
Abstract
Epidemiological studies indicate that the incidence of shaken baby cases is overestimated and that this is due to biased classifications, based on ethical rather than scientific considerations. In the present paper, we analyze the nature of the ethical considerations and how they made their way into the classification procedures. We argue that the ethical considerations and derived values are associated with the aim of protecting infants from abuse. We further argue that these values are applied in choosing between two opposing mechanism theories: (1) in the absence of any “acceptable” explanation for certain symptoms and signs, the infant must have been shaken violently and (2) the symptoms and signs might have other and even natural causes. According to the first theory, almost all such cases will be classified as shaken babies, but almost none according to the second selected theory. Thus, the choice of theory has consequences for the classification of shaken baby cases. In this manner, values enter the scientific classification “through the backdoor,” hiding them from criticism. Such classifications have consequences when calculating the diagnostic accuracy of the symptoms and signs, which might become perfect or almost perfect. The near-perfect results are, however, based on circular reasoning which might be self-reinforced when repeated. We conclude that the classification of shaken baby cases in most previous publications is based on a value-impregnated choice of theory, which obscures the values as if the classifications were based solely on scientific reasoning.
Introduction
In an epidemiological study from the USA, it was suggested that the officially registered increase in infanticides during 1980–2005 is an effect of biased classifications, attributable to issues such as ethics and increased societal sensitivity to child abuse. 1 Similar corroborating results have recently been presented in two Swedish studies.2,3 All three studies indicate that non-scientific considerations have biased the classification process, resulting in an overestimation of at least shaken baby cases, a typical case being a two-month old infant with subdural and retinal hemorrhages, but no external signs of head trauma. Such cases constitute approximately one-third of all so-called abusive head trauma (AHT) cases which also include cases with external signs of trauma – e.g. bruises and fractures. 4
The aim of the present paper is to identify the nature of such non-scientific considerations and to try to explain why criteria favoring shaken baby syndrome/abusive head trauma (SBS/AHT) are applied. Our thesis is that the criteria used by a child protection team are based on a certain theory of the mechanism of findings associated with traumatic shaking, and that the choice of this theory is value based. 5 These values enter, however, “through the backdoor”; thus, the clinical criteria appear to be solely scientifically based. 5 The determination of suspected SBS/AHT cases by individual clinicians and child protection teams has, in turn, consequences for the researchers’ classification of SBS/AHT cases. In this manner, the scientific enterprise facilitates circular reasoning and an overestimation of cases.
In the following, we present arguments supporting our thesis.
The triad issue
The theory underlying the SBS/AHT criteria for classifying positive cases is based on a pathogenic theory, here referred to as the traditional shaken baby theory, which presupposes that only relatively high energy force can cause subdural hematoma, encephalopathy and retinal hemorrhages – referred to as the triad. 6 According to this theory, three separate and independent factors are supposed to affect the brain, the bridging veins and the eyes: violent shaking is supposed to (i) have a direct impact on the brain by damaging nerve fibers, to (ii) tear one or more bridging veins, resulting in a subdural hematoma and to (iii) tear the vitreous body from the retina, resulting in retinal hemorrhages, allegedly pathognomonic. 6
Studies have, however, indicated that the retinal hemorrhages are not pathognomonic but most probably secondary to increased intracranial pressure. 7 Moreover, the encephalopathy seems to be caused by hypoxia, brain edema and increased intracranial pressure, rather than by disrupted nerve fibers.8,9 Finally, it has also been suggested that isolated shaking – without impact on the infant’s head – is not enough to bring about the triad. 10
The choice of mechanism theory and risk of circular reasoning
According to the traditional shaken baby theory, formation of a subdural hematoma in a baby requires violent shaking.6,11 Thus, according to this theory, if a subdural hematoma is identified in the absence of signs of external impact on the baby’s head, it is concluded that the infant must have been violently shaken – regardless of the statements to the contrary by the parent. 12 Such a case is classified as shaken baby syndrome (SBS) – or if the outcome is fatal, as infanticide.
Hence, the selected theory has a strong impact on the criteria applied by a child protection team investigating a suspected case of child abuse, or when a team member appears as an expert witness in court – increasing the risk of false confessions. 12 Decisions made by child protection teams are subsequently used by researchers when classifying the cases of SBS/AHT in observational studies which are also used for calculating the diagnostic accuracy of the triad as a diagnostic test. However, in order to calculate the accuracy of a diagnostic test, the “diagnosis” (in this case: traumatic shaking) must be verified with a corroborated measure – a reference test or if possible a gold standard. If the selected reference test, however, is identical to the diagnostic test to be evaluated, only true positive (TP) and true negative cases will be disclosed: false positive (FP) and false negative cases will disappear 13 – see Table 1.
Shows the two options (Yes=Positive and No=Negative) of the diagnostic test and reference test.
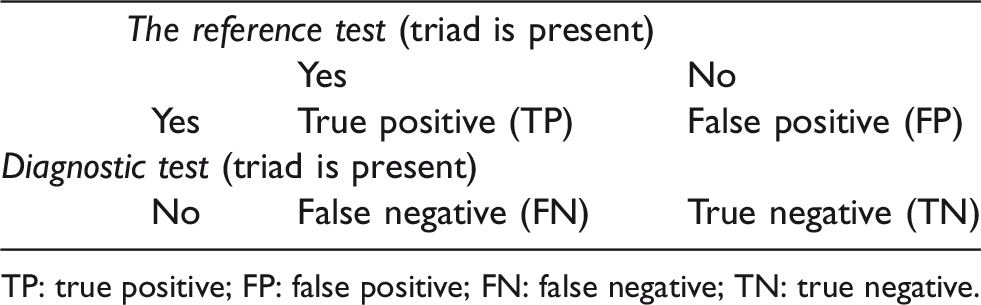
TP: true positive; FP: false positive; FN: false negative; TN: true negative.
The potential of the diagnostic test to predict traumatic shaking, given that it has really happened, is calculated as the proportion of TP divided by the sum of TP plus FP. The potential of a test to predict that traumatic shaking has taken place is referred to as the test’s positive predictive value, calculated as TP/(TP+FP). If the number of FP cases is zero, the calculation becomes TP/TP, i.e. 1 or 100%: thus, the positive predictive value will be perfect. 13 In other words, based on the calculated diagnostic accuracy, it might be concluded that in cases where the triad is present, and after exclusion of certain diseases or accidents, violent shaking is the only explanation.
Normally, however, when calculating the diagnostic accuracy, it is a requirement that the reference test is independent of the diagnostic test. Failure to ensure that the two tests are adequately separated will result in an increased risk that what is tested is already taken for granted as truth – a procedure referred to as circular reasoning. 13 If the diagnostic test and the reference test are identical, the diagnostic accuracy is based on nothing but circular reasoning. Using child protection teams’ clinical determinations of SBS cases based on the presence of the triad without impact as the reference test and the triad without impact as the diagnostic test will by definition result in circular reasoning.
If circular reasoning is combined with the traditional shaken baby theory, the SBS enterprise will become self-reinforced 13 – see Figure 1.
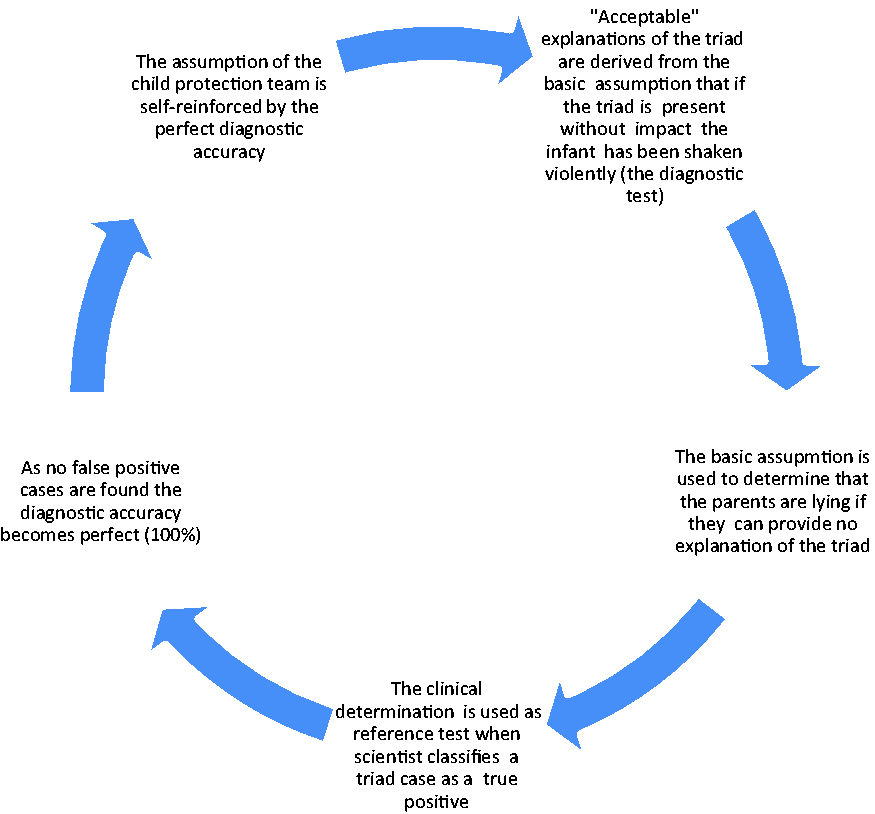
The self-reinforced power of a diagnostic test if it is based on certain basic assumptions and circular reasoning. 13 The triad implies subdural and retinal hemorrhages combined with encephalopathy but in this context without external signs of trauma.
If the traditional shaken baby theory was consistent, coherent and correct, the criteria and epidemiological classification of SBS cases and non-SBS cases would be readily accepted – although not the circular reasoning. However, the traditional shaken baby theory seems to be neither coherent nor consistent.6,12,13 For example, it has been suggested that there is a discrepancy between what is expected to be observed according to the selected theories and what is actually observed. 12 While rupture of a bridging vein has been suggested to result in a large, localized subdural hematoma, the triad cases usually have only a thin blood film covering both cerebral convexities.6,12
Further, there are alternative theories explaining the mechanisms underlying the development of a subdural hematoma. One such alternative mechanism theory is the hypoxia-capillary theory.8,9 This theory has actually gained support in a Bradford Hill assessment and is strongly preferred to the traditional shaken baby theory 14 . This is why we have chosen to present the hypoxia-capillary theory here.
The hypoxia-capillary theory
According to this theory, hypoxia results in brain edema (swelling) and increased intracerebral pressure, which in turn leads to a capillary-based subdural hemorrhage of the type described above.6,8,9 According to the hypoxia-capillary theory, shaking without signs of impact is certainly not a prerequisite for the development of a subdural hemorrhage or the triad. Hence, if this theory is applied, such cases would probably not be classified as intentional and we might refer to the non-shaking baby theory.
Thus, we contend that the criteria for classifying infant deaths as accidental, natural or homicidal depend on the theory applied – the traditional shaken baby theory or the hypoxia-capillary theory. It seems reasonable to assume that for physicians involved in investigations of child abuse, the choice of theory is influenced by values and preferences associated with the prevailing aim of protecting infants from abuse. 13 Application of the traditional shaken baby theory implies that very few or no babies will be at risk of negligence and that all suspected abusers, including an unknown number of innocent parents, will be charged. Under the traditional shaken baby theory, the number of child abuse cases – fatal or not – will be overestimated.
Under the hypoxia-capillary theory, it is likely that no triad cases without impact would be classified as caused by intentional trauma. This theory would thus discourage police and prosecutors from assuming that there is no “acceptable” explanation other than violent shaking. This in turn would reduce the incidence of false confessions. Furthermore, such cases would probably be excluded from epidemiological studies and the number of registered cases of AHT cases would decrease by approximately one-third. 4 However, the hypoxia-capillary theory has been questioned and a systematic literature review which has criticized the observational studies behind the traditional shaken baby theory has been described as “catastrophic” and “disastrous.”15–17 Critics of the traditional shaken baby theory have even been described as “denialists” of child abuse! 18
Values in the name of science
It is not unusual for societal and scientific interests to interact. But if enfolded into political ideologies, religious beliefs or certain societal values, science might become ideological. With respect to SBS/AHT research, pediatric and societal values and preferences have had a pronounced influence on the investigation of suspected SBS cases. The societal values and subsequent attitudes are expressed in, e.g. the Swedish Social Services Act, which requires healthcare providers to report concerns that an infant might be risk of abuse or neglect. Societal preferences in the care and protection of infants and small children have also been illustrated more generally in a recent experimental study of attitudes among the general public towards exposure to danger: the highest prioritized group comprised infants in strollers. 19
Societal values and laws regarding prevention of child abuse have legitimized the concerned clinicians’ procedures. But the choice of the traditional shaken baby theory seems to be merely value-impregnated. 5 In this manner, the SBS/AHT scientific enterprise has become ideological – although presented as if it were based solely on scientific studies.
Concluding remarks
The classification of SBS/AHT cases is based on a value-impregnated choice of theory, but the values based on child protection teams’ preferences are obscured as if they were based on purely scientific reasoning and are reinforced by increased societal sensitivity to child abuse. Thus, the scientific approach to determination of cases of SBS has been misdirected by ideology, facilitating applied circular reasoning, which results in overestimation of SBS/AHT cases.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: In a recent systematic review of the scientific literature on SBS, commissioned by the Swedish Agency for Health Technology Assessment and Assessment of the Social Services, the authors participated in a group of six experts. 15 We do not consider this governmental and impartial systematic review of the literature to have resulted in conflicts of interest. The aftermath of the review has, however, confirmed that the SBS/AHT issue is highly controversial and emotionally charged, and accordingly we find it appropriate to mention our contribution to the Agency’s assessment.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.