
Abstract
The present studies examined the feasibility and acute alerting effects of additional in-vehicle lighting within a passenger car. These factors were examined during morning driving (Study 1) and evening driving (Study 2). In a balanced within-subjects design, 37 participants drove a test car two times in the morning or in the evening. The test vehicle was equipped with either a daylight-supplementing interior lighting system or a placebo system, which participants were told would refresh the air. Both studies used identical protocols, and participants participated either in Study 1 (n = 18) or Study 2 (n = 19). In both studies, corneal illuminance levels were recorded while driving. Feasibility of the systems was assessed using subjective ratings. Efficacy outcomes were spindle rates in the alpha bandwidth of electroencephalogram recordings, performance on a psychomotor vigilance task and subjective sleepiness ratings. In both studies, daylight-supplementing significantly increased corneal illuminances while driving and did not cause any negative visual side-effects. Study 1 revealed lower spindle rates while driving under daylight-supplementing lighting, indicating that drivers had higher physiological alertness when exposed to additional light in the morning. This alerting effect of daylight-supplementing lighting, however, was not observed in Study 2. In both studies, performance on the psychomotor vigilance task as well as subjective sleepiness ratings did not significantly differ between the experimental conditions. The present studies provide novel evidence for the feasibility and positive impact of daylight-supplementing in-vehicle lighting systems on the physiological alertness of drivers under naturalistic driving conditions. Further studies are warranted to evaluate carry-over effects of increased alertness on road safety measures.
1. Introduction
1.1 Sleepiness while driving
Roughly 10–20% of all road crashes are associated with sleepiness 1 and reduced alertness of drivers. 2 Interestingly, these types of crashes peak during the early morning between 4:00 and 6:00 AM when cognitive performance and vigilance, modulated by the circadian system, drop to their daily low. These performance factors drop again to a smaller extent in the mid- to late afternoon from 3:00 to 5:00 PM.3–6
Decreased vigilance associated with drowsiness is likely a major factor underlying driving impairments while sleepy, especially in monotonous situations. Accordingly, sleepiness-related car crashes occur more often in situations associated with higher monotony such as driving at night 7 and driving on motorways compared with other types of roads. 8
The most common measures employed to combat driver drowsiness require taking breaks (e.g. to consume caffeine, to nap or to take a walk) or are implemented while driving (e.g. turning on the audio system or opening a window 9 ). Studies have shown that pausing long drives to nap and take breaks can effectively reduce sleepiness.10,11 In contrast, countermeasures designed to reduce sleepiness while driving are far less effective and, if at all, work over only a very short time span. 12
1.2 Bright light exposure as countermeasure to sleepiness
Research has shown that a single, short exposure to bright light may have non-visual effects in humans, such as excitation of non-visual physiological systems. Nighttime light exposure has an acute effect on circadian endocrine,13,14 cardiovascular and thermo-regulation parameters. 15 Furthermore, bright light exposure may even increase alertness and cognitive performance16–20 and, thus, may be an effective countermeasure to sleepiness both during driving breaks and while driving. However, studies investigating the effects of bright light exposure on alertness during the daytime are inconclusive.21,22 Systematic reviews have recently summarised some evidence for increased subjective alertness,23–25 but demonstrate heterogeneous results on objective alertness parameters.26,27
1.3 Reduced in-vehicle light exposure during daytime
When outdoors, light exposure ranges from 100 to 600 lux during twilight28,29 to more than 50 000 lux during full daylight.30–32 In contrast, indoor light levels, measured at eye level and generated by artificial light sources, typically range from 100 to 300 lux.33–36 So far, no research has been published on light exposure levels experienced by drivers while driving, either during the day or during twilight. A previous light exposure study conducted by our research group under sunny daylight conditions (data on file), demonstrated that front- and back-seat car passengers were exposed, on average, to 2900 lux and 800 lux, respectively, at eye level. Compared to outdoor illuminance levels, corneal illuminances measured in the car (i.e. vertical illuminance as assessed at the eye level of a seated person) were significantly reduced (5–27% of outdoor light levels).
1.4 Study goals
It can be hypothesised that increasing light exposure of drivers, especially during times of reduced daylight exposure, may have acute effects on their alertness. Research into the effects of light on car drivers is scarce and has, thus far, mainly investigated the effects of low-intensity, narrowband blue light during nighttime driving.37–41 To our best knowledge, only one study has quantified the potential of artificially increased light exposure to increase alertness while driving trucks under naturalistic, daytime conditions. 42 However, no studies to our knowledge have investigated this non-visual effect in passenger cars during the daytime.
We have developed a daylight-supplementing (DS) in-vehicle lighting system and have integrated it into a passenger car. Coupled with the illuminance levels measured at the windshield, this system aimed at also increasing illuminance levels at the eyes of drivers (measured by corneal illuminance levels). Based on the aforementioned preliminary unpublished data, we assumed that light exposure is especially low during twilight, and that increasing drivers’ retinal light exposure could have acute non-visual effects on alertness.
To maximise potentially alerting effects of a supplemented daylight intervention, the studies were performed at times when (a) alertness levels are typically reduced (i.e. early morning and late afternoon), (b) daylight levels in the car are low (i.e. in winter months during dawn [Study 1] and dusk [Study 2]) and (c) monotony is high (i.e. prolonged commuting trips on the motorway).
A main goal of these two experimental studies was to investigate the feasibility of the new DS lighting system. We expected that additional in-vehicle lighting, adjusted to outdoor illuminance levels, would substantially increase drivers’ corneal illuminance levels without causing any adverse visual side-effects. Another major aim of these studies was to assess the effects of light supplementation on alertness and neurophysiological arousal while driving under monotonous conditions. We hypothesised that driving with increased corneal illuminance levels, both during dawn and dusk, would acutely raise cortical arousal levels. In both studies, we further examined potential carry-over effects of increased light exposure, mainly after the end of the drive. We hypothesised that higher cortical arousal levels induced by supplement light may be a longer lasting effect and further improve cognitive and subjective alertness parameters immediately at the end of the drive.
2. Materials and methods
2.1 Study participants
Several hundred employees at Daimler AG, working in various departments of the company, regularly volunteer to evaluate new products. From this pool, more than 200 employees had received a special training in driving safety and were separately insured to drive test cars to evaluate newly developed products while driving (e.g. navigation and driving assistance systems). These participants were invited for study participation and informed that the study aimed at testing the feasibility and efficacy of two newly developed systems, which might support the driver’s fitness.
To start the studies at similar daytimes in winter, we restricted data collection to a period of four weeks. By implementing a within-subject design and conducting both studies in parallel, a maximum of 40 participants could be included. Participants were excluded if they had (1) any sleep disorders such as obstructive sleep apnoea or restless leg syndrome, (2) moderate to heavy caffeine or nicotine consumption (i.e. more than three cups of coffee per day and/or difficulties to refrain from smoking for at least 6 hours) and (3) a height of more than 1.85 m (restricted by the employed light-supplementation device). Additionally, participants who require eye glasses (contact lenses allowed) and those with colour vision deficiencies (tested with Ishihara cards) were excluded from participation. The first 40 participants who wanted to participate in Study 1 (n = 20) or Study 2 (n = 20) and who met the eligibility criteria for participation were included. Each participant could choose to drive the test car in the morning (Study 1) or evening (Study 2) and was exposed to both interventions (within-subject design). To characterise the samples, participants rated their daytime sleepiness level (Epworth Sleepiness Scale, 43 ESS), nighttime sleep quality (Pittsburgh Sleep Quality Index, 44 PSQI) and chronotype (Morningness–Eveningness Questionnaire, 45 D-MEQ). A detailed description of these three scales is given in the Supplementary Data. The ages of the participants ranged from 25 to 55 years, constituting a representative sample of the commuting population.
All study participants provided written, informed consent and received financial compensation for their participation. The study was carried out in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the University of Regensburg.
2.2 Study interventions
Two passenger cars (Mercedes-Benz, W213, E400 4Matic sedan, 2017) were equipped with either an adaptive DS system on the driver’s side of the passenger cabin or a system that participants were told would refresh the air (AR). General ambient car lighting was dimmed and fixed to neutral white light. Car lighting and instrumental lighting were identical in both cars. Participants were told that the study aimed to quantify the effects of the two interventions on alertness while driving.
2.2.1 Adaptive daylight-supplementing lighting system
The luminaire prototype had dimensions of 240 mm (L) × 160 mm (W) × 20 mm (H) and comprised a light-outcoupling structure redirecting light to the face and body of the driver and the vehicle interior nearby the driver (see Figure 1). The elevation angle from the line of sight to the centre of the luminaire was 25°, and the system was placed at a distance of approximately 0.20 m to the eyes of the driver. Image showing the supplemental daylight (DS) intervention to provide drivers with more illumination while driving
The integration of the system necessitated the removal of the sun visor on the driver’s side of the passenger cabin. Taking into consideration that the absence of a sun visor may cause direct glare when driving towards the rising and setting sun, the driving route of the study was chosen to reduce driving toward the sun. The outward drive was primarily directed to the south, while the return drive was directed to the north. Thus, the rising and setting sun was always in the peripheral visual field of the driver.
The luminaire fulfilled the following three design criteria: (1) the light-emitting surface should generate a sky-like visual impression (i.e. ‘convertible feeling’), (2) the emitted light should stimulate photosensitive retinal ganglion cells with peak sensitivity between 460 and 490 nm and (3) the luminance of the light-emitting surface should be limited to avoid glare while driving. In regards to design criterion 1, the ‘convertible feeling,’ light was generated by 18 blue LEDs (Nichia NCSB 219BT-V1, 40 lm, peak wavelength: 471 nm) and 36 white LEDs (Nichia NSSL 157AT-H3, 25 lm, 2700 Kelvin, CRI 80). The colour temperature of the emitted light was kept constant across all dimming levels. With respect to design criterion 2, we determined non-visual parameters of optical radiation measured perpendicular to the light-emitting surface of the luminaire. The melanopic efficacy of luminous radiation (see CIE S 026:2019) was 3.62 and the circadian action factor (see DIN 5031-100:2008) was 2.77. These values were considerably higher than corresponding factors of a standardised daylight spectrum D65 (i.e. 1.32 for melanopic efficacy of luminous radiation and 0.94 for the circadian action factor; see CIE 51.2:1999). Measured non-visual values varied considerably across different beam angles – for example, at the corneal level of the driver, the melanopic efficacy of luminous radiation and circadian action factor were approximately 1.81 and 1.27, respectively.
Figure 2 shows the normalised emission spectrum of the luminaire prototype measured perpendicular to the light-emitting surface, the action spectra for calculating the melanopic efficacy and circadian action factor and the human brightness sensitivity curve for a 2° standard observer. Normalised emission spectrum (blue) measured perpendicular to the light-emitting surface and action spectra for visual and non-visual photometry; DS: daylight-supplementing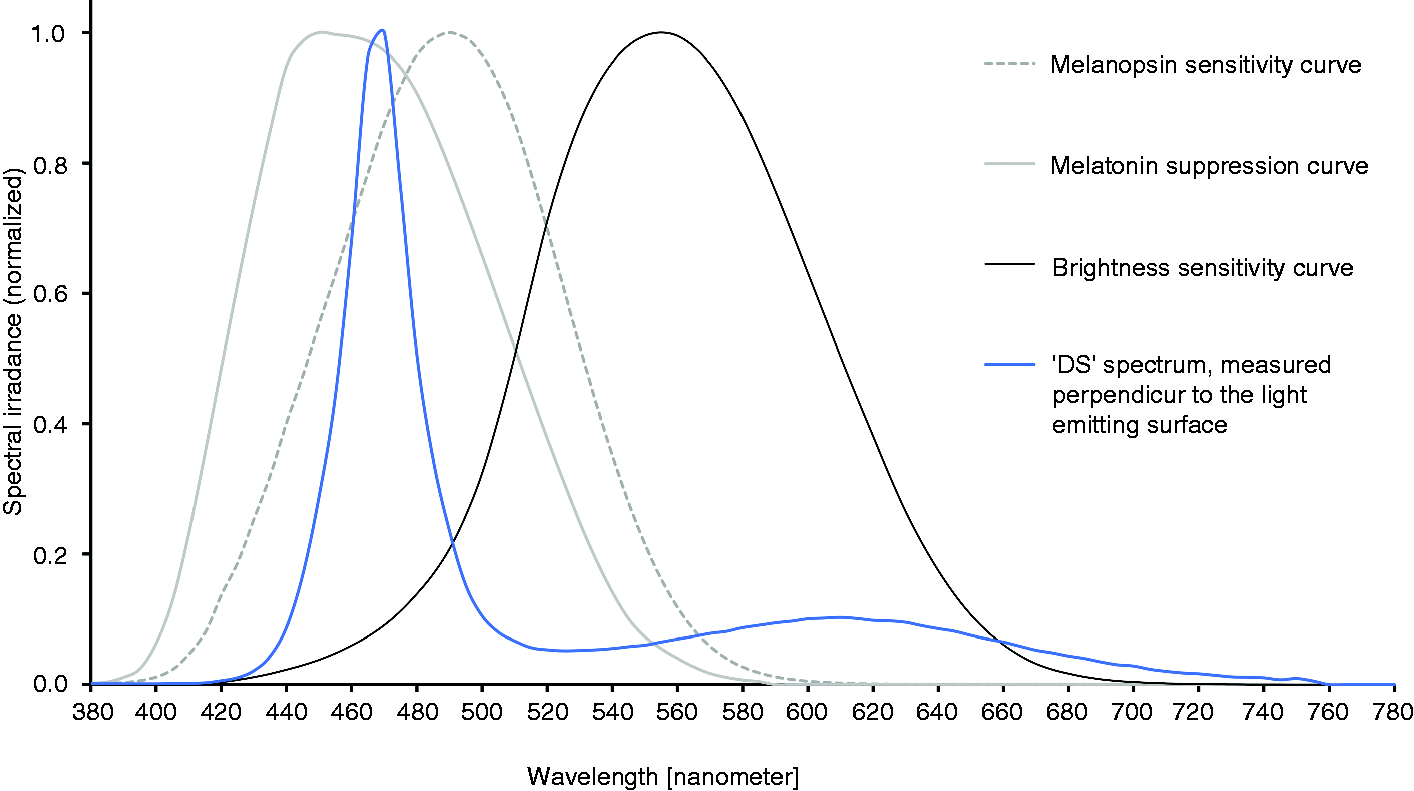
To determine the outmost acceptable luminance level of the light-emitting surface to avoid dazzle while driving (see design criterion 3), a small preliminary pilot study with five test drivers was conducted. In this pilot study, a passenger car was driven during twilight under various but fixed dimming levels of the luminaire, and the test drivers were asked to rate perceived glare levels. The pilot study clearly indicated that drivers did not perceive glare when the dimming levels of the luminaire were adjusted to outdoor illuminance levels. By synchronising outdoor and in-vehicle illuminances, lighting conditions similar to driving a convertible were generated. The pilot study further indicated that the luminance of the light-emitting surface should be restricted to 4500 cd/m2, irrespective of the outdoor lighting scenario, which implied that the corneal illuminance of the driver could be increased by at most 1500 lux. To the best of our knowledge, no study has yet demonstrated that visual performance parameters of convertible drivers are impaired when avoiding direct glare from sunlight (the sun’s luminance at noon on a sunny day is approximately 1.6 × 109 cd/m2).
To fulfil these criteria, a daylight adaptive lighting control strategy was implemented and used in the experimental condition (DS). A high-dynamic-range digital photosensor (Adafruit TSL2591, Figure 3) was placed near the windshield in the middle of the cockpit area and continuously recorded illuminance levels with a sampling frequency of 1 Hz. These data were then averaged over 5-second bins, generating a dimming signal for the luminaire (Table 1). In brief, 33 lux were added with DS when illuminances at the windshield were between 25 and 50 lux. With higher illuminances at the windshield (up to 2000 lux), DS generated an additional two-thirds of the windshield illuminance level at the cornea of the driver (i.e. with 2000 lux at the windshield, the luminaire added up to a maximum of 1320 lux). The photosensor of ‘LuxBlick’ (indicated with a red box) continuously measured illuminances at the windshield Dimming scheme for the luminaire DS: daylight-supplementing lighting.

2.2.2 Placebo intervention
Due to disagreement about what an ineffective placebo light condition for a light impact study could be, we decided to use an intervention mode that focuses on a different sensory modality entirely. The placebo condition (AR) was thus a mock-up air refreshing system which consisted of a large white box placed in the trunk of the test vehicle. This box had a feigned connection to the air conditioning system of the car. Participants were shown the box before they started the test drive and told that effects of the air refreshing system on driver’s alertness would be investigated. No further details on the mode of action of this box were given to the study participants. A black switch on top of the box was turned on, and participants could see a bright red indicator lamp and hear a buzzing noise indicating an active status. The device simply sucked air out of the trunk and emitted it back into the trunk without changing the air quality within the vehicle.
2.3 Study protocols
In the two field studies (Study 1, morning driving; Study 2, evening driving), we compared acute effects on arousal of the DS experimental intervention and AR placebo during and after driving. The same study protocols were used for each study and for each condition within the studies. Participants in both studies were assigned to the interventions in a counterbalanced manner and had a break of one or two days between the two driving sessions.
Data collection occurred in winter (between 22 January 2018 and 16 February 2018). In both studies, the drive included a round trip on a German motorway. It started at the motorway access point ‘Böblingen,’ changed driving direction after a short break at the motorway service area ‘Engen im Hegau,’ and returned to motorway access point ‘Böblingen.’ The drive was primarily on a two-lane motorway with low traffic volume. During the time frames of data collection in the morning and evening, traffic volume in this rural area was generally low. To further evaluate prevailing traffic conditions, we recorded trip durations as an indirect measure of low or high traffic volume (see B1, Supplementary Data).
Participants drove the route unaccompanied as this is mimicking a natural monotonous driving situation. The overall driving distance was 234 km. Participants were instructed to maintain a vehicle speed of 120 km/h (resulting in a driving duration of approximately 2 hours), to drive in the right lane and to avoid overtaking. Furthermore, participants were instructed not to use the steering assistant and, to avoid arousing effects besides those from the interventions, were not allowed to use the audio system of the car. They were also not allowed to make phone calls, eat, smoke or chew gum during the whole driving and assessment procedure.
Drives in Study 1 started exactly 30 minutes before sunrise (i.e. when civil dawn began) to guarantee that the adaptive DS lighting system was active for a similar duration for all participants. Consequently, starting times varied between 6:31 AM and 7:06 AM. Motorway trips in Study 2 started exactly 50 minutes before sunset (between 4:04 PM and 4:44 PM). As a consequence, sunset occurred halfway during the drive just before the break at the motorway service area, and the return trip took place under civil and nautical twilight conditions. This provided the opportunity to measure potential carry-over effects of daylight supplementation when DS was automatically switched off after the break due to a lack of daylight.
Generally, participants arrived at the study location (laboratory in the city of Böblingen) 90 minutes before the start of the drive. Upon arrival, participants filled in a sleep questionnaire and rated their sleep quality of the previous night using the ‘Self-rating scale of Sleep and Awakening Quality’ (SSA). The EEG cap was then fitted.
Before the test drive started and while sitting in the car, participants conducted a 10-minute sustained attention test (the psychomotor vigilance task (PVT) records reaction speed to visual stimuli with the reciprocal reaction time [RRT; 1/s] as the main outcome variable
46
). Directly after performing the PVT, participants rated their subjective alertness and sleepiness states using the Karolinska Sleepiness Scale (KSS; provides nine rating steps ranging from 1 [‘extremely alert’] to 9 [‘very sleepy, fighting sleep’]).
47
The test drive then began. After driving for approximately 1 h, participants reached the motorway service area, where they had a short 5-minute break. During this time, participants rated their sleepiness state (KSS) again. After this break, participants drove back to the start of the drive. Immediately after the conclusions of the drive, participants rated their state of sleepiness (KSS) for a third time and performed the PVT again. Finally, participants rated their acceptance of the intervention, filled in a questionnaire about its potential side-effects, and completed a driving logbook. Figure 4 visualises the study protocol of the two studies including times of sunrise and sunset as well as the active period of the DS intervention. All measures used to quantify the feasibility of the interventions (7-point semantic differential, visual side-effects questionnaire, and the body-worn photic measurement device ‘LuxBlick 2.0’) are described in detail in A1 and A2, Supplementary Data. Study protocol for Studies 1 and 2 for both the experimental and placebo conditions; blue squares indicate the 6-minute route segments with monotonous driving conditions, which were subjected to data analysis PVT: psychomotor vigilance test; KSS: Karolinska sleepiness scale; EEG: electroencephalogram, continuous EEG recording; Q: acceptance and side-effects questionnaire and driving logbook; at the beginning and end of the study, PVT, KSS and Q were performed at in the car in a laboratory without daylight and strongly dimmed room light Electroencephalogram (EEG) alpha spindle rates across driving periods (Study 1); squares indicate mean spindle rates for AR; rectangles indicate mean spindle rates for DS; data are given as mean ± standard error

Vigilance of drivers has traditionally been measured using driving simulators in highly controlled laboratory environments. In these studies, behavioural (e.g. steering and driving behaviour) and gaze-related data are usually used as markers of vigilance. Because these parameters cannot be easily measured under natural driving conditions, we utilised physiological measures to quantify varying arousal levels. A promising recently published approach for this purpose is the usage of parameters derived from EEG data recorded while driving.48–50 It has been shown that parameters related to the spindle rate in the alpha bandwidth (7–12 Hz) of the EEG spectrum are strongly associated with a driver’s level of arousal51,52 during extended driving periods. 53 In fact, even short-term variations in attention can be quantified using these measures. 51 Thus, we chose the alpha spindle rate of the EEG while driving under monotonous conditions as primary outcome measure. Details on the method used to calculate alpha spindle rates in the time–frequency decomposition of the EEG signal are given in A3, Supplementary Data. Furthermore, the applied alertness rating scale (KSS) and psychomotor vigilance parameters (PVT) are explicitly described in A4 and A5, Supplementary Data. Finally, a comprehensive description of the methods used for statistical analysis is also given in Supplementary Data.
3. Results
3.1 Study samples
Demographics, sleepiness, sleep quality the night before and chronotype of participants in Study 1 and Study 2
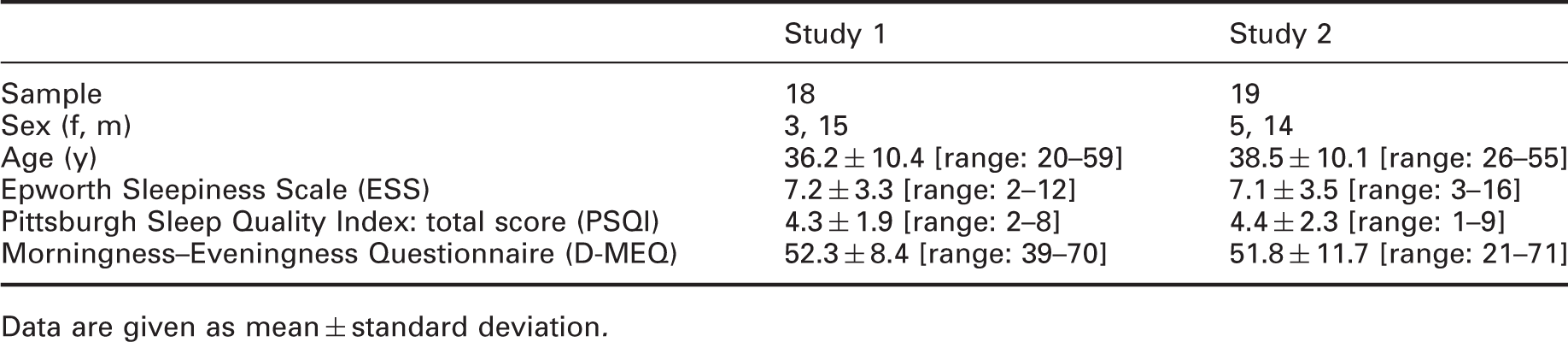
Data are given as mean ± standard deviation.
3.2 Feasibility: corneal illuminance level and acceptance of the light intervention
3.2.1 Corneal light exposure of drivers
Corneal photic stimulation of drivers in Study 1

Indicates the driving period when sunrise occurred; data are given as mean ± standard error.
Indicates a significant difference (p < 0.050) between the two study conditions for the corresponding driving period.
A r-ANOVA yielded a statistically significant interaction between the two factors of ‘intervention’ and ‘time’ on corneal illuminance in Study 1 (F[12, 204] = 23.22, p < 0.001, partial η2 = .577). Bonferroni-adjusted post hoc tests revealed that corneal illuminances were significantly increased under DS after sunrise (i.e. for the driving periods ‘5’ to ‘13’ [all p < 0.050 compared to AR]). Further, there was a statistically significant interaction on corneal circadian action factor in Study 1 (F[12, 204] = 8.96, p < 0.001, partial η2 = 0.345). Post hoc tests showed that circadian action factors were significantly higher under DS compared to AR from period ‘6’ to ‘13’ (all p < 0.050).
Descriptive statistics for corneal illuminances and corneal action factors during the outward driving phase of Study 2

Indicates that sunset occurred after this driving period; data are given as mean ± standard error.
Indicates a significant difference (p < 0.050) between the two interventions for the corresponding period.
r-ANOVAs were used to compare the two measured light parameters (corneal illuminance and circadian action factor) at the level of the drivers’ eyes. There was a statistically significant interaction between the two factors ‘intervention’ and ‘time’ on corneal illuminance in the evening (F[6, 108] = 7.82, p = 0.003, partial η2 = 0.303). Bonferroni-adjusted post hoc tests showed that corneal illuminances were significantly higher for the first five driving periods (periods ‘1’ to ‘5’) under DS compared to AR (all p < 0.050).
Further, a statistically significant interaction was found on corneal circadian action factors in Study 2 (F[6, 108] = 6.39, p = 0.001, partial η2 = 0.262). Post hoc tests showed that circadian action factors were significantly higher under DR compared to AR in six out of seven driving periods of the outward drive (i.e. from driving period ‘1’ to ‘6’; all p < 0.050).
3.2.2 Acceptance ratings
Fisher’s exact test was used to compare acceptance levels of the two interventions. In both studies, ratings for two items did not show any significant differences: ‘pleasant-unpleasant’ (Study 1: p = 0.531; Study 2: p = 0.504) and ‘relaxing-activating’ (Study 1: p = .459; Study 2: p = 0.761). In contrast, ratings for the items ’familiar–unfamiliar’ and ‘unobtrusive–obtrusive’ differed significantly in Study 1 (p < 0.001 for both) and in Study 2 (p = 0.012 and p < 0.001, respectively). Although DS was perceived as more unfamiliar and obtrusive compared to the placebo intervention in both studies, distributions of associated ratings indicated a high degree of familiarity and unobtrusiveness of DS.
3.2.3 Reports on negative visual side-effects

3.3 Impact assessment of the light intervention
3.3.1 EEG alpha spindle rate
In Study 1 (Figure 5), there was no significant two-way interaction between the factors ’intervention’ and ‘time’ for alpha spindle rate (F[12, 204] = 0.71, p = 0.618). However, the main effect of ‘intervention’ was statistically significant in Study 1 (F[1, 17] = 5.14, p = 0.037, partial η2 = 0.232), with lower spindle rates under DS (9.9 ± 7.0) compared to AR (11.2 ± 7.0). Additionally, there was a significant main effect of ‘time’ (F[12, 204] = 12.94, p < 0.001, partial η2 = 0.432). Post hoc tests revealed lower alpha spindle rates (all p < 0.050) in period ‘1’ (9.5 ± 7.2 counts per minute), ‘2’ (8.9 ± 6.7 counts per minute), ‘3’ (9.6 ± 6.7 counts per minute) and ‘4’ (9.5 ± 6.5 counts per minute) compared to the remaining driving periods after the break (i.e. period ‘8’ [11.2 ± 7.0 counts per minute], ‘9’ [11.5 ± 7.4 counts per minute], ‘10’ [11.6 ± 7.4 counts per minute], ‘11’ [11.5 ± 7.3 counts per minute], ‘12’ [11.8 ± 7.1 counts per minute] and ‘13’ [11.4 ± 7.2 counts per minute].
During the light intervention period (from period ‘1’ to period ‘7’) in Study 2, there was no significant interaction between the factors ’intervention’ and ‘time’ in alpha spindle rate (F[6, 108] = 1.19, p = 0.323), and no significant main effect of ‘intervention’ (F[1, 18] = 2.11, p = 0.164). However, the main effect of ‘time’ was significant in Study 2 (F[6, 108] = 2.81, p = 0.030, partial η2 = 0.135). Post hoc tests showed a significantly lower alpha spindle rate in period ‘3’ (10.23 ± 5.77 counts per minute) compared to period ‘5’ (11.49 ± 6.41 counts per minute; p = 0.026).
After-effects of the DS intervention, potentially occurring in periods ‘8’ to ‘13,’ were not observed; the interaction between the factors ’intervention’ and ‘time’ and main effects of ‘intervention’ and ‘time’ were not significant (interaction: F[5, 90] = 0.31, p = 0.843; main effect ‘intervention’: F[1, 18] = 2.20, p = 0.155; main effect ‘time’: F[5, 90] = 1.58, p = 0.196).
3.3.2 Subjective alertness
In Study 1, no significant interaction or main effect of ‘intervention’ in KSS sleepiness scores was seen in an r-ANOVA analysis (F[2, 34] = 0.02, p = 0.979; and F[1, 17] = 0.49, p = 0.494, respectively). However, there was a significant main effect of ‘time’ (F[2, 34] = 12.85, p < 0.001, partial η2 = 0.431). Post hoc tests showed higher subjective sleepiness during the driving break (KSS: 6.2 ± 2.1) compared to before (4.0 ± 1.8) and after the drive (4.8 ± 1.7; all p < 0.050).
Regarding sleepiness ratings recorded immediately before and after the light intervention period in Study 2 (i.e. before begin of drive started and during break), an r-ANOVA did not show a significant interaction in KSS (F[1, 18] = 0.40, p = 0.537) as well as no main effect of ‘intervention’ (F[1, 18] = 0.03, p = 0.858). However, sleepiness scores were increased during the break compared to before the drive (F[1, 18] = 7.44, p = 0.014, partial η2 = 0.293; KSS before drive: 3.6 ± 1.6; during break: 4.5 ± 1.9). Comparing sleepiness ratings after the light intervention period in Study 2 (i.e. during the break and at the end of the drive), there was no significant interaction between the factors ’intervention’ and ‘time’ (F[1, 18] = 0.44, p = 0.515) and no significant main effect of ‘intervention’ (F[1, 18] = 0.01, p = 0.937) or ‘time’ (F[1, 18] = 0.70, p = 0.415).
3.3.3 Psychomotor vigilance task (before/after drive)
We observed no significant interaction or main effect of ‘intervention’ on reaction speed in Study 1 (F[1, 16] = 0.07, p = 0.796; and F[1, 16] = 0.98, p = 0.338, respectively), but there was a significant main effect of ‘time’ (F[1, 16] = 4.84, p = 0.043, partial η2 = 0.232) on higher reaction speed after the drive (RRT [1/s]: 3.68 ± 0.50) compared to before the drive (RRT: 3.60 ± 0.49). All interactions and main effects of the factors ‘intervention’ and ‘time’ were not significant for the remaining PVT parameters (i.e. fastest 10% of reaction times, slowest 10% of reaction times, and number of lapses; p > 0.050). Furthermore, we observed no significant interaction or main effect of ‘intervention’ for reaction speed in Study 2 (F[1, 18] = 0.12, p = 0.731 and F[1, 18] = 1.59, p = 0.224, respectively) but there was a significant main effect of ‘time’ (F[1, 18] = 16.29, p = 0.001, partial η2 = 0.475) with higher reaction speed after the drive (RRT: 3.89 ± 0.43) compared to before the drive (RRT: 3.68 ± 0.49).
Neither interactions nor main effects of ‘intervention’ and ‘time’ were significant for the fastest 10% of reaction times (interaction between ‘intervention’ and ‘time’: F[1, 18] = 0.25, p = 0.624; main effect of ‘intervention’: F[1, 18] = 0.00, p = 0.985; main effect of ‘time’: F[1, 18] = 1.44, p = 0.246) and number of lapses (interaction between ‘intervention’ and ‘time’: F[1, 18] = 3.40, p = 0.082; main effect of ‘intervention’: F[1, 18] = 0.90, p = 0.356; main effect of ‘time’: F[1, 18] = 4.25, p = 0.054). Finally, there was also no significant interaction between ‘intervention’ and ‘time’ or a significant main effect of ‘intervention’ for the slowest 10% of reaction times (F[1, 18] = 2.74, p = 0.115 and F[1, 18] = 0.39, p = 0.541, respectively). However, the main effect of ‘time’ for the slowest 10% of reaction times was significant (F[1, 18] = 6.48, p = 0.020, partial η2 = 0.265), with lower reaction times after the drive (RT in ms: 370 ± 62) compared to before the drive (RT in ms: 397 ± 73).
4. Discussion
4.1 Feasibility of the light intervention under natural driving conditions
In the present study, a DS lighting system was able to increase corneal illuminance of drivers at least by a factor of 4 when driving on a motorway from south to north and back during dawn (Study 1). In addition, this system exposed drivers to larger amount of light also during dusk (corneal illuminances were increased by a factor of two to three; Study 2). Besides heightened corneal illuminance levels, the portion of short wavelength radiation reaching the eyes of the drivers was significantly higher with the DS lighting system in Study 1 and Study 2. Summarising these results highlights the fact that during daytimes with reduced daylight levels, the amount of light as well as the portion of short wavelength radiation entering the eyes could significantly be increased with the additional in-vehicle DS lighting system.
While the DS intervention used in the present study was perceived as less familiar and more obtrusive compared to the placebo AR intervention, both were rated as equally pleasant by the drivers. Importantly, participants further reported no visual side-effects (e.g. veiling reflections, direct glare, visual distraction, impaired vision) while driving under the adaptive DS lighting system. This confirms and highlights the feasibility of the DS light intervention under natural driving conditions.
4.2 Impact assessment of the light intervention
A central strength of the present study is that it provides novel evidence of a positive impact of additional in-vehicle lighting on directly increasing the alertness of drivers, indicated by reduced alpha spindle rates, under natural driving conditions in the morning.
Research has shown that the alpha spindle rate is highly correlated with a driver’s selective attention performance. 54 There is also evidence 55 that higher alpha spindle rates are associated with reduced driving performance (e.g. prolonged brake reaction times). Furthermore, compared to power in the EEG alpha band, alpha spindle rates are less vulnerable to artefacts and are more sensitive in characterising the current alertness of drivers. However, this alerting effect of additional in-vehicle lighting was not observed during the evening drive. Furthermore, the light intervention did not affect alertness levels quantified by subjective ratings and a PVT immediately after driving in both studies. However, subjective alertness was decreased during the break compared to before the drive, and psychomotor vigilance (reaction speed) was improved at the end of the drive compared to before the drive in the morning and the evening under both interventions. Several factors may have influenced these results.
It is plausible to state that the following two requirements have to be fulfilled for an in-vehicle light intervention to increase alertness: (1) the current alertness level of the driver must be reduced, and (2) the driver must be exposed to relatively low levels of natural light over an extended period of time. Both requirements were fulfilled in Study 1, but probably not in Study 2.
In Study 1, participants may have started the drive with a reduced alertness level 56 because test drivers had shorter sleep durations the night before (5.75 hours on average; D1.3, Supplementary Data). Further indicators that participants drove under reduced alertness levels, at least during the first half of the morning drive, could be seen in subjective ratings of sleepiness and psychomotor vigilance parameters. Contrary to expectations, subjective sleepiness did not rise steadily during the monotonous 2-hour motorway trip but was higher only during the break. Additionally, reaction speed (PVT) was higher after the drive compared to at the beginning of the drive in both experimental conditions. As was expected, though, drivers in the placebo condition showed a reduced reaction speed and, thus, were less vigilant after the monotonous 2-hour motorway drive. Taken together, it remains unclear if the documented alerting effect of the additional in-vehicle light in Study 1 was primarily due to the reduced alertness levels of drivers at the start of the test drive in the early morning.
In contrast, participants in Study 2 reported normal sleep duration the night before (on average 7.0 hours; D2.3, Supplementary Data), but, similar to Study 1, reported higher sleepiness during the driving break (compared to the beginning and end of the drive) and showed an increased reaction speed after the drive. In the second study, however, no direct alerting effect of additional in-vehicle lighting could be observed. Higher mean reaction speed on the PVT and lower KSS scores before the drive in the evening compared to the morning drive may indicate a potentially higher alertness level of drivers before the drive in the evening.
It can further be hypothesised that two light exposure-related factors may have contributed to the lack of direct alerting effects of additional in-vehicle lighting in Study 2. First, the effective light intervention duration in the evening was significantly shorter than in the morning drive (five 6-minute periods in Study 2 and nine 6-minute periods in Study 1, respectively; Tables 3 and 4). Although it has been reported 57 that bright light affects the human circadian system in a non-linear manner (i.e. a short bright light exposure exerts a stronger effect than an extended bright light exposure), a non-linear dose–response relationship for daytime alerting effects of bright light is currently not known.21,58 Second, participants in Study 2 were also exposed to daylight before the drive started, whereas those in Study 1 did not receive any daylight exposure in the early morning before the drive. It is well known that non-visual light effects (e.g. nighttime melatonin suppression and circadian phase shifting) are modulated by the photic history (i.e. the amount of light exposed in the previous hours before the actual light exposure takes place). 59 Taken together, it remains open for future studies to elucidate the impact of an extended light exposure period and of a more controlled daytime light exposure history on the potentially alerting effects of additional in-vehicle lighting.
4.3 Limitations of our studies
In the present study, direct effects of the adaptive DS lighting system were investigated during specific daytimes (i.e. civil twilight and subsequent short periods with reduced daylight levels). We did not quantify light intervention effects during the night and during periods of high daylight levels primarily because additional in-vehicle lighting during nighttime driving increases the risk of impairing visual performance of drivers under scotopic viewing conditions and may also negatively affect the circadian system. As a consequence, light impact research in cars during the night has primarily been conducted in driving simulators.39,40
It can be hypothesised that increasing in-vehicle light levels during periods of high daylight levels may not evoke arousal effects due to four reasons. First, natural corneal light levels of drivers are high on sunny days (2900 lux; as reported in our unpublished research) and adding light may not have an arousing effect. Second, the additional photic stimulus must have a restricted strength to avoid glare while driving. In the present study, the light intervention generated a maximum corneal illuminance of 1320 lux. To increase the non-visual potency of the light stimulus, we used blue enriched white light, which may induce a potentially stronger alerting effect than white polychromatic light alone. 60 Third, daytime alertness levels are generally high and thus may not be increased by additional light exposure. Finally, research shows mixed results on alertness-related effects of bright light above 1000 lux in healthy, well-rested participants.21,61
Transferability of the present study results is restricted because starting time of drives were coupled to sunrise and sunset times to control the period of additional light exposure. However, commuters typically begin their trips at fixed daytimes, and driving starts are not related to sunrise and sunset times. Consequently, the in-vehicle lighting system would be inactive when commuting takes place during darkness hours (e.g. in months with shorter daylight periods) or would be at its maximum illuminance with yet unknown arousing effects when it is bright outside (e.g. in summer months with sunset and sunrise times hours before or after commuting times). Furthermore, the impact of shorter and longer light intervention periods remains unknown.
Usability of the light intervention in our study is restricted as well because the installation of the luminaire necessitated the removal of the sun visor. To avoid dazzling the participants in our studies, the drives took place under low sun elevation angles. Additionally, we carefully selected the driving route on the motorway (mainly north-south with the sun in the peripheral visual field of drivers). However, drivers typically use the sun visor to reduce glare when driving towards the rising and setting sun in the morning or evening. Increasing in-vehicle light levels for drivers during this period would not be necessary considering the natural outdoor lighting. In future research, the in-vehicle light intervention should be miniaturised to be integrated into the sun visor and automatically deactivated when the driver uses the sun visor.
5. Conclusions
Developing in-car countermeasures to prevent sleep- and attention-related crashes is and will remain a challenge. In-vehicle light exposure as an alternative intervention is still novel and must be applied carefully to avoid impairing the vision of drivers. The current studies demonstrate the feasibility of an adaptive DS lighting system and deliver first evidence of direct alerting effects of this intervention on a physiological level. Future studies are warranted to explore light effects on driving parameters. More research is also needed to substantiate reported acute alerting effects of light while driving during the day.
Supplemental Material
sj-pdf-1-lrt-10.1177_1477153520982371 - Supplemental material for Feasibility and acute alerting effects of a daylight-supplementing in-vehicle lighting system – Results from two randomised controlled field studies during dawn and dusk
Supplemental material, sj-pdf-1-lrt-10.1177_1477153520982371 for Feasibility and acute alerting effects of a daylight-supplementing in-vehicle lighting system – Results from two randomised controlled field studies during dawn and dusk by M Canazei PhD, W Pohl MSc, S Schüler MSc, D Betz PhD, J Ottersbach MSc, R Popp PhD in Lighting Research & Technology
Footnotes
Acknowledgements
We are grateful to Johannes Böhringer for his assistance in integrating the two interventions into the test cars and supporting data collection in the two field studies. In addition, we would like to thank Siegfried Rothe for several critical discussions about the two interventions and the study design. Finally, we further acknowledge Stefan Wolf and Christoph Schierz of the Technical University Ilmenau for providing ‘LuxBlick’ measurement devices for the study.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sebastian Schüler and Daniel Betz are employees of Daimler AG; Markus Canazei, Siegmund Staggl, Wilfried Pohl, Julia Ottersbach, and Roland Popp declare no potential conflicts of interest with respect to the research, authorship and/or publication of this paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.