11-1, BE3970/12-1).
Supplemental material
Supplemental material for this article is available online.