
Abstract
Reducing healthcare-associated infections is critically important. A new hybrid lighting system technology, designed to provide both visible white light and disinfecting UV-A (λmax = 366 nm) radiation, was retrofitted into a modern hospital newborn intensive care unit. The UV-A dosing was set to levels calculated to be safe for human occupation (maximum of 10 W m−2 for 8 hours at eye level). Eight-hour exposures at 3 W m−2 on newborn intensive care unit counter surfaces were effective for suppressing selected pathogens identified by the Centers for Disease Control and Prevention as problematic for healthcare facilities. Professional staff accepted the hybrid lighting system, although its implementation in this newborn intensive care unit was not completely satisfactory. An analysis of photodegrading effects suggested that UV-A resistant equipment and furnishing may need to be installed with this technology. The present findings should form the foundation for the next generation of this lighting technology.
1. Introduction
Hospital patients are at risk from infections acquired there. Approximately 1 in 25 patients in the United States contract healthcare-associated infections (HAIs). 1 Patients are particularly at risk if the previous patient in that room had an infection.2,3 Standard cleaning procedures usually involve manual application of detergents and disinfectants. 4 The efficacy of these manual cleaning procedures can vary considerably among hospitals.5,6 In fact, less than 50% of the patient room surfaces are properly cleaned. 1
Given the rather poor effectiveness of manual cleaning, the efficacy of alternative, so called, no-touch methods have been examined with the expectation that decontamination of room surfaces will improve when the human element has been removed. Among these no-touch methods, the efficacy of short-wavelength optical radiation, from ultraviolet (UV) to blue light (200 nm to 410 nm), has been studied.7–9 Short wavelengths can kill pathogens through a variety of pathways, depending upon the wavelength, the duration, and the amount of optical radiation. 10 UV-C (100–280 nm) at 100 J m−2 can fuse DNA base pairs and can produce reactive oxygen species, both of which are lethal to the pathogen. 11 UV-A (315–400 nm) and blue light (approximately 380–410 nm) can also produce reactive oxygen species, but more energy needs to be absorbed by the pathogen to kill it.12,13 The advantage of UV-C technologies for minimizing HAIs is that effective dosage can be achieved with short time durations (<1 hour) 14 ; the disadvantage of UV-C is that the optical radiation must be applied when the hospital room is unoccupied. For UV-A and blue light applications, several hours of exposure may be needed to effectively reduce pathogen presence, but, depending upon the wavelength and dose, people can occupy the room without harm.
With regard to human safety, exposure to UV-A can cause erythema of the skin (reddening). For wavelengths longer than about 350 nm, however, erythemal effects are negligible. 15 Exposure to blue light wavelengths longer than about 380 nm can cause permanent damage to the retina; this phenomenon is known as blue light hazard. 16 Unlike erythemal effects, which depend upon irradiance on the skin, the radiance of the source must be minimized to avoid blue light hazard,16,17 so unless an image of the source is formed on the retina, little damage to the retina will occur from blue light exposure. According to industry standard safety recommendations 18 however, exposures to UV-A wavelengths between about 350 nm and 380 nm can be considered safe for humans at doses that would still be effective for reducing HAI pathogens.
Short wavelengths can also affect non-living materials. Materials with fugitive pigments, including watercolor paintings and organically dyed textiles, can fade or discolour after exposure to short wavelengths. 19 Further, short wavelengths can induce fluorescence (glowing) from some materials, particularly fabrics that have been washed in detergents containing bluing agents. Subjective judgments of materials within a space irradiated with short wavelengths could logically be affected by the dominant blue colour of the illumination or by ‘unnatural’ fluorescence of materials within the space.
The present field study was designed to evaluate a hybrid lighting technology that could provide both visible white light and UV-A optical radiation. The site for the study was a recently built newborn intensive care unit (NICU). Three types of assessments were performed: (a) an assessment of the UV-A exposure for mitigating pathogens found in this unit, (b) examination of UV-A potential for photo-degradation of materials, and (c) subjective assessments of the lighting system by professional staff within the unit. Occupant exposure safety was implemented by applying published safety limits 18 for UV-A exposures and confirmed through radiometric measurement.
2. Method
2.1 Study site
The field study was conducted in the NICU at the Memorial Beacon Children’s Hospital in South Bend, Indiana, USA. This 39-bed NICU provides an advanced level of care for babies born prematurely or with a critical illness. The facility was designed and built in 2017 to minimize an institutional appearance. For example, rather than caring for multiple babies in one ward, premature babies have private patient rooms (Figure 1). These patient rooms include a private lounge, sleeping, and bathing facilities for each family. Each patient room has a separate sink and counter surface for families and medical staff. The sink and counter area in the patient rooms were the primary focus for assessing UV-A mitigation of pathogens because these high-touch areas are most likely to contain human-borne pathogens.
Typical patient room sink and counter before retrofit with hybrid lighting system; each patient room serves one family and their infant(s) (available in colour in online version)
The study was conducted in six of the NICU patient rooms. With regard to the lighting, some daylight was available in the patient rooms, but most of the ambient illumination was provided by ceiling- and wall-mounted luminaires. These luminaires included a diverse collection of recessed downlights and colour-changing cove lights near the sink (Figure 1, left). Equipment-mounted uplights were also part of the lighting design (Figure 1, right).
2.2 Cleaning
Nurses work in 12-hour shifts, either 07:00–19:00 or 19:00–07:00. At the start of each shift (morning and night), nurses clean the sink and counters (PDI Super Sani-cloth germicidal disposable wipes). Once a day, environmental cleaning crews attempt to sanitize the many surfaces in each patient room, including the sink area (Diversey Oxivir 1 Wipes); environmental cleaning staff are not responsible for cleaning the counters.
2.3 Hybrid luminaires
The hybrid luminaires (‘Lumination’ LBU 22 Disinfection Series D-Light, manufactured by GE Current, a Daintree company) were surface mounted in the patient rooms above the counter and sink areas after the existing luminaires in that area were removed. The hybrid luminaires had two circuits that could be used independently (Figure 2). White light was provided by conventional light-emitting diodes (LEDs) controlled by the occupant using a dimmable wall switch. The UV-A LEDs were controlled by the manufacturer on a separate circuit using a remotely programmed time clock. At maximum output, each luminaire had a power demand of 18 W for white light, but due to occupant operated wall-mounted dimmers, the luminaires may have drawn less power during the study. The UV-A channel is capable of drawing up to 111 W per luminaire, but for this particular study, they were operated at 50–70% output to meet industry safety standards
18
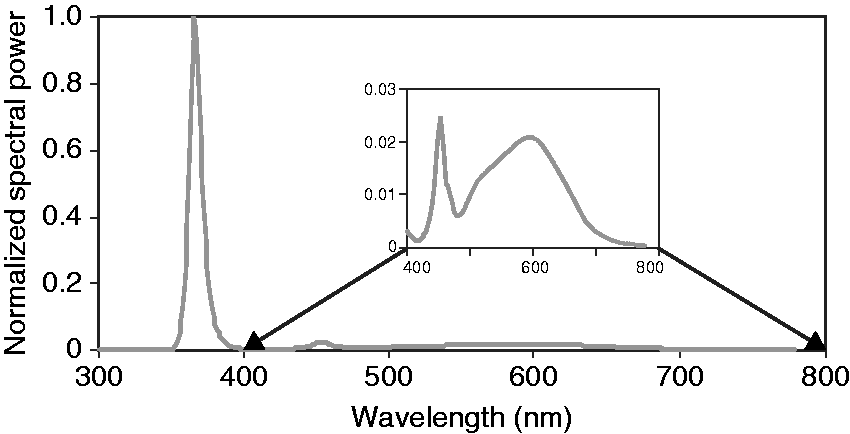
for this application. The spectral power distributions (SPDs) of the two luminaire channels are shown in Figure 3. The hybrid luminaires produced a diffuse luminous intensity distribution.
Typical sink and counter space with the hybrid lighting system, providing white light (left) UV-A (centre) and both (right). The UV-A and the white light could be energized with separate circuits (available in colour in online version) Relative SPDs of the two hybrid lighting LED channels, UV-A (λmax = 366 nm; full width half maximum = 9.4 nm) and white light (correlated colour temperature = 3870 CCT, colour rendering index = 84, gamut area index = 72). The inset (400–800 nm) shows the SPD for the white light on the same relative scale as the main plot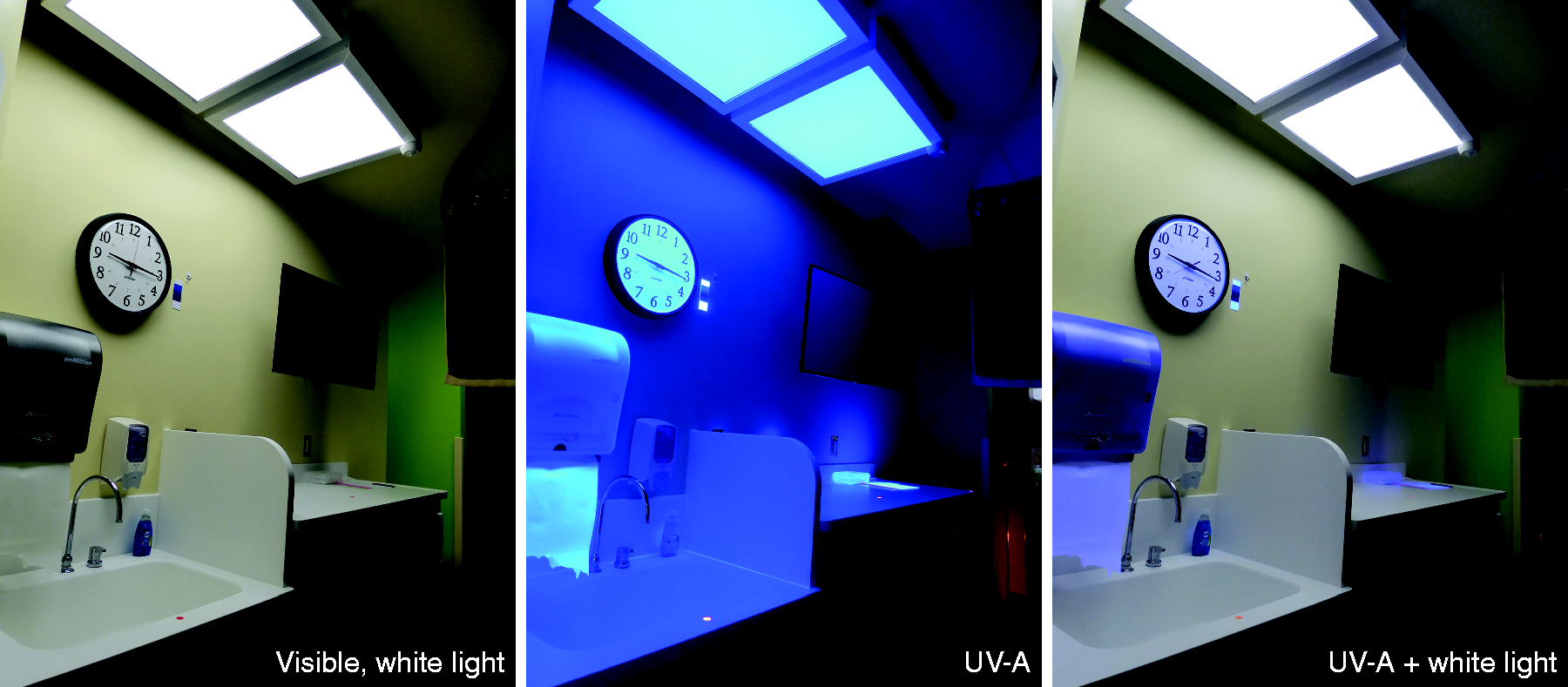
2.4 UV radiation safety
For human safety, the manufacturer relied on IEC Standard 62471:2006, ‘Photobiological Safety of Lamps and Lamp Systems’. 18 Standard 62471 gives thresholds for near-UV (UV-A; 315–400 nm), far-UV (actinic; 200–400 nm), and blue light (300–700 nm) exposures. For near UV, the irradiance limit is 10 W m−2 on the skin or at the eyes for 8 hours and for actinic UV, the actinic-weighted irradiance limit is 0.001 W m−2, also for 8 hours on the skin or at the corneas. For blue light imaged on the retina, however, the exposure duration and the radiance of the source, rather than irradiance of the source at the eyes, are critical for estimating blue light hazard.16,17 So diffuse, low-radiance sources like those exhibited by the hybrid lighting system pose no blue light hazard risk.
The white light and UV-A radiation in the patient rooms was modelled using photometrically accurate calculation software (AGi32 version 19, by Lighting Analysts, Littleton, Colorado, USA). The hybrid lighting system’s diffuse, approximately Lambertian luminous intensity distribution would produce the greatest irradiance directly underneath the fixture. A person standing directly beneath the fixture would therefore receive the highest UV-A dose. Anticipating this possibility, the modelled UV-A radiation emitted by the hybrid lighting system was limited to 10 W m−2 at 6 ft (2 m) above the finished floor plane, corresponding to an eye height of a very tall person. Consequent to this safety limit, these luminaires would produce UV-A irradiance levels of approximately 3 W m−2 at counter and sink heights of 3 ft (0.9 m) above the finished floor plane. Because Standard 62471 does not provide safety guidelines for exposures longer than 8 hours in a single day, the duration of UV-A operation for this study was limited to 8 continuous hours per day.
2.5 Curtains
Despite the fact that the UV-A output was set at levels deemed safe for adults,
18
extra precautions were taken to keep direct UV-A irradiance off the infant patients during the study. Weale
20
showed, for example, that infants’ crystalline lenses transmit more UV-A than older people; thus, greater protective measures are needed for this population.
20
Short, blackout-type curtains were hung in the six patient rooms (Figure 4); the bottom of these curtains was 5 ft 5 in. (1.65 m) above the floor. In addition to curtains, nursing personnel were ordered by the NICU Director to drape baby bassinets/isolettes when occupied (Figure 4).
Examples of curtains in two of the six patient rooms; shown in the foreground of the left image is a baby isolette draped in fabric (available in colour in online version)
2.6 Measurements
Average illuminance (lx) and the associated standard deviation (s.d.) in patient rooms (average of one measurement in each of five or six patient rooms)
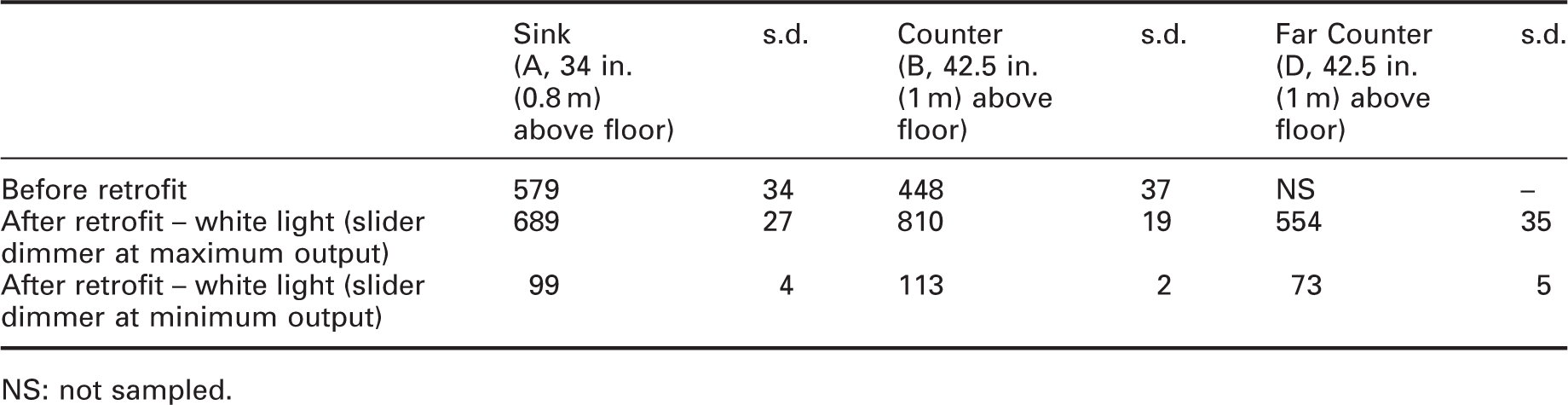
NS: not sampled.
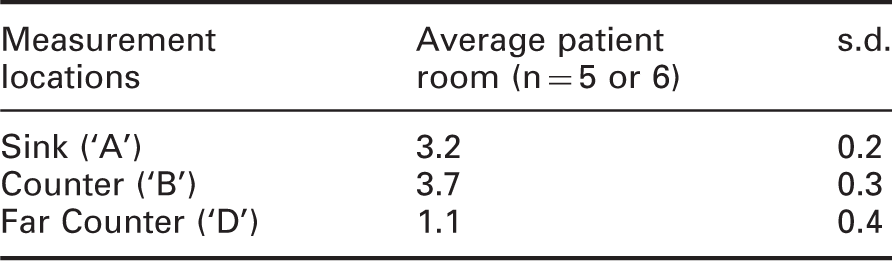
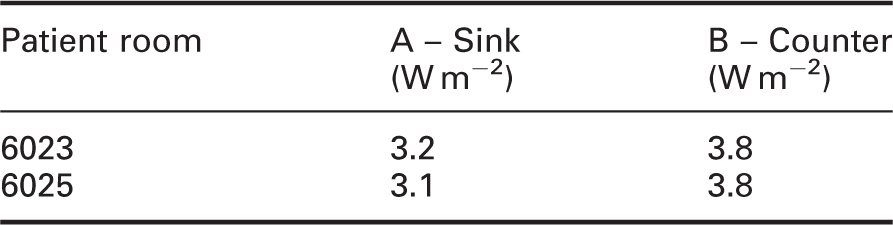
Average irradiance levels (W m−2) and associated standard deviation in patient rooms (none exceeded 10 W m−2 at 6 ft (1.8 m))
The white-light illuminance levels (Table 1; Gigahertz-Optik BTS256-E) and the UV-A irradiance levels (Table 2; Gigahertz-Optik BTS2048-UV-S) were measured before and after installation of the hybrid luminaires in the patient rooms. Similar illuminances were available at the sink (‘A’ in Table 1) before and after retrofit. At patient room counters (‘B’ in Table 1), illuminances at full output were higher after the retrofit.
As shown in Table 2, radiometric measurements confirmed the modelled irradiance level of 3 W m−2 at the primary locations (Sink ‘A’ and Counter ‘B’). Ancillary spaces far from the UV-A luminaires had lower irradiance levels (i.e. far counter ‘D’ in patient rooms).
3. Protocol
3.1 Schedule
The one-week protocol was repeated three times (15–20 April, 6–11 May, and 14–18 May 2019) with the hope that during one or more weeks, pathogens would be present for sampling. In advance of each data collection week, three patient rooms that would be occupied were identified and provisions were made to energize the hybrid luminaires for those rooms. Except for the second week when all rooms were occupied, one vacant room was also included for evaluation. The UV-A sources were programmed to operate 09:30–17:30 each Wednesday and Thursday in the patient rooms (i.e. 8 hours on each of two consecutive days).
ATP samples (detailed below) were collected Monday through Saturday of each study week. During the first week, however, insufficient numbers of available ATP testing materials led to reduced testing, resulting in two days of UV-A exposure for three patient rooms, and one day of exposure for one patient room. At each measurement point, ATP was sampled at least three times per day; in some cases, ATP sampling was repeated after cleaning times. ATP was sampled mornings (mean time = 08:37; range = 07:44–09:31), evenings (mean time = 17:28; range = 14:51–18:12), and midnight (mean time = 23:52; range = 23:31–0:17). There were a total of 746 ATP samples collected in the patient rooms over the three weeks.
3.2 Cleaning adjustments
Day-shift nurses normally start their shift by cleaning, but when the researchers were attempting to sample before and after cleaning, nurses slightly delayed their cleanings in collaboration with data collection procedures.
3.3 ATP sampling
Naturally, the presence of freely occurring organisms was measured, rather than introducing pathogenic materials into this active NICU.
ATP is present in all organic material. ATP sampling is practical, inexpensive ($3.63/sample), and useful for assessing hygiene. 21 ATP samples were obtained using surface swabs (Neogen, Lansing, Michigan) and then measured with a reader (AccuPoint Advanced HC; Neogen). ATP counts above 300 relative light units (RLU) are considered above the threshold for cleanliness in this NICU. It should be noted that in routine quality control testing, this NICU often had the lowest ATP values in the entire hospital.
The ATP sampling locations were defined by metal templates placed at the same positions on the tops of the sinks and counters. During data collection, the template was moved from point to point and from room to room, and cleaned after use in each room using the Sani-cloth wipes.
3.4 Inoculated culture plates
To directly assess the efficacy of the UV-A exposures, three pathogen types were selected for study based upon the following three criteria:
A pathogen previously identified as present in this NICU A pathogen identified by the Centers for Disease Control and Prevention (CDC) as among the top 10 pathogens of concern for HAIs
22
A pathogen identified by the NICU Director as particularly problematic
The pathogens selected for the follow-up study were as follows:
Enterococcus faecalis, a bacterium that causes, most commonly, urinary tract infections. This bacterium is particularly resistant to antibiotics. Staphylococcus aureus, a bacterium associated with upper respiratory infections.
23
Escherichia coli, a diverse group of bacteria that can cause a variety of maladies including severe dehydration.
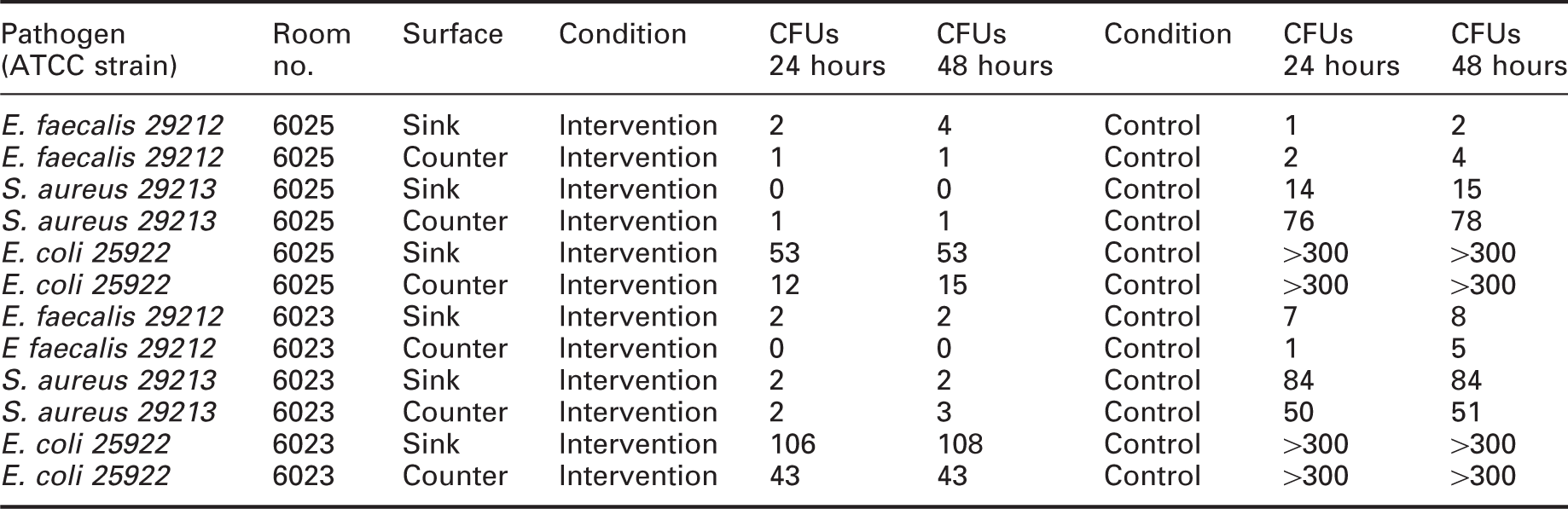
Cultures of a given pathogen type were divided into two groups. A control group was placed on culture plates covered with a transparent, UV-blocking cover (Steiner #334 film) and an intervention group was placed on culture plates covered with the usual borosilicate, UV-transparent cover plates (Figure 5). The two groups were placed at the same locations that were selected for the previous ATP sampling (patient rooms 6023 and 6025, sink and counter). The hybrid lighting system with the UV-A source energized was operated as it was before, that is continuously for 8 hours at approximately 3 W m−2 (Table 3). For a given pathogen type, the culture plates with the UV-blocking covers (control group) were expected to exhibit significantly higher colony forming units (CFUs) than the same pathogen type grown in culture plates with UV-transmitting covers (intervention group).
Inoculated culture plates at a patient room sink (left) and counter (right); borosilicate glass covered all test plates, and additional orange-coloured UV-blocking film covers each control group (available in colour in online version) Irradiances at two measurement locations, in two rooms, during the inoculated culture plate experiment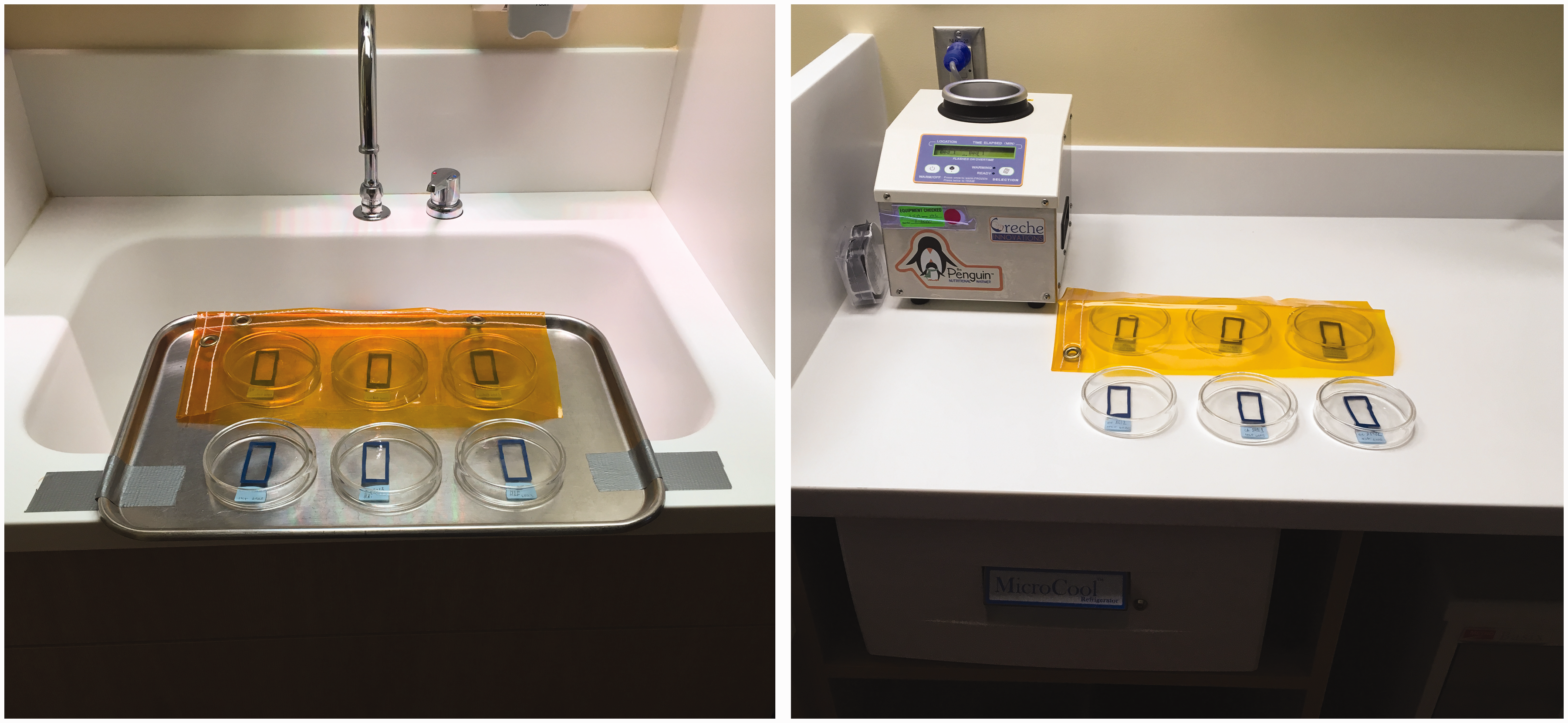
3.5 Photodegrading effects
Two ISO Blue Wool Standard fade test cards (TALAS, Brooklyn, NY, USA) were mounted next to the wall clock in each patient room. The tops of the test cards were 25 in. (63.5 cm) below the hybrid lighting system (Figure 6, left). Based on the computer modelling, irradiances on the fade test cards were estimated to range from 4.2 W m−2 to 4.7 W m−2. A Blue Wool card consists of eight, juxtaposed blue-dyed strips of different lightfastness (Figure 6, right). The strips were numbered 1 through 8, with 1 being the least colourfast strip and 8 being the most colourfast strip. According to the manufacturer, each successive strip takes approximately two to three times longer to fade than the previous strip when illuminated by sunlight. One test card remained mounted in each room for the entire duration of the study (‘long-term’, 71 days). The second test card was only mounted on the wall for the first week of the study (‘short-term’, 5.5 days). A single Blue Wool test card was kept in the dark for the duration of the study to serve as reference for computing colour change of the other strips.
Examples of the Blue Wool test cards in situ (left, indicated by arrow) and in detail (right), including colourfast level designations (1–8) (available in colour in online version)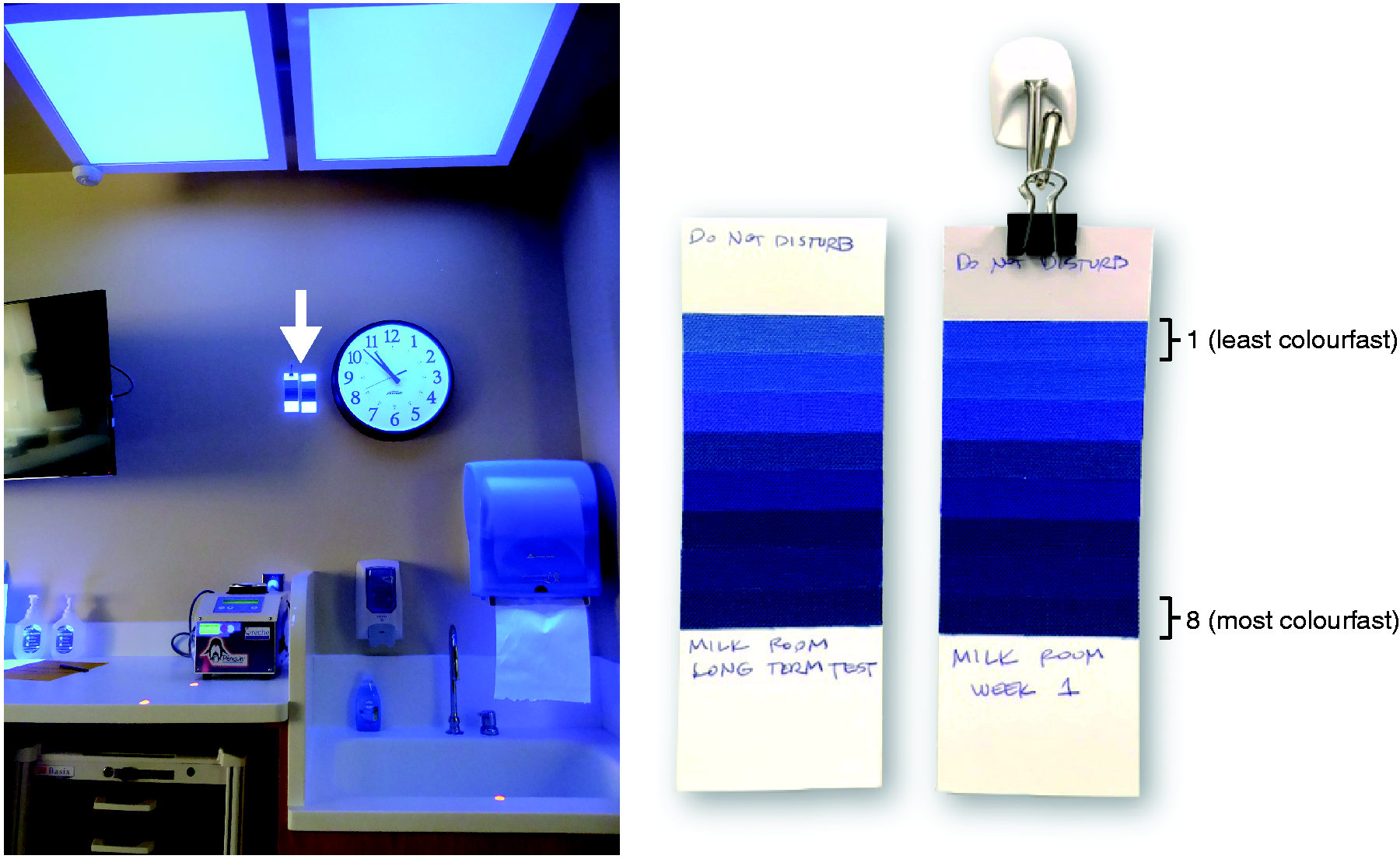
After both the long-term and short-term exposures, a Blue Wool card was placed in a light-tight container and returned to the laboratory for spectral reflectance measurements. A spectroradiometer (PhotoResearch PR740) was used to measure spectral reflectance factors from 380 nm to 780 nm for 0° incident angle and 45° viewing angle. Spectral reflectance values were calibrated to a Spectralon® white reflectance standard (Labsphere SRT 99-050) illuminated by a tungsten-halogen source (Phillips EHD 500 W/120 V) positioned 4 ft (1.2 m) from the sample.
3.6 Staff questionnaires
Staff lighting questionnaire before and after retrofit, in patient rooms
4. Results
4.1 ATP sampling
ATP samples were obtained from three surfaces in 3–4 patient rooms for each of the three weeks. The raw RLU data were plotted on a logarithmic ordinate for visual clarity; to show all of the data on the log-scale ordinate, a value of 1 was added to every measurement. There was wide variation among the samples, making it difficult to draw inferences about the efficacy of any intervention. Indeed, the incidence of organic material was low, usually lower than the hospital threshold for ‘clean’ of 300 RLU. This, of course, is very good news for families, physicians, and staff in the NICU, but such a clean environment makes it difficult to draw inferences about the efficacy of the UV-A intervention in this environment.
Figure 7 illustrates the method used to assess the efficacy of the UV-A intervention, in terms of the change in sampled RLU values. ATP samples were obtained in the early evenings (mean time = 17:50; range = 17:33–18:12) each of six days for three weeks in occupied patient rooms. Early evenings correspond to the time at the end of the UV-A application on Wednesdays and on Thursdays. To determine if the 8-hour (09:30–17:30) UV-A exposure from the hybrid lighting system was effective, the change in ATP counts was determined relative to those collected on the previous evening at the same time. The slopes of these changes were determined ((Day n + 1 − Day n)/Day) for each of the sampled counter and sink areas underneath the hybrid luminaire. The number of negative slopes relative to all slopes for each 24-hour interval (≈18:00 to ≈18:00) was determined. The probabilities of obtaining a negative slope relative to all slopes were determined from a binomial distribution along with the probabilities of a Type I error. The proportion of negative slopes relative to all slopes for each week are shown in Table 5 along with the associated probability of a Type I error when the data for all weeks were aggregated.
Example ATP results, measured in RLUs, for one location (sink), in one room (6024), for one week (week 3). The solid line indicates the change in RLU values on a log scale for each successive ATP sample. Solid dots illustrate the RLU values obtained each evening at approximately 18:00; the dashed line indicates the evening-to-evening slope changes used in Table 5. Vertical lines indicate midnight of each day. Shaded areas indicate UV-A exposure periods. ATP: adenosine triphosphate Based on ATP sample counts collected in occupied patient rooms on successive afternoons (circa 18:00), the proportion of sample count reductions (negative slopes on successive days) relative to all changes (positive, negative, or no slope changes) each week ATP: adenosine triphosphate; NS: not sampled; UV: ultraviolet. aPatient room 6023 only had the UV-A sources on for one day, so the Wednesday–Thursday (two days of UV) values were moved to Thursday–Friday (no UV). Significant positive slope.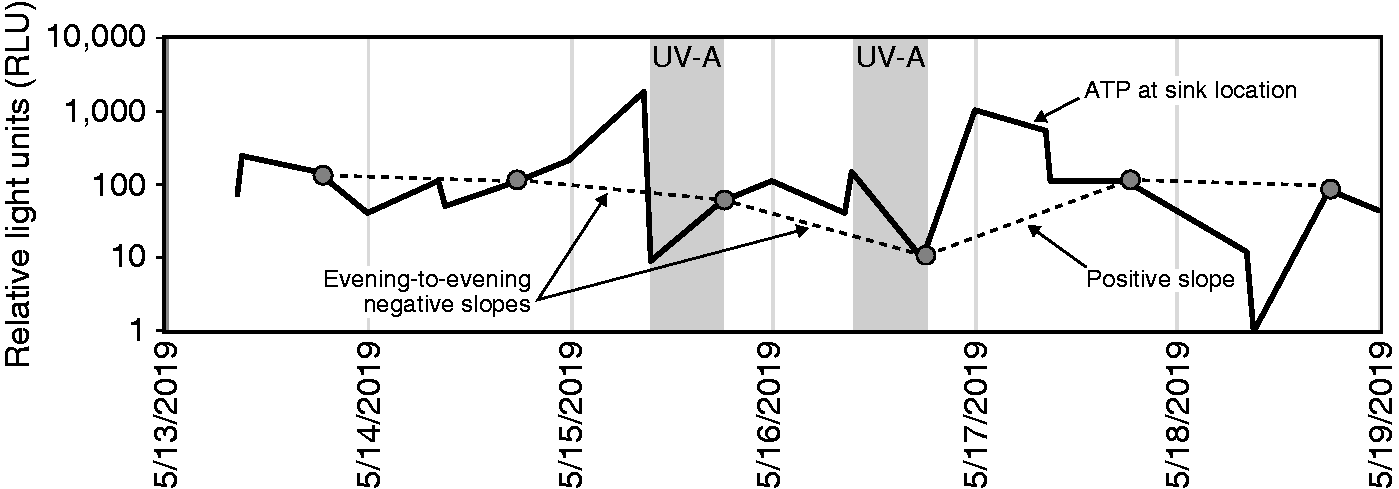
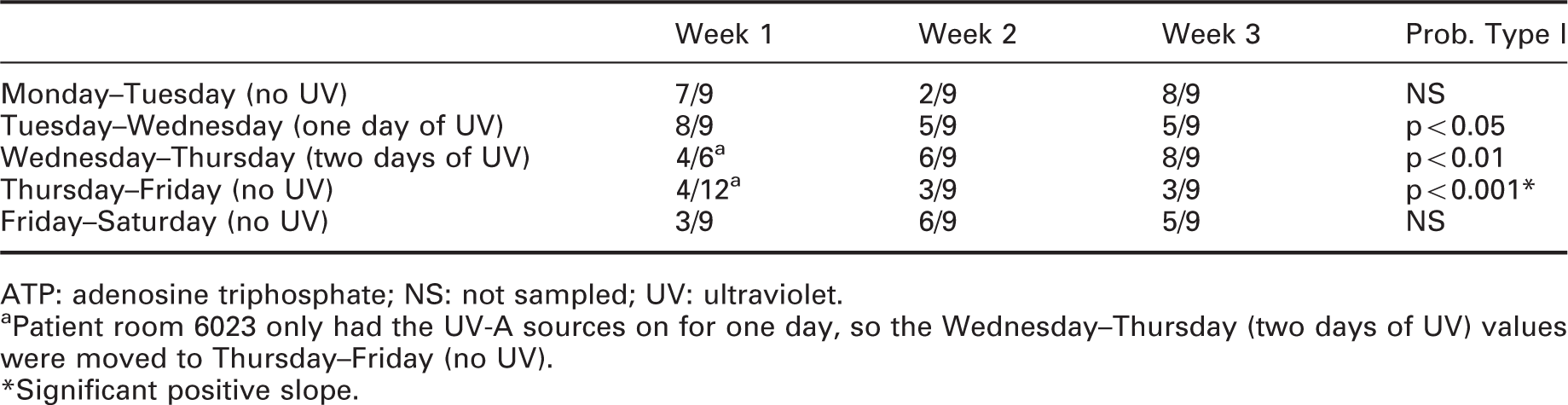
Table 5 shows exactly what would be expected if the UV-A exposure was effective in reducing the pathogen burden. For Monday to Tuesday and for Friday to Saturday when the UV-A sources were not energized, there was no aggregated slope change in the ATP counts, indicating that the existing afternoon cleaning procedures were all statistically equally effective. After 8 hours of the UV-A application on Wednesday, however, there was a statistically significant reduction in ATP counts which, in turn, was reduced even more from Wednesday to Thursday after two days of 8-hour UV-A exposures. Importantly, when the daily 8-hour exposure of surfaces by the UV-A radiation was discontinued from Thursday to Friday, there was a statistically significant increase in ATP counts.
4.2 Inoculated culture plates
Table 6 shows the results of cell culture plates inoculated with the three pathogens in two patient rooms. Using the combined data, Student’s one-tailed t-tests comparing the UV-transmitting (intervention) and the UV-blocking (control) cultures showed statistically significant CFU reductions for E. faecalis (t(5) = −1.98, p = 0.05), S. aureus (t(3) = −3.52, p = 0.02), and E. coli. (t(3) = −12.58, p = 0.0005). It should be noted that although the culture counts were greater than 300 CFUs for E. coli in the control (no UV-A) condition, 300 CFUs was the value used for the statistical comparison. Following microbiological convention, Figure 8 shows these results in terms of per cent CFU reduction; this shows the differential impact of the UV-A intervention relative to the control for all three pathogens.
Average CFU per cent reduction (1−(Intervention/Control) × 100) following ≈3 W m−2 exposures of UV-A; error bars indicate standard deviation. CFU: colony forming unit Inoculated culture plate results, colony forming units (CFUs) at 24 and 48 hours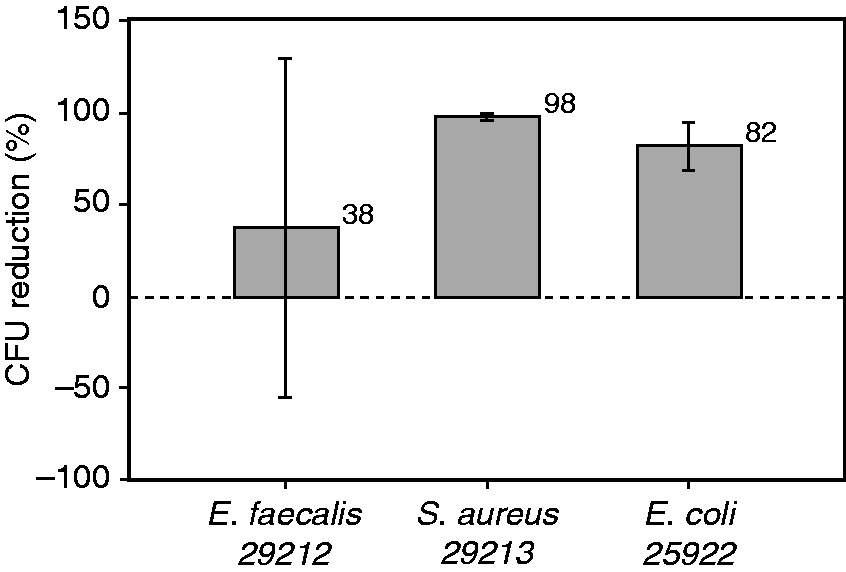
4.3 Photodegrading effects
Colour changes to the Blue Wool strips relative to the reference strips held in the dark were determined using a standard method recommended by the Commission Internationale de l’Eclairage. 24
Inherent colour differences between the spectral reflectance values of the reference strips and the test strips limit precise estimates of colour changes due to the light and UV-A exposures. From a visual inspection of the test strips, there seemed to be reliable colour shifts from the patient rooms only for test strips 1 and 2. Indeed, a linear regression analysis for colour change as a function of cumulative UV-A sources operation showed significant slopes for only test strips 1 and 2 (Figure 9, p = 0.046 and 0.014, respectively). All other test strips for the initial week and long-term durations had non-significant slopes at the p < 0.05 level.
Colour change vs cumulative UV-A exposure time for Blue Wool test strips 1 (a) and 2 (b) that had linear regression slopes significantly different than zero. Strips placed in a common area (‘Milk Rm’) were irradiated for 118 hours; these data are included for the regressions. The significant non-zero y-intercepts (p < 0.001) presumably represent the colour change due to the LED room lighting alone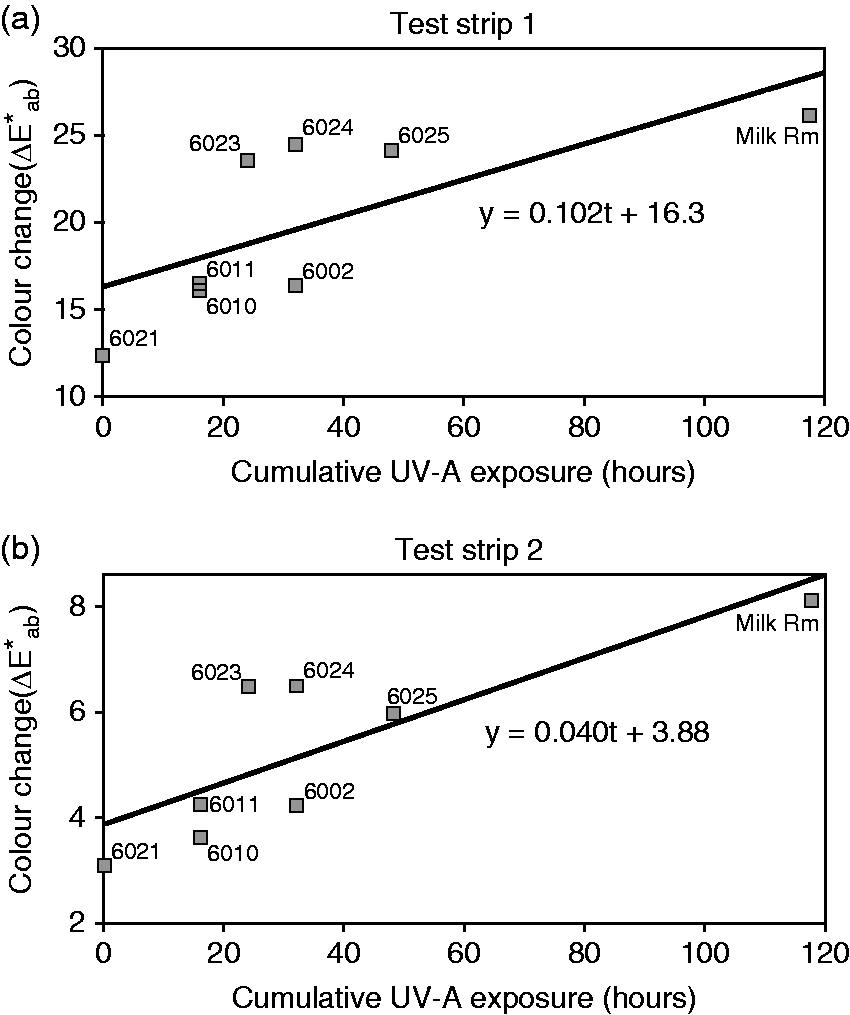
4.4 Staff questionnaires
Before retrofit, 34 staff members provided subjective assessments of the lighting in the patient rooms. After retrofit, 19 staff members responded. Staff consistently indicated that they typically spend more than 1 hour in patient rooms.
Average staff responses and the associated standard deviations to Likert scale questions
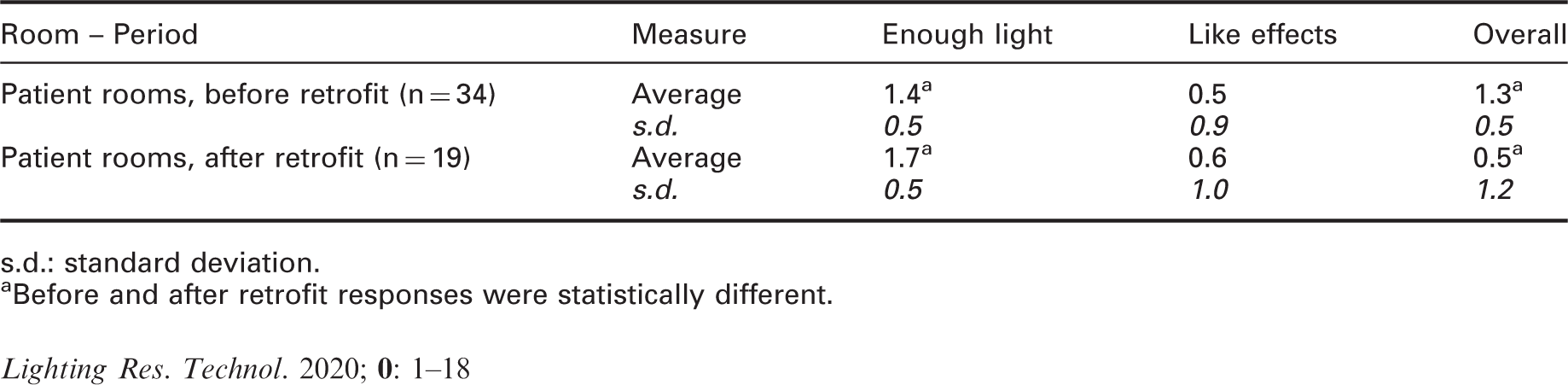
s.d.: standard deviation.
aBefore and after retrofit responses were statistically different.
5. Discussion
5.1 ATP sampling
ATP samples are routinely collected in many units of Memorial Hospital as an inexpensive technique for quality assurance of their cleaning procedures. The hospital NICU studied here is very clean, as reflected in the low ATP counts obtained during this study. Indeed, over the three weeks of the study, ATP counts were rarely over the 300 RLU threshold for cleanliness in this hospital. In fact, the NICU Director reported that his unit consistently receives internal recognition as one of the most consistently clean units in the hospital. To better gauge the level of cleanliness in the NICU, ATP spot checks of public areas in the hospital were sampled. ATP RLU values were as high as 6000 RLU in public areas, supporting the inference that this NICU is particularly clean.
From an experimental perspective, low ATP counts made it difficult to assess the pathogen mitigation efficacy of the UV-A radiation from the hybrid lighting system. Nevertheless, support for the effectiveness of this hybrid lighting technology for killing bacteria was obtained from an analysis of the daily change in ATP counts (Table 5). Without the UV-A radiation, there was no statistically reliable change in ATP counts, but there were statistically significant reductions in ATP counts following the UV-A exposures. And, importantly, stopping the UV-A treatment led to a significant increase in ATP counts. Future demonstrations of the hybrid lighting technology should be undertaken in hospital units with greater bio-burden. Significant reductions in pathogen counts after UV-A exposures should then be related to reduction in HAI incidence.
5.2 Inoculated culture plates
The inoculated cell culture analysis was important for a variety of reasons. First, this NICU was particularly clean, making it difficult to demonstrate the efficacy of the UV-A applications. Second, ATP samples do not differentiate pathogens that might cause HAIs from other organic materials. Third, a side-by-side comparison of cell culture growth, ambient lighting with and without UV-A, must be conducted to unambiguously demonstrate that UV-A exposures affect pathogen growth. Specifically, the side-by-side test conducted here showed that important pathogens identified by the CDC as problematic sources of HAIs and ones actually found in the NICU were directly abated by the UV-A applications actually used in the present field study.
5.3 Photodegrading effects
The Blue Wool test cards had sufficient sensitivity to measure significant colour changes due to the ambient room lighting without added UV-A as suggested by the highly significant positive y-intercept values of the regression of colour change on UV-A exposure (Figure 9). Nevertheless, operating the UV-A circuit contributed significantly to colour changes with rates of 0.1 and 0.04 ΔE*ab per hour of operation for test strips 1 and 2, respectively (Figure 9). These most sensitive test strips, however, are not representative of the actual dyes and pigments found in most décor and building products which typically have much better lightfastness, as do the higher numbered Blue Wool test strips that exhibited no meaningful colour changes over the limited UV-A exposure time available during the study.
As an adjunct to direct measurements using the Blue Wool test, CIE 15724 provides a recognized method for estimating exposure times that produce a just noticeable change in colour based on irradiance, SPD, and the type of material being irradiated. The standard provides material parameters for five categories of museum display materials. Under the assumption that these museum display categories share similar parameters with objects found in hospital rooms, different light sources can be compared based on the exposure times needed to elicit a just noticeable change in colour. The categories are described as follows: (a) low-grade paper (e.g. newsprint), (b) rag paper, (c) oil paints on canvas, (d) textiles, and (e) watercolours on rag paper. These categories exhibit varying absolute and spectral sensitivities with category (a) being the most sensitive to UV-A radiation. Since colour change is proportional to the product of exposure time and spectrally weighted irradiance, critical values of dose, measured in units of lux hours, for a just noticeable colour change (ΔE*ab = 1) can be calculated for combinations of light source spectrum and material category. A lower critical dose means that a shorter exposure time at a particular photopic illuminance level produces a noticeable colour change. These critical values are displayed in Figure 10 for the hybrid luminaire used in the present study (both white light and UV-A sources operating simultaneously) along with three other common light sources in combination with the material categories of CIE 157.
The amount of illumination (critical dose in lux hours) needed to produce a just noticeable change in colour (ΔE*ab = 1) for the hybrid luminaire (UV-A fixture) and three other common light sources. Values were calculated as per CIE 157:2004 (higher bars are better for preserving colour). LED: light emitting diode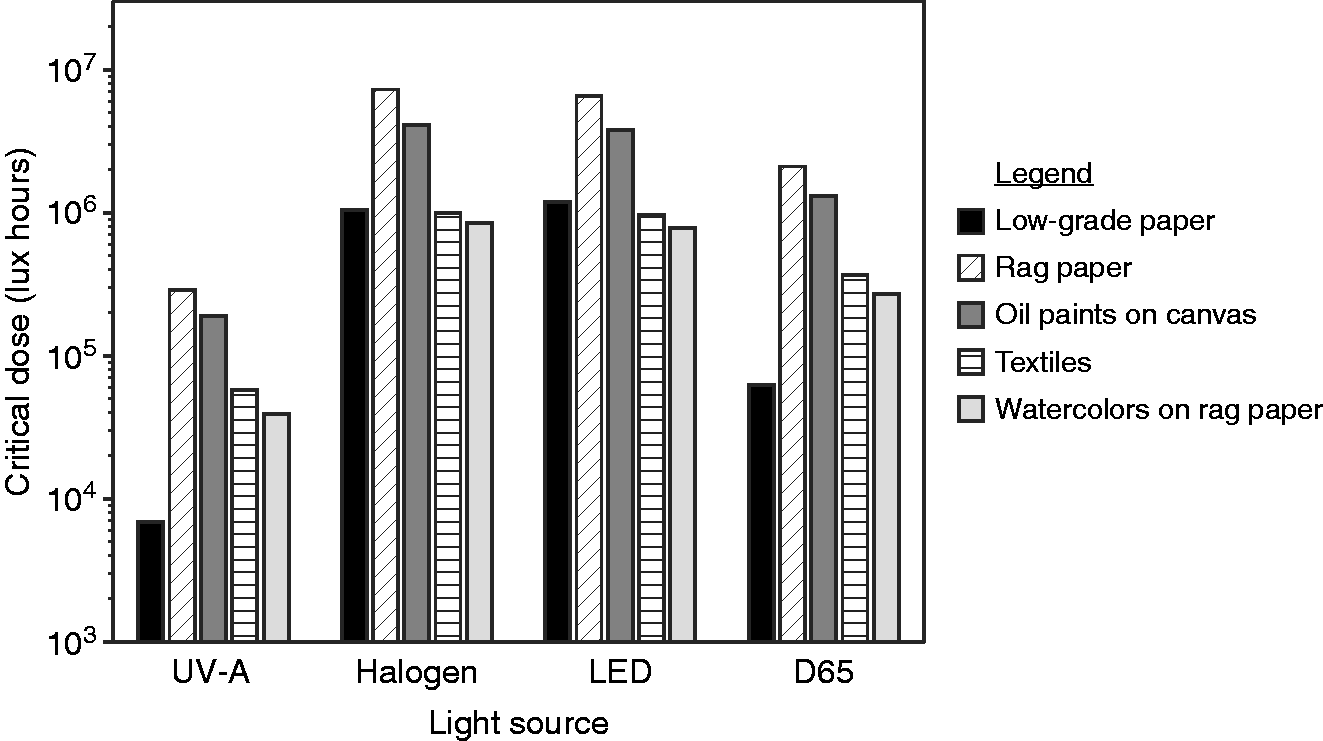
The hybrid luminaire has much smaller critical dose values than the other sources, even daylight (D65), because of the relatively high levels of UV-A. The ratios of critical doses across material categories are nearly the same for the hybrid luminaire and daylight, with daylight being associated with a dose approximately seven times greater to reach a noticeable colour change. The similarity of ratios is attributed to both sources having high amounts of UV-A. Comparing ratios of the hybrid luminaire with halogen and LED sources shows large differences between the low-grade paper (ratios of 150 and 250) and the other materials (ratios of approximately 20) which is explained by the low-grade paper having much higher spectral absorbance in the UV-A region than in the visible while the other material categories have a more uniform spectral sensitivity.
Note that even though the hybrid luminaire has lower critical doses than a daylight spectrum, the irradiance from the hybrid luminaire is much lower than outside daylight irradiance levels. As shown in Figure 11 for an interior illuminance of 750 lux provided by the hybrid luminaire, the critical exposure time for threshold colour change is approximately 1.8 times longer than that for outside daylight levels corresponding to 10,000 lux.
Critical exposure times needed to produce a just noticeable change in colour (ΔE*ab = 1) for the hybrid luminaire (UV-A fixture) at 750 lux vs D65 daylight at 10 000 lux. Values were calculated as per CIE 157:2004 (Higher bars indicate slower colour degradation.)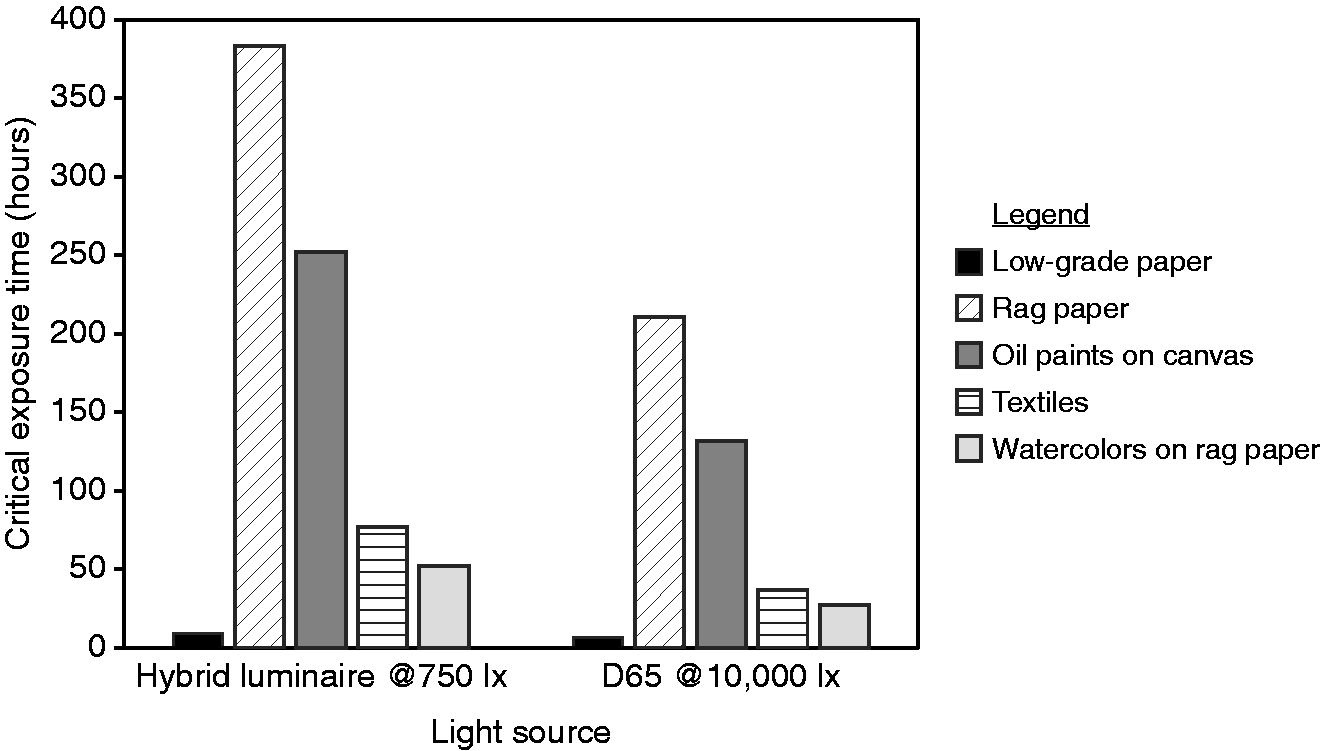
Based upon the measured changes with the Blue Wool test and the calculations using the CIE method, materials insensitive to UV-A should be selected for the hospital environment where the hybrid luminaire would be operating. Future field studies should measure not only direct irradiance, but may also need to consider reflected irradiance for any shiny or mirrored surfaces. 25
5.4 Staff questionnaires
Unprompted comments from the professional staff provide some insight into the results presented in Table 7, showing statistically significant improvement in their ability to see (‘enough light’) but reduced appreciation (‘overall’) of the hybrid lighting system retrofit.
The professional staff did like the higher light levels produced by the hybrid lighting system (e.g. ‘New lighting definitely improves vision significantly in comparison to current lighting’)
The staff were less than enthusiastic about the overall appearance of the patient rooms after the hybrid lighting system retrofit (Table 7, ‘overall’ ratings). As might be anticipated, some staff reacted to the fluorescing materials in the rooms when the UV-A channel was operated (e.g. ‘I don’t like the way it [UV] changes the colour of everything’). Of some surprise, the staff did not like the curtains requested by the NICU Director to shield the infants from the UV-A (e.g. ‘I hate the ugly curtains hanging down’). These rather strong opinions about the curtains probably contributed a great deal to the more negative ‘overall’ ratings of the hybrid lighting system (e.g. ‘I don’t like the curtains at all. Other than that, no complaints’). It should be remembered too, that the retrofitted hybrid lighting system was not fully integrated into the architecture, potentially affecting the ‘overall’ ratings. Finally, the public, including the hospital professional staff, have health concerns about UV radiation in general. These concerns most likely stem from public service messages about the need to shield skin from sun causing erythema and thereby to minimize risk of melanoma (e.g. ‘I really don’t want to be exposed to UV light since I just had eye surgery 13 weeks ago. It sort of hurts my eyes’).
In general, the hybrid lighting system created a unique visual environment for the professional staff. People often have negative reactions to novel stimuli, so perhaps after some time, these effects might seem ‘more natural’. The overall ratings were also negatively affected by the curtains that were installed to block direct exposure of the infants to the UV-A radiation. This intervention, stemming from abundant caution by the NICU Director, reflects the public concern for UV exposure. More effort is needed to demonstrate, if true, the benign nature of the UV-A emitted by the hybrid lighting system and, importantly, to communicate those results to the hospital professional staff. This shared knowledge among the professional staff would then eliminate the need for curtains in the patient areas.
6. Conclusions
The present field study is the first to examine the efficacy of UV-A (λmax = 366 nm) for reducing pathogens in the context of a working hospital where professional staff could evaluate the technology while in operation. The hybrid lighting system used in the present study could independently emit visible white light or UV-A radiation or both. A series of analyses support the inference that the UV-A radiation will reduce the burden of HAIs in doses set to minimize negative health effects for human occupants (max = 10 W m−2 for 8 hours). Professional staff accepted the hybrid lighting system, but less so than the lighting system that was in place before the retrofit. There were several reasons for this, but a primary one was the staff’s dislike for the curtains that were placed in the NICU to block direct UV-A radiation on the infant incubators. An analysis of the photodegrading effects of the UV-A radiation was also undertaken. The results strongly suggest that precautions should be taken to select UV-resistant materials in rooms where the UV-A sources in the hybrid lighting system might be operated. In sum, this new technology offers great promise for hospital applications. The hybrid lighting system is safe to operate in occupied spaces under the radiation restrictions described here, but collateral effects need to be considered before it will be widely adopted.
Footnotes
Acknowledgements
The authors would like to thank Jane Kaiser and Mashelle Monhaut from the Memorial Hospital NICU for supporting this research; Smruti Damania and Alissa Lehto-Hoffman from the South Bend Medical Foundation for testing the biological cultures; Berney Montavon from GE Current, a Daintree company for engineering assistance; Katherine Snively, David Pedler, and Rebekah Mullaney from the Lighting Research Center for assistance with preparing the manuscript; and Ryan Sebasty of Pemberton Davis Electric, the electrician for this project.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by GE Current, a Daintree company.