
Abstract
Evening exposure to electric light can acutely suppress melatonin levels and adversely affect subsequent sleep. We conducted a systematic review with meta-analysis investigating the influence of evening illuminance levels on polysomnographically (PSG)-assessed sleep. We also explored how melanopsin (expressed in melanopic equivalent daylight illuminance (EDI) affects human sleep features. We included polysomnographic laboratory sleep studies with healthy humans for effects of illuminance and exposure duration, for pre-sleep exposures between 6:00 p.m. to 1:00 a.m. From 440 identified articles, 114 met eligibility criteria for screening, and 21 also reported type of light source/spectral characteristics, with 12 identified as eligible for review. Meta-analysis showed evening light affects sleep latency, sleep efficiency and slow wave sleep, with overall effect sizes (95% confidence interval) of 0.69 (−0.50; 1.88), 0.34 (−0.13; 0.82) and −0.61 (−1.85; 0.62), respectively. Estimated melanopic EDI in the range of 100–1000 lx yielded clear dose–response relationships for sleep latency and sleep efficiency, but not for slow wave sleep. Whilst illuminance and duration indicated no apparent effects for a single evening light exposure on PSG-assessed sleep latency, sleep efficiency and slow wave sleep, we observed evidence for a relationship between light exposure and sleep effects based on melanopic EDI. Hence, melanopic EDI may provide a robust predictor of non-visual responses on human sleep.
1. Introduction
With the advent of electric lighting and the use of self-luminous devices, light has also found its way into our bedrooms. This has allowed for different pre-sleep activities (e.g., reading in bed) by forcing away darkness and lengthening the day. 1 Importantly, light maximally shifts human circadian melatonin and core body temperature rhythms around dawn and dusk. 2,3 Thus, special attention in the use of artificial light needs to be taken in the evening after sunset when countless people switch to electric light prior bedtime. In fact, current recommendations for healthy evening indoor light exposure in residential areas endorse maximum light levels of 10 lx as the melanopic equivalent daylight illuminance (melanopic EDI) at least 3 hours before bedtime. 4 Melanopic EDI represents the metric for predicting a circadian impact of environmental illumination on melatonin suppression. 5 Although the recommended evening photopic illuminance in 4 is rather low and corresponds to ∼25 lx for a fluorescent light source with 3000 K, it represents a good trade-off between the visual and non-visual comfort zone of light in healthy adults only minimally affecting melatonin secretion but still allowing usual evening activities (e.g., watching TV) at home. According to a recent study by Cain et al., 2020, 6 the average “melanopic illuminance” 3 hours prior bedtime was about “20 melanopic lux”, corresponding to 18 lx (melanopic EDI) for LED and fluorescent light.
Non-visual effects of light comprise many physiological and neuropsychological measures in humans ranging from circadian gene expression to subjective perception of alertness and mood (for reviews, see 7,8 ). Another photoreceptor system besides rods and cones forms a key element in transmitting the non-visual action of light to the brain, namely the intrinsically photosensitive retinal ganglion cells (ipRGCs) containing the photopigment melanopsin. 9,10 Animal work shows that ipRGCs yield a strong afferent input to the central circadian pacemaker in the suprachiasmatic nuclei (SCN), but also project to the olivary pretectal nucleus (OPN) mediating pupillary light responses and the ventrolateral preoptic nucleus (VLPO), which plays an important role in regulating sleep. 11 Thus, via ipRGCs, light influences behaviours essential for our health and quality of life, such as sleep, but are mostly independent of image formation. 12 Recent recommendations for light exposure are based on data from 18 laboratory studies using both monochromatic and/or polychromatic light sources, which reported non-visual light responses for circadian phase shifting of melatonin or core body temperature rhythms, increased subjective perception of alertness, and acute melatonin suppression. 13 Results from different studies showed that these three non-visual effects of light can be best-predicted by a melanopic irradiance-response model. 13–16 However, it remains unresolved whether other non-visual effects of light, particularly its repercussions on sleep, can be modelled similarly. So far, studies on non-visual effects of light focusing on sleep reported mixed results, particularly PSG-assessed sleep outcomes such as sleep latency, sleep efficiency and slow wave sleep (for a review, see 17 ). Furthermore, light’s effects on human sleep hallmarks has not yet been quantified by the use of recent CIE metrics 5 for ipRGC-driven light responses.
Thus, here we focused on light’s effects on human sleep, more specifically the ramifications of evening light exposure on the following night-time sleep episode. For this purpose, we conducted a systematic review to investigate the impact of different illuminance levels in the evening on PSG-assessed sleep of healthy participants in controlled laboratory studies. Based on previously reported light-driven effects on sleep architecture (for reviews, see 18,19 ), we selected the following PSG-derived sleep measures for our analyses: sleep latency, sleep efficiency (i.e., percentage of time asleep during time in bed) and slow wave sleep (i.e., deep sleep, stages 3 and 4 or N3). Firstly, we performed a meta-analysis to test the prediction that pre-sleep light exposure acutely lengthens sleep latency, reduces sleep efficiency and reduces time spent in slow wave sleep. Secondly, we tested the prediction that pre-sleep light exposure affects those three sleep measures in a dose-dependent manner. Thirdly, as an exploratory analysis, we investigated whether the effects of pre-sleep light exposure on sleep latency, sleep efficiency and slow wave sleep depend on the dosing of melanopic EDI, as is currently reported for increased subjective alertness, circadian phase shifting and melatonin suppression. 13
2. Methods
This systematic review was conducted in accordance to Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA). 20 Eligibility criteria were that (1) the studies included humans, (2) sleep was assessed polysomnographically in a laboratory setting, (3) illuminance levels and duration of light exposure were reported, (4) the type of light source and/or spectral characteristics were indicated, and (5) the active light and control light exposure occurred in the evening during the time interval from 6:00 p.m. to 1:00 a.m. prior to night-time sleep and lasted at least 30 minutes. There were no restrictions regarding study design, prior light history, participants’ sex or age. Letters to the editor, conference abstracts and literature reviews were excluded.
2.1 Search and study selection
The search was performed on 22 January 2021 in the databases PubMed® and Web of Science. The search string included the following items: ((Light title OR Lighting title) AND Sleep title) AND human MeSH (Medical Subject Headings)). After removing duplicates, the search yielded 440 articles, which were screened by C.C. for exclusion of studies in clinical settings with patients (69) and studies without PSG measures (247), resulting in 114 remaining studies that were assessed for eligibility by four independent reviewers (C.C., I.S., S.L.C. and O.S.). All reviewers screened titles, abstracts and full texts, in that order, for inclusion/exclusion. Results from these four independent screenings were compared, and disagreements were resolved by mutual consensus, and finally resulted in 21 studies to be included for further analyses.
2.2 Data collection process and data items
Description of the included studies and subgroups
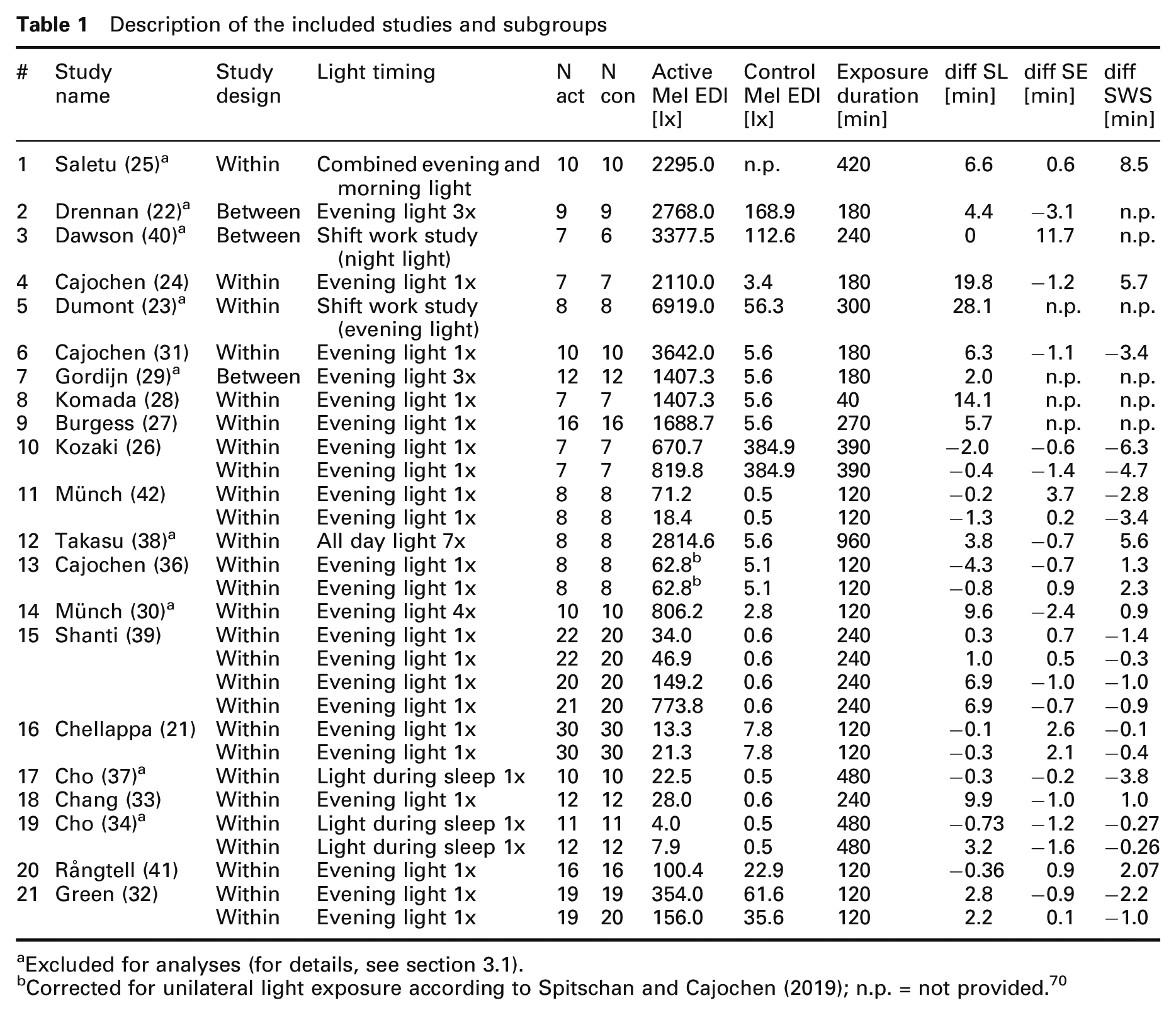
aExcluded for analyses (for details, see section 3.1).
bCorrected for unilateral light exposure according to Spitschan and Cajochen (2019); n.p. = not provided. 70
2.3 Statistics
Forest plots were used to illustrate and compare weighted mean differences (WMD) across studies. The WMD is the average value after pooling results of individual studies. The contribution of each study to the mean difference is weighted by its sample size. Heterogeneity among studies was estimated by the Cochran Q test and quantified by the I2 statistic. 46 The Doi plot and the LFK index were used as graphical and quantitative method for detecting bias in meta-analysis according to Furuya-Kanamori et al. 47 . The graphical outputs and the statistics were performed by MetaXL 5.3 (Epigear International), which is an add-in for meta-analysis in Microsoft Excel. Dose–response relationships between melanopic EDI and the sleep measures were performed by SigmaPlot (Ver.11, SystatSoftware, Inc) via its dynamic fit wizard function. The best model fits were chosen based on the best r 2 value.
3. Results
3.1 Study selection and characteristics
Figure 1 illustrates the study selection procedure according to PRISMA. From 964 records, excluding duplicates, there were 440 identified articles, 114 articles were eligible as they met criteria 1 to 3 of our study selection. Of those, only 21 articles met the fourth criterion of our study selection and are listed in Table 1. Of the 21 studies, nine were excluded due to the following reasons: Saletu et al.
25
used a combined morning and evening light treatment for their active light condition; Drennan et al.
22
used a shift work paradigm applying bright light during three consecutive evenings; Dawson et al.
40
used light at night from 0:00 a.m. to 8:00 a.m. during a simulated night shift; Dumont et al.
23
applied bright light on three consecutive evenings; Gordijn et al.
29
also used multiple evening light exposures (three times); Takasu et al.
38
exposed their volunteers to bright light from 8:00 a.m. to 0:00 a.m. for 7 days; Münch et al.
30
applied evening light treatment on four consecutive nights; and in the studies of Cho et al.
34,37
volunteers were exposed to light during their night-time sleep episode while asleep. Although some of these nine studies provided results supporting our initial hypotheses (see Table 1), they did not intend to measure acute effects of evening light exposure on subsequent sleep, but rather secondary light effects on sleep most likely due to changes in the circadian timing system. In fact, most of these studies reported significant changes in either circadian phase of core body temperature or melatonin rhythms, along with the observed sleep changes. PRISMA flow diagram of the literature screening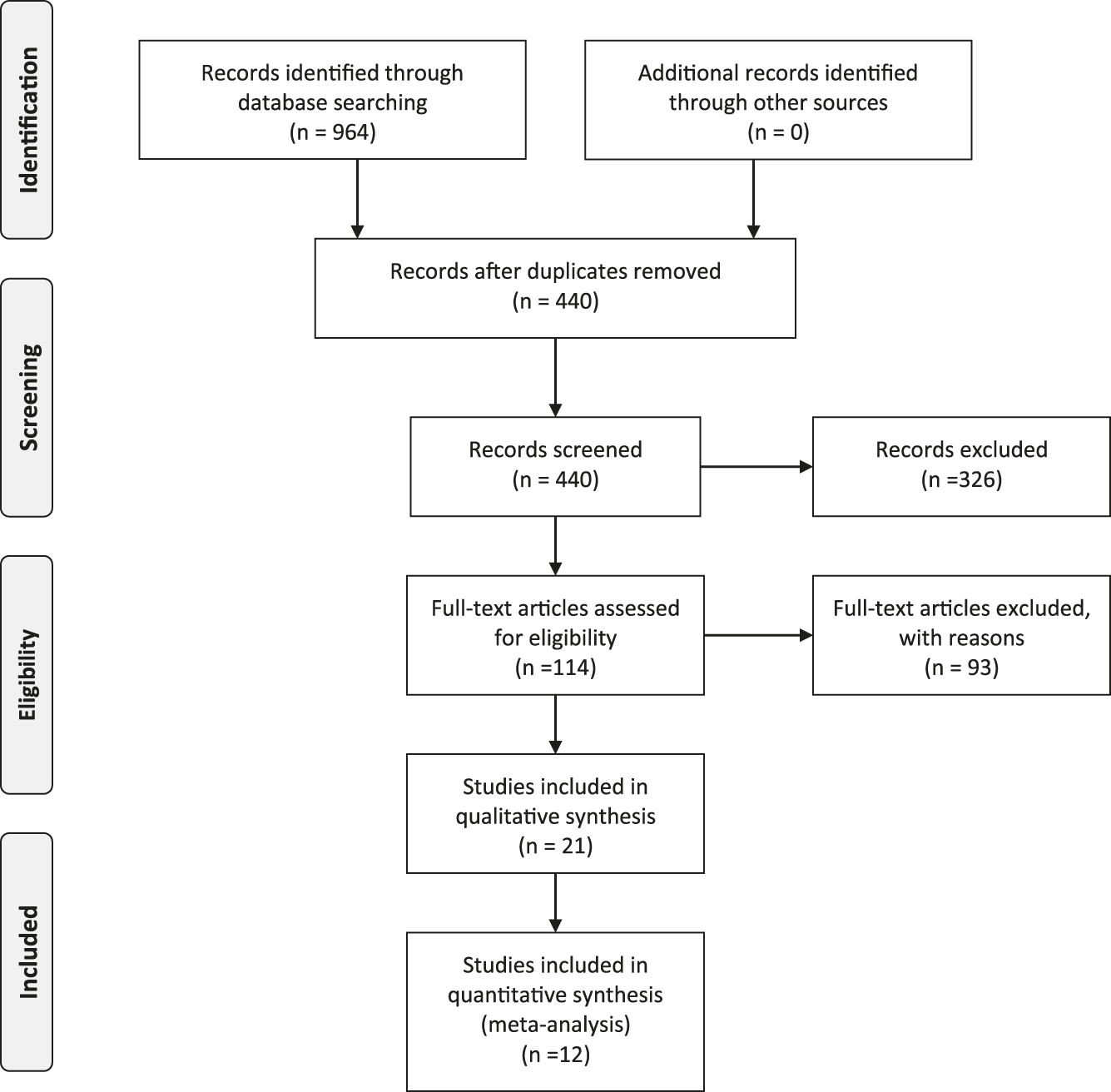
The remaining 12 studies investigated the acute effects of a single evening light exposure on PSG-assessed sleep structure and reported results for sleep latency (12 studies), sleep efficiency (10 studies) and slow wave sleep (10 studies). As such, these articles were deemed eligible for inclusion in the meta-analysis.
3.2 Studies with quantitative analyses
Twelve studies entered quantitative analyses, with six studies providing more than two evening light conditions. The studies entered the meta-analysis irrespective of reporting alpha-opic illuminances and the type of study design, yet, the resulting studies coincidently all used a within-subject design. Overall, 20 different evening lighting conditions entered the meta- and dose–response analyses (see Table 1). Figure 2 panels a–c show the results of the meta-analyses for the three sleep measures: sleep latency, sleep efficiency and slow wave sleep, respectively. The results for total sleep time are provided in Supplemental Figure S1. (a)–(c) Forest plots for the weighted mean difference (WMD) and 95% confidence intervals (CI) for (a) sleep latency (min), (b) sleep efficiency (%) and (c) slow wave sleep (min or % of total sleep time). Positive effect sizes indicate longer sleep latencies, higher sleep efficiency and more time spent in slow wave sleep after the active light in comparison with a control evening light condition, whereas negative effect sizes indicate the reverse.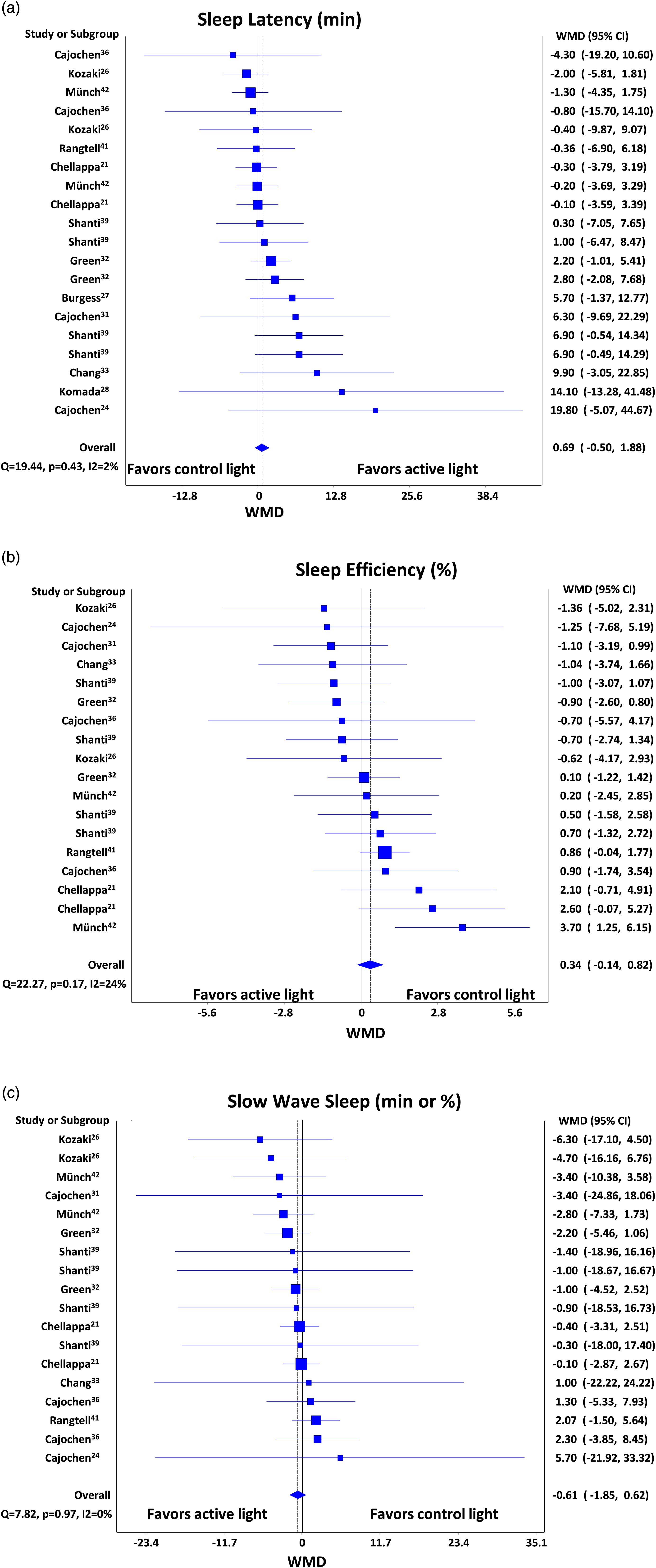
3.3 Effects of pre-sleep evening light on sleep latency
Out of the 20 data points (i.e., 20 different evening lighting conditions used in the 12 selected studies) included in the meta-analysis for sleep latency (see Figure 2(a)), 10 showed null or negative differences between the active and control light groups, while the other 10 showed positive differences (longer sleep latencies) after the active light condition resulting in a mean difference of +4.5 min (SEM: 7.5 min). The effect size for sleep latency was 0.69 (95% CI: −0.5; 1.88).
3.4 Effects of pre-sleep evening light on sleep efficiency
Out of the 18 data points (i.e., 18 different evening lighting conditions used in the 12 selected studies) included in the meta-analysis for sleep efficiency (see Figure 2(b)), nine showed negative differences between the active and control light groups (i.e., reduced sleep efficiency after active light), while nine showed positive differences after the active light condition resulting in a mean difference of +0.17% (SEM: 1.4%). The effect size for total sleep efficiency was 0.34 (95% CI: −0.14; 0.82).
3.5 Effects of pre-sleep evening light on slow wave sleep
Out of the 18 data points (i.e., 18 different evening lighting conditions used in the 12 selected studies) included in the meta-analysis for slow wave sleep (see Figure 2(c)), 13 showed negative differences between the active and control light groups (i.e., less slow wave sleep after active light), while five had positive differences after the active light condition resulting in a mean difference of −1.2 min (SEM: 6.4 min). The effect size for total sleep time was −0.61 (95% CI: −1.85; 0.62).
3.6 Between-study heterogeneity and potential bias
The between-study heterogeneity quantified by the I2 statistic resulted in I2 values of 2% for sleep latency, 16% for sleep efficiency and 0% for slow wave sleep, respectively. Our values indicated a low between-study heterogeneity according to Higgins et al.,
48
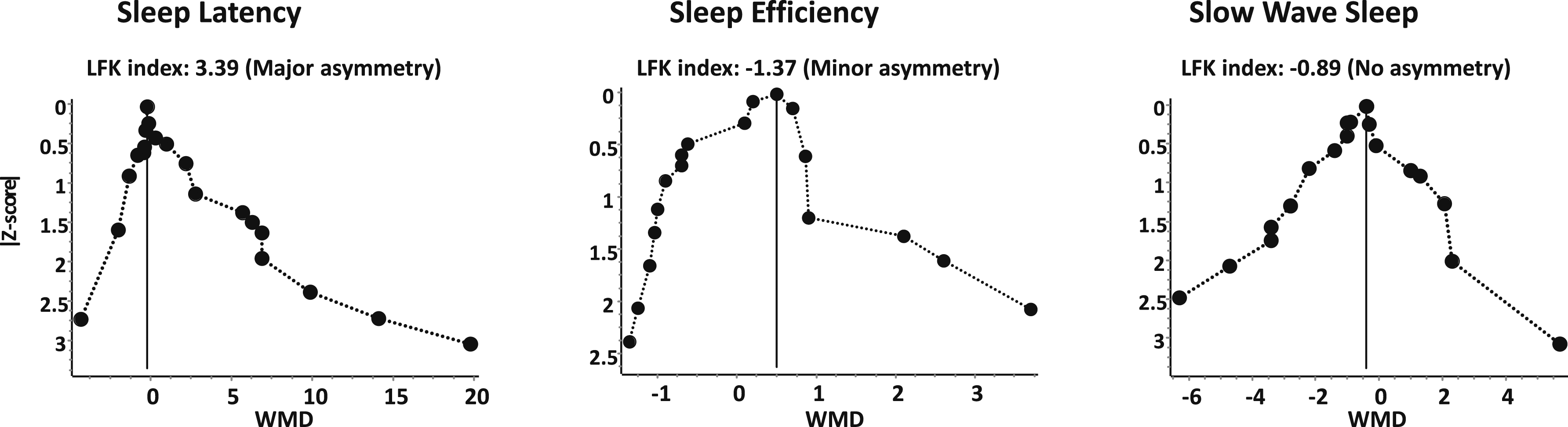
who assigned low, moderate and high heterogeneity to I2 values of 25%, 50% and 75%. Potential bias according to the Doi plots and LFK values are illustrated in Figure 3. These plots indicated a major asymmetry for sleep latency, a minor asymmetry for sleep efficiency and no asymmetry for slow wave sleep. Doi plots for sleep latency, sleep efficiency and slow wave sleep. These plots visualise asymmetry and provide the Luis Furuya-Kanamori (LFK) index, to detect and quantify asymmetry of study effects in Doi plots. The closer the value of the LFK index to zero, the more symmetrical the Doi plot. The Doi plot is a folded variant of the normal quantile v effect plot. The studies form the limbs of this funnel. For more details see
47
3.7 Melanopic EDI as predictor of non-visual responses on sleep
Grouping the data for sleep latency according to the melanopic EDI resulted in a dose–response relationship, which could best be modelled with an exponential growth function: (a) Dose-response relationship between melanopic equivalent daylight illuminance (melanopic EDI, lx) and sleep latency (min), by study and subgroups. The data were modelled according to: 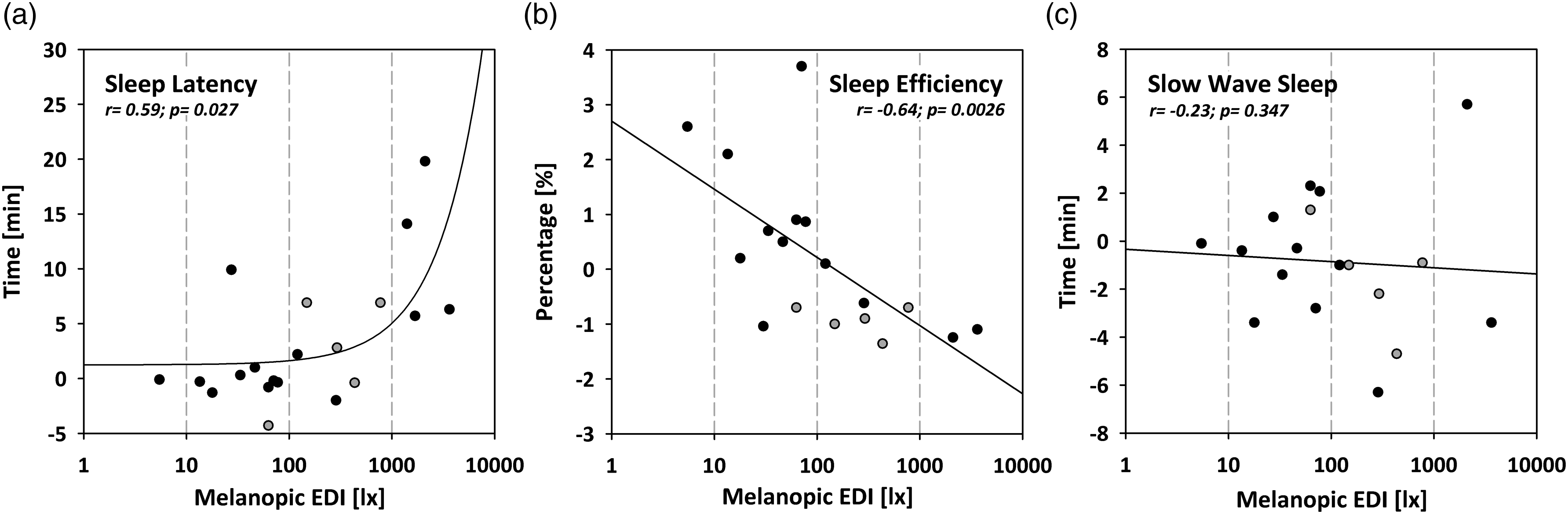
4. Discussion
4.1 Summary of findings
Our meta-analysis indicates no clear evidence that a single evening light exposure alters PSG-assessed sleep. The medium effect sizes of 0.69 and −0.61 for sleep latency and slow wave sleep, respectively, along with the fact that the overall 95% confidence intervals only slightly touched or passed the zero (i.e. the no effect line), suggest that a single evening light exposure might lead to a longer time to fall asleep and to a reduction in deep sleep. Importantly, we show that melanopic EDI, the best available metric to predict melatonin suppression, is a robust predictor of the effects of evening pre-sleep light on sleep, as indexed by its dose-dependent effects on night-time sleep measures. Based on the I2 values, we do not have evidence for robust differences underlying the results of the studies included in our meta-analysis (heterogeneity). 48 In contrast, publication bias 47 may have played a role, as indicated by the large asymmetry (LFK value of 3.3) for sleep latency.
When grouping the data according to the different evening lighting conditions used in the 12 selected studies by melanopic EDI (as in 5 ), we found significant dose–response relationships for melanopic EDI and sleep latency, sleep efficiency, but not for slow wave sleep. These dose–response relationships remained the same when accounting for light exposure duration, expressing the melanopic EDI light dose (in lx min). As such, it is unlikely that differences in light exposure duration within each study mask our reported dose–response relationships between melanopic EDI (in lx) and sleep structure. In contrast to Prayag et al. (2019) 14 and Brown (2020), 13 who successfully model dose-relationships for melanopic EDI and melatonin suppression in the evening using a four-parameter logistic model, our data could best be fit with an exponential growth curve for sleep latency or with linear regressions for sleep efficiency and total sleep time. Thus, our dose-relationships for the sleep response to melanopic EDI point to both exponential and linear models depending on the sleep outcome. The exponential model for sleep latency is likely based on the non-normally distributed data for sleep latency. In other words, good sleepers either fall asleep within 10 minutes or go beyond this time interval with a non-linear (exponential) increase. Brighter lighting conditions in the evening may favour the latter. The reason for the discrepant models describing light’s dose-dependent suppression of melatonin and our observed sleep effects may be due to differences in temporal acuteness. The light impact emerged at evening melanopic EDI levels close to 1000 lx for sleep latency, and close to 100 lx for sleep efficiency and total sleep time. The latter corresponds to the half-max response model for melanopic EDI and melatonin suppression reported earlier. 13,14
A plethora of reasons may explain different characteristics of light’s dose-relationships on melatonin suppression and PSG-derived measures. First, the timing in melatonin suppression and sleep study protocols is different. Melatonin suppression is measured during acute light exposure. At the same time, sleep usually follows 1–2 hours after the end of the light exposure treatment and encompasses sleep measures taken during the entire 8-hour sleep episode thereafter. We excluded studies in which sleep was measured more than 24 hours after the last evening light exposure. 29,30 Assessments of sleep variables more than 24 hours after the last light exposure, as well as after multiple evenings with light exposure treatments, rather appraise indirect effects of light on sleep mediated by changes in the circadian timing system. 31 Evening light can phase delays human circadian melatonin and core body temperature rhythms, 2,3 leading to a shorter phase angle between the dim light melatonin onset (DLMO) and preferred usual bedtime, thereby exacerbating the adverse effects on sleep as reported in the following studies. 22,23,29,30 Of note, applying light while asleep (i.e., during the entire 8-hour sleep episode) has been shown to reduce slow wave sleep. 34,37 However, such light exposure is likely less frequent in daily life and is against the recommended maximal ambient melanopic EDI of 1 lx measured at the eye during night-time in residential areas. 4
Second, brain structures underlying sleep regulation differ from brain circuits controlling melatonin secretion in mammals, including humans (for a review, see Cajochen et al. 7 ). Although, it is certain that light is the main synchroniser of circadian rhythms by setting the circadian phase of neuronal activity in the central pacemaker in the suprachiasmatic nuclei (SCN) in mammals, 49 extra SCN pathways are crucial for the impact of light on sleep. 50,51 This is because the most important photoreceptors for light’s non-visual effects, the intrinsically photosensitive ganglion cells, develop different subtypes, which form a complex system targeting different brain regions responsible for eliciting different behaviours including the sleep-wake behaviour. 52–54
A third reason for the difference between fitting melatonin and sleep measure data in response to light could simply lie in the characteristics of the data distribution and its variability. Both measures, melatonin suppression by light and PSG-assessed sleep ability, show high inter-individual differences. 55,56 For sleep studies, volunteers are usually screened for a good night sleep in the lab before study inclusion. In contrast, individuals are never screened for their ability to suppress melatonin by light prior to study inclusion. Thus, in controlled laboratory sleep studies, a selection bias in recruiting only good sleepers increase homogeneity in the sleep measures compared with studies only measuring melatonin suppression without any melatonin-related inclusion criteria. In all studies included in our meta-analysis, volunteers were screened for good sleep, and all underwent a within-subject design (i.e., each volunteer was its own control). Still, the confidence intervals of the included endpoints varied considerably among studies (see Figure 2). Thus, it is unclear whether sleep measures such as sleep latency, sleep efficiency and slow wave sleep or melatonin measures show higher individual differences. This may be important to clarify, since it has recently been reported that individual differences in light sensitivity (i.e., indexed by melatonin suppression) affect sleep and circadian rhythms. 56
4.2 Strengths
A key strength of this systematic review is that we only included laboratory studies using PSG-assessed sleep, which (despite limited real-life suitability) is still the current gold standard in human sleep research and sleep medicine. 57 Subjective (e.g., questionnaires) and objective (e.g., PSG) sleep measurements display huge discrepancies, particularly for symptoms of disturbed sleep (e.g., sleep latency and number of awakenings). Many studies report disrupted subjective sleep quality with mixed and/or inconclusive results for objective sleep. 58–60 Our systematic review focused on objectively assessed sleep characteristics (i.e. sleep latency, sleep efficiency, total sleep time and slow wave sleep), which were standardised according to previous work. 44,61 . Hence, we minimised a potential source of heterogeneity regarding the effects of subjective/objective sleep characteristics.
All studies reported at least the timing and duration of light exposure in the evening. All studies reported quantitative light measurements at least photopic illuminance (in lx), some correlated colour temperature, and most of the studies indicated the lamp type used (see Supplemental Table). This is particularly relevant, as many studies often do not report these minimum requirements of light specifications. 62 Furthermore, all studies included in the analysis applied a within-study design, some with multiple evening light conditions. While continuous outcomes from within- and parallel studies can be included in meta-analyses using weighted mean difference and the standardised weighted mean difference, the relative weight of the crossover design is larger in combined-design meta-analysis. 63 Thus, comparisons of relative intensities of light within the same study designs (here, within-subject designs) were possible in our analysis. This aspect was lacking in a former review on the effects of light on sleep in community-dwelling adults, and thus a dose–response rate of the light amount in relation to sleep was not possible. 17 Of note, while the control light condition within each study was oftentimes dim (i.e., melanopic EDI < 8 lx), in some studies the control condition did not represent an actual dim light control. Due to the relatively low number of studies, we could not perform additional analyses controlling for this potential covariate of interest. Hence, the dose–response relationships might be affected by this potential source of differences. This highlights the need for future research involving non-visual light effects on sleep to carefully select actual dim light conditions to enable appropriate comparisons with active light conditions.
4.3 Limitations
We included only controlled laboratory studies with healthy good sleepers. While this is a first step to establish whether light per se affects sleep, the translational relevance to sleep disturbances, particularly insomnia disorder, is limited. There is growing interest in using wearable devices to monitor sleep (e.g., wrist-worn actigraphs). While wearable devices like actigraphs are overall a useful and valid means for estimating e.g., total sleep time and wakefulness after sleep onset in field and workplace studies, there are limitations regarding the specificity with other markers including sleep efficiency. 64 Another major drawback is that only a few studies provided light spectra, which does not conform to the current recommendations on how to report light exposure in human chronobiology and sleep research experiments. 5,62 Moving forward, adherence to the minimum reporting guidelines will be needed for specifying light exposure and stimulus conditions in sleep research to enable meta-analyses of light data. 5,62
4.4 Future directions
Future work is needed to include cumulative light exposure from the natural environment and electrical light during office hours across days to investigate how prior light history affects human sleep. 65 This is of importance since daytime and early-evening exposure to bright light can mitigate some of the sleep-disruptive consequences of light exposure in the later evening. 66 Recently, healthy individuals exposed to evening/night blue-depleted light (melanopic EDI range: 6–19 lx) had increased total sleep time and REM duration, as compared to a standard lighting (melanopic EDI range: 27–63 lx) in a hospital setting. 67 These findings highlight the translational relevance of designing buildings or hospital units, taking into account optimal evening and night-time light settings. Furthermore, one should account for individual differences in both melatonin suppression and sleep structure changes in response to light. Accordingly, individuals with high light sensitivity may exhibit worse sleep quality after evening/night light exposure than those with low light sensitivity. 56 Future work is also needed to include potential effects of the light source size (e.g., smartphone vs. an evenly lit room). This is of ecological relevance, since many people, including adolescents, spend long durations in front of a small light emitting device, which is often the only light source in a dark room prior to sleep. 68 Lastly, homeostatic sleep measures, including slow wave activity, should be assessed and reported in future sleep studies, since there is emerging evidence that environmental light also affects homeostatic sleep-wake regulation in humans 69 and has been repeatedly shown to be reduced in the first NREM-REM sleep cycle after evening light exposure. 21,24,42
5. Conclusion
Using photopic measures alone, our meta-analysis indicates no apparent effects for a single evening light exposure on PSG-assessed sleep latency, sleep efficiency and slow wave sleep. Of translational relevance to the light field, we show that melanopic EDI, which is currently the best metric to predict hallmarks of circadian photosensitivity (e.g., melatonin suppression) is an accurate predictor of the effects of evening pre-sleep illumination levels on hallmarks of sleep physiology. The latter was assessed here as the impact of evening on pre-sleep illumination levels on PSG-derived sleep measures in a dose-dependent manner. Collectively, melanopic EDI is likely to be a relevant predictor of non-visual responses on PSG-assessed human sleep under laboratory conditions. Ultimately, our findings have ramifications for future light recommendations in residential areas and concepts of light hygiene in sleep medicine.
Supplemental Material
sj-pdf-1-lrt-10.1177_14771535221078765 – Supplemental Material for Influence of evening light exposure on polysomnographically assessed night-time sleep: A systematic review with meta-analysis
Supplemental Material, sj-pdf-1-lrt-10.1177_14771535221078765 for Influence of evening light exposure on polysomnographically assessed night-time sleep: A systematic review with meta-analysis by C Cajochen, O Stefani, I Schöllhorn, D Lang and SL Chellappa in Lighting Research & Technology
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.