
Abstract
Typical home lighting practice is mainly centred on visual aspects to enable safe movement between spaces, flexibility in multiuse spaces, a sense of aesthetics and energy efficiency. Whilst lighting impacts on the health of residents have not received similar consideration, this area is gaining increasing interest. This is even more important and actual in the context of the recent pandemic where people have been working or studying from home. A combination of bright daytime light and night-time darkness is essential for circadian entrainment and maintenance of a regular daily sleep–wake cycle, whereas exposure to light at night can negatively impact circadian rhythms and sleep patterns and ultimately lead to potential health problems. Additionally, lighting also has the potential to affect health through associated effects such as flicker, glare, optical hazards or electromagnetic fields. This article discusses the main areas of concern related to home lighting and outlines general recommendations to limit detrimental effects and contribute to good health.
1. Introduction
Current lighting practice is mostly dominated by a focus on visual aspects. This is understandable since the main function of lighting is to support visual performance and comfort through provision of adequate visual conditions for human activities to be carried out safely, accurately, quickly and comfortably. 1 In addition, in a variety of sectors, such as lighting for homes, there are also aesthetical needs for enhancing the appearance of spaces, people and objects.
Importantly, alongside visual and perceptual aspects, light can also have non-visual effects on human physiology. 2 – 4 These have been associated with impacts on health, 5 which is defined by the World Health Organization as ‘a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity’. 6 Light acts as the key driver affecting human circadian rhythms, and thus regulates the cycle of waking and sleep and various bodily functions and behaviours such as immune responses and appetite. 5 A combination of bright daytime light and night-time darkness is essential for circadian entrainment and maintenance of a regular daily sleep–wake cycle, whereas exposure to light at night can negatively impact circadian rhythms and sleep patterns and ultimately lead to potential health problems. Furthermore, light can also have acute non-visual effects on alertness, attention and mood. 2 – 4
Outdoor natural light has provided the entraining mechanism for human physiology over hundreds of millennia of evolution. It is relatively recently in the evolution timeline, mostly over the last century or so, that the arrival of artificial lighting and advances in lighting technologies have contributed to a gradual shift in human activities and behaviour making the current generations spend most of their time in an indoor environment. However, most indoor environments provide reduced exposure to daylight compared to the outdoors, and not only is the electric lighting used therein still unable to match the varying amount and spectral characteristics of daylight but it also allows for exposure to light even in the hours of natural darkness. In addition to circadian impacts, light also has the potential to affect health through associated aspects such as visual effects (flicker and glare), optical hazards or electromagnetic fields.
The home environment receives natural light through daylight openings which may be supplemented by electric lighting as needed throughout the day. Electric lighting then continues into the evening or night and may even resume before dawn the following day. Typical residential lighting design is centred upon enabling safe movement from one space to another, flexibility in multiuse spaces such as combined kitchens and dining or living rooms, a sense of aesthetics, as well as energy efficiency. Although less attention has been paid to how lighting can affect the health of residents, an increasing interest in this area can be noted. This has become even more actual and important these days in the context of the recent pandemic where large populations have started to work or study mostly from home. In response to this, this paper discusses the main potential impacts of home lighting on residents’ health and outlines general recommendations to limit detrimental effects and contribute to good health.
Main characteristics of home lighting
Most habitable rooms in a dwelling will have a window and hence one would expect natural light to be available in typical dwellings. Whilst almost every window will provide a certain degree of view out, the amount and quality of natural light allowed inside will depend on the geometry and characteristics of rooms, openings, glazing materials and the external environment. Location and orientation will also play a role in terms of direct sunlight. Standards exist for daylight in buildings, including dwellings, such as the recent European standard EN 17037, 7 which gives recommendations for adequate provision of daylight and sunlight, adequate view out and control of glare from windows. Although such standards are expected to facilitate optimal daylit environments, particularly in new dwellings, this is not always reflected in practice. Whereas typical houses are more likely to benefit from sufficient natural light, there are dwellings with lower levels in habitable rooms than recommended, as found by several studies performed on UK housing.8,9 For example, single aspect apartments with combined, deep plan lounges and kitchens would typically fail to meet daylight provision recommendations, particularly in the kitchen areas; if also facing north, they would lack direct sunlight, too. Balconies above apartments or nearby obstructions, such as adjacent building sectors or internal courtyards, increase the likelihood of reduced daylight and sunlight provision. On the other hand, dual aspect dwellings, especially those with large and/or tall windows and free from obstructions, would typically achieve the highest levels of natural light.
In terms of electric lighting, there is limited guidance on designing lighting for homes and recommendations are generally restricted to specific building types such as multi-residential buildings or care homes.10,11 Existing regulations are limited to the energy efficiency of lighting, yet when it comes to dwellings, these are applicable at product level (for example, lamp luminous efficacy) rather than at system/installation level. As a result of this, homeowners and occupants benefit from significant freedom and flexibility in choosing the light sources, luminaires and lighting controls that they like, as well as in arranging their lighting and furniture according to their own tastes. LED, tungsten halogen and compact fluorescent lamps tend to be the most common light sources used nowadays in homes. 12 Such lamps are available in a wide range of wattage, luminous flux, colour appearance and colour rendering specifications. There is also a wide variety of luminaire types and designs for domestic settings. For example, depending on the occupants’ preferences, habitable rooms can be lit using arrangements of ceiling-mounted pendants or downlights, ceiling recessed or track mounted spotlights, or wall mounted and/or floor-standing uplights, all in combination with strategically placed table lamps. Illuminance uniformity for such arrangements is typically low, which is not necessarily something to avoid as it contributes to spatial variation and attractiveness of the lit space. Somehow less variation is expected in terms of traditional control systems, which are typically limited to on/off switches or dimmers; however, there is growing uptake of touch- or voice-based controls associated with smart LED lighting. Display screens such as TVs, computers, tablets and mobile phones could also be counted as sources of light, particularly when these are used in a dark environment, such as in the evening with the lighting switched off or dimmed to a minimum level.
Additional influences can arise from the characteristics of the interior decor. Having light colour, high reflectance surfaces in a room increases the amount of daylight and artificial light in the space. This increases the likelihood of receiving a higher dose of light at the eye wherever the individual looks and reduces the levels of discomfort glare through a more balanced luminance distribution in the visual field.
All of the above characteristics lead to a large variety of lighting arrangements in domestic settings and, consequently, to a great variation in the lighting conditions to which residents are likely to be exposed.
3. How lighting can affect human health
3.1 Exposure to light at night
Diurnal species, including humans, have evolved a complex mechanism to regulate physiological processes to the time of day. This is achieved through circadian rhythms that are entrained by the natural 24-hour light–dark cycle. The human circadian system is controlled by the master body clock, or the circadian clock, located in the suprachiasmatic nuclei of the brain’s hypothalamus. 13 The physiological processes known to be controlled by the circadian clock include metabolism, hormone secretion, body temperature, cardiac function and ageing. 14 There are other clocks in the organs and cells in the body, which need to be synchronised to the circadian clock to maintain health. The intrinsically photosensitive retinal ganglion cells in the retina (ipRGCs) contain the photopigment melanopsin which, in response to the incoming light, transmits signals to the suprachiasmatic nucleus to enable resetting of the circadian clock. In conditions of darkness, the pineal gland synthesises the hormone melatonin which is absorbed into the bloodstream and then circulated as a chemical messenger to other clocks in the body. 2 The body’s level of melatonin is frequently used as a biological marker for circadian impact.
Whilst there are a number of factors that can affect the circadian clock, such as eating or exercising, most research indicates that circadian rhythms are mainly regulated by light exposure, which is generally accepted as the major time cue. 15 – 18 In the absence of light, the circadian clock continues to operate but at a period slightly longer than 24 hours which over time leads to various disturbing effects including sleep difficulties.15,19– 22 It is exposure to the natural light–dark cycle, as an external stimulus, that resets the circadian clock to a 24-hour period. When our circadian clock is synchronised with the solar cycle, we feel alert during the day and sleepy at night. However, exposure to artificial light at night can lead to desynchronisation of the circadian clock by delaying or advancing the clock so that sleepiness and alertness may occur at the wrong times. This effect, which is well documented, is additive since photic history, or light exposure mainly over the previous 24 hours, also impacts circadian entrainment. 23
Circadian entrainment is marked by normal levels of melatonin, which are high at night and low during the day. However, the wrong light at the wrong time can affect the natural melatonin cycle. Bright light suppresses melatonin production, and it has been suggested that 30 minutes exposure to 30 lx at the eye from a warm white light source would be a conservative threshold for suppressing melatonin by light at night. 24 A two-hour exposure to self-luminous tablet computers generating illuminances in the range 5–50 lx has also been found to reduce melatonin levels. 25 Nevertheless, melatonin suppression is also impacted by the spectral composition of the incident light. Melanopsin, the photopigment contained in the ipRGCs, has been found to have peak sensitivity at around 480 nm,18,26 and melatonin suppression increases between 446 nm and 477 nm. 27 Hence the circadian system is most sensitive to light in the blue area of the spectrum. Blue light has also been found to impact alertness, body temperature and heart rate. 28 Whilst evening light exposure to blue enriched light, even at relatively low light levels, affects sleep regulation, 29 filtering blue light before sleep can improve sleep quality and mood. 30
Lacking a consistent pattern of light and dark as well as sufficient entrainment signals during the day will increase vulnerability to circadian disruption from light at night.17,31,32 Optimal sleep duration for the average individual appears to be 7–8 hours in a 24-hour period; otherwise health problems can occur, such as cardiovascular diseases, diabetes, obesity, depression, and learning and memory problems. 32 – 35 However, average adult sleep duration in the UK and the US was found to be shorter,13,36 whereas worldwide children sleep 1–2 hours less on school nights than a century ago. 4
Health effects of light at night in the general population relate to reduced melatonin production. Melatonin has been found to play important immunity functions, including protection against various types of cancer. 37 – 42 Lower melatonin levels at night translate into reduced cancer-suppressing effects as found by various researchers.40,43– 47 Nonetheless, other studies did not find the same relationship, potentially due to various other confounding factors including lifestyle.48,49 A recent study in Canada found no association between residential outdoor light at night and breast cancer risk. 50
3.2 Insufficient daytime exposure to light
Various studies have shown the positive effects of daylight on human physiology and health-related concepts such as stress and mood. Exposure to daylight can regulate circadian rhythms and improve sleep quantity and quality, 51 enhance mood, 52 reduce subjective sleepiness53,54 and decrease production of the stress hormone cortisol.55,56 Entrained circadian rhythms have also been found to benefit the cardiovascular system. 57 Children exposed to sufficient daylight are less prone to develop myopia as they grow. 58 – 61 Daylight has additional benefits for people with visual impairments or eye diseases like age-related macular degeneration, cataracts or glaucoma, which are common in the older population, by aiding visual tasks. 62 – 64 Daylight has been associated with healing effects in healthcare,65,66 contributing to less post-surgery pain medication and faster recovery. 67 – 72
Exposure to sunlight outdoors benefits health through vitamin D synthesis, which is essential for maintaining normal blood levels of calcium and phosphorus and thus ensuring healthy bones.73,74 Additionally, sufficient levels of vitamin D have been found to protect against cancer, diabetes, influenza, cardiovascular and autoimmune diseases, 75 – 77 as well as mental health disorders like depression or schizophrenia.78,79 Vitamin D is synthesised when the skin is exposed to UVB radiation (280–315 nm) but this is blocked by conventional window glass. Exposure to daylight through windows, even to bright sunlight, does not result in vitamin D synthesis and thus controlled outdoor exposure to sunlight is recommended.80,81 Nonetheless, sunlight, even through window glass in homes, has been shown to benefit occupant health with respect to infectious diseases.82,83 Residential sunlight exposure was also found to reduce the risk of prostate cancer. 84 In addition to entraining the circadian system, allowing daylight indoors helps to establish visual contact with the outside through daylight apertures, which has been shown to benefit health and mood. 4
Lacking exposure to sufficient daylight may provide reduced health benefits. For example, an investigation of daylight exposure impacts on sleep amongst Londoners aged 65 years and over in summer and winter 85 found that exposure to daylight could help elderly people with poor sleep quality to reduce the number of awakenings at night, since the participants woke up at night more frequently in winter than in summer, which could be related to getting reduced exposure to daylight in winter, insufficient for circadian entrainment. Also, not receiving sufficient short-wavelength light during the morning was found to delay sleep onset and reduce sleep duration in adolescents, which in turn can result in poorer academic performance.86,87 The spectral composition of daylight changes over the course of the day: in the morning there is a higher content of shorter wavelength blue light compared to the late afternoon, when the proportion of longer wavelength red light increases. 4 Based on this model, where indoor daylight provision is insufficient, blue-enriched bright light at the correct times of day, particularly in the morning, could also be used to synchronise circadian rhythms, correct disrupted sleep or increase alertness.21,22,27,88
3.3 Flicker
AC-operated light sources produce rapid and repeated changes over time in their light output or spectral power distribution. These fluctuations lead to visual phenomena generally known as temporal light artefacts (TLAs) which include flicker, stroboscopic effect and phantom array effect. The TLAs differ in that flicker involves a static observer in a static environment, stroboscopic effect refers to a static observer in a non-static environment and causes a change in the perception of motion, and phantom array effect occurs in the case of a non-static observer in a static environment and affects the perception of shapes or spatial positions of objects. 89
Flicker is the most widely known TLA and the most common in typical indoor lighting. The visual system is particularly sensitive to flicker. Whether flicker is visually perceived or not will depend on its frequency and percentage modulation, the proportion of the visual field over which it occurs, and the luminance of the light source. 2 Whilst the Commission Internationale de l'Éclairage (CIE) definition of flicker assumes it to be a visual perception effect, 89 flicker has also been investigated at fluctuation frequencies above the threshold at which it can still be perceived by the human eyes. This threshold, known as critical flicker frequency, has been found to be up to 90 Hz. 90 – 94 Below critical flicker frequency, immediate biological effects have been found to include, depending on individual sensitivity, malaise, fatigue, eyestrain and headaches as well as seizures, including in people without a previous history or diagnosis of epilepsy. 92 However, there are also effects of flicker above critical flicker frequency.
Flicker in the range 100–200 Hz has been found to be non-visually detected by the human retina.92,94 This triggers a chain of sensory and neural responses which, particularly in the case of long-term exposure, have been associated with visual fatigue, eyestrain, excessive eye movements, reduced visual performance and headaches.92,94– 97 People with good vision and health can still be sensitive to flicker above critical flicker frequency. 92 However, flicker sensitivity varies between individuals: people suffering from headaches or migraines, autism or photosensitive epilepsy are more likely to be affected; flicker can also be a concern in case of reading tasks and tasks involving the use of screens.92,98
3.4 Glare
Whilst human eyes can adapt to a wide range of luminances, comfortable vision occurs only within a limited range at any one time. Excessive luminances and luminance contrasts in the visual field may cause glare. Disability glare and discomfort glare are the types of glare that can typically occur in indoor environments.1,2,4
When light from a very bright source reaches the eyes, it gets scattered mainly in the cornea and lens and becomes straylight that reduces the contrasts of the retinal image and the visibility of the scene.99,100 This causes disability glare, which is experienced as impaired or, to some degree, even temporarily lost vision. Although disability glare is not a health risk in itself, it may lead to indirect safety risks by affecting the ability to see and recognize objects. 4 Straylight and thus the probability of disability glare increases strongly with age even in healthy eyes.2,100 This is more accentuated for people suffering from cataracts. 101 In general, sunlight is the most common source of disability glare in the home environment.
It is generally agreed that discomfort glare occurs in the presence of uncomfortable luminance contrasts in the visual field. It is experienced as visual discomfort without necessarily an impaired ability to see. Discomfort glare has been associated with fluctuations in pupil size102,103 as well as contractions in the muscles surrounding the eye that may cause pain effects. 104 It is believed that the pupil, lens, facial and extra-ocular muscles are engaged in a constant pursuit of retinal image clarity, and this continuous muscle readjustment can cause discomfort, tension and pain. 105 Discomfort glare can manifest itself through annoyance, irritability, distraction and visual fatigue or eyestrain. Typical symptoms include soreness of the eyes, dry or watery eyes, itchiness, blurred or double vision, difficulty to focus on objects, irritation of the eyes and lids, tense muscles, as well as headaches and other forms of discomfort such as neck- and backache. 1 –4,106 Discomfort glare has also been linked with adverse effects on mood and wellbeing. 107 Notwithstanding that discomfort glare varies within the same space depending on the position and direction of view, 108 there are also significant individual differences in sensitivity. Some people may be unaware of, or undisturbed by, glaring lighting, whilst others in the same space may experience discomfort symptoms. 105 People suffering from migraines are more sensitive to light than other people, even when they are not experiencing a headache, and hence they are more likely to experience glare or not tolerate bright light. 109
The spectral power distribution of the light incident at the eyes has been found not to have a marked effect on disability glare but to impact ratings of discomfort glare: 110 – 115 light sources that emit more short-wavelength light induce more discomfort glare at the same luminance level compared to light sources with less short-wavelength content. Hence light sources with a higher content of blue light, such as cool white light sources, may be perceived as causing more discomfort glare for the same amount of light reaching the eyes. Older people may experience this more intensely given that light scattering in the eyes increases with age.
3.5 Other health risks from lighting
In some situations, depending on exposure duration and light source luminance, angular size and spectrum, exposure to too bright light, apart from causing disability glare, can also lead to eye damage.2,4 This can take various forms, such as photokeratitis (damage to the cornea) and photoconjunctivitis (damage to the conjunctiva), causing irritation, light sensitivity or even severe pain; cataract (damage to the lens), causing lens opacity, light scattering and less light reaching the retina; photoretinitis and retinal burns (damage to the retina); or macular degeneration (damage to the fovea of the retina), resulting in loss of central vision. 4 Since their lenses are more transparent, infants and children are more sensitive to retinal damage. Individuals having had their lenses removed or replaced with artificial ones, as well as individuals with age-related macular degeneration are also more sensitive to retinal damage.109,116
Given the higher energy associated with it, short-wavelength radiation such as blue light is the most damaging, hence the term blue light hazard. 117 Most white LED light sources use a blue LED and a phosphor coating and thus have peak emissions in the blue range of the spectrum; other lamp types of similar correlated colour temperature (CCT) have comparable amounts of energy in the blue area of the spectrum. However, the blue light hazard is a function of spectrally weighted irradiance on the retina and exposure duration, which in turn depends on source size, radiance and viewing conditions. 118 In fact, the blue light hazard is proportional to the spectrally weighted radiance of the light source. In a recent evaluation of several types of light source, 119 white LED light sources (rated 3000 K, 4000 K and 6500 K) did not show higher risk for the blue light hazard compared to an incandescent lamp, which can be explained by the higher luminance of the filament in the incandescent lamp; as expected, pure blue LEDs displayed a greater risk but this was still significantly lower than that posed by direct sunlight. Limiting the exposure time to such high-risk light sources would be required.
Radiation can also cause skin damage. Visible and infrared radiation raise the skin temperature and, when this is sufficient under very high levels of radiation, burns can occur. 2 Typical light sources for normal lighting generate far lower levels than the threshold for thermal injury of the skin and therefore burns from radiation are not an issue;4,109 however, touching a hot lamp or luminaire might cause burns. Other types of skin damage such as erythema (sunburn), elastosis (photoaging) and cancers are caused by exposure to ultraviolet radiation. 4 Still, this typically occurs outdoors as ultraviolet levels are much lower indoors. Fluorescent light sources can emit some ultraviolet radiation, whilst LEDs emit little or no ultraviolet,117,119 and typical indoor lighting would not cause skin damage due to ultraviolet radiation. Some people suffering from specific skin diseases such as chronic actinic dermatitis can be particularly sensitive to ultraviolet radiation and avoiding exposure to unscreened lamps that might emit ultraviolet radiation is recommended.4,120,121
Electromagnetic fields above a certain intensity can induce electrical currents in the human body; at low frequency, these currents can stimulate the nerves and muscles and at high frequency they can cause tissue heating. 120 Some individuals can be more sensitive to electromagnetic fields and experience dermatological symptoms such as reddening, tingling and burning sensations, but also headache, fatigue, dizziness, nausea and concentration difficulties. 120 Nonetheless, technological advances have enabled electromagnetic fields generated by lighting products to decrease substantially. Various studies 122 – 126 have shown that the intensities of electromagnetic fields generated by typical light sources, including fluorescent and LED lamps, are significantly below the limits recommended by the International Commission for Nonionizing Radiation Protection. 127
Additionally, standards and regulations are in place that provide exposure limits for artificial optical radiation and electromagnetic fields118,125,127– 130 and the levels associated with lighting are well below values that could be considered harmful. Therefore, in normal conditions of use, artificial lighting is deemed to involve no risks to human health arising from optical hazards and electromagnetic fields.109,117,120
4. Minimising detrimental impacts from home lighting
Residents’ health and safety can be affected by the lighting in the home environment. Insufficient light levels or glare caused by excessive luminances can affect the ability to distinguish objects and thus lead to trip or fall hazards, particularly on stairs or thresholds. Uncomfortable luminance contrasts can result in discomfort glare and associated effects like annoyance, irritability, eyestrain, headaches, neckache or backache. Flicker, even above the visual perception threshold, can cause health problems like headaches, eyestrain, fatigue or seizures. Visual aspects of concern such as flicker, glare or insufficient lighting are generally easier to identify compared to non-visual effects of light. Since the latter can in fact have stronger health implications in the long run, 4 raising awareness in the general population of their importance and remedial measures where needed would be required.
4.1 Getting the right light at the right time
Typical daytime lighting in the home environment has been found to be insufficient for stimulating the circadian system and therefore most residents may effectively be living in biological darkness. 109 On the other hand, there is increased exposure to artificial light after sunset, and, despite significant variations between homes 131 and artificial light levels in domestic settings being lower than those in other environments such as workplaces or than those used in laboratory simulations of home lighting, 132 the light levels attainable from home lighting before bedtime can still cause changes in the timing of the sleep–wake cycle and circadian rhythms. 132
Studies on biological effects of light in domestic applications indicate that light in the home environment has the potential to affect sleep and overall health depending on the amount and spectrum of light, the timing and duration of exposure and the photic history. However, the extent of the effects varies with the characteristics of the lighting installation 131 as well as between and within individuals, depending on the type of activity and individual characteristics such as the momentary mental state, the level of chronic fatigue and chronotype. 5 Individual differences between people in circadian light sensitivity appear to be higher at typical indoor light levels. 130 High sensitivity to evening light was found in young adults, with 50% melatonin suppression observed at around 25 lx, yet individual sensitivity varied by a factor of more than 50. 133 Exposure to evening light in home settings (27 lx) was also found to delay sleep onset (by 17 minutes) in elderly people. 134 A study comparing maximised (65 lx on average) versus minimised (3 lx on average) home lighting, 132 each over a week, found average delays of 14 minutes in bedtime and 73 minutes in melatonin onset under maximised home lighting. A recent study in Australian homes 131 found increased exposure to evening light to be associated with increased wakefulness after bedtime and poorer sleep, whereas melanopic irradiance levels were almost double in homes with energy-efficient lighting (such as fluorescent and LED) compared with incandescent lighting. This study also found substantial variation in individual sensitivity, adding to the idea that whilst typical home lighting can affect sleep and the circadian system, it is difficult to predict individual impacts due to the large variation in circadian light sensitivity as well as in the amount and quality of light between homes.
Electric light sources present a wide variety of spectral compositions. Overall, cool white light sources (with a higher CCT) are richer in blue light (400–500 nm) and can be more effective at stimulating the circadian system given its sensitivity to light in this part of the spectrum. As such, the blue content should be reduced towards the end of the day to avoid harmful effects on circadian rhythms. Current LED technology allows for variation of the spectrum of the emitted light throughout the day, as well as its intensity. LEDs can also be produced to generate light in specific areas of the spectrum, even in an overall light emission that appears white to the naked eye. Using this property, called metamerism, it is possible to develop LED light sources that deliver a constant light output and CCT yet changeable spectral compositions to produce variable effects on melatonin suppression but not on alertness. 135 Colour-rendering quality also needs to be maintained, and a recent study 136 showed that by using a combination of four narrowband LEDs (red 625 nm, lime 565 nm, blue 490 nm and violet 415 nm) and a broadband white LED (3600 K), it was possible to achieve a 21% difference in melatonin suppression with changeable spectral compositions whilst maintaining a nominal CCT of 4000 K and a colour-rendering index above 80. There is still scope to optimise LED spectra further in order to produce white light sources of other CCTs, such as the widely used warm white 2700 K or 3000 K, that provide daytime circadian stimulation and night-time circadian protection whilst maintaining optimal visual qualities. Nonetheless, for night-time situations in the home environment, even where light sources with a reduced circadian stimulation potential – as assessed based on the spectral composition relative to circadian sensitivity – are used, prudence is still recommended to ensure sufficiently low light levels so as to enable a light–dark pattern resembling as much as possible the natural daily cycle.
The increased use before bedtime of display screen equipment such as TVs, computers, tablets and mobile phones, particularly when such screens emit light that is rich in short wavelengths, may also impact melatonin production, sleep onset and quality, as well as next morning alertness.25,137– 139 Filtering out blue light and dimming the screens could help in this respect. Other studies found that using such devices before bedtime, for example for social interaction, may affect sleep quality but without necessarily reducing melatonin levels.140,141
In recent years, several sets of metrics have been proposed for lighting that supports circadian entrainment. These are based on measures at eye level weighted against the spectral sensitivity of the melanopsin-containing ipRGCs. However, other retinal photoreceptors can contribute via ipRGCs to the non-visual effects of light.18,142,143 The CIE standard S 026/E 144 introduced an α-opic metrology based on spectral sensitivity functions for each of the five types of retinal photoreceptor that can contribute to the non-visual effects of light. In a subsequent Position Statement, 142 drawing upon findings that non-visual responses are largely controlled by melanopsin-based photoreception135,145,146 and that melanopic illuminance could be an acceptable predictor for circadian responses in most cases as found in a recent review of laboratory studies using subjects with dilated and undilated pupil, 147 the CIE recommended the use of melanopic irradiance or melanopic equivalent daylight illuminance, which is the illuminance from daylight that produces a melanopic irradiance equivalent to that of the light source considered. These metrics are based on vertical quantities at the front of the eye, i.e. at the cornea, and therefore present a clear practical advantage as they are relatively easy to measure in typical practice. Yet, they offer an approximate quantification of the impacts on the biological processes involved in the non-visual effects of light in the general population. Further investigation will be needed to quantify the influence of other factors such as, for example, pupil size affecting retinal irradiance,145,147 spatial distribution of radiance in the field of view relative to spatial distribution of ipRGCs in the retina,143,148 age 149 or photic history. 23
Nonetheless, the CIE also provides an α-opic toolbox 150 to derive various quantities and ratios of the α-opic metrology defined in CIE S 026/E from user measurement results or pre-defined illuminants. These include melanopic efficacy of luminous radiation (MELR) – the ratio of melanopic radiant flux to luminous flux – and melanopic D65 efficacy ratio (MDER) – the ratio of MELR of a light source to MELR for the CIE standard illuminant D65. MELR and MDER can be used to evaluate the potential of a light source to stimulate the circadian system via the melanopsin-containing ipRGCs: the higher the values, the higher the circadian stimulation potential.
Characteristics of the assessed light sources
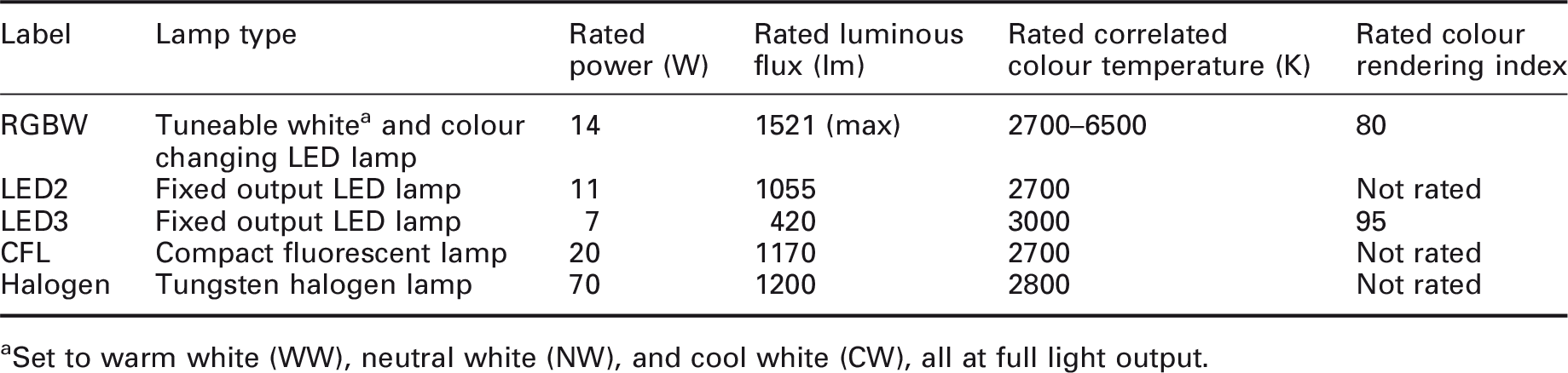
aSet to warm white (WW), neutral white (NW), and cool white (CW), all at full light output.
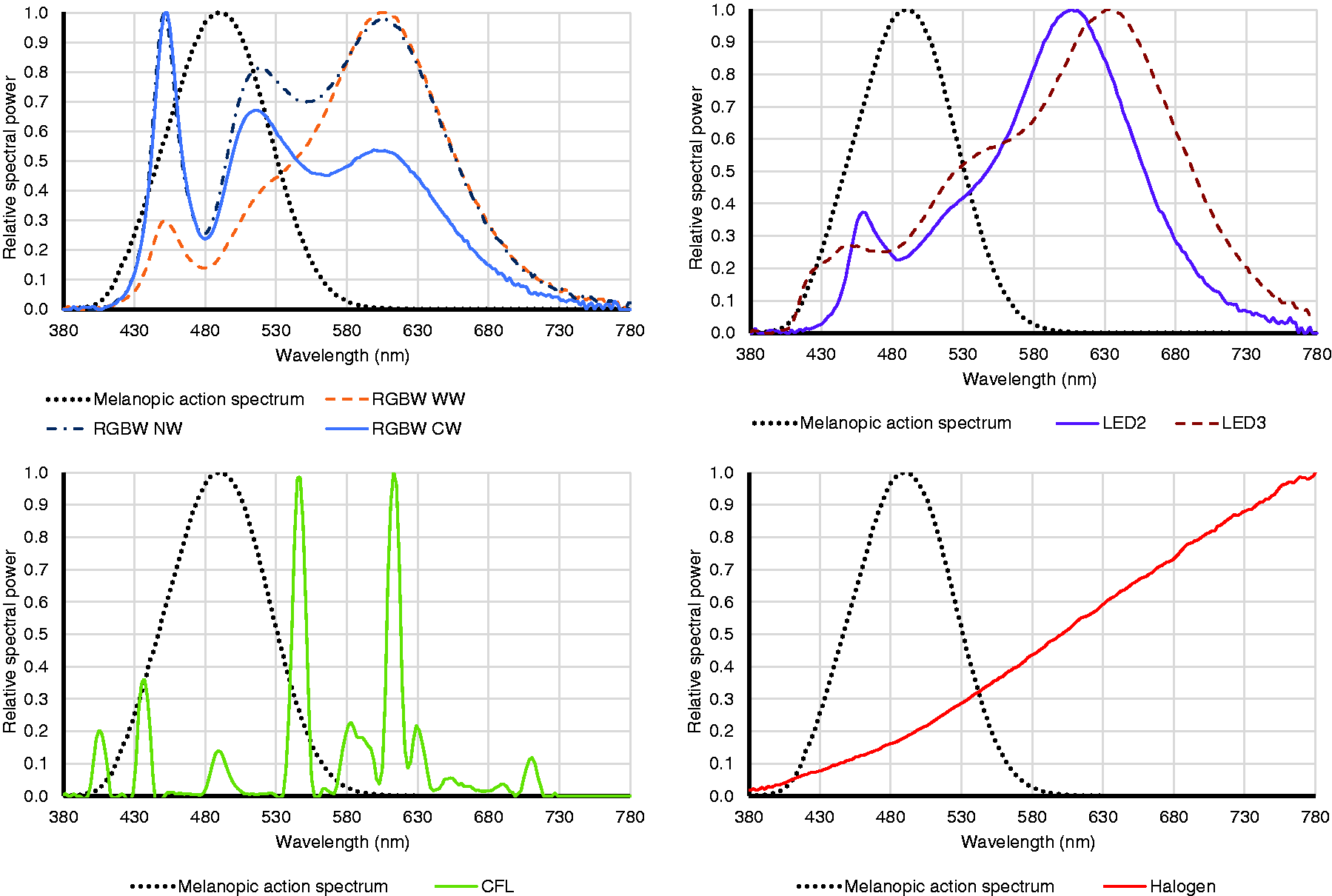
Normalised spectral power distributions of the assessed lamps relative to the melanopic action spectrum (dotted line)
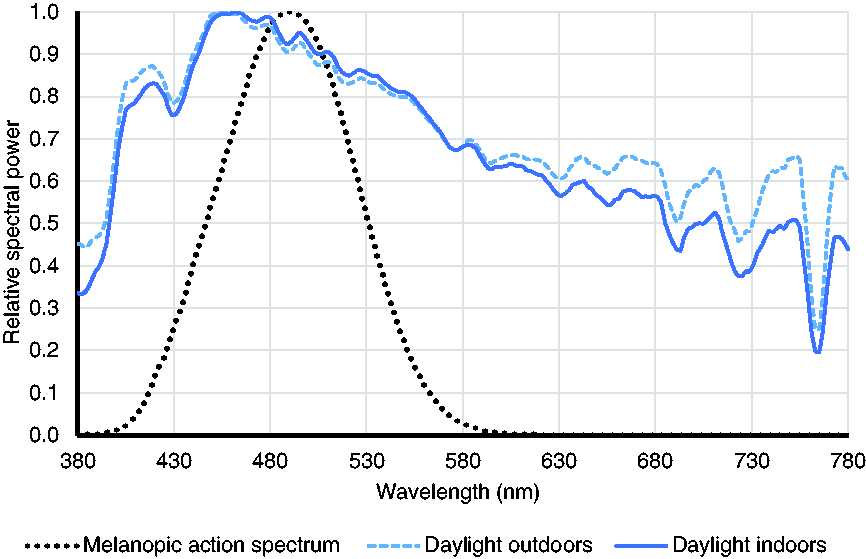
Normalised spectral power distributions for example daylight measurements relative to the melanopic action spectrum (dotted line)
Summary of the measured correlated colour temperature (CCT), colour rendering index (CRI), melanopic efficacy of luminous radiation (MELR) and melanopic D65 efficacy ratio (MDER) for each of the assessed light sources
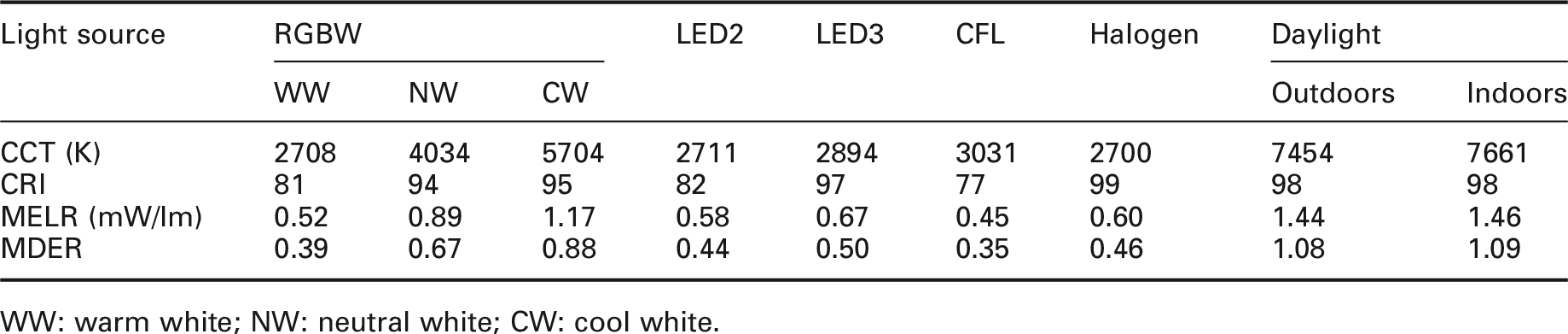
WW: warm white; NW: neutral white; CW: cool white.
Overall, except for the RGBW lamp set to cool white, and to some extent neutral white, the lamps in the assessed sample were relatively inefficient at producing melanopic effects. As such, they would be more appropriate in the evening (also in combination with reduced light levels) than during the day, when daylight or lamps with high MDER also producing higher light levels would be needed.
In general, the easiest way for residents to get circadian stimulation when indoors is through the use of daylight. This would be the case particularly when facing and sitting close to windows. However, under such circumstances, consideration should be given to allowing for blinds or curtains to prevent discomfort glare, or even disability glare from direct sunlight, from occurring. Window size, room shape, dimensions and surface finishes, and task details would also have an impact.
Overall, setting up the artificial lighting in the home environment to ensure circadian entrainment would be best aimed at the times of highest sensitivity to light, i.e. early morning and late evening, when most people would be at home and light would have the strongest biological effects. Bright early morning light, particularly if blue enriched, can stimulate the circadian system and advance its timing, and positively impact alertness and mood, helping individuals to get ready for a new day. In contrast, relatively dim and blue-depleted evening light, or even darkness before bedtime, can help maintain natural levels of melatonin and avoid disruption of sleep and circadian rhythms.
4.2 Avoiding flicker
Homes in Europe are generally supplied from AC mains with a typical frequency of 50 Hz. Unless high frequency control gear is used, fluctuations in electric light source output occurs at a double frequency of 100 Hz. Although the human eyes cannot visually perceive flicker of this frequency, the retina can still detect it. So long as there are no slow fluctuations in the supply voltage, flicker from incandescent light sources does not occur. However, fluorescent lamps are more prone to flicker since the flicker probability depends on the output of their control gear and quality of the phosphor coatings. High frequency control gear (operating at 20 kHz or more) reduces the effects of flicker.1,3,95,151
LED light sources powered directly from an AC supply are prone to flicker due to their rapid response to current fluctuations. Most LED lamps use high frequency drivers that convert the AC component of the mains supply into a DC output that produces a reduced light output modulation and thus helps to reduce flicker. 152 Nonetheless, flicker can still occur when dimming LED light sources, particularly when paired with existing lighting controls in a retrofit situation or when using phase-cut controls or pulse-width modulation. 98 DC drivers can be used to dim the light output of the LEDs to less than 1% without using pulse width modulation, thus avoiding the risk of flickering from light output fluctuations. 152
Modulation depth (percent flicker) and flicker index have often been used to quantify flicker, yet these metrics do not account for differences in periodic frequency as they were defined for a single waveform period and have also been found to not score objectively the level of flicker as actually perceived. 153 Instead, the IEC-standardised ‘short-term flicker severity’ or ‘short-term flicker indicator’ PstLM metric has been proposed to objectively measure flicker.3,153 This is a measure of flicker evaluated over a specified time interval of a relatively short duration (typically 10 minutes). 154 Flicker is one of the functional criteria in the new eco-design requirements for light sources and separate control gear entering into force on 1 September 2021. 155 To comply with the flicker requirement, short-term flicker indicator PstLM should not be more than 1, which is the value corresponding to 50% probability for flicker to be detected by the average observer. Where verification is carried out by authorities, the value measured at full output should not depart from the declared value by more than 10%. At present, the information displayed on the package of lighting products does not include data on flicker. Whilst the lighting products sold on the market should in principle comply with the eco-design requirements, if a consumer wishes to verify the flicker performance, they can request this information from the manufacturer or perform a flicker measurement using a dedicated instrument (and ideally following the standardised testing procedure). There is also the alternative of pointing a digital camera at the light source to see if flicker is visible on the screen (in which case there would be moving dark and light bands travelling slowly across the screen).
All the lamps presented in Table 1 were also assessed for flicker (measured over three minutes in each case), and the short-term flicker indicator PstLM was well below 1 in all cases, thus complying with the new eco-design requirements. Whilst one would expect that light sources brought to the market, particularly from 1 September 2021, comply with the eco-design flicker requirement, it should be noted that this applies to lamps set to full output only. Currently, there is no criterion for dimmable lamps set to different dimming levels. There is an increasing variety of LED lamps available in the marketplace that consumers are free to choose from for their homes. Some of these lamps are also dimmable, yet, in the absence of flicker requirements for dimmed lamps, flicker performance of such lamps is not regulated. As such, flicker from lighting in the home environment could still be an issue when dimming some LED lamps. Choosing light sources that use high frequency control gear and using compatible dimming/tuning lighting controls can help reduce the risk of flicker from dimmed lamps.
4.3 Avoiding glare
Glare in the home environment can occur from bright light sources such as spotlights, bare lamps or bright parts of luminaires, particularly on a darker background, but also from windows during the day. In most cases, residents can change their spatial positions and/or adjust their artificial lighting. However, this is not always possible. For example, when no or insufficient amendments can be made, such as when residents have reduced mobility (e.g. physically incapacitated persons) or the space lacks flexibility to allow residents to change their position and thus avoid glare. Therefore, avoiding glare in the home environment calls for adequate consideration.
Although there may be some tolerance to glare from windows, particularly when there is an interesting view out, 156 depending on their orientation, windows can pose a risk of glare from both direct sunlight and diffuse skylight. Whilst sunlight is beneficial and is often preferred in the home environment and residents can generally move around freely, glare from sunlight may not be of particular concern; yet, when it becomes a nuisance, appropriate blinds or curtains with a sufficiently low visible light transmittance can be used to block it. On the other hand, windows can cause discomfort glare through excessive luminance contrasts between the visible sky and internal surfaces in the field of view; this can be overcome by using translucent blinds or see-through shading to maintain a degree of view out or by painting window walls and reveals in a light colour.
As for electric lighting, using suitable shielding such as diffusing covers for spotlights or opaque or low transmittance shades can reduce the risk of glare. Appropriate uplighting (with light sources above eye level and a relatively uniform spread of light on the ceiling) can reduce the risk of both disability glare by shielding the light sources from direct view and discomfort glare by creating a better luminance balance in the visual field.
Today’s residents spend more time using display screen equipment such as TVs, computers, tablets and mobile phones. Most displays have reflective screens which, for specific positions and view directions, can cause reflected glare. This can take the form of veiling reflections, when images of light sources are reflected off screens, or reduced contrasts on the screen. Such effects can be reduced by limiting the luminance of the light sources as described above, or by using matt screens. Light room surface finishes as well as adjusting the screen position relative to bright light sources will also help, for example by avoiding direct sunlight on the screen or ensuring a comfortable contrast between the screen and its background in the field of view.
5. Conclusion and recommendations
Informed by existing guidelines and research findings, recommendations can be made to ensure that lighting in the home environment has no detrimental effects on residents’ health, but in fact can be used to maximise health benefits. Such recommendations include:
Spend as much time outdoors as possible, preferably in the morning. When indoors, occupy rooms that have outside views and receive daylight and, wherever possible, sunlight. Find indoor seating positions that receive abundant daylight levels but still allow for visual comfort to be maintained. For example, facing towards windows but at an angle and/or at a distance away from them so that glare does not occur, and visual task details are perceived easily, quickly and comfortably. Use suitable shading such as adjustable blinds or curtains for control of glare (ideally whilst still allowing for comfortable view out). Retract the shading when not needed. When necessary, supplement insufficient daylight with electric lighting to achieve adequate light levels on the task areas and at the eyes. When using electric lighting, ensure it is brighter and has a cooler white colour appearance from mid-morning until early afternoon, then dim it down and set it to warmer white colour appearance towards the end of the day.
Gradually reduce the light levels to achieve a minimum at least three hours before bedtime. Keep all electric light sources to the warmest white colour appearance attainable (CCT of no more than 3000 K). If using coloured mood lighting, do not use blue or near-blue colours. Face away from electric light sources as much as possible to reduce light levels at the eyes. Reduce the use of display screen equipment before bedtime. When in use, filter out blue light and reduce screen brightness (for example by using software applications that take into account local sunset and sunrise times as well as personal sleep and waking times). At bedtime, switch off all light sources and, if relevant, close blinds to avoid any light ingress from the outside. If waking up at night, try to avoid switching on normal lighting and use dedicated low level night-time lighting (preferably emitting light in the long-wavelength area of the spectrum).
Use lamps that are dimmable and, ideally, colour tuneable. If colour-tuneable lamps are not an option, then use warm white lamps (with a rated CCT of no more than 3000 K). Use compatible dimming/tuning lighting controls to avoid problems like flicker from dimmed LEDs. Use lamps with high frequency control gear to avoid flicker effects. Use luminaires with suitable shielding of lamps, preferably with an upward light component and wall washing effects whilst still ensuring sufficient downward component for specific tasks such as kitchen activities. Use lamps with good colour rendering properties (for example, CRI of at least 80). Use light finishes for main room surfaces such as ceilings and walls to enhance the overall brightness of the space and visual comfort. Place screens, including TVs, computer displays, tablets and mobile phones, so that reflected glare from light sources like electric lighting and windows is reduced or completely avoided (matt screens instead of glossy would limit the reflected glare effect).
Current knowledge indicates that human health, safety and comfort can be affected by light. Yet further research is needed to deepen the understanding of the processes involved, particularly around non-visual effects of light, and to provide reliable models for quantifying the impacts. Research on home lighting and its associated health effects is still scarce and inferences are generally drawn using outcomes of laboratory or other sector studies. It would be valuable for future research to explore actual lighting conditions in real homes, what health outcomes these might have amongst specific populations and how such outcomes might be influenced by individual habits and preferences and by cultural or socioeconomic factors. Notwithstanding the significant variation in the lighting conditions to which residents are likely to be exposed in their homes as well as the variety of other factors affecting human health, it is hoped that the above recommendations for home lighting are of assistance in taking remedial measures wherever necessary to limit detrimental effects of lighting and contribute to residents’ good health.
Footnotes
Acknowledgements
The author would like to thank Professor Peter Raynham for insightful comments on a draft version of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.