
Abstract
In 2006, CIE published a technical report on an action spectrum for the production of previtamin D3 in human skin. CIE procedure is to publish guidelines (e.g., an action spectrum) and let the community test them before moving to define a standard. The CIE previtamin D3 action spectrum has been in use for 15 years, and challenged on several occasions; a number of alternative action spectra have been suggested. To date (2021) no alternative action spectrum has shown clear advantages over the CIE version when tested against experimental outcomes. Thus, the CIE action spectrum remains widely used, but not fully accepted as best representing the photobiology in human skin leading to synthesis of vitamin D. We report on a CIE workshop designed to address the challenges to the CIE action spectrum, and explore alternative action spectra. The workshop concluded that the CIE action spectrum probably requires amendment, with several candidates for consideration in determining any changes. However, until there is a clear alternative, the CIE action spectrum should remain in use whilst ensuring full spectral information about sources of ultraviolet radiation. Thus, results are comparable between studies and can be recalculated to an updated action spectrum if necessary.
1. Introduction
The CIE action spectrum for the production of previtamin D3 in human skin 1 represents the first step in cutaneous synthesis of vitamin D. Vitamin D is well known for its importance in maintaining a healthy musculoskeletal system, and has also been associated with a range of other health benefits.2,3 The vitamin has two sources, through the diet (including supplements) and from synthesis in the skin after exposure to ultraviolet radiation (UVR). Modern, unsupplemented, diets are often poor in vitamin D, making cutaneous synthesis the major source for many. 4 Vitamin D reaching the circulation, either from the gut or from the skin, is hydroxylated mainly in the liver to 25-hydroxyvitamin D (25(OH)D), the metabolite that is used to measure vitamin D status.
Cutaneous synthesis begins with 7-dehydrocholesterol (7-DHC) in skin cells, predominantly the epidermis. Exposure to UVR, mainly UV-B wavelengths, converts 7-DHC to previtamin D. Previtamin D itself can photoisomerise to several isomers (7-DHC, lumisterol and tachysterol) in reversible photoreactions also driven by slightly different wavebands of UVR. The resulting balance of isomers depends upon the length of irradiation and the spectrum of the irradiating source. In sunlight, the previtamin D becomes limited with prolonged exposure, while lumisterol and tachysterol continue to increase. 5 Once formed, previtamin D then undergoes a relatively rapid membrane enhanced non-enzymatic isomerisation to vitamin D that takes a few hours to complete; vitamin D is then removed to the circulation attached to vitamin D binding protein (DBP). 6
7-DHC in skin is not unprotected. It is found in the cell membrane, and so transmission of the skin becomes important in determining which UV photons reach the molecules of 7-DHC to initiate previtamin D production, and hence what an action spectrum ‘in human skin’ will look like. Transmission of the skin is wavelength dependent and changes with depth, depending on factors such as skin pigmentation and epidermal thickness.7–9 These vary from person to person and also with body site on the same person and may wavelength-shift the action spectrum. Note that the CIE action spectrum is defined for white skin as highly pigmented skin types (brown / black skin) were not used in the original experimental work 10 on which it is based. The impact of melanin on the action spectrum remains to be further explored in ensuring that public health messages are fully inclusive.
The CIE defines an action spectrum (or spectral weighting function) as a ‘function representing the relative spectral effectiveness of optical radiation, for a specified biological effect, in a specified system’. 11 The CIE action spectrum for the production of previtamin D3 in human skin 1 therefore clearly specifies the biological effect and the system. It assumes this first step is the only relevant photoreaction in the major route of vitamin D supply (7-DHC to vitamin D). However, as noted in the CIE publication, this action spectrum strictly only applies to initial doses of UVR, especially when the irradiating source is polychromatic (e.g., the sun). With continuing irradiation after previtamin D3 has formed, other isomers start to appear and the incident UVR is driving more than one reaction. The limiting dose at which other reactions involving previtamin D3 begin to occur depends on the source spectrum and skin type, while the time for such a dose depends on source intensity (continually varying for the sun but can be as short as a few minutes). Thus, we use the terms ‘small doses’ and ‘short irradiations’ to imply only 7-DHC to previtamin D3 reactions are occurring, since we cannot give a single quantity for these terms. Such short, frequent (i.e., daily or near daily) exposures are the most efficient way to improve vitamin D status. The terms ‘prolonged’ or ‘short’ exposure are also relative to the ratio of the exposure time to the timescale in which previtamin D isomerises into vitamin D, which is temperature dependent, but typically takes 2.5 hours. 6 If exposure time is very long, such that vitamin D3 has formed and is also irradiated, then the vitamin D can also be converted to other isomers by slightly longer UV wavelengths. 12 Such reactions can inhibit (or even reverse) further production of vitamin D.
Given that, for small doses and short irradiations, 7-DHC to previtamin D3 is probably the only photoreaction involved, but previtamin D3 is not the final biological endpoint; we must also consider whether an action spectrum should be defined for a different endpoint, for example, vitamin D3 or 25(OH)D3. The latter certainly has the advantage that it is easier to measure in vivo, and is used as the determinant of vitamin D status, but every step away from the original photoreaction brings the possibility of further modifiers in the pathway from radiation to measured response.
The workshop presented our collective views of the CIE action spectrum for previtamin D3 synthesis in human skin, and several potential alternative action spectra for consideration. This paper represents the discussions at the workshop and our joint opinions on the topic.
2. Questions raised about the basis of CIE action spectrum for previtamin D3
The CIE action spectrum for synthesis of previtamin D3 in human skin 1 is based primarily on the only action spectrum measured in human skin, 10 albeit not in vivo but ex vivo, that is, in recently excised viable human skin. The CIE publication discusses the challenges of the original data, including the need to extract the data from a linear plot in the publication, and uncertainties about the detection limits of the equipment used and thus the long wavelength end-point of the action spectrum. The CIE Technical Committee (TC) chose to present the action spectrum on a logarithmic scale and instead of stopping it at 315 nm, ~1.5 orders of magnitude below the peak, to extend it by a further ~ 2.5 orders of magnitude (to wavelength 330 nm). This was achieved by a tangential extrapolation (on the log scale) to the final portion of the measured data. This ‘roll off’ was based on physics arguments, and allowed for limited sensitivity in the original experimental design. It has been much criticised since,13,14 but the TC calculated that with sunlight as the UVR source, the uncertainty in vitamin D effective UVR with and without the roll off was small. However, it is not insignificant, especially in winter, as will be discussed later. The impact for artificial sources of UVR may be greater, dependent on the spectrum of the artificial source.
When compared with the underlying reaction kinetics (the photochemistry of pure 7-DHC, previtamin D3 and its isomers15–20) this action spectrum in human skin is shifted a few nanometres towards longer wavelengths. However, it is expected that the transmission of skin will influence the wavelength dependency of the action spectrum since transmission is known to be wavelength dependent, with longer UV wavelengths penetrating the upper layers of the skin better than shorter wavelengths, for example, 50% transmission is found at a skin depth of 10 µm for a UV-B wavelength of 297 nm, and at 30 µm for a UV-A wavelength of 365 nm. 7 This, in principle, could explain the red-shift, though the original action spectrum 10 on which the CIE spectrum is based was, and remains, the only action spectrum measured in human skin.
The workshop raised two additional queries to the CIE action spectrum, beyond those detailed in the original TC report. The first was to question the bandwidth of the monochromator used in the experimental work. The experimental points are plotted as effectiveness at a single wavelength, but in practice it is difficult to achieve truly monochromatic radiation, and this was more so in the 1980s. This becomes particularly important if the action spectrum is steep, when any stray light in the irradiating spectrum can give misleading results. We learned that the monochromator bandwidth was 3 nm–5 nm, and this must be further assessed for its potential impact on the measured action spectrum.
The second criticism concerns an apparent contradiction. 13 It is often stated that ‘no vitamin D can be made in skin in winter’, at middle to high latitudes, 5 and this is frequently observed as a seasonal cycle in vitamin D status. 21 However, if one convolves the solar spectrum in winter at higher latitudes with the CIE previtamin D3 action spectrum, it is apparent that the potential conversion of 7-DHC to previtamin D3 is not zero (Figure 1). The extrapolation beyond 315 nm in the CIE spectrum may be part of the problem. For the summer and winter spectra from New Zealand in Figure 1, a truncation of the action spectrum to wavelengths less than 315 nm reduces the previtamin D3 weighted UVR by 4.5% and 14.5% respectively. If the CIE action spectrum is shifted to shorter wavelengths as has been suggested (see sections below), the summer/winter contrast would be much larger, which would be more consistent with the observation that little vitamin D is produced in winter at latitudes greater than 40°. However, more work is required before accepting such a revision. Indeed, other spectral shapes may also be plausible, as discussed below.
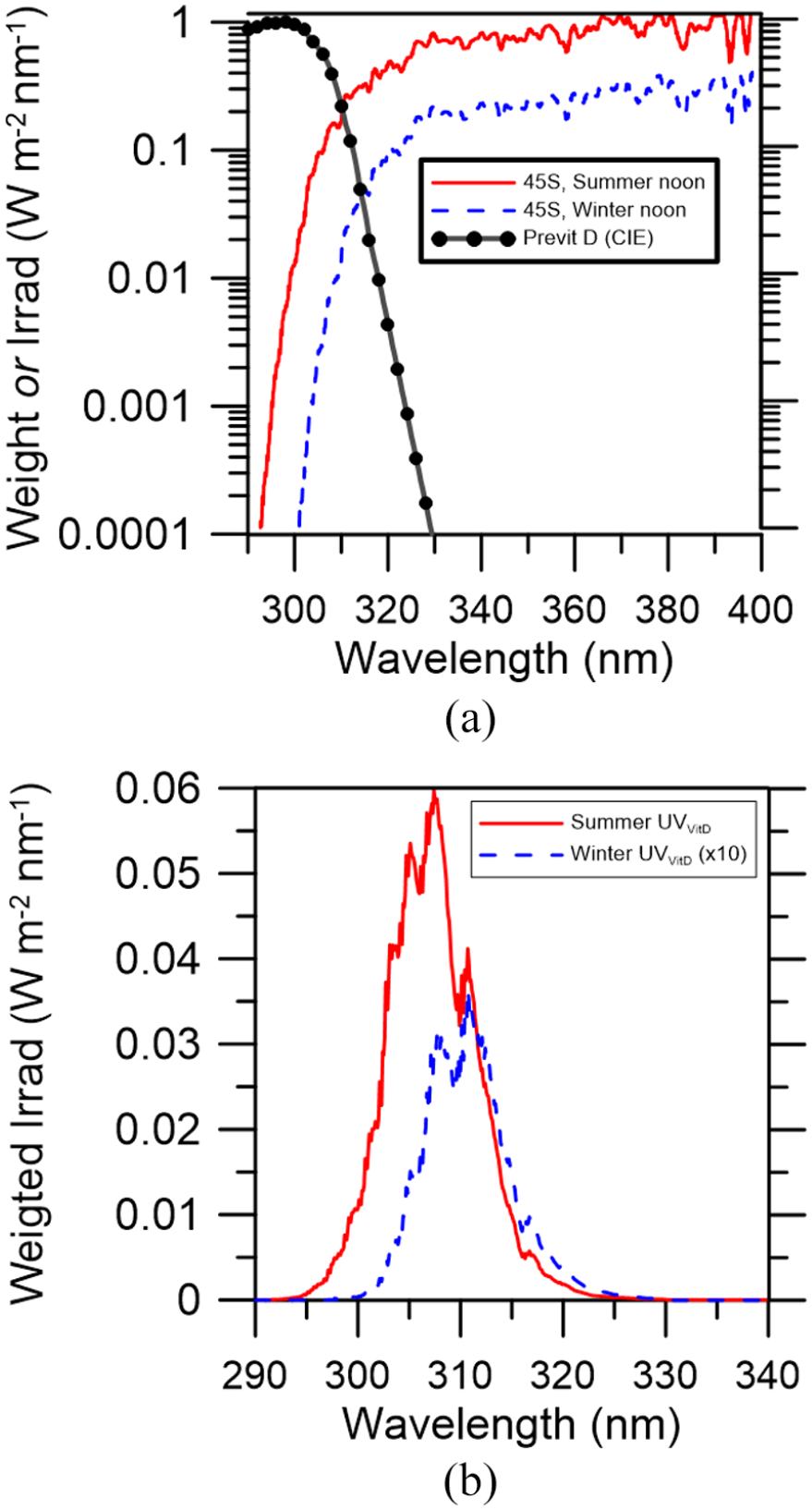
Panel (a) shows typical spectral irradiances for noon near the summer and winter equinoxes at latitude 45°S (Lauder, New Zealand), along with the action spectrum for previtamin D production as defined by the CIE. The curves in panel (b) show the corresponding spectrally weighted irradiances. Note that the curve for winter has been scaled up by a factor of 10 for clarity
This criticism has been taken as an argument that the action spectrum must be wrong, but there are other considerations to be taken into account. The fact that some conversion of 7-DHC could theoretically take place does not mean that a biologically useful amount of conversion can be gained in a practical exposure time in normal conditions, 22 given that it is usually also cold so that skin is covered by clothing, and day lengths are short. This is not a matter of the action spectrum, but rather of misconstrued communication: ‘no vitamin D in winter’ was a convenient if imprecise and generalised shorthand for the previous sentence. The original publication that assessed winter-time conversions at several discrete locations at different latitudes did indicate no conversion in winter at higher latitudes, 5 but the question of sensitivity of the assay used must again be considered. It was agreed that a better statement would be that ‘no biologically relevant amount of vitamin D is made in skin in winter at mid to high latitudes’. This would be a more precise statement even if the current action spectrum were to be amended or replaced.
It was agreed that the original measurements in human skin were state of the art in the 1980s, and there was nothing more recent to work with before the CIE action spectrum was published in 2006. However, it is now 40 years since that original work was completed and technological advances in both irradiation systems and assay systems have improved, as has our understanding of the limitations of older technology. Furthermore, consideration could be given to different biological endpoints in the vitamin D pathway, since they must all begin with the same initial photoconversion, but the downstream products may be more appropriate and/or easier to assess.
3. The QUT action spectrum for vitamin D3
William Olds, then a PhD student at Queensland University of Technology (QUT), developed an in vitro action spectrum for the production of vitamin D3, using a solution of 7-DHC, irradiated with UVR, and then incubated at 37°C to allow for the formation of vitamin D3.23–25 After 24 hours, 7-DHC and vitamin D3 in the solution were measured by High Performance Liquid Chromatography. The outcome was an action spectrum that drops more steeply with wavelength than the CIE spectrum, and is shifted to shorter wavelengths (by about 8 nm at the long wavelength limit). However, the QUT action spectrum was heavily criticised for experimental procedures, foremost of which was the breadth of the cuvette used.26,27 This was found to be too great, such that the solution at the front of the cuvette masked that at the back of the cuvette and there was not uniform irradiation of the 7-DHC. This QUT action spectrum was never published in the peer-reviewed literature. Mathematical solutions to the experimental controversies, correcting for the reported problems with self-absorption, partial irradiation of the cuvette, normalisation of the action spectrum and skin transmission, have been proposed. 28 Although the QUT action spectrum (which does not account for attenuation by the transmission spectrum of the skin) is sometimes referred to as agreeing with/supporting other action spectra, one should use it with caution.
4. The RIVM computational action spectrum
In exploring the CIE action spectrum, Norval et al. 14 asked: ‘Is the action spectrum for the UV-induced production of previtamin D3 in human skin correct?’. They concluded: ‘. . . the construction of an entirely new computational model to predict previtamin D levels is recommended’. This challenge was taken up by Van Dijk et al.28,29 in the Netherlands who published their proposed computational ‘action spectrum’ in 2016.
The computational action spectrum provides for the production of previtamin D3, and accounts for the complex photochemistry involved in prolonged irradiation (see Terenetskaya 20 ), including the photoisomerisation of vitamin D3 on irradiation. It includes absorption cross-sections and quantum yields for all the previtamin D3 isomers and their reversible reactions, and for vitamin D3. It also includes skin transmission, and enables transmission to be altered for different skin types and body sites. It is not therefore a single action spectrum in the traditional sense, but a multi-faceted predictive tool that can in principle remove many of the caveats associated with applying the CIE action spectrum (e.g., limitation to short irradiations). In doing so it can also change the irradiating spectrum to mimic that of the changing solar irradiance received at the Earth’s surface throughout the day. Applying this computational model to the question of the vitamin D winter for the Netherlands shows that the vitamin D winter is 9 days longer in both autumn and spring (18 days in total) than when calculated with the CIE action spectrum. The computed action spectrum for previtamin D3 production is blue-shifted, that is, moved to shorter wavelengths than the CIE action spectrum by an amount between 3 nm and 8 nm.
This work relies on experimental data from a range of sources as inputs, and these are not without uncertainty. The uncertainty in the input data limits the model output. Better spectral measurement data on skin transmissions, quantum yields and absorption spectra of substances involved, as well as of the 7-DHC concentration in skin as a function of depth at different body sites for different skin types, could greatly improve the model. There is also a need to measure the extent to which quantum yield spectra differ for substances that are free in a solution and for substances that are fixed in a matrix in human skin. Antenna effects in the latter situation can introduce huge differences. On the one hand, the momentum of a UV photon that hits a 7-DHC molecule may be swiftly deferred to neighbouring molecules via the bonds with which the 7-DHC molecule is fixed in the skin matrix, thus preventing a ring opening from occurring. Alternatively, the bonds with which a 7-DHC molecule is fixed in the skin matrix may reduce that molecule’s flexibility and thus make it more susceptible to ring-breaching after a hit by a UV photon. Antenna effects are strongly dependent on the wavelength and therefore affect the shape of the action spectra derived from this theoretical model.
Note that a bug in the original code for this model has been identified and corrected since it was originally published. This does not affect the theoretical basis of the model and the qualitative conclusions, but numerical values reported for prolonged exposure have changed by up to some tens of percent. Nonetheless, it remains true that the ultimate validation of this computational action spectrum would require comparison with in vivo data collected in tightly defined conditions of exposure.
The great advantage is that the model can explore different theoretical inputs in a way that could not be done without great expense and time experimentally/clinically. It can address modifiers, for example, skin type (melanin) to provide ‘personalised’ action spectra, but with the proviso that the input data are well known.
5. New tool for the assessment of candidate action spectra for the production of 25(OH)D
Normally, action spectra are derived on the basis of the (relative) response of a given endpoint to monochromatic sources. Mathematically seen, there is no objection to using a series of non-monochromatic sources instead and disentangling the information of the different contributing wavelengths afterwards, assuming, for example, wavelength additivity. Polychromatic responses can be used to validate a candidate action spectrum by determining how well it represents the response to different sources of irradiance. Immediately before the CIE workshop, a new study was published 30 exploring the nature of the action spectrum for the production of 25(OH)D3. In this study, 75 healthy young volunteers underwent full- or partial-body suberythemal irradiation with five different polychromatic UVR spectra every 3 days for five consecutive doses. For all these exposures, in vivo measurements were taken of the concentration of the downstream metabolite of vitamin D that is used to define vitamin D status, that is, circulating 25(OH)D. This new set of measurements can be used to assess candidate action spectra for (pre-) vitamin D3. In such an assessment, the candidate action spectrum is used to simulate the full set of exposures and responses in the new study. Statistical measures for the correspondence between the responses simulated with the candidate action spectrum and the actual responses in the volunteers express the likelihood of the candidate action spectrum being representative for the photoproduction of 25(OH)D3.
In applying the CIE previtamin D3 action spectrum, only one of the polychromatic light sources that were used had a significant weighted irradiance contribution from the wavelengths shorter than 295 nm. We do not expect a future improved action spectrum to be fundamentally different from the current one. Therefore, we conclude that the new tool cannot discriminate between candidate action spectra for wavelengths shorter than 295 nm. This means that the new set of samples (endpoint 25(OH)D3) can only be used to assess the solar part of the UV spectrum (no shorter wavelength UV-C). Additional samples for UV lamps with variation in complementary subranges of wavelengths are required to make the newly developed tool cover a broader wavelength domain. This may be necessary if the method is to be used to estimate the vitamin D production of solaria.
6. Action spectrum for the production of 25(OH)D3
In the classical vitamin D pathway (7-DHC to previtamin D3 to vitamin D3 to 25(OH)D3) there is no reason to assume that an action spectrum for 25(OH)D3 would differ from an action spectrum for previtamin D3, except for a scaling factor that accounts for the efficiency of the conversions to vitamin D3 and to 25(OH)D3. To recap, UVR reaching the skin surface initiates the photoreaction 7-DHC to previtamin D3. This is followed by a heat isomerisation to vitamin D3, transport out of the cell and into the circulation attached to DBP, and a hydroxylation in the liver to 25(OH)D3. If prolonged exposure is avoided (or in other words: for a low dose, as was the case in the clinical trials that were presented) then 7-DHC to previtamin D3 is the only radiation driven step in this pathway.
Young et al. 30 used the above new tool to estimate which shift in wavelength of the original CIE action spectrum for previtamin D3 would best describe the synthesis of 25(OH)D3. They calculated the effect of shifting the CIE action spectrum in multiples of 1 nm to shorter wavelengths. The shifted CIE action spectra have no other conceptual or biological basis than the expectation that they may perform better than the classical CIE action spectrum in the analysis described above. The tool showed that the CIE action spectrum shifted 5 nm to shorter wavelengths performed far better than the original action spectrum by this test, and could then be considered the action spectrum for 25(OH)D3 production.
However, in addition to some of the modifiers already mentioned (e.g., skin type and body site), this 25(OH)D3 action spectrum is subject to additional uncertainties, for example, genetic variations in control of the metabolic pathways to 25(OH)D 31 ; variations in response associated with the starting vitamin D status of individuals. 32 The clinical trial was performed on carefully matched white (skin type I and II) individuals in their twenties with mean starting 25(OH)D3 for each group of between 29 nmol/L and 38 nmol/L. Whether the resulting action spectrum can be applied to other demographics by, for example, a simple scaling, remains to be seen.
7. Public health communications
Spectral accuracy in action spectra matters in providing accurate sun exposure advice to optimise benefits and reduce risks to health. Nonetheless, while accepting that there is a scientific drive to ensure that the ‘vitamin D’ action spectrum is correct for its chosen endpoint, it was noted that consistency of expression is vital in gaining traction with public health messaging. Given the known interpersonal variation in response to a dose of UVR even in controlled conditions, and the vast array of personal characteristics and behaviour of the general population, no single action spectrum is going to represent everyone. An action spectrum can only indicate a ‘typical’ outcome. Within this context there must be a really good reason to change the current action spectrum, especially if it leads to a change in public health messaging. Changing messages lead to confusion, in what is already a complex story of balancing benefit and risk of sun exposure. Therefore, while it is important not to mislead the public, before moving from an action spectrum that is sometimes disputed but widely used, it is important to ensure that any replacement action spectrum is widely accepted and not likely to be further disputed.
8. Discussion
The ‘vitamin D’ action spectra discussed here have a variety of different endpoints and account, or don’t account, for different elements in the UV-skin-circulation pathway between UVR exposure and vitamin D status. The endpoints are previtamin D3,1,28 vitamin D3 25 and 25(OH)D3. 30 Skin transmission is inherent in the experimental data underpinning the action spectra from CIE 1 and Young et al., 30 missing entirely from QUT, 25 and calculated by RIVM. 28 Nonetheless, the human in vivo 30 and ex vivo1,10 studies are based only on white skin, and European genetic types. 30 With the exception of the RIVM computational action spectrum, the others are simple relationships between wavelength and response. In their application it is accepted that they have to be adjusted to account for any skin transmission 25 or to account for other than white skin.1,30 At present any such scaling tends to be a simple multiplier, based on clinical data (e.g., Farrar et al. 33 as applied in Webb et al. 34 ), or it might conceivably be based on the erythema response to UVR exposure in different skin types. Figure 2 shows the proposed new action spectrum for 25(OH)D3, the CIE action spectrum for previtamin D3 and the calculated RIVM action spectrum for previtamin D3 synthesis in skin of the lower back.
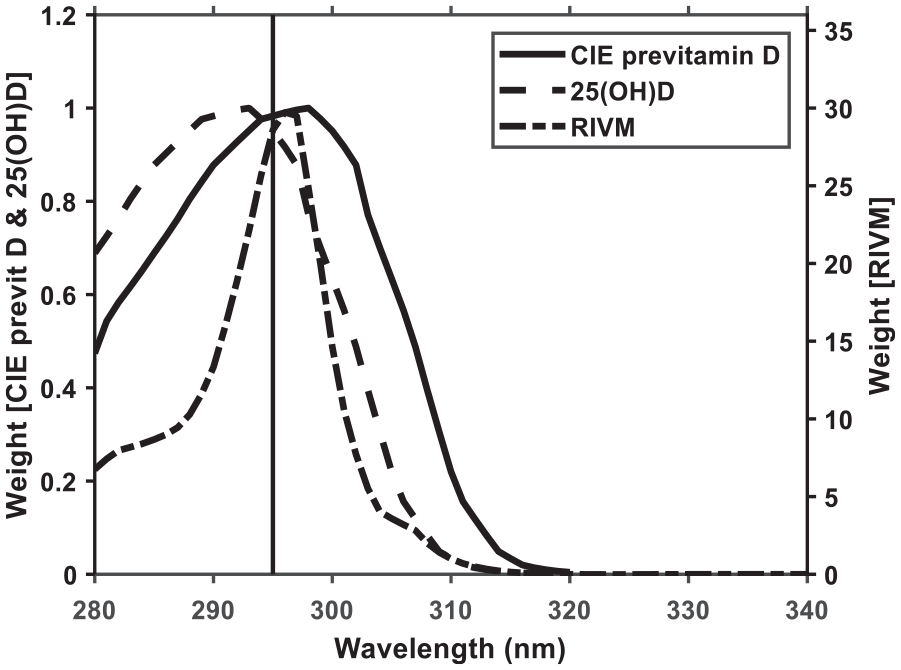
Vitamin D related action spectra: the CIE action spectrum for previtamin D3 synthesis in human skin (solid line), proposed action spectrum for production of 25(OH)D in humans (dashed line) and modelled action spectrum for previtamin D3 synthesis in lower back skin (dash-dot line). The vertical line at 295 nm marks the approximate limit of solar radiation
Prior to selecting a final ‘vitamin D’ action spectrum to use as a standard, the photobiology/public health/endocrine community must determine the preferred endpoint and level of adaptability required of the action spectrum. Should it be a single line action spectrum with simple multiplier scalings, a matrix of scalings for a basic single line action spectrum (e.g., to account for wavelength dependent skin transmission) or an almost personalised computational action spectrum with variable inputs? The former two are relatively straightforward, easily understood and with clearly defined scaling act as a standard. Almost by definition they represent an average or typical response and are best applied at a population level. The latter is an adaptable tool that in principle could be applied at an individual level (sufficient inputs being available). However, because of its adaptability it could not act as a standard unless the inputs are set at pre-determined (standard) values for this purpose.
9. Conclusion
The workshop concluded that the CIE action spectrum probably does need to be amended, and there are several suggested candidates with which to work in determining any changes.
However, until that work is completed and there is a clear alternative, we should continue to use the existing CIE action spectrum whilst also ensuring full spectral information about sources of UVR is provided. In that way results are comparable between studies and can be recalculated to an updated action spectrum for a different vitamin D endpoint if necessary, in future. Meanwhile, the tool recently presented by Young et al. 30 could be used to assess candidates other than the shifted CIE action spectra for their ability to represent the vitamin D outcome of irradiating (white) skin with UVR.
Footnotes
Acknowledgements
This work was the focus of a workshop delivered at the CIE 2021 Midterm Session.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.