
Abstract
Objectives
During the COVID-19 pandemic, healthcare resources including staff were diverted from paediatric services to support COVID-positive adult patients. Hospital visiting restrictions and reductions in face-to-face paediatric care were also enforced. We investigated the impact of service changes during the first wave of the pandemic on children and young people (CYP), to inform recommendations for maintaining their care during future pandemics.
Design
A multi-centre service evaluation was performed through a survey of consultant paediatricians working within the North Thames Paediatric Network, a group of paediatric services in London. We investigated six areas: redeployment, visiting restrictions, patient safety, vulnerable children, virtual care and ethical issues.
Results
Survey responses were received from 47 paediatricians across six National Health Service Trusts. Children's right to health was largely believed to be compromised by the prioritisation of adults during the pandemic (81%; n = 33). Sub-optimal paediatric care due to redeployment (61%; n = 28) and the impact of visiting restrictions on CYP's mental health (79%; n = 37) were reported. Decreased hospital attendances of CYP were associated with parental fear of COVID-19 infection-risks (96%; n = 45) and government ‘stay at home’ advice (89%; n = 42). Reductions in face-to-face care were noted to have disadvantaged those with complex needs, disabilities and safeguarding concerns.
Conclusion
Consultant paediatricians perceived that paediatric care was compromised during the first wave of the pandemic, resulting in harm to children. This harm must be minimised in subsequent pandemics. Recommendations for future practice which were developed from our findings are provided, including maintaining face-to-face care for vulnerable children.
Introduction
The Coronavirus disease 2019 (COVID-19) pandemic has presented a higher disease burden in adults, with children commonly experiencing milder symptoms.1,2 Consequently, paediatric services in the UK were reconfigured, diverting resources to adult care. During the ‘first wave’ between January to July 2020, 3 one-fifth of junior-level paediatric staff were transferred to adult services. 4 Reduced paediatric staffing posed risks to standards of hospital and community care.
In order to increase hospital capacity for COVID-positive adults, some children's emergency departments and inpatient wards were closed. 5 Certain paediatric intensive care units (PICUs) were remodelled to support adult patients, with paediatric inpatients transferred to tertiary children's hospitals.6,7 Diverting children to alternative sites may have harmfully delayed treatment.
Infection-control measures further threatened families’ wellbeing. In one study, 41% of parents in neonatal intensive care units felt unable to bond with their child due to visiting restrictions. 8 Reductions in face-to-face care posed risks that vulnerable children were undetected and unsupported, with 50% fewer safeguarding referrals recorded during the first wave. 9
Moreover, one study reported 93% of UK paediatric services experiencing decreased urgent care and emergency department activity following the first national ‘lockdown’. 4 Reduced medical need within children, including fewer sports-related injuries, 10 may have contributed. However, parental hesitancy to visit hospitals due to fears of COVID-19 infection, 11 and government ‘stay at home’ messages posed potential barriers for children in accessing care.
Under the United Nations Convention on the Rights of the Child, children have the right to good health. 12 This right was potentially challenged by the prioritisation of adult healthcare during the pandemic. We aimed to investigate paediatricians’ perceptions of the impact of healthcare service changes during the pandemic's first wave on children and young people (CYP). Our results informed recommendations for maintaining children's care in future pandemics.
Methods
Study design and participants
We performed a multi-centre service evaluation of 17 paediatric care providers within the North Thames Paediatric Network (NTPN). 13 Consultant paediatricians (CPs) were recruited through purposive sampling, due to their overview of multidisciplinary teams and patient experiences within paediatric services. An introductory statement within the open survey informed participants of its anonymous, voluntary and confidential nature. Completion of the survey was taken as consent to participate.
Survey structure
A 16-part survey was designed from relevant literature, and through consultation with the study team which included three members of the Great Ormond Street Hospital Paediatric Bioethics Centre, a consultant paediatrician and a medical student (supplemental material 1). Certain questions explored specific changes within North London hospitals and North Thames community services. Multiple-choice questions were included, with free-text boxes for participants to share additional comments or case examples. Responses to all questions were voluntary. Consideration was given to whether the order of questions would lead to bias. The survey was pre-piloted by four CPs.
Data collection
After liaison with the NTPN Co-ordinator, the paediatric clinical directors were sent an invitation email containing a REDCap (Version 10.6.3) online survey link. The directors were asked to: complete the survey, forward the invitation to all hospital and community CPs within their services, and notify the study team of circulation numbers. Responses were collected from 20th January 2021 to 9th April 2021, with three email reminders shared to the directors. A sample size calculation was not performed, as we aimed to distribute the survey to all CPs within 17 NTPN services.
Study data were collected using REDCap electronic data capture tools hosted at UCL.14,15 REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies, providing: (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for importing data from external source.14,15
Data analysis
Only complete survey responses were analysed. Survey data were exported from REDCap into SPSS (IBM SPSS Statistics for Macintosh, Version 27.0). SPSS was used for descriptive statistics. Quantitative data from multiple-choice questions were summarised with valid percentages, excluding missing responses as some questions were not relevant to all participants.
Qualitative data from free-text responses were summarised through ‘manifest’ content analysis. 16 Inductive coding was used to develop new concepts from responses. 17 Codes were grouped into overarching categories. Codes and categories were cross-checked by two team members.
Ethics approval
This project was registered under the Great Ormond Street Hospital Clinical Audit and Service Evaluation Team (Registration number: 2933). Ethical approval was not required as this service evaluation involved staff only. 18 Participants’ identities were protected by the survey's anonymity.
Results
The survey was circulated to 181 consultant paediatricians (CPs) within six National Health Service (NHS) Trusts; Barts Health NHS Trust: n = 68 CPs, Homerton University Hospital NHS Foundation Trust: n = 13, North Middlesex University Hospital NHS Trust: n = 22, Royal Free London NHS Foundation Trust: n = 20, University College London Hospitals NHS Foundation Trust: n = 37, Whittington Health NHS Trust: n = 21. Forty-seven complete responses were received, presenting a response rate of 26.0%. We present our findings on six areas: redeployment, visiting restrictions, patient safety, vulnerable children, virtual care and ethical issues.
Redeployment
During the pandemic's first wave, 89% (n = 42) of participants witnessed staff redeployment within their department. Seventy-percent (n = 33) felt that staffing remained appropriate for caseloads within their service and 30% (n = 14) reported sufficient quality of care. Nevertheless, 61% (n = 28) conveyed that decreased staffing had generally impacted standards of paediatric care and 48% (n = 13) noted lower quality care within North Thames community paediatric services. Participants described poorer support for cancer patients due to social worker redeployment and children feeling ‘short-changed’.
Visiting restrictions
Although 75% (n = 35) felt that hospital visiting restrictions were necessary, consequences were highlighted for the mental health of children (79%; n = 37) and their caregivers (89%; n = 41). Restrictions were regarded as, ‘… terrible for YP [Young People] and their families’; notably ‘Particularly tragic during end of life care and at diagnosis of cancer relapse’ and ‘Very difficult for children with disabilities’. The exclusion of fathers who were unable to visit neonatal units alongside mothers was raised in one comment. Although 50% (n = 23) relayed that effective virtual-visiting facilities were available, one-third (n = 15) disagreed. Comments mentioned variable hospital provision of technology, alongside poorer accessibility for Non-English-speaking families and those with reduced technological access.
Patient safety
Whilst 40% (n = 19) felt that the reduction in children attending hospitals was due to decreased medical need, including, ‘…reduced common viral illness transmissions’ during school closures, 60% (n = 28) opposed this. Caregivers’ fear of COVID-19 infection-risks in hospitals (96%; n = 45), government ‘stay at home’ advice (89%; n = 42) and 111 advice (85%; n = 40) were regarded as causes. Adequate virtual care provision was generally not believed to contribute to decreased hospital presentations (87%; n = 41).
Over 80% reported that ‘near misses’ (delayed hospital presentations posing risks of serious harm) in children were related to factors including fear of COVID-19 infection-risks in hospitals and reduced community care availability (Figure 1).
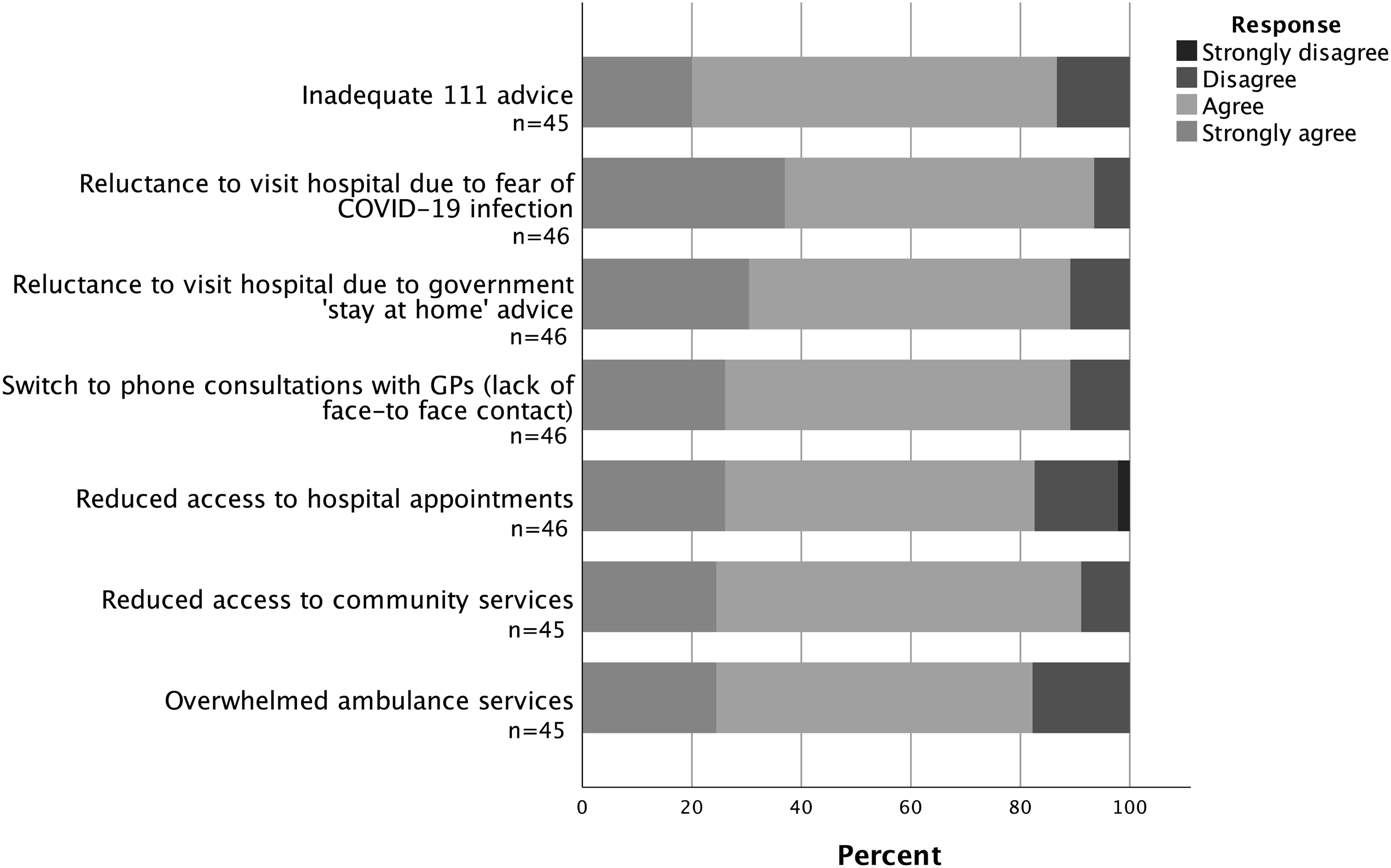
Participants’ opinions on causes behind ‘near misses’ (delayed hospital presentations posing risks of serious harm) during the pandemic.
Within reconfigured North London paediatric services, hospital-organised transportation of children requiring acute care from a district general hospital to a tertiary centre was noted to harmfully delay treatment by 43% of respondents (n = 12). Eighteen respondents (67%) felt that families were poorly informed of Paediatric Emergency Department (PED) closures. Fifteen respondents (68%) conveyed risks of harm to children due to delayed triage for families who were diverted from closed PEDs to alternate sites and were required to self-organise transport. Threats to patient safety included ‘inadequate risk assessments’ before diverting patients and ‘rapid deterioration’ during travel. Reported case examples highlighting potential harm to children during transport between North London sites are provided in Table 1.
Case examples shared by participants highlighting the risk of harm to children during hospital-organised transport or self-organised transport by families between North London sites during the pandemic.
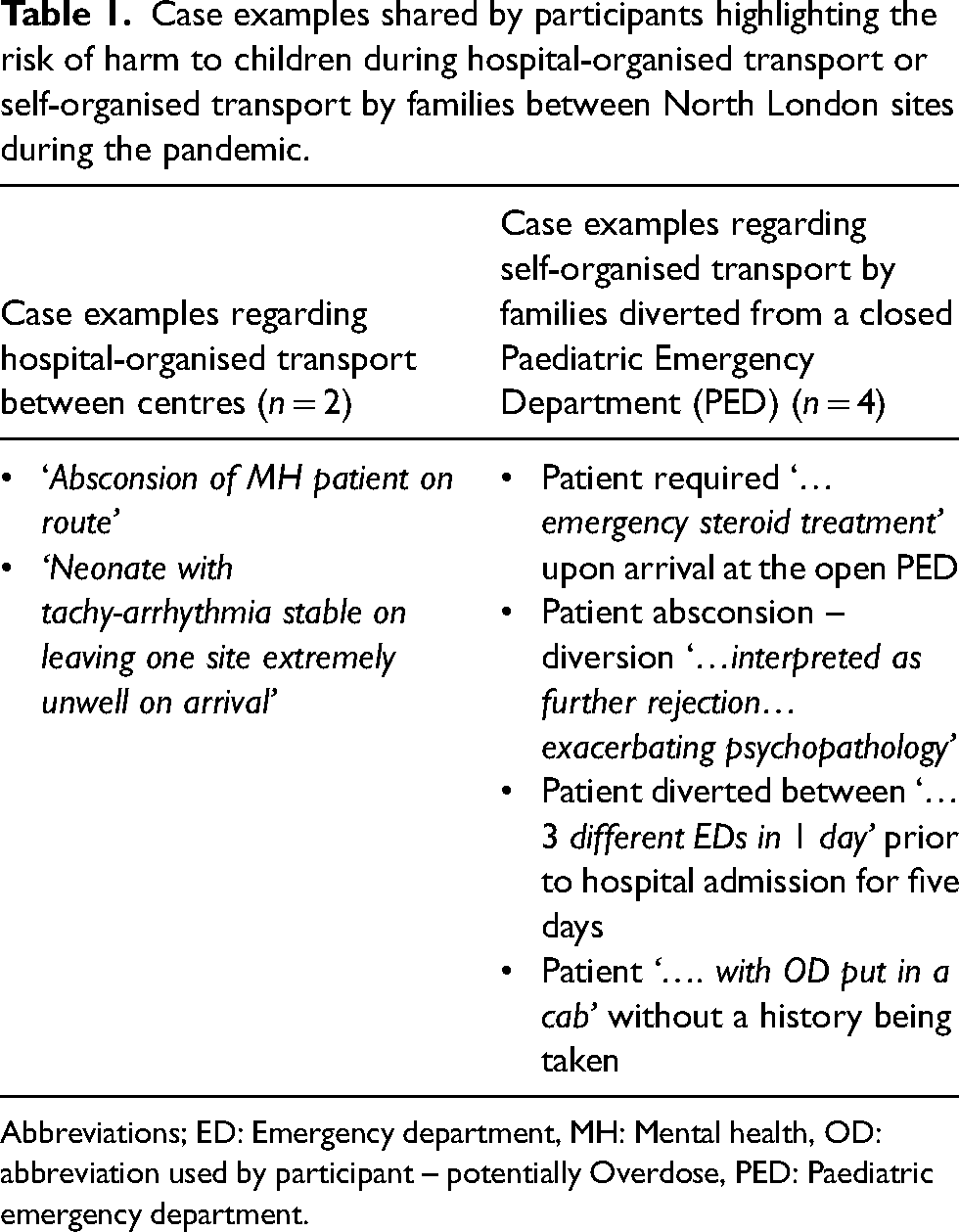
Abbreviations; ED: Emergency department, MH: Mental health, OD: abbreviation used by participant – potentially Overdose, PED: Paediatric emergency department.
Vulnerable children
Over 90% of respondents perceived that school closures, social isolation and reduced home-visiting by health and social care professionals had contributed to the decrease in child safeguarding referrals during the pandemic (Figure 2). Comments emphasised inadequacies in face-to-face community healthcare provision, including poorer health visitor availability and, ‘Lacks of PPE [personal protective equipment] for community-based staff to do home visits safely’.
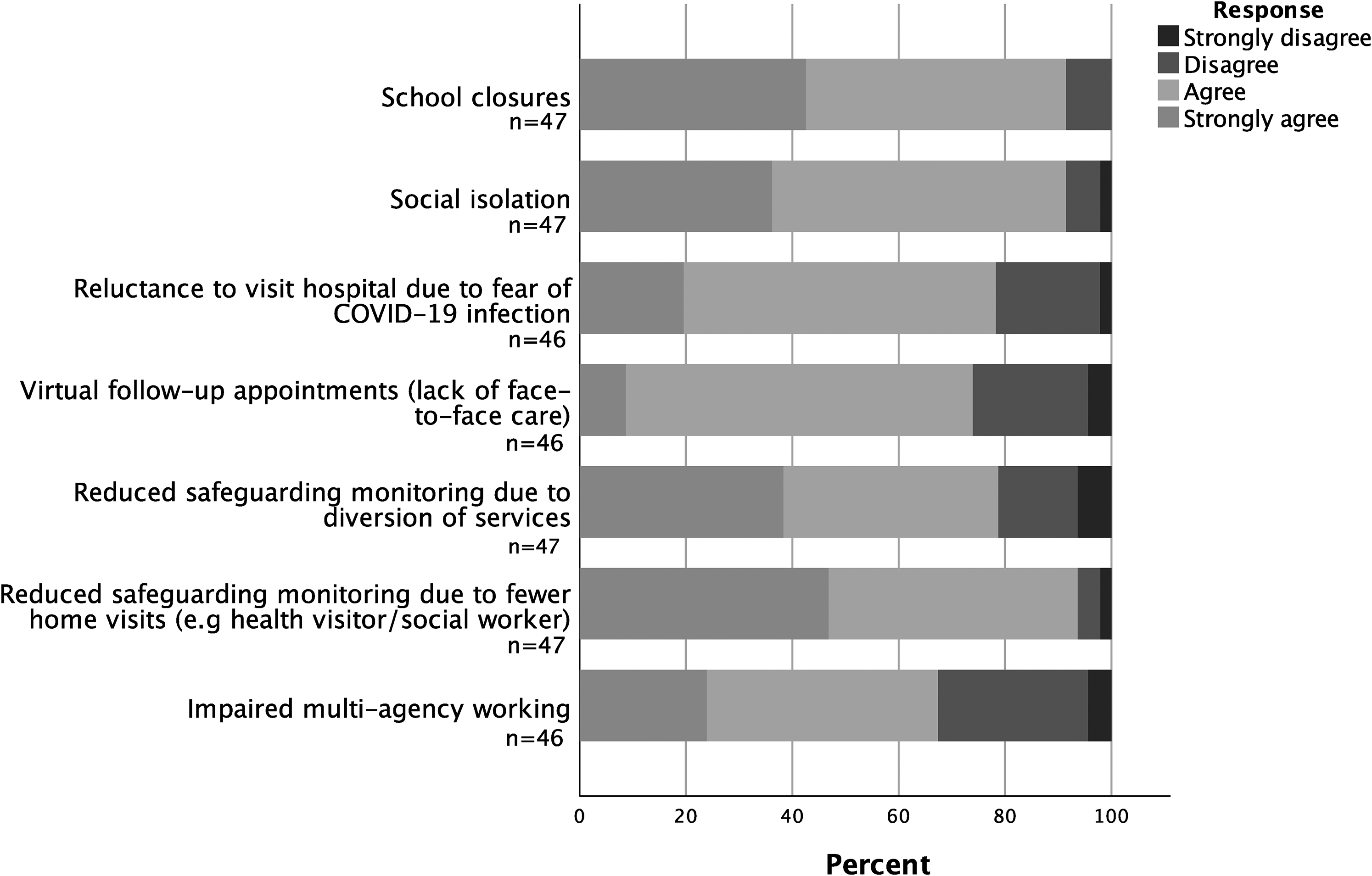
Participants’ opinions on causes behind the decrease in child safeguarding referrals recorded during the pandemic.
Participants reported that children with complex needs and disabilities were unable to access essential therapies from local services (84%; n = 37) and schools (91%; n = 39). Necessary face-to-face reviews were believed not to have occurred with this cohort by 68% (n = 29). Increased risks of harm to these patients due to poorer care accessibility was reported (79%; n = 34). Comments stated that, ‘Children with complex needs have suffered the most’ and had found it, ‘Very difficult to access all services’.
Virtual care
Sixty-five percent of participants (n = 30) perceived that virtual appointments offered lower quality of care compared to face-to-face care. Poorer assessments of children's physical health (76%; n = 34) and mental health (78%; n = 36) were reported, alongside impaired recognition of child safeguarding concerns (89%; n = 41). Difficulties in patient communication (85%; n = 39) and maintaining confidentiality (87%; n = 40) were raised. Although 52% (n = 24) felt that care accessibility had improved with virtual formats, inequities for those with reduced technological access or skills (83%; n = 38) and unsuitability of virtual consultations for new patients were raised (Table 2).
Advantages and disadvantages of virtual appointments for children, young people and families, as reported by participants (n = 10).
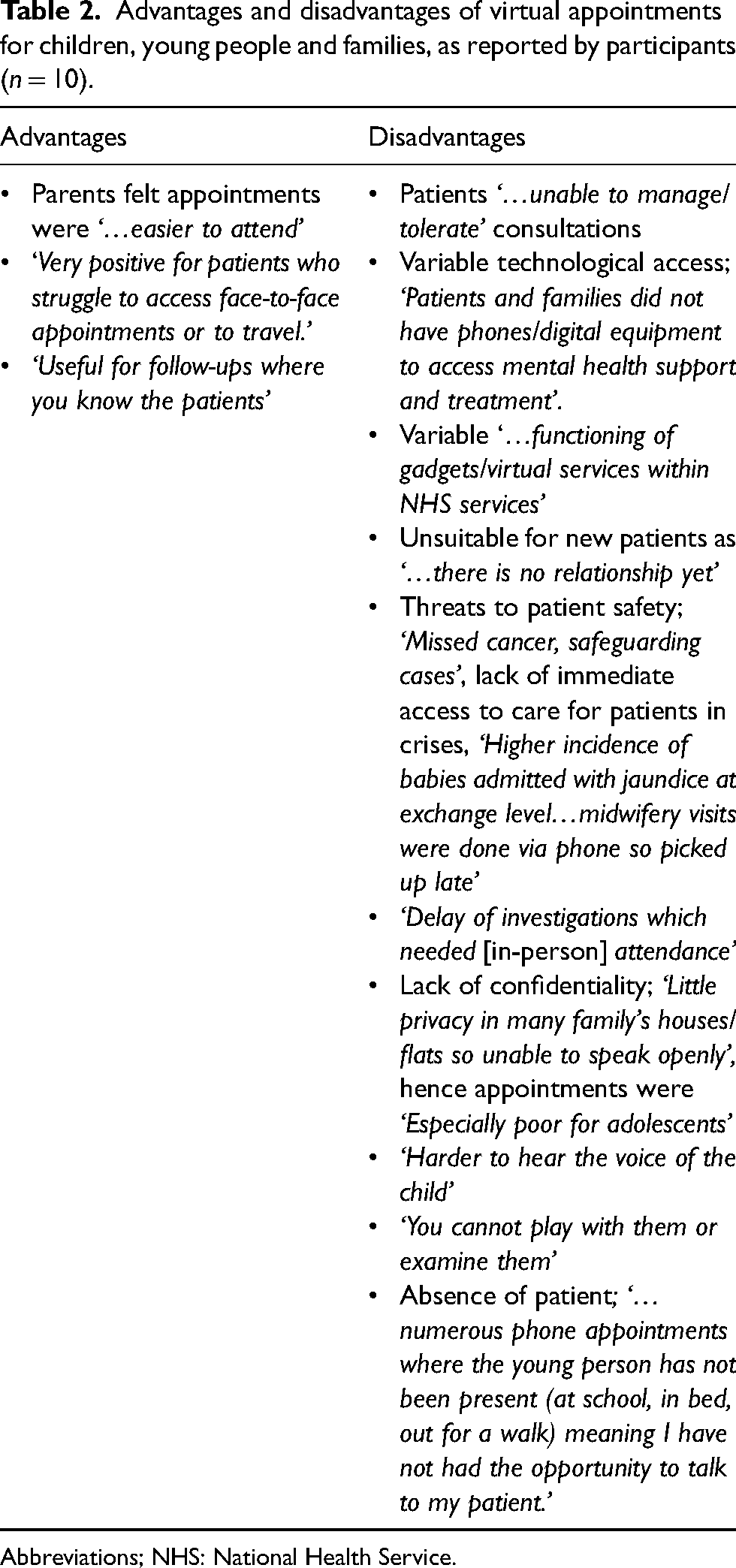
Abbreviations; NHS: National Health Service.
Ethical issues
Respondents voiced that children's fundamental right to health was unprotected during the pandemic (88%; n = 41), challenged by prioritising the general population's right to health (81%; n = 33; Figure 3). Whilst 44% (n = 20) felt that this prioritisation was justified, 46% (n = 21) opposed this. One comment stated, ‘We can all understand the utilitarian argument’, whilst others relayed that, ‘CYP [were] sacrificed for adults unjustly’, with the years of life remaining for infants in comparison to adults not, ‘… taken into calculations’. Long-term consequences were raised, including that, ‘The impact of this on our CYP will be felt for many years to come in terms of health, wellbeing and education/career’.
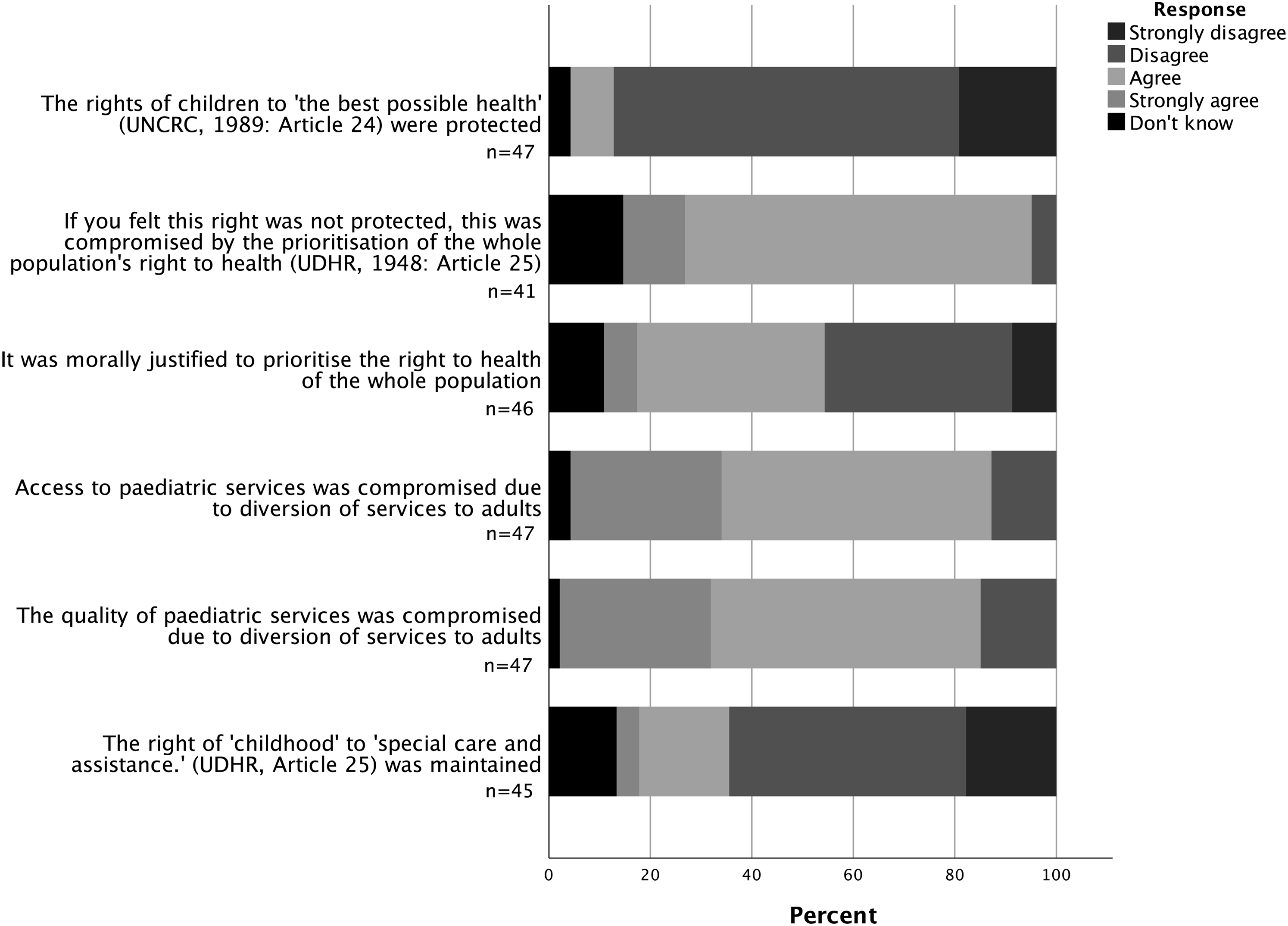
Participants’ opinions on ethical issues during the pandemic, including the protection of children's rights. Universal Declaration of Human Rights (UDHR) United Nations (1948). United Nations Convention on the Rights of the Child (UNCRC). United Nations (1989).
Almost half (47.8%; n = 22) of participants experienced ethical challenges due to service changes, including difficulty in maintaining, ‘… expert and consistent care’ for eating disorder inpatients transferred between sites. Participants conveyed difficulties in providing holistic care (84%; n = 38) and in fulfilling their duty of care to children 64% (n = 29). Participants’ comments on ethical concerns are summarised in supplemental material 2.
Discussion
During the COVID-19 pandemic, paediatric services adapted to reduce face-to-face contact with children and families, and divert resources to adult services. Our service evaluation presents concern amongst consultant paediatricians (CPs) regarding compromised paediatric care during service changes, with resulting harm to children.
Lower standards of care due to staff redeployment were relayed by 61%, with almost half of respondents noting poorer quality of community care. Nevertheless, 30% felt that paediatric care standards were maintained and some comments revealed reduced caseloads during the lockdown, reflecting variation between services.
Despite general agreement that visiting restrictions were necessary, the impact on children's and caregivers’ mental wellbeing was emphasised. This echoes the experiences of 41% of parents in one study of neonatal intensive care units who felt unable to bond with their new-born due to visiting regulations, 8 and the distress experienced by the family of a COVID-positive 13-year-old who died alone in hospital. 19 Restrictions for vulnerable patients including those under palliative care, and the exclusion of fathers from visiting neonatal units, were raised as concerns.
Although decreased medical need, including reduced non-COVID-19 viral illness transmission, was noted to contribute to fewer hospital presentations of children, 60% of CPs disagreed that this was a key cause. Fears of contracting COVID-19 within hospitals, alongside government or 111 ‘stay at home’ advice, were strongly believed to have hindered parents from accessing care for their children. These findings echo previous studies which revealed reluctance within some caregivers to visit hospitals during the pandemic.11,20 This hesitancy, alongside decreased availability of community and face-to-face primary care, was believed to result in delayed hospital presentations of children. Our results highlight concern amongst paediatricians that barriers to accessing care contributed to the documented delayed presentations of children during the first wave,4,21,22 and consequently threatened patient safety. Moreover, concerns were raised around harm to children during hospital transfers and self-organised transport by families to limited sites providing paediatric care.
Concerningly, the decrease in child safeguarding referrals 9 was largely attributed to impaired safeguarding monitoring due to reductions in face-to-face contact with children. This included: fewer hospital attendances, the transition to virtual appointments, and reduced home-visiting by health and social workers. The impact of school closures was emphasised, reiterating the proportion (18%) of safeguarding referrals that arise within schools. 23 Furthermore, participants relayed that children with complex needs and disabilities were unable to access essential therapies, threatening this patient group's wellbeing. This echoes the experiences of 61% of these patients in one study who had become less physically active during the first national ‘lockdown’, with 65% of parents reporting poorer mental health in their child due to restricted access to services. 24
Inadequate mental and physical health assessments, poorer patient communication and difficulties in maintaining confidentiality within virtual consultations with children were highlighted. This contradicts the views of 99% of parents in another study that doctor-patient relationships and privacy were maintained within virtual appointments. 25 Our findings also present a more negative view than portrayed in a survey of children, in which only 27% felt less satisfied with virtual consultations in comparison to face-to-face reviews. 20 This discordance between stakeholders’ perceptions highlights the need to further investigate experiences of virtual care.
Our findings present paediatricians’ concern that children's right to health was compromised by the prioritisation of adults and the general population's right to health during the pandemic. Despite divided opinion on whether this prioritisation was justified, paediatricians conveyed difficulty in fulfilling their duty of care to children, and possible long-term impacts on children's wellbeing were raised.
Although children are not primarily affected by COVID-19, our results and alternative studies highlight harm occurring to children during the first wave. Impacts on children during a pandemic must be fully considered when reconfiguring services. Based on our findings, we propose recommendations for maintaining children's care during future pandemics (Box 1). This includes: involving staff in service planning, maintaining face-to-face reviews for vulnerable children, and reassuring families of infection-control measures within hospitals.
Recommendations for maintaining the care of Children and Young People (CYP) in future pandemics
Prioritising children
Keep children's welfare a priority.
Prioritise the provision of safe care to children within service changes.
Supporting staff
Include clinical staff in service planning, incorporating their feedback.
Support ethical considerations in challenging situations for clinicians, with access to ethical guidance within trusts and the community (e.g. regarding visiting restrictions for children who are seriously ill).
Service changes
Perform risk assessments of staffing levels and of CYP being diverted to alternate services.
Provide paediatric inpatient beds to minimise patient transfers to alternative hospitals.
Ensure an individualised approach to the enforcement of visiting restrictions in cases including palliative care, complex needs and intensive care, considering psychological impacts of restrictions on families and parents’ rights to receive ‘respect for their family life’ (Article 8; European Convention on Human Rights). 27
Maintain core community paediatric and allied health professional services to; support hospital discharge, perform timely child development assessments, adequately monitor child protection cases.
Vulnerable children and young people
Maintain face-to-face reviews for vulnerable children (e.g. safeguarding cases, children experiencing mental health difficulties), with increased face-to-face General Practitioner (GP) appointments and adequate Personal Protective Equipment to allow home-visits by healthcare and social workers.
Maintain access to essential therapies for CYP with complex needs and disabilities during general service restrictions, as the National Health Service is required to provide ‘reasonable adjustments’ for this patient group (Equality Act). 28
Virtual care
Identify CYP and families who benefit from virtual care and can readily access this.
Ensure that disadvantaged CYP (e.g. those with reduced technological access) continue to receive an appropriate service.
Offer face-to-face reviews when patient assessment or engagement is suboptimal through virtual formats.
Provide adequate training, for instance through phone calls, to improve families’ confidence and skill in using virtual care and virtual-visiting measures.
Ensure hospitals are supplied with the resources to provide appropriate technology for virtual communication with families.
Service integration
Create a single ‘safeguarding hub’ within North London or the North Thames Paediatric Network, which oversees collaboration between education, health and social care in safeguarding monitoring.
Ensure collaboration of healthcare services with educational and childcare facilities in order to maintain children's welfare.
Reducing healthcare inequities
Identify patients who struggle to access services and provide targeted support, for example; ensure translators can be accessed for virtual or face-to-face appointments, ensure timely and accessible transport for families during service relocations.
Service communications
GP practices, schools and childcare facilities should provide: regular updates for families on healthcare service changes, reassurance regarding infection-control measures in place within hospitals, and information on criteria for presentation to hospital.
Key information could be provided through; texts, emails, social media, direct consultation (including phone calls), posters, news networks.
Nationally, a consistent message is required by the government and all services including 111 services, emphasising when families should seek face-to-face care.
Limitations
Although we achieved a response rate of 26%, a higher rate could minimise non-response bias. Due to restrictions on applying for ethical and regulatory approval from the Health Research Authority, and local research and development departments during the pandemic, we could not include children and their families in this work. Their inclusion in future research, alongside other stakeholders such as: service managers, nurses, therapists and health visitors, would enable further exploration of the experiences of children and staff.
Strengths
A strength of our study is the collection of survey responses from paediatricians within multiple hospitals and community services. The survey's anonymity and modification of leading questions during pilot-testing aimed to ensure that participants felt able to fully share their views.
Conclusion
There is a duty to act ‘…if patient safety, dignity or comfort is compromised’. 26 Consultant paediatricians perceived that paediatric care was compromised during the first wave of the COVID-19 pandemic, resulting in harm to children. Our findings highlight the need to prioritise the welfare of our children and young people during the recovery from this pandemic and in future pandemics. Whilst a utilitarian approach may be considered appropriate, children's right to health 12 must be maintained.
Supplemental Material
sj-pdf-1-cet-10.1177_14777509211063590 - Supplemental material for North Thames multi-centre service evaluation: Ethical considerations during COVID-19
Supplemental material, sj-pdf-1-cet-10.1177_14777509211063590 for North Thames multi-centre service evaluation: Ethical considerations during COVID-19 by Namithaa Sunil Kumar, Pippa Sipanoun, Mariana Dittborn, Mary Doyle and Sarah Aylett in Clinical Ethics
Supplemental Material
sj-pdf-2-cet-10.1177_14777509211063590 - Supplemental material for North Thames multi-centre service evaluation: Ethical considerations during COVID-19
Supplemental material, sj-pdf-2-cet-10.1177_14777509211063590 for North Thames multi-centre service evaluation: Ethical considerations during COVID-19 by Namithaa Sunil Kumar, Pippa Sipanoun, Mariana Dittborn, Mary Doyle and Sarah Aylett in Clinical Ethics
Footnotes
Acknowledgements
The authors would like to thank all of the participants, who generously gave up their time to share their views and experiences. The authors would like to thank the North Thames Paediatric Network Co-ordinator, Dr Kate Plunkett-Reed, for her support in distributing the survey within the network. This service evaluation was supported by The GOSH Paediatric Bioethics Centre and by University College London. Our work has previously been presented as a poster at the Institute of Medical Ethics Student Conference 2021 and the GOSH Conference 2021 ‘Above and Beyond'.
Author contributions
NSK and PS led survey development, with contribution from all authors. SA led submission of service evaluation registration with contributions from all authors. NSK led the writing of the manuscript with contribution from all authors. All authors revised and approved the final draft.
Data availability
An example of data can be made available upon request to the authors.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The four co-authors work within certain services included in the North Thames Paediatric Network - the target population of our service evaluation. However, the anonymity of the survey participants was of great importance, with the survey being designed with this in mind.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.