
Abstract
Given the nature of the discipline, it might be assumed that clinical psychology is an ethical profession, within which effective ethical decision-making is integral. How then, does this ethical decision-making occur? This paper describes a systematic review of empirical research addressing this question. The paucity of evidence related to this question meant that the scope was broadened to include other professions who deliver talking therapies. This review could support reflective practice about what may be taken into account when making ethical decisions and highlight areas for future research. Using academic search databases, original research articles were identified from peer-reviewed journals. Articles using qualitative (n = 3), quantitative (n = 8) and mixed methods (n = 2) were included. Two theoretical models of aspects of ethical decision-making were identified. Areas of agreement and debate are described in relation to factors linked to the professional, which impacted ethical decision-making. Factors relating to ethical dilemmas, which impacted ethical decision-making, are discussed. Articles were appraised by two independent raters, using quality assessment criteria, which suggested areas of methodological strengths and weaknesses. Comparison and synthesis of results revealed that the research did not generally pertain to current clinical practice of talking therapies or the particular socio-political context of the UK healthcare system. There was limited research into ethical decision-making amongst specific professions, including clinical psychology. Generalisability was limited due to methodological issues, indicating avenues for future research.
Introduction
Clinical psychologists aim to reduce distress and improve well-being for people across the lifespan with a range of psychosocial difficulties, by drawing on different assessment, formulation and intervention methods, as outlined by the British Psychological Society (BPS). 1 This may involve working directly, indirectly or through consultation, with individuals, families, groups or professionals. In the UK, the majority of clinical psychologists work for the National Health Service (NHS), though many are employed in other statutory services or private organisations, 1 and others may work in the not-for-profit sector. The title ‘Clinical Psychologist’ is protected in the UK, requiring registration with the Health and Care Professions Council (HCPC), who regulate a number of ‘Practitioner Psychologists’ (including but not limited to Forensic Psychologists, Health Psychologists and Counselling Psychologists). Practitioner Psychologists must complete an accredited Doctoral degree and ongoing Continuing Professional Development (CPD) to maintain registration. 1
Given the high degree of sensitive personal information shared by users of clinical psychology services, it is therefore essential that clinicians are able to practice ethically. Clinical psychologists in the UK are required to work within the HCPC Standards of Conduct, Performance and Ethics 2 and Standards of Proficiency for Practitioner Psychologists. 3 If this is not adhered to, registration can be withdrawn. 3 Guidance is also available in the BPS Code of Ethics and Conduct, 4 focusing on the four ethical principles of: respect, competence, responsibility and integrity, that members are expected to uphold. An earlier version of this guidance offers a system for approaching ethical decisions based on theoretical frameworks. 5 These codes were developed through reviewing existing codes and guidance and reflection on what is expected ethically by the Society and in relation to other professions. 4
The existence of such codes, the regulation and the imperative for ethical behaviour may lead to the assumption that clinical psychology is an ethical profession. However, there remains a need for developing ways to support ethical practice, as the challenges that clinical practice presents change and have become more demanding. In 2018, HCPC Conduct and Competence Committee panel hearings resulted in three practitioner psychologists being removed from the register, seven having conditions placed on their practice and five being suspended for ethical breaches. 6 As there were 24,340 practitioner psychologists on the register in April 2019, 7 this is a relatively small proportion; but, of course, this represents only the most serious breaches that were reported and substantiated. It may be reasonable to assume that more ‘minor’ breaches are not covered by these statistics, are not discovered and/or are not reported.
Although there are different regulatory frameworks for psychologists outside of the UK, no further statistics were available for UK practice or professional opinion on different behaviours which could pose ethical challenges. Turning to the USA then, a survey of psychologists (n = 456) found that 2.9% reported ‘engaging in erotic activity’ with a client, 8.1% reported discussing ‘a client (by name) with friends’ and 5.9% reported practicing under the influence of alcohol. 8 However, 95.0, 94.5 and 89.5% of those surveyed believed that these behaviours are never ethical, respectively. A more recent replication of this survey (n = 325) suggests that ethical practice may have become more conservative in the USA, particularly for early career psychologists. 9 The psychological implications of ethical breaches are serious for those using clinical psychology services and for the level of trust placed in the profession of clinical psychology. It is therefore important that complacency is avoided.
Leaving serious infractions aside, recognising and responding appropriately to ethical dilemmas is arguably part of the day-to-day practice of clinical psychology. It is therefore important for quality assurance that a thorough understanding is developed of how ethical decision-making occurs. Pope et al.
8
concluded that: The integrity of psychology is contingent to a great degree on the extent to which we – both as a discipline or profession and as individuals – can regulate our behavior. Our ability to engage in effective and ethical regulation, in turn, is contingent on our willingness to study our own behavior and our beliefs about that behavior. (p. 1004).
With regards to counselling, a narrative review 10 of theoretical models and empirical studies on ethical decision-making concluded that ‘… surprisingly little research has been done on ethical decision making or models of decision making in counseling. There is much work in the ethics area that must be accomplished’ (p. 281). Given that this review itself is nearly two decades old, and ‘few studies have empirically examined the decision making process …’, in clinical psychology 11 since then, this is arguably an opportune time to systematically assess the available relevant literature.
Literature reviews completed between November 2017 and May 2019 revealed no comprehensive empirically derived or tested models of ethical decision-making in clinical psychology, and very few when broadened out to related disciplines. This appears to contrast other fields such as bioethics, whereby 309 published empirical articles were identified in a review of nine journals between 1997 and 2003. 12 As clinical psychology is underpinned by ethical codes and regulation,2–5 the disparity in levels of research between these professions may at first seem surprising. A number of hypotheses are suggested to explain this, including the relative size of the professions. In 2019, there were 24,340 practitioner psychologists registered with the HCPC in the UK, with approximately half of these being clinical psychologists. 7 This compares to 312,689 doctors registered with the General Medical Council in the UK in 2020. 13 Furthermore, bioethics is a broad field, much of which is considered applicable to the practice of, and research into, ethical decision-making within clinical psychology. Given that ethical decision-making in clinical psychology is less obviously physically risky or invasive, it may also be that the focus of research within ethical decision-making is narrower.
A systematic review of empirical research into ethical decision-making in clinical psychology and related fields was therefore indicated, with the aim of summarising the literature available. Although there are some important differences between professions in terms of the training backgrounds and regulatory frameworks, the search was extended to include professionals delivering talking therapies (this was defined as: clinical psychologists, counselling psychologists, applied psychologists, counsellors and psychotherapists) and to explore factors affecting ethical decision-making, as well as models of ethical decision-making. The following research question was therefore investigated: What does empirical research suggest about how professionals who deliver talking therapies make ethical decisions related to their work?
Method
A systematic review of literature addressing this question was completed between April and May 2019 drawing on best practice guidelines for systematic reviews in psychology. 14 Searches were carried out using the following databases: PubMed, Scopus and PsycARTICLES. Table 1 shows the search terms used.
Literature search terms used in systematic review.

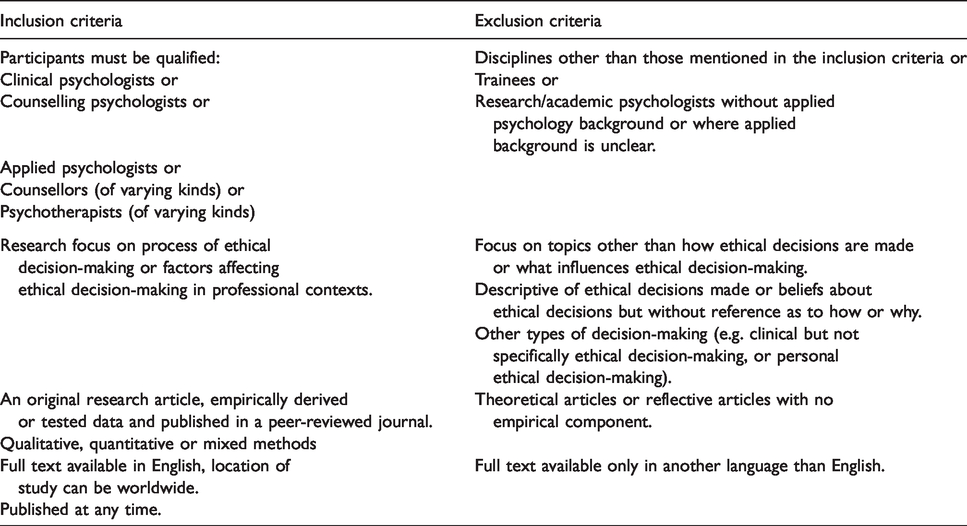
Table 2 highlights the inclusion and exclusion criteria. Due to the limited number of publications on the topic, an earliest publication date was not specified nor was a country of origin (although all must be published in full in English). It is recognised that these criteria may have brought some limitations, as discussed later.
Inclusion and exclusion criteria for research included within systematic review.
In total, 957 articles were identified; of these, 33 were duplicates, giving an initial pool of 924 unique articles to be considered against the criteria outlined in Table 2, to determine their suitability for inclusion in this review. On this basis, 819 of these articles were screened out by reviewing their title. These articles were considered to be unsuitable as their titles indicated that the research did not fit with one or more of the inclusion criteria. For example, many titles made reference to ethical decision-making in different professional groups or to the processes related to personal (rather than professional) ethical decision-making.
This meant that abstracts from 105 of the 924 articles were read to further consider if they met the criteria for inclusion in the present review. Of these 105 articles, 50 were considered unsuitable for the present review and were therefore screened out due to the abstract indicating that the research was not empirical in nature; 29 were screened out due to not fitting with the participant inclusion criteria, and 11 were screened out due to not fitting with the ethical decision-making criteria, both outlined in Table 2. Based on the information in their abstracts, 15 articles were therefore taken forwards to be read in full, to assess whether they met the inclusion criteria for this review. Five further articles were identified through other means, such as from a review paper, 10 reference lists and articles already known to the lead author. Full-text reviews were therefore completed on these 20 articles. Of these articles, three were subsequently screened out due to information within the body of article indicating that the research did not fit with the participant inclusion criteria, outlined in Table 2 (which had not been apparent from review of their titles or abstracts alone). For example, one study included participants from a variety of professional groups, including social work, nursing and medicine, as well as psychology. 15 Of the 20 articles which were reviewed in full, a further two were screened out due to not fitting with the inclusion criteria related to ethical decision-making (for example, an exploration of participants’ experiences of ethical challenges within their social context), 16 a further article was screened out as only the title and abstract were available in English, and one final article was screened out due to the body of the text clarifying that this was not empirical research. Therefore, based on the inclusion criteria outlined in Table 2, 13 of the originally identified pool of articles were found to be suitable for this systematic review.11,17–28 This process is summarised in Figure 1.
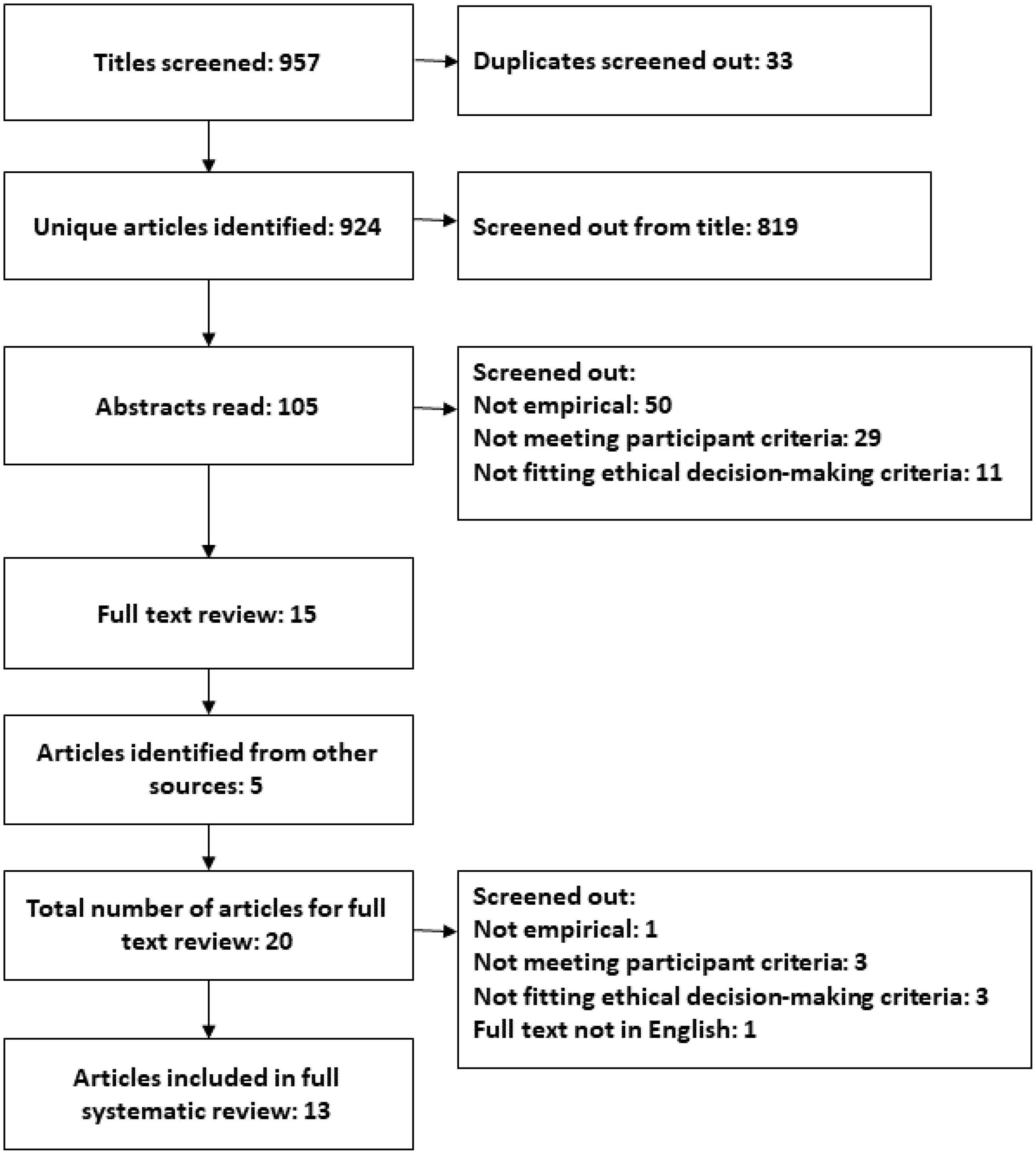
Flow chart to show the systematic review process.
Of the 13 articles, 10 employed survey methodology.11,17–25 Of these, eight employed quantitative methods solely11,17–23 and two used mixed methods.24,25 Whilst it is recognised that there are specific tools to evaluate the quality of mixed-method research, 29 both of these studies presented very little information about the qualitative aspect of their research, and results were mainly reported quantitatively. In the interests of enabling comparison of quality between articles, these 10 articles were all appraised using Burns and Kho’s 30 quality assessment criteria. This provides a framework for assessing the quality of seven aspects of design and reporting, deemed to be important for high quality survey research. 30 Three articles comprised qualitative analyses of semi-structured interviews. These were appraised using Tracy’s 31 quality criteria, a tool to assess quality across eight areas of qualitative research methodology and outcomes, which can be flexibly applied to different types of qualitative research. 31
Two independent reviewers (the first and fourth authors) read and quality assessed the articles separately. Using the above structured assessment tools, the reviewers made written notes and rated the extent to which each article met each of the criteria. For example, with the quantitative articles, when considering Burns and Kho’s 30 first criterion, the authors recorded whether they felt that clear research questions had been outlined in each article (i.e. yes, no or to some extent) and provided some explanatory notes, such as highlighting where articles had stated research objectives but had not phrased them as questions, or where the participant group was not explicitly defined within the research question. Similarly, with the qualitative articles, when considering Tracy’s 31 first criterion, for example, the authors recorded whether they felt that each article represented a worthy topic by considering whether it was relevant, timely, significant and interesting.
The first author then compared both reviewer’s notes and highlighted the differences between them. It is notable that, on the whole, the two sets of reviews were concordant. The reviewers then met to compare their notes and develop agreed positions for all the criteria relevant to each article. Agreement was reached in these areas through joint review of the relevant parts of the article, discussion of each reviewer’s rationales and adopting a negotiated position where necessary. Discrepancies were generally attributable to minor differences in interpretation of the quality criteria or preference for style. For example, in one article, 21 one reviewer felt that the survey had been pilot tested according to criterion four, 30 whereas the other did not. Upon re-examination of the article, it was rated as partially meeting the criterion, as aspects of the survey had been tested individually but not in entirety in its final form.
Results
Two models to explain aspects of ethical decision-making were identified. Two types of factors were found to influence ethical decisions: factors relating to the decision-maker and factors relating to the ethical dilemma itself. Following this, methodological strengths and weaknesses of the literature are described as well as identified gaps.
Models of ethical decision-making
Two studies tested theoretical models of aspects of ethical decision-making: one amongst clinical psychologists 11 and one with school counsellors. 22 A qualitative study 26 put forward themes to explain aspects of counsellor ethical decision-making.
A survey 11 asked clinical psychologists in Israel (n = 395) to respond to one of two vignettes relating to either dual relationships or financial matters. This research assessed ethical intention (an ethical decision which is made, which can be hypothetical, rather than a completed action) in comparison with the Theory of Planned Behaviour. The model suggests that decision-makers’ reported attitudes (such as a positive evaluation of a course of action), subjective norms (such as social pressure) and perceived control of their ability to implement a particular behaviour both impact ethical intention. They added professional commitment towards the client into the model and found that this explained more variance than without it. They report that attitudes and commitment predicted ethical intention most significantly, and this is thought to then drive behaviour. A strength of this study is that this model was tested across two different ethical dilemmas. However, a limitation is that each participant responded to only one dilemma, meaning that comparison between groups is restricted. Their results suggest that whilst the type of vignette impacted ethical intention, the model does not encompass contextual factors related to the dilemma or the interaction between the dilemma and the decision-maker. A limitation of this research is that there is no qualitative aspect; participants could rate only the influence of factors stipulated by the researchers. If other factors had influenced their decision-making, this would not have been identified. It is unclear whether the findings can be generalised to the UK context due to Israel having elements of both individualistic and collectivist cultures 32 which may influence attitudes anda different political context (political beliefs are considered to impact ethical decision-making). 33 Further, clinical psychologist qualifications may not necessarily be equivalent between Israel and the UK, 34 and as such the level of experience and training route may have an impact on ethical decision-making.17,22,23
Luke et al. 22 compared USA school counsellors’ (n = 897) ethical decision-making to the Intercultural Model of Ethical Decision Making using a cross-sectional survey. This is a stepwise framework to guide counsellors in ethical dilemmas involving cultural, religious or worldview factors. A limitation with this research is that only one vignette was used, with multiple complexities around the protagonists’ cultures, religious beliefs and worldviews. Although this has ecological validity, it is unclear which factors or what proportion of each impacted the decision-making. The authors report low levels of ethical sensitivity in their sample (10% of participants identified that the vignette depicted an ethical dilemma), which itself had a low response rate (less than 7% of those the survey was sent to).
Together, these models explain aspects of ethical decision-making, but are not comprehensive. There are clear limits as to how generalisable they are to the UK clinical psychology context due to the different cultural contexts, differing regulatory standards and professional training backgrounds. Furthermore, both articles test models, which have been theoretically developed, rather than inductive methods informing the development of a model.
Decision-maker factors
A large number of factors relating to the professional were identified as impacting ethical decisions. Several of these were only found in only one article and as such are not reviewed in detail here. These include the professional’s theoretical orientation, 17 commitment to the client, 11 personal biases, 19 commitment to transparency, 26 professional judgment 27 and perception of clients’ motivations. 24
Professional perception of clients’ best interests
There was agreement in the literature that professional’s perception of what is in the client’s best interests are taken into account when making ethical decisions. Considering the USA managed mental healthcare payment model, 21 the principles of autonomy and beneficence were most highly prioritised in ethical dilemmas in a survey of child and paediatric psychologists (n = 252). Strengths of this research include the use of three ethical dilemmas to explore the one context and the high credibility ratings given by participants of the dilemmas (between 83 and 97.6% across the different dilemmas). A limitation is the focus on the payment system, which is less applicable to countries like the UK, where there is publicly funded healthcare. There is also limited clarity as to how the vignettes were generated, whereas other studies have based their vignettes on existing literature, 11 case material 18 or through consultation. 24
In a grounded theory study, 27 it was found that family therapists (n = 15) drew on what they believed to be in the client’s best interests when making ethical decisions. The methodology increases the external validity of the study, as these ideas were generated by participants rather than selecting from a pre-determined list. Another grounded theory study 25 identified a key theme of ‘maintaining a therapeutic relationship to facilitate client self care’ (p. 101) amongst clinical psychologists (n = 5) making ethical decisions. This arguably shares characteristics with taking account of what the decision-maker considers to be in the client’s best interests. Strengths of this research include aspects of its credibility, involving triangulation within interviews and member checking. A mixed-methods survey 25 of USA clinical psychologists (n = 113) found that perception of what was in the client’s best interests impacted ethical decision-making. However, sparse information on the qualitative aspect of this research meant that only the quantitative aspect could be evaluated in this review. A strength of their research is the use of 12 different vignettes compared to those who asked each participant to consider one vignette only.11,22 Overall, this suggests that those delivering talking therapies are likely to draw on their beliefs about what is in the clients’ best interests when making ethical decisions.
Personal ethics
There was agreement that personal ethics impacted professional ethical decision-making. A phenomenological study 26 showed a vignette representing a boundary issue to counsellors (n = 5) and asked them to describe how they would reason through it. A potential limitation with this method is that it suggests a reasoned thinking process will necessarily be found, although it is possible that decisions may be more automatic and involve only limited conscious processing.35,36 This is however argued to be a robust method, and improvements in reliability can be achieved through triangulation. 37 This was addressed through summarising during data collection, member checking, group coding and group review of transcripts during analysis. 26
This is supported somewhat by a mixed-methods survey 24 assessing factors impacting psychologists’ (n = 40) acceptance of gifts from clients, in which two participants indicated that they would decline gifts, due to their personal ethical codes. A limitation of this article was that insufficient information was given about the qualitative aspects to enable quality assessment on the most appropriate criteria, as with the other mixed-methods research in this review. 25 This study also had a small number of participants, a low response rate (27%) and only looked at one type of ethical decision (gift acceptance). A strength of this research is the multiple-varied dilemmas, enabling comparison of the influence of different contexts. Overall, this suggests that professionals delivering talking therapies are likely to be influenced by their personal ethics when making ethical decisions.
Professionals’ gender
There was limited agreement about the influence of gender upon ethical decisions. Two studies14,20 found that gender had an impact, whereas one did not. 21 When USA psychologists (n = 294) were presented with 10 vignettes on five different topics, 17 male psychologists were more likely to act to ensure that sexual exploitation was reported, whereas females were more likely to inform the client of their rights. In another vignette, male and female participants were both likely to decline services in lieu of payment, but this was demonstrated more strongly for female participants. Unfortunately, these findings are difficult to interpret due to inconsistent reporting within the article about their participant demographics, making it unclear whether their sample was representative of the population from which it was drawn. In a survey 20 of paediatric psychologists (n = 169), participants were asked to identify, from a list of behaviours (such as ‘lying to a child’ or ‘breaking confidentiality if client is suicidal’), whether they had done each one and give a rating of how ethical they perceived it to be. They found that female psychologists tended to endorse more extreme positions (i.e. ‘unquestionably ethical’ and ‘unquestionably unethical’). Limitations of this research include the exploratory rather than experimental nature of the research and the length of the questionnaire (101 non-randomised items, which may have led to order effects). A strength of the study is that there was an approximately even gender split (45% male), although this may mean that males were overrepresented in the sample compared to the population at the time. 38 Conversely, another survey of psychologists working with children, 21 with an approximately even gender split in participants (47.4% male), found no differences between male and female psychologists’ attitudes towards managed care. This suggests that gender may have an influence on ethical decision-making, but there may be numerous reasons for this.
Professionals’ work settings
Another area of debate was whether professionals’ work settings impacted their ethical decision-making. Psychologists working privately held more negative attitudes towards the managed care model than those in hospitals. 21 The setting may be particularly relevant to the managed care context due to the differing financial implications, whereas another study found that setting had no impact. 17 This suggests that, where salient, professionals’ work settings may have an impact on ethical decision-making.
Professionals’ level of experience
Another area of debate between articles was found with regard to years of experience. More experience was correlated with less reporting and more indirect action in two of 10 vignettes from one study. 17 A survey 23 asked rehabilitation counsellors (n = 658) to rate how ethical they felt behaviours were and give confidence ratings. Of the behaviours that were rated overall as controversial, participants with three or more years of experience were more confident in their ratings of these items. A strength of this research is that the questionnaire had been validated, and the additional rehabilitation-specific questions were tested with a panel with expertise. A limitation is the length of the questionnaire (104 items) and that the items were presented in a static order, as per another study in this review. 20 Similar to years of experience, it was suggested that dilemmas which had the strongest consensus were more widely discussed (such as sexual behaviour, confidentiality and risk), so participants may be more familiar with ethical decision-making in these areas. 25 However, another study found no effect of years of experience on ethical decision-making, in the managed care context. 21
Related to years of experience, there was debate in the literature about whether professionals’ level and type of ethics training influenced their ethical decision-making. In one study, 17 hours of formal ethics training did not have an impact on ethical decisions or reasons. This may be explained as one study found perceptions of a disconnect between training in ethics and practice. 26 Psychologists who had trained at courses approved by the American Psychological Association (APA) were found to endorse more extreme positions (i.e. ‘unquestionably ethical’, ‘unquestionably unethical’) than those who had trained elsewhere. 20 Taken together, the literature suggests that professionals’ level and type of experience in ethical decision-making may have an impact on the ethical decisions, under certain contexts.
Dilemma factors
A number of factors related to the dilemma itself were found to influence ethical decision-making and are now reviewed.
Dilemma context
Perhaps not surprisingly, the context of the ethical dilemma was found to impact ethical decisions. Comparing two dilemmas, differences were found in the factors taken into account by the two groups of participants making different ethical decisions. 11 Although the authors concluded that decision-maker factors play a substantial role in ethical decision-making, these contexts may influence the decision-maker differently. The managed care context was found to negatively impact decision-making, 21 with some participants reporting that they would purposefully misdiagnose a client. Where professionals rated ethical decisions as difficult, there was less agreement about whether an action was considered ethical. 23 As outlined above, ethical topics which appear to be more widely discussed had greater consensus. 25 This could be about familiarity, or an aspect the dilemma, such as the availability of guidelines.
Gift value
Considering gift giving, it was found that the perceived value of a gift from a client impacted the likelihood of it being accepted; with less expensive gifts being more readily accepted. 24 This finding was also observed to interact with the client’s age, whereby professionals were more likely to accept a low value gift from a child, than they were a high value gift from an adult. 20 The authors hypothesised that this may be influenced by the psychologist’s theoretical orientation and the lack of clear professional guidelines on the acceptance of gifts. This suggests that factors related to financial value in a dilemma can impact professional ethical decision-making, in relation to gift acceptance.
Cultural factors
Two studies suggested that cultural factors can impact ethical decision-making.22,24 As described above, 22 the culture of an organisation (such a procedural pressure) and differences in religious beliefs or worldviews between professionals and clients or families may mean that ethical decisions are more process-oriented than value-based. Similarly, if gift giving by clients was perceived to be borne out of cultural significance to the client, then professionals were more likely to accept it. 24 This suggests that cultural factors related to the dilemma can impact professional ethical decision-making.
Situational pressure
In a survey 18 of USA mental health counsellors (n = 72), increased pressure in an ethical dilemma reduced the quality of the decision-making style, leading participants to be hypervigilant, and seek quick solutions or novel courses of action with limited regard for the risks. It is not clear what the authors mean by the high- and low-pressure conditions in their vignettes as only one example was provided. However, this is inferred to relate to more immediate risks. Strengths of this study include a moderate response rate achieved through a follow-up procedure. These findings are supported by results of a survey 19 of USA psychologists (n = 625), which found that where clients’ behaviours were considered higher risk, this impacted the decision to breach confidentiality, when working with clients with HIV. This study also found that a decision-maker factor (endorsement of homophobic attitudes) had a similar effect. It is notable that all participants were from one state in the USA, and, like all research, this is bound to a particular time-context. Although their questionnaires were adapted and combined in a random order from previously published questionnaires, the quality of this is limited by the lack of detail about how this was done and the validity and reliability of the new scale, making it difficult to replicate. That being said, similar findings were found in another study20 to support the role of higher risks as impacting ethical decision-making, such as the perceived severity of the client’s presenting problem.
Overall, this suggests that factors related to the ethical dilemma, such as those related to the client, or facets of the dilemma itself, have an influence on professional’s ethical decision-making. This is in comparison with decision-maker factors, where there is more debate in the literature about whether specific characteristics impact ethical decision-making.
Quality assessment
Methodological strengths and difficulties have been outlined above with reference to specific articles. At this point, commonalities between the quality of the literature will be reported.
Areas of methodological strength
Except for one article, an exploratory study, 20 all the research shows methodological quality through the research questions, hypotheses or general area of research being clearly defined. This enabled the results to relate back to these clearly, which, on the whole, were presented with sufficient data to allow the reader to generate their own conclusions. In general, the interpretations provided by the authors aligned with the results presented. All studies identified their target population and provided detail on participant demographics. The qualitative articles26–28 can all be considered worthy topics as they extend the literature on professional ethical decision-making and highlight further areas for research.
Areas of mixed methodological strengths and difficulties
There was variation in the level of validity and reliability measures. For example, credibility is demonstrated in the qualitative studies by the inclusion of member checking26,28 and triangulation.26–28 However, in a quantitative survey, 20 only one reliability check was reported through the duplication of a question, which was found to be unreliable. This limits the conclusions and implications which can be drawn from this article, and the results are therefore considered in the context of results from other articles. Contrastingly, quality is demonstrated in another article 11 through an extensive pilot to develop responses to their vignettes. They report acceptable levels of reliability of the instrument utilised (Cronbach’s α ratings between 0.64 and 0.95). Across the remaining articles, there was variability in the quality of how the vignettes are generated, such as having limited information, 25 or by drawing on literature, 11 consultation, 24 case material 18 or a combination of methods. 22
Areas of methodological difficulties
Across the review, common themes of methodological difficulties were noted. Only one of the articles 25 provided information on how missing or incomplete data was handled for the purposes of data analysis, meaning that the reader cannot directly assess the validity of statistical conclusions reached in other articles. Similarly, no articles presented their questionnaires in full for the reader to review, and many articles only gave an example vignette rather than providing all of them for examination. All surveys had a low-to-moderate response rates, and on the whole, non-responders were not followed up, which could have increased generalisability of the research.
Most studies employed hypothetical ethical dilemmas in the form of vignettes, rather than asking participants about their experience of ethical decision-making. Some research suggests that hypothetical, compared to actual ethical decision-making may rely on different neural mechanisms. 39 Two qualitative studies26,28 investigated participants’ ethical decision-making in clinical practice. However, neither reported how situational ethics (ethical issues arising out of the research; for example, if participants had disclosed illegal or ethically uncomfortable practices) were, or would have been managed.
Discussion
Gaps in the literature
Drawing the literature together, some important gaps are highlighted in relation to the topic and methods. Despite there being many commonalities between professionals delivering talking therapies, there are also important differences in their approach, client groups, settings and levels of training; all of which may have an impact on their ethical decision-making.
No studies speak to the UK context specifically, and all but one 11 was based in the USA. There are obvious differences between the healthcare systems in these countries, with UK clinical psychologists mainly working in the NHS. 1 Further cultural differences are relevant between the USA and UK. For example, an article about rural communities in the USA 27 included participants who supported a population of >100,000 people, which is less likely to be considered rural in the UK.
The time context is also considered to be important. Ethical problems and beliefs can change over time, 9 as does the makeup of the workforce. Many of the articles inlcuded in this review are a number of decades old now, and it remains to be seen whether the findings are still relevant today.
Several of the articles utilise only one vignette,11,22,26 and some use several vignettes but representing different aspects of one type of dilemma.21,24 Whilst this depth enables thorough assessment of those factors in particular, having fewer vignettes may limit generalisability to other aspects of ethical decision-making.
Articles utilising qualitative and quantitative methods of enquiry were found, yet no high quality mixed-methods research was identified. The quantitative research limited participants to commenting only on survey items already selected by the researcher, whereas the qualitative research had relatively small sample sizes, potentially limiting generalisability.
Implications and further research
As outlined in the introduction, there are a number of hypotheses about why there appears to be less research into ethical decision-making in clinical psychology compared to other disciplines such as medicine (although it is acknowledged that there can be a significant overlap in applicability of the research). However, the present systematic review has identified specific gaps in the research focusing on ethical decision-making amongst those delivering talking therapies, suggesting that there is a need for further research here. Specifically, up-to-date, profession-specific research is indicated, although it is recognised that the relative smaller size of each of these professions may pose a constraint. This review also suggests that mixed-methods research, drawing upon more than one vignette to illustrate ethical dilemmas, may increase the methodological quality of any future research undertaken.
Implications of this review suggest that it may assist professionals delivering talking therapies in their reflective practice to consider aspects of themselves (such as their perception of the client’s best interests and their personal ethical beliefs, in relation to others) and aspects of the dilemma that may be influencing their ethical decision-making. However, further research is needed into when factors related to the ethical decision-maker (such as gender, level of experience and work setting) are likely to impact the decision, as there was limited agreement in these areas. Although there was more agreement about how factors relating to the dilemma impact ethical decision-making, it is also suggested that further research is needed. 25 This could include altering the independent variable of dilemma context, or client-related factors through multiple similar vignettes.
Mixed-methods approaches and the use of multiple ethical dilemmas could increase generalisability of research into ethical decision-making amongst professionals delivering talking therapies. Increased generalisability of findings could have important clinical implications for professional groups, and this may be particularly useful during training and CPD. Further research using vignettes could enable the development a structured tool for use in professional instruction in ethics however, 23 : ‘… it would be important to construct an instrument that utilizes scenarios so that a context for the ethical behaviours being rated is provided’. (p. 16)
Limitations
Some limitations were noted with this review, related to the inclusion criteria and the quality assessment tools used. The inclusion criterion of articles published only in English in full meant that at least one article that may have been relevant was not included. 40 From the abstract (available in English), this research looked at clinical psychologists’ (n = 182) beliefs and behaviours in relation to non-sexual dual relationships, in the Republic of China. Nevertheless, as with the research from Israel, 10 there may be important cultural and training differences between clinical psychologists working there and in the UK.
The inclusion criteria of only articles published in peer-reviewed journals may have introduced a publication bias and some potentially relevant unpublished quantitative research or research from the grey literature may have been missed. However, some studies did report non-significant findings,17,21 and this criterion was set to ensure that the highest quality research was included. Whilst this study attempted to systematically review all the available articles on the topic from peer-reviewed journals, further research could include attempts to explore grey literature, in order to consider the topic more comprehensively.
A limitation of one of the quality assessment tools 30 is that there are no criteria to assess ethics of the research. The authors acknowledge this and suggest that consent is implied by participants returning questionnaires. 30 However, inclusion of a criterion related to whether ethical implications have been considered would improve the rigour of this tool and would be particularly pertinent to research looking at ethics. A strength of the qualitative assessment tool 31 is the focus on how different types of ethics have been approached. A limitation of this is that procedural standards (such as whether a research question is stated) are less well explored than they are in the quantitative tool. 30
Summary
In summary, there is a limited body of empirical research into ethical decision-making amongst professionals delivering talking therapies and specifically in clinical psychology. This review suggests that there are a number of factors related to ethical dilemmas and to the decision-maker which impact ethical decision-making amongst professionals who deliver talking therapies. The review identified a need for further, up-to-date, research into ethical decision-making and a focus on individual professions. One empirically tested model of ethical decision-making in clinical psychology was identified, 11 which may have limited generalisability to the UK context. This suggests the need for the development of an empirically derived model of ethical decision-making in clinical psychology to increase the understanding of the process, including the interplay between dilemma factors and factors related to the decision-maker. As summarised by Levitt et al., 26 the ‘… development of a practitioner’s ethical decision-making model may be useful to both further research and practice’ (p. 97).
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.