
Abstract
Background
Physician-assisted suicide is a controversial issue and has sometimes raised emotion-laden reactions. Against this backdrop, we have analyzed how Swedish physicians are reasoning about physician-assisted suicide if it were to be legalized.
Methods and participants
We conducted a cross-sectional study and analyzed 819 randomly selected physicians’ responses from general practitioners, geriatricians, internists, oncologists, psychiatrists, surgeons, and all palliativists. Apart from the main questions about their attitude toward physician-assisted suicide, we also asked what would happen with the respondents’ own trust in healthcare if physician-assisted suicide were legalized. Response options were that trust would decrease, not be influenced, or would increase.
Results
We identified a strong statistical association between on the one hand those whose own trust would increase and who were pro physician-assisted suicide, and on the other hand those who were against physician-assisted suicide and whose own trust would decrease [relative risk: 16.7 (95% confidence interval: 10.2–27.2)]. Among those whose own trust would not be influenced (n = 456), 60% were pro pysician-assisted suicide, 16% were against, and 24% were undecided. Of those whose trust would increase or not be influenced, a large majority supported autonomy-based arguments, whereas those whose trust would decrease supported non-maleficence-based arguments.
Conclusion
Analyzing the answers after having divided respondents into those whose own trust in healthcare would decrease or increase and not be influenced brings about interesting results such as how the three groups prioritize arguments for and against physician-assisted suicide. This way of analyzing the data seems to be a promising strategy when identifying value-impregnated factual claims.
Keywords
Introduction
In most countries, healthcare professionals have a legal right to abstain from performing medical interventions that are contrary to their own conscience or personal values—referred to as conscientious objection.1,2 Examples of medical interventions that could be perceived as issues of conscientious objection are abortions, plastic operations on the hymen for females exposed to honor-related threats, in vitro fertilization of homosexual females, and physician-assisted suicide (PAS) or euthanasia.1–4
In a few countries; however, there is no opportunity of conscientious objection, for instance in Sweden. 4 Here, healthcare professionals are obliged to participate in procedures considered part of their job description, and there is no legal room to refuse with reference to one’s conscience. 4
PAS is not legalized in Sweden. However, other end-of-life decisions, such as discontinuing life-sustaining treatment, are allowed, even if discontinuation would shorten the patient’s life. This is, for instance, the case with patients with tetraplegia who are dependent on a ventilator.5,6 If such a patient wants to discontinue ventilator treatment, healthcare professionals must respect the patient’s wish if the patient is considered decision competent. Because it is evident that discontinuing ventilator treatment in such a case would result in suffocating, deep sedation is offered before the ventilator is switched off.5,6 Not respecting a competent patient’s wishes would imply somatic coercive treatment, which is prohibited in Sweden even though the patient’s life is shortened. Hence, the concerned physicians are supposed to assist such a patient, and to our knowledge, no physician has so far declined to do so.
When it comes to PAS, which typically concerns patients with fatal diagnoses with short life expectancies, some Swedish physicians have an outspoken negative attitude. In a recent survey from 2020, 7 a significantly larger proportion of Swedish physicians supported PAS compared to a similar study conducted in 2007. 8 However, in the 2020 survey, physicians working in specialties such as palliative care and geriatric care tended to be mostly against PAS. 7 The survey also indicated that there are considerable value-based tensions between the physicians who are for and the physicians who are against PAS, both within and between specialties. 7 Previously conducted studies have shown that the more controversial an issue is the more it tends to bring out personal emotional reactions and that personal values are often hidden and tacitly influence the estimation of factual claims.3–5,9,10 The latter claim is partly analogous with the philosophy of science’s claim that observations are influenced or tacitly impregnated by theories.4,5
In the present study, we aimed to elucidate the values at stake when discussing PAS. Both tacitly disguised and openly declared values regarding the controversy of whether or not PAS should be legalized in Sweden are presented and analyzed.
Participants and methods
During the autumn 2020, we conducted a cross-sectional and questionnaire-based survey among the following Swedish clinical specialties: general practitioners, geriatricians, internists, oncologists, psychiatrists, and surgeons. 7 Approximately 240 participants were randomly selected from each of these specialties including the whole country, and on average 60% responded. Because palliative medicine became a new specialty in 2015, all were included (n = 123). In total, 934 physicians responded, of which 115 of the responses were based on a final short version of the questionnaire. The questionnaire was distributed three times—with 10-day intervals—at full length, but a final version was shorter to obtain more responses regarding the two main questions. Apart from the figures in Tables 1 and 2, which include all respondents who responded to these questions, the numbers of responses to all other issues are based on 819 full responses.
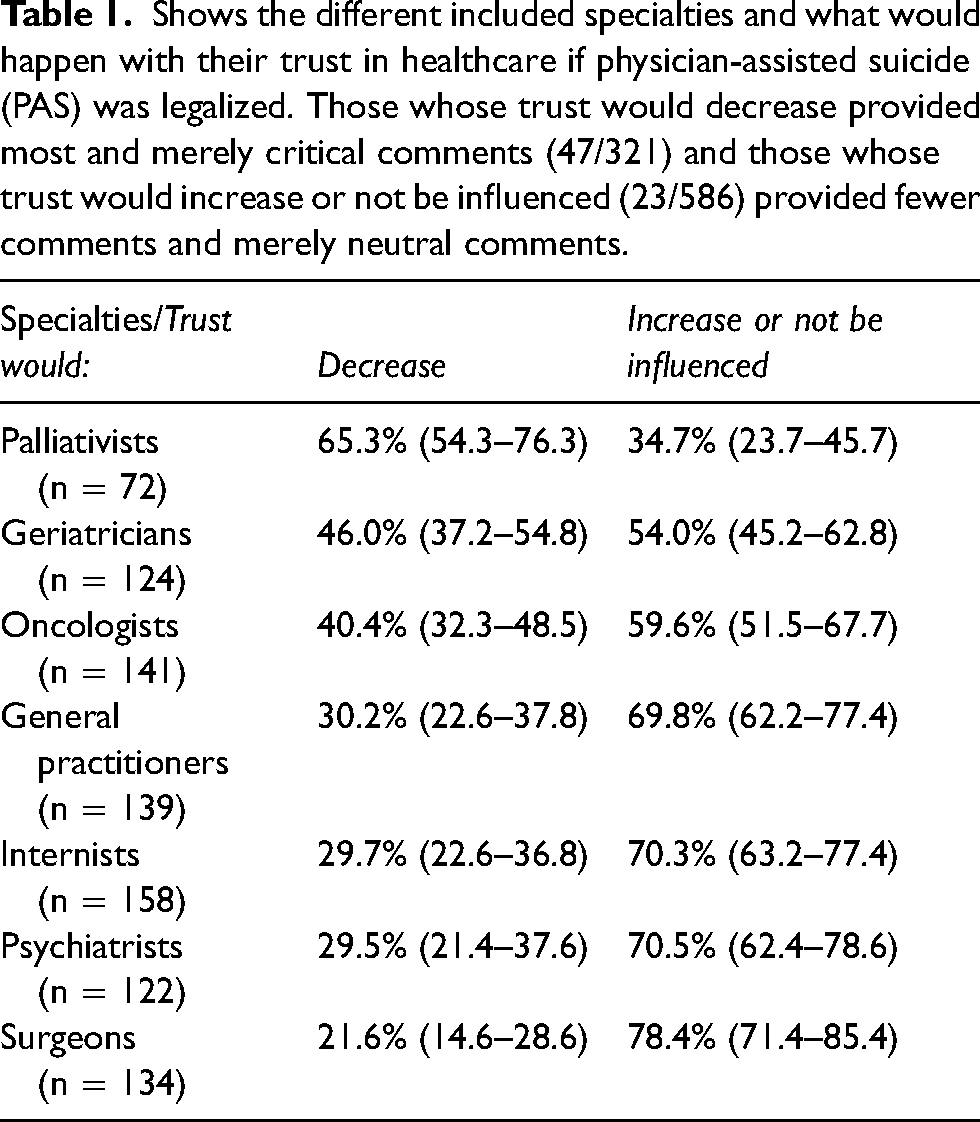
Shows the different included specialties and what would happen with their trust in healthcare if physician-assisted suicide (PAS) was legalized. Those whose trust would decrease provided most and merely critical comments (47/321) and those whose trust would increase or not be influenced (23/586) provided fewer comments and merely neutral comments.
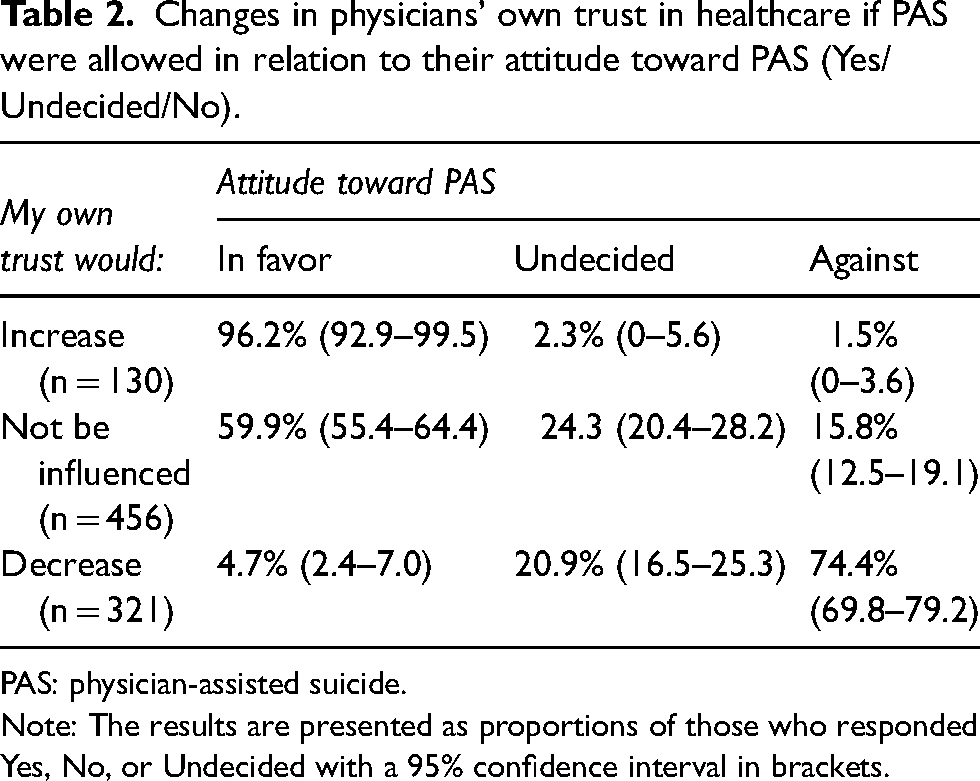
Changes in physicians’ own trust in healthcare if PAS were allowed in relation to their attitude toward PAS (Yes/Undecided/No).
PAS: physician-assisted suicide.
Note: The results are presented as proportions of those who responded Yes, No, or Undecided with a 95% confidence interval in brackets.
The participants received a postal questionnaire that included questions about their attitude toward allowing PAS, whether the participants would like to be offered such treatment themselves, and whether or not they would be prepared to prescribe the needed drug for a patient’s self-administration. Response options were Yes, No, or Undecided. Moreover, participants were asked what would happen to their own trust in healthcare if PAS were legalized and what they thought would happen with the general public’s trust in healthcare if PAS were legalized. The response options for the latter two questions were that trust would decrease, not be influenced, or would increase.
In the present paper, we have focused on what would happen with the participating physicians’ own trust in healthcare if PAS were legalized. We assume that reporting decreased trust in healthcare if PAS is allowed is another way of speaking against PAS. Correspondingly, reporting increased trust is assumed to be another way of stating support for PAS. Finally, reporting that trust would neither decrease nor increase could be regarded as stating a more neutral standpoint toward PAS. This latter group of respondents was classified as neutrals.
The idea is that reporting that a new legislation would affect one’s own trust in healthcare is to be considered a strong claim for or against PAS. If one is against PAS, but not saying that allowing PAS would affect one’s trust in health care, one’s resistance against PAS is likely less strong than if one is against PAS and saying that allowing PAS would affect one’s trust in healthcare. The same goes for being in favor of allowing PAS and (not) increasing one’s trust
With this point of departure, we examined whether the respondents’ estimations of what they believe might happen with the general public’s trust in healthcare are influenced by what they think would happen with their own trust in healthcare.
The material consisted of four fixed response options as well as space for spontaneous commentaries (n = 995). To elucidate openly stated arguments, we identified 11 pairs of contrasting arguments for and against PAS. The comments were primarily provided by the participants who were against PAS and whose own trust in healthcare would also decrease if PAS were legalized. These comments were contrasted to comments selected among those whose trust would not be influenced or who were pro PAS. The distribution of respondents from the seven different specialties regarding what would happen with their own trust in healthcare is presented in Table 1.
The quantitative results are presented as proportions with a 95% confidence interval (CI), confidence intervals that is not overlapping are assumed to be significant at 0.05 level, as if a hypothesis test had been conducted; associations are presented as relative risks (RRs) with a 95% CI. The Epi Info software program 6.04d was used for registration of data and statical calculation. 11
Ethical review
The study was approved by the Swedish Ethical Review Authority, Dnr: 2020-01842.
Results
When comparing what would happen with the physicians’ own trust in healthcare with the estimation of what would happen with the general public’s trust in healthcare if PAS were legalized, a majority [82.3% (95% CI: 77.8–86.8)] of those whose trust would decrease estimated that the general public’s trust would decrease. Of those classified as neutrals, 67.5% (95% CI: 62.8–72.2) estimated that the general public’s trust would not be influenced, and of those whose own trust would increase, 63% (95% CI: 54.3–71.7) estimated that the general public’s trust would increase.
We examined whether values influenced the participants’ attitude toward PAS and what they thought would happen with their own trust in healthcare if PAS were legalized. As shown in Table 2, there were significant differences between those who reported that their own trust would decrease or increase.
As shown in Table 2, a majority (60%) of those whose own trust would not be influenced (the neutrals) were in favor of PAS, and only 16% were against. It is also noticeable that the neutrals were the largest group [50.3% (95% CI: 47.0–53.6)] and were significantly larger compared to the group whose own trust would decrease [35.4% (95% CI: 32.3–38.5)].
If we focus on an increase and decrease of one’s own trust on the one hand and being in favor/against PAS on the other hand, which is the association measure, the RR becomes rather high [RR: 16.2 (95% CI: 9.8–26.9)] (Table 1), which was similar to the association between what would happen with one’s own trust (increase/decrease) and wishing to be offered PAS oneself [RR: 20.2 (95% CI: 11.2–35.9)].
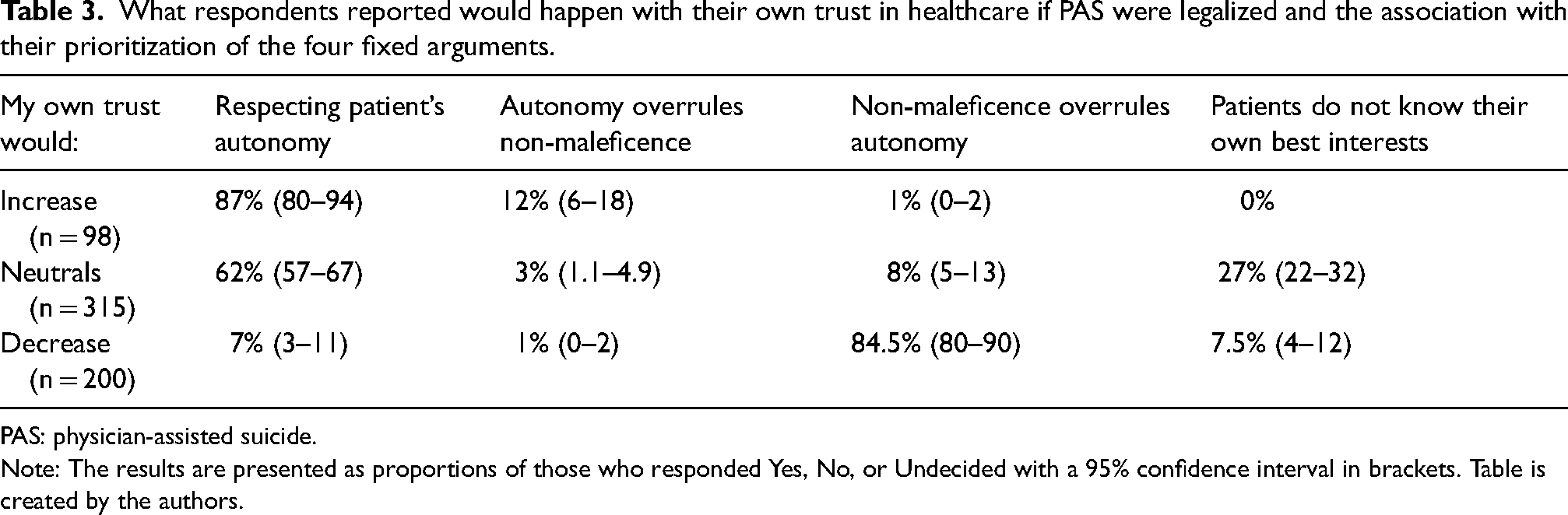
The participants were also asked to prioritize between four fixed arguments for and against PAS. Among those whose own trust in healthcare would decrease, the vast majority [84.5% (95% CI: 80–90)] stated that the most important argument was that “the non-maleficence principle should overrule the autonomy principle”. Among those whose trust would increase, a vast majority [87% (95% CI: 80–94)] stated that the most important argument was “respect for the patients’ autonomy”. Among neutrals, a majority [62% (95% CI: 57–67) prioritized the respect for the patient’s autonomy argument (Table 3).
What respondents reported would happen with their own trust in healthcare if PAS were legalized and the association with their prioritization of the four fixed arguments.
PAS: physician-assisted suicide.
Note: The results are presented as proportions of those who responded Yes, No, or Undecided with a 95% confidence interval in brackets. Table is created by the authors.
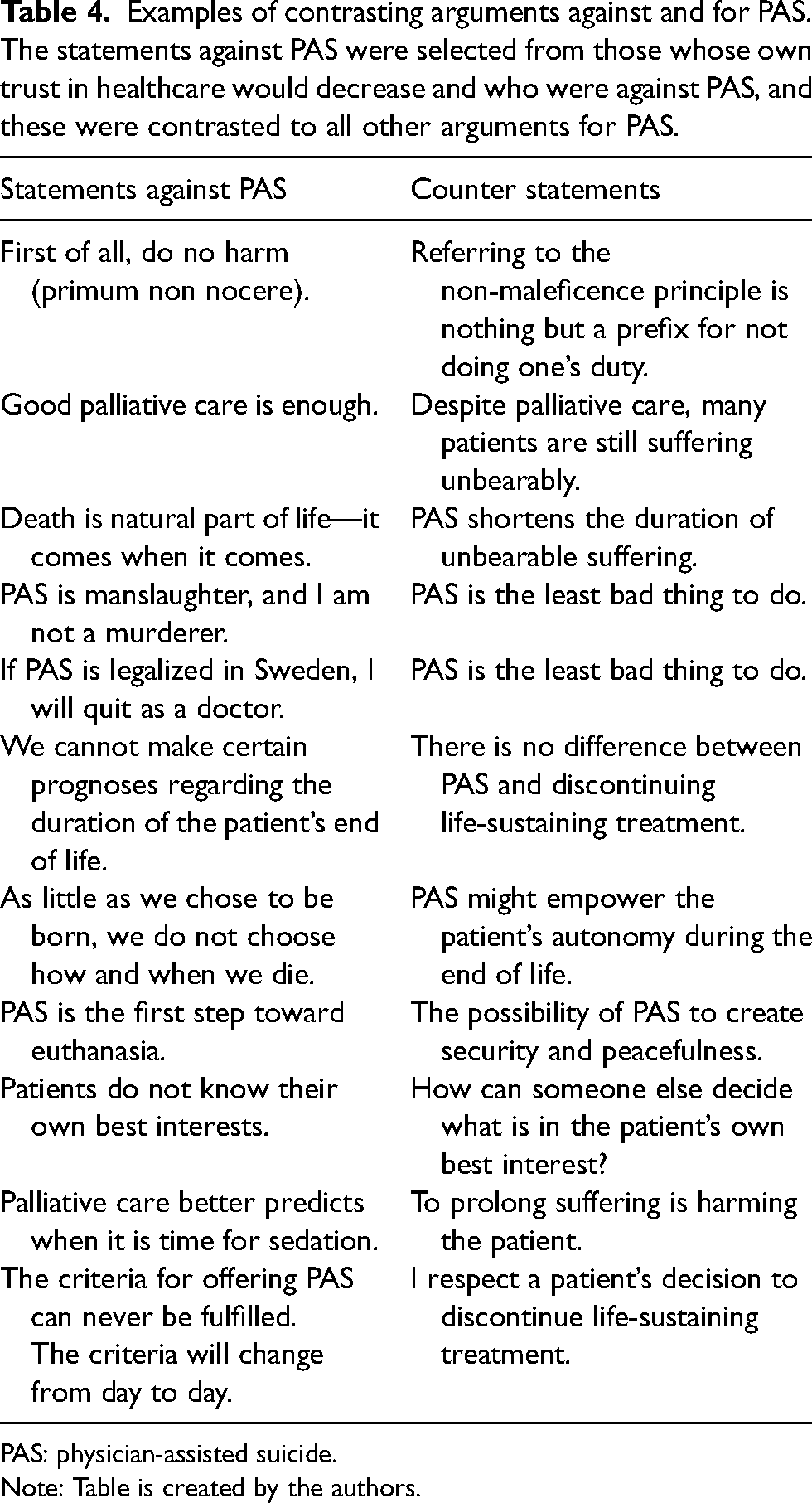
Finally, we identified and selected examples of the participants’ comments in which it was possible to contrast statements against PAS and statements supporting PAS (Table 4).
Examples of contrasting arguments against and for PAS. The statements against PAS were selected from those whose own trust in healthcare would decrease and who were against PAS, and these were contrasted to all other arguments for PAS.
PAS: physician-assisted suicide.
Note: Table is created by the authors.
Some of the respondents who were against PAS and whose own trust would decrease (n = 255) wrote many and rather long responses (n = 46), and some also stressed what they stated using all capitals, e.g. “NEVER! PHYSICIANS PROTECT LIVES – NOT FACILITATING DEATH!”
Discussion
The results indicate that what physicians reported would happen with their own trust in healthcare also influenced their estimation of what would happen with the general public’s trust in healthcare if PAS were legalized. This is in line with previous research, 10 although when asking the general population what would happen with their trust in healthcare if PAS were allowed, a large majority stated that their trust would increase or would not be influenced. 12 If that study about what would happen with the general population’s trust is correct, physicians whose own trust would increase or not be influenced are closer in their estimation to what would actually happen with the general population’s trust in healthcare.
Furthermore, the results also illustrate a strong association between reporting an
The prioritization of the fixed arguments for and against PAS also illustrate that “what would happen with one’s own trust in healthcare” functions as a divider between the pro and con arguments as well as between these two groups and the responders classified as neutral. The fact that those who reported an increase in their own trust prioritized autonomy-based arguments, and those who reported a decrease in their own trust tended to prioritize non-maleficence arguments and “the patient does not know their own best interests”, might not be surprising. More interesting is the response pattern in the neutral group. Here, a majority (65%) prioritized autonomy-based arguments, but the minority who did not support a paternalistic argument, namely that the patient does not understand their own best interests (27%). If a patient is considered not competent to make decisions, someone else (e.g. the physician) has to make decisions for what is supposed to be in the patient’s best interests, and this is allegedly a form of defensible soft paternalism. 13 It is notable that the neutrals prioritized this argument more often than the disguised paternalistic argument “the non-maleficence principle should overrule the autonomy principle”. 13 Perhaps, the latter argument appears less defensible compared to the former, which could be supported by a free-text comment for PAS stating that the non-maleficence principle could be understood as a “pretext for not fulfilling the duties of a physician”.
The results of the present study may be strengthened by a Swiss study concerning the evaluation of patients who prefer PAS to palliative care, where it was obvious that physicians were more inclined to claim that such patients were not competent.14–16
The reason why several participants declared that they would quit their job as physicians if PAS were legalized might be due to the fact that most respondents were aware that there is no room for conscientious objection in a Swedish context.
The group whose trust would not be influenced
It is perhaps not surprising that there was a strong association between being in favor of PAS or against PAS on the one hand and that one’s own trust in healthcare would increase or decrease on the other hand. But what is new in the present context is that those whose own trust would neither increase nor decrease (the neutrals) were the largest group [50.3% (95% CI: 47.0–53.6)], which might be compared with a similar study conducted in 2007 in which the proportion of neutrals was 35.8% (95% CI: 32.0–39.6). 10 If the proportion of neutrals continues increasing in the future, this might indicate that the issue of PAS is becoming less emotionally laden and the arguments less value impregnated.
What does “not harming” mean in a PAS context?
Many of the provided comments against PAS were merely factual claims, likely sometimes influenced by the physicians’ own personal values. An example of such a claim is that very few patients need PAS due to palliative measures being sufficient. But the (allegedly) low number of patients in need of PAS is a questionable argument for not offering PAS. In a situation of treatment-refractory unbearable suffering, one might argue that there is a medical indication to offer PAS regardless of how often or in how many patients such situations may occur. 4
Concerns about a patient’s competency and decision-making capacity are also factual aspects that might be influenced by the physician’s own values. Such values can be actualized when patients want to discontinue life-sustaining treatment such as dialysis or ventilator treatment. One might ask why it is important to worry about evaluating, for example, competency or underlying depression in a PAS context, but less so when it comes to the discontinuation of a life-sustaining treatment. 5 There might be legal aspects to consider because disrespecting a competent patient’s right to discontinue a life-sustaining treatment would imply coercive somatic treatment, which is not legal in a Swedish context. However, it seems obvious that a majority of those who reported being against PAS in the present study prioritized the argument that the non-maleficence principle should overrule the autonomy principle, which actualizes the issue about what constitutes harm. Does shortening life on the request of a terminally ill patient to shorten the patient’s suffering imply that such a patient is harmed? The answer hinges on the relative harm of shortening life versus experienced suffering and is by no means self-evident. 17 As one of the respondents claimed, PAS might just as well be considered the least bad thing to do in such a situation.
Among the participants who were both against PAS and whose own trust would decrease (n = 255), several were concerned that the criteria would never be fulfilled and that external influence on the patient’s decision could never be avoided. Also, here the counterargument was the question—what is the difference between a patient’s wish to discontinue a life-sustaining treatment and PAS? If there is no relevant difference in the two situations regarding others’ impact or estimation of the patient’s competency, we ought to respect such a patient’s wish as well as a patient who prefers PAS to good palliative care. But we might also consider whether prolonging a patient’s suffering is equivalent to harming a patient. This statement was identified as a counterargument against the statement that palliativists are better at predicting when it is time for palliative sedation.
Strengths and limitations
Because conscientious objection is a non-option in Sweden, personal values might be disguised or filtered by self-censorship, at least with inference to the best explanation. In the present study, we have presented a method to elucidate otherwise hidden values by asking what would happen with the physicians’ own trust in healthcare if PAS were legalized. The method has been validated in different contexts and appears reproducible and reliable. 3
Even though the sample of physicians was randomly selected, except for palliativists where the whole sample was included (n = 123), other specialties could also have been included such as neurology, neurosurgery, pulmonology, and rehabilitation, i.e. specialties managing different neurodegenerative diseases and chronic respiratory diseases. However, in order to compare the present study with a similar study from 2007, we only added palliativists, which became a clinical specialty of its own in 2015 and hence was not included in the 2007 study. 8
Conclusion
We found a strong association between reporting a decrease in one’s own trust in healthcare if PAS were to be legalized and being against PAS on the one hand and reporting an increase in one’s own trust in healthcare and being in favor of PAS on the other hand.
Those reporting an attitude against PAS often provided factual claims supporting their attitude; however, these factual claims seem value-impregnated to some extent.
The present study suggests that the group of neutrals has increased significantly compared to a study conducted in 2007. If this trend continues, the discussion of PAS might become less emotional and the arguments against PAS less value impregnated.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The study was approved by the Swedish Ethical Review Authority, Dnr: 2020-01842.