
Abstract
Participation of community stakeholders in health research priority setting is an emerging trend. Despite this, the involvement of marginalised groups in research prioritisation is limited and where they are involved, sample sizes are small, where individuals are merely consulted with, rather than coproducing the research agenda. Without addressing power dynamics inherent in research prioritisation with marginalised groups, their engagement in the research process can be tokenistic and the resulting research agenda unreflective of their needs. This article, therefore, aims to generate knowledge on how feminist participatory action research was used to co-produce an obesity research agenda with British Pakistani women, a seldom heard population, living in deprived areas. The methodology enabled Pakistani women to be involved in all stages of the project, culminating in the co-production of an obesity research agenda that accurately reflects their unmet needs. Women’s engagement in the project led to their increased confidence, the formation of relationships that lasted beyond the research project, improvements to their lifestyles, and engagement in further research. Feminist participatory action research may be used by researchers as a guiding methodology due to its ability to improve women’s lives and develop research agendas for women’s health.
Keywords
Introduction
Research priority setting assists health researchers and policymakers in effectively targeting research to provide the greatest benefit to public health (Viergever et al., 2010). Traditionally, research priorities have been determined by researchers and policymakers with little involvement from the community (Abma et al., 2015). Experiential knowledge from those directly affected by the issue being researched improves the quality and relevance of the research through identifying appropriate research questions and improving the clarity of communications (Madden and Morley, 2016). Despite this, evidence exists that being female, economically disadvantaged, and/or belonging to particular ethnic groups means individuals are either listened to less or not at all in priority setting for health research (Shayo et al., 2012). Given the health inequalities encountered by Black Asian and minority ethnic (BAME) populations, it is fundamental that these communities engage in research prioritisation to incorporate their perspectives. To amplify the voice of Pakistani women, a seldom heard group in research priority setting, I, (the 1st author) made a conscious decision to adopt a research design heavily endorsed by feminist researchers: feminist participatory action research (FPAR) for this research project.
Although research priority setting exercises aimed at improving the health of BAME groups exist (Iqbal, West, et al., 2021), sample sizes are either too small or there is little involvement of these groups in any stage of the process. The structure of commonly used research prioritisation frameworks (a joint process involving public and professional stakeholders) may not be appropriate to ensure engagement of BAME communities due to potential power dynamics where the voices of professionals are privileged. Without addressing power dynamics, community engagement can be tokenistic (Pratt, 2020). Participatory methodologies, therefore, are advocated in research priority setting with BAME groups (Pratt, 2019). This article presents our methodological reflections on how utilising FPAR enabled me, a novice insider researcher, to develop a research agenda with Pakistani women living in deprived areas of Bradford. It is beyond the scope of this article to discuss the research data. For more information, please see (Iqbal, West, et al., 2022) and (Iqbal, West, et al., 2022a).
The project: Research prioritisation with British Pakistani women living in deprived areas
I was interested in establishing what Pakistani women felt were important areas for research to examine in relation to improving their health. They are disproportionately affected by adverse health including poor mental health (Kapadia et al., 2017), obesity (Ludwig et al., 2011), and diabetes (Abuelmagd et al., 2018), This project, therefore, aimed to develop a research agenda to address the health concerns of Pakistani women living in deprived areas to incorporate the unmet needs of this population. The inclusion criteria were British Pakistani women, both English and non-English speaking, aged over 18. The project also included input from multisectoral stakeholders to explore their perspectives, as is good practice in research priority setting (Viergever et al., 2010). Ethical approval was granted from the University of Bradford Ethics committee (reference E722) and data were collected and analysed by the 1st author between June 2018 - May 2020. There were three phases to the project (see Figure 1). Phase 3, Part 1 obtained the input of multisectoral professional stakeholders interested in the health of Pakistani women in Bradford and will therefore not be discussed in this article. Phases of the research.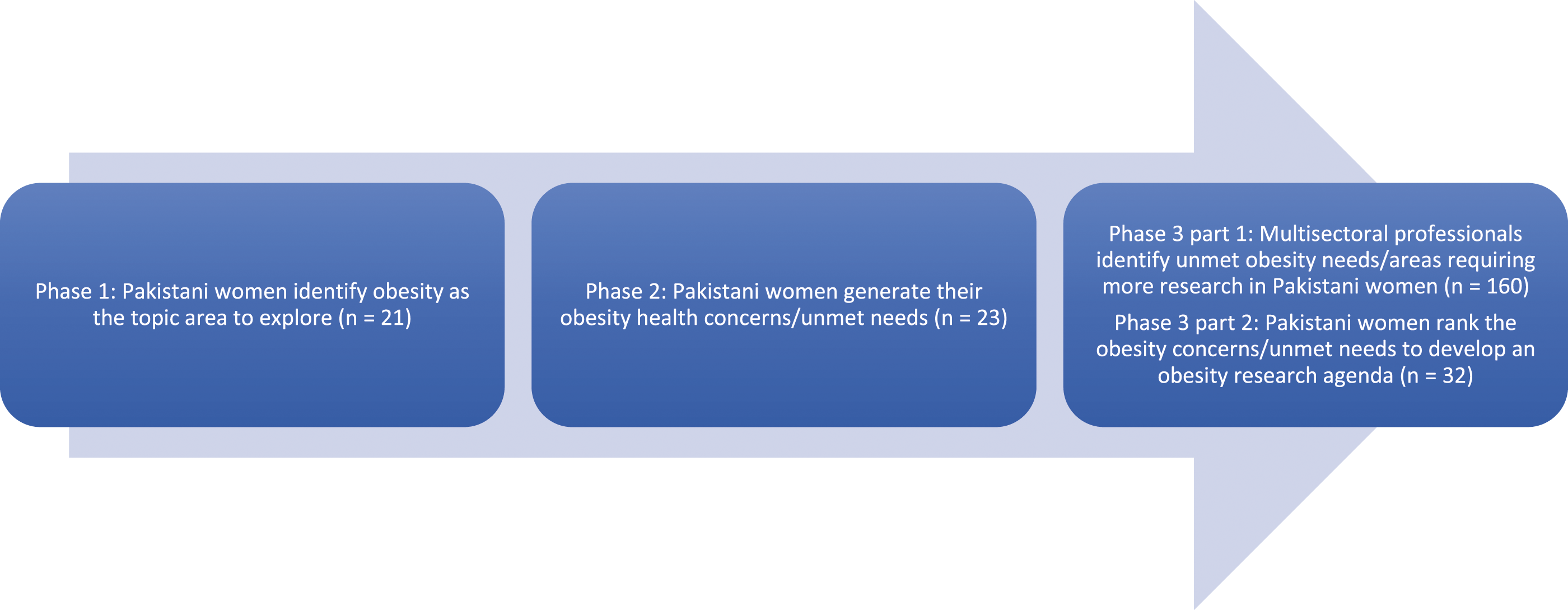
Feminist participatory action research
It is widely recognised that collaborative research practices such as coproduction should be promoted. Coproduction is supported by ethical and practical reasoning (Flinders et al., 2016). However, there is a lack of consensus about what coproduction is, how it should be done, and its effects on the research. Researchers coproduce with stakeholders in multiple ways, however, some approaches involve little interaction such as when stakeholders are mere recipients of research findings. Others interactions are more active such as seeking advice about policy agendas, or, stakeholders are equal partners in the research relationship (Oliver et al., 2019) which is regarded as true coproduction. There is limited evidence about the impact of strategies deployed by researchers in coproduction. There is, however, literature outlining limitations of performing coproduced activities such as the amount of time and resource involved (Oliver et al., 2019); difficulties in involving communities due to misaligned goals, power (Fuentes, 2019), and knowledge (Kaartemo and Känsäkoski, 2018).
Increasingly, Feminist participatory action research (FPAR) is used to set women’s health research agendas (Langan and Morton, 2009) therefore being particularly well-suited for establishing a research agenda with British Pakistani women living in deprived areas. Although there is no single definition of FPAR, it has been posited as a conceptual and methodological framework that facilitates a critical knowledge of women’s multiple viewpoints and promotes inclusion, involvement, and action while questioning the underlying assumptions researchers bring into the study process (Reid and Frisby, 2008). FPAR advocates the need for women to be involved in all stages of the research process which includes identification of the problems to be explored, carrying out data collection, and interpreting and acting upon the results (Maguire, 2004). In FPAR, priority is given to the perspectives of community members as experts, rebalancing power in the research relationship (Gustafson and Brunger, 2014). This focus on inclusion by FPAR researchers provides an avenue for researchers focused on women’s health, to foster meaningful engagement with marginalised women.
Positionality as an insider researcher
It is important to examine the insider/outsider debate given my membership of the participant group, and the impact my positionality may have on the research process. Researchers working within their own cultures are classed as insiders, whereas those who study cultures different to their own are perceived as outsiders (Narayan, 1993). I belonged to the same ethnic, gendered, and religious community as the women researched in that I am a Pakistani, Muslim woman, living in an economically deprived area of Bradford. A shared status can prove beneficial in gaining access to participants and provides a common foundation for the research (Corbin Dwyer and Buckle, 2018) in being able to modify activities in relation to data collection, interpretation and representing the needs of participants (Chavez, 2008). However, despite sharing the same cultural identity, the researcher may still be perceived as an outsider within the community due to their level of education and positioning as a researcher (Smith, 2012). The way in which my insider identity as a member of the community, and outsider identity as a university researcher interacts throughout the research process will be discussed in this paper.
Use of FPAR principles in the research process: Involving women in decisions around research design
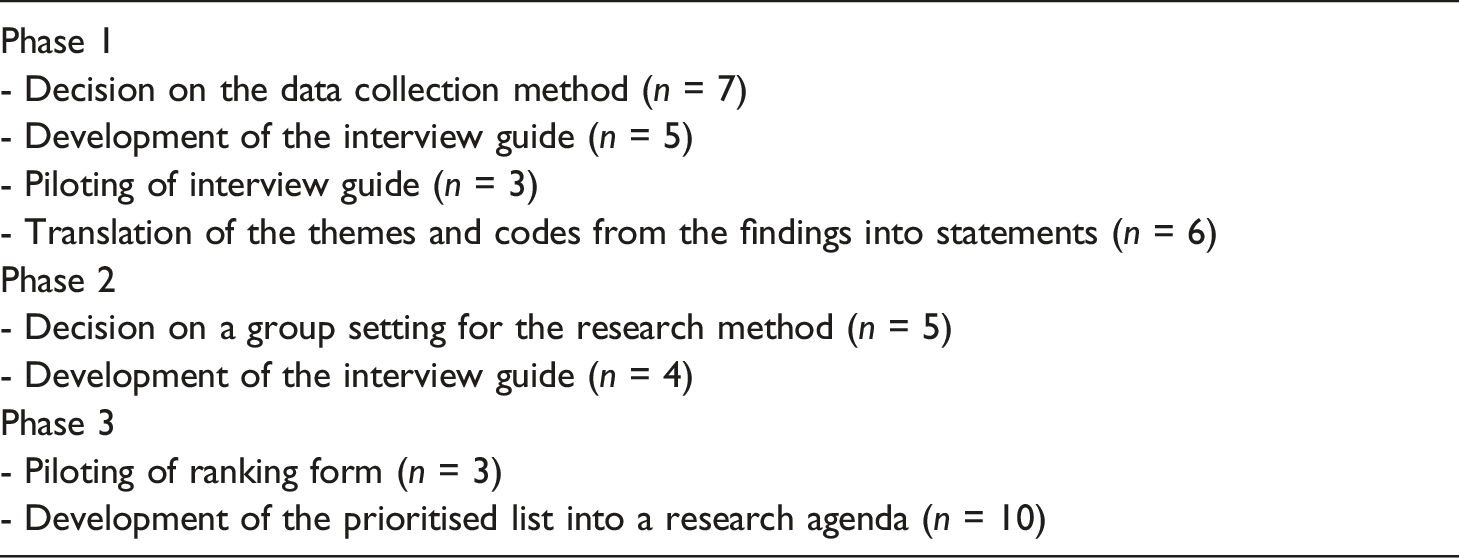
There were points in the research process where it was difficult to involve women directly in decision making. Instead, building on FPAR principles, rather than making decisions myself I consulted with members of the public who reflected the participants; Pakistani women living in deprived inner-city areas of Bradford. Public involvement in this project outside the direct involvement of participants, is displayed in Box 1.
Phase 1: interviews with Pakistani women to identify their health concerns to direct the research topic (n = 21)
Typically, the research priority setting process begins with an information gathering stage in which domains and categories are identified through a working group or planning committee consisting of experts in the field (Iqbal, West, et al., 2021). The resulting domains and categories may not align with what BAME communities themselves would define. A principle of FPAR is involving women in identifying the problem to be explored (Maguire, 2004). Therefore, the first phase of this project was an initial, bottom-up exploratory study with Pakistani women, to negotiate a shared research focus to inform the subsequent stages of the project. The aim of this phase was to explore the health concerns of Pakistani women living in deprived inner-city areas of Bradford. During consultations, Pakistani women stated their preference for individual interviews and focus groups to discuss their health. The semi structured interview has affinity with feminism (McIntosh and Morse, 2015) due to its informal and conversational nature (Longhurst, 2003) and ability to generate rapport, aligning with the principles of FPAR. Semi-structured interviews also provide opportunities for interviewees to convey their own experiences rather than answering structured questions which they may not have control over (Ryan et al., 2009). This could re-balance the power dynamic in the interview in the favour of the participant, which is advocated by FPAR.
Quotes are used to demonstrate the impact of PAR principles on those involved in the project. Pseudonyms were given to protect anonymity. Quotes were captured using either field notes or an audio-recorder.
Reflecting on the first four interviews, I was unable to generate adequate rapport with women leading to very brief answers to my questions. It was possible that despite my insider status, my identity as a researcher may have persisted as a barrier in engaging women in the research process. After consulting with feminist literature, I realised that I could build rapport with women by using my insider status and shared characteristics as common ground to build discussions upon (Chavez, 2008). I discussed elements of my life to put the women at ease, such as local places we frequent to eat, the local greenspaces in our residential area, and cultural foods we enjoyed consuming. This assisted in breaking the ice. As one woman exclaimed: “You shop at X too? Did you know they have some really good offers there on a Monday. Especially on meat. It’s quite newly opened and I didn’t know many people knew about it. Did you know they’re started doing organic chicken there too…?” (Salma, aged 38, non-English speaking)
It was imperative to demonstrate that despite possessing outsider status as a university researcher, I was also an insider. Therefore, I sought to actively address the impact of power and hierarchy among us so I informed them, at every opportunity, that I was interested in making change and enriching their lives as well as my life by helping us collectively improve our situation as Muslim, Pakistani women by increasing knowledge about their lived experiences. Once I had adjusted my approach it was clear women felt more at ease, rapport was built and they were subsequently more responsive, offering more richness and depth in their discussions. It also became apparent that by injecting humour in places this helped to ease any pre-existing tension that may have been prevalent. I knew this was effective because women disclosed that they did nor feel as acutely they were taking part in research but instead were engaged in a conversation with a friend: “This feels like a chat over chai and rusk cakes with my close mates, not like a serious research thing” (Aisha, 28, English speaking)
I was aware that sharing of my personal stories to encourage women to talk may result in women feeling as though they had developed a friendship with me. This issue was mitigated by me setting clear boundaries such as maintaining professionalism throughout the study and dissolving our relationship after the project had ended. I maintained contact only with those women who had specifically expressed that they would like to take part in further research (see the Action in FPAR section below). In addition, I took care to treat each woman equally. No plans were made to socialise with them, nor did I disclose to them my personal contact details.
During phase one of the project, Pakistani women identified obesity-related health concerns and unmet needs. Although research priority setting exercises in obesity exist (Iqbal et al., 2021), they have not included South Asian populations in the process. Previous research has noted that in research priority setting, participants find it difficult to translate issues of their daily lives into well-structured research questions (Manikam et al., 2017) and this may be even more difficult when involving seldom-heard communities, such as Pakistani women. This phase of the study, therefore, ended with public contributors translating the themes and codes from the findings into statements, rather than research questions, to be ranked by importance in the final phase of the project.
Phase two: focus groups with Pakistani women to explore their obesity concerns (Three focus groups n = 23 women)
This phase aimed to explore in more detail the obesity concerns of Pakistani women living in deprived areas of Bradford. In line with FPAR, I conducted further consultative work with Pakistani women to ascertain their preferred method of data collection. All women preferred a group setting, so that they could hear the perspectives of others to see if they aligned with their own views. For feminist researchers, focus groups provide a valuable methodological tool (Wilkinson, 1998) as they can reduce interviewer input and can facilitate a safe environment for minority groups where they can develop and elaborate their perspectives by interacting with one another, on a research topic, thus reflecting FPAR principles.
I approached gatekeepers in three settings; two school and one community group, to access women. In two of the settings (school and community), the women were part of established groups which has been identified as particularly useful by feminist researchers for adding depth to discussions as individual opinions are formed through conversing with friends about events and issues in everyday life (Wilkinson, 1998). For the other school, I attended the school assembly to discuss the study aims and form a focus group with eligible women who were unfamiliar with one another.
The gatekeepers informed me that some women in the established groups had low confidence and poor mental wellbeing. They attended group sessions in a safe space, among others in similar situations to get them out of the house. I realised that I needed to build a trusting relationship with these women, by becoming familiar to them. I attended each established group session twice to engage with the women before conducting the focus groups. This was time consuming and took effort on my part. However, this was crucial to reach a stage where communities are willing to support research activities (Islam et al., 2022).
Reflecting on conducting the focus group in which women did not have any pre-existing relationships, the five women were very reserved and there were long silences. I again deployed feminist strategies to effectively engage them. Which enabled women to become less formal and fully engage in conservations in which they revealed personal stories, shared healthy recipes, and cooking tips, discussed creative ways to exercise from home, and shared information on safe routes to walk locally. Following one of the focus groups with women with pre-existing relationships, they expressed gratitude for being able to take part in the study. They stated that they lacked trust in researchers and research, and felt excluded from research as no one ever asks their views, yet had wanted to be a part of my research project because I was a Pakistani, Muslim woman myself, stating: “We wouldn’t normally get involved in something like this but it’s nice to see an Apni (one of our own), so I trust you. You’re looking out for your own” (Fatima, aged 32, non-English speaking)
In another focus group with women with pre-existing relationships, when I informed women that I would be enlisting their assistance in data analysis and ranking, they replied that because they had been let down by researchers in the past, they felt that I would not be true to my word, explaining: “These people, researchers, came here, like, two years ago, to ask us about portion sizes in desi food (South Asian cuisine). Like, a group chat that they recorded, and it lasted a while. They said they’d get us involved in the next part of that work, but we never heard from them again. I don’t trust researchers. They use us for their work, and we don’t hear from them again. I don’t think you’ll be back here either” (Bushra, aged 46, English speaking)
Feeling used has been previously identified by Quay et al. (2017) who found one reason for mistrust in research by South Asians is that researchers conduct studies involving them and are never heard of again once the data has been collected. I assured the women repeatedly that I would be in contact again soon to arrange the next steps in the research. They informed me that they really enjoyed the interaction and hearing what others thought. A testament to this was that this session lasted 90 minutes rather than the scheduled hour that was allocated for it. This sentiment was reinforced by the gatekeeper who later contacted me to inform me that the women wanted to set a date to assist me in data analysis.
Data were analysed using thematic analysis (Braun and Clarke, 2019). Participants verified the transcripts to ensure they were a true reflection of what was said during the focus groups. This was particularly important as cultural slang was used in both groups and I may misinterpret their words due to a lack of certainty of their translated meaning, I, therefore, revisited the two pre-existing groups and the women who were shown the codes and themes were asked to provide feedback. As was done in Phase 1, the findings were translated into statements to be ranked in the final phase but this time, it was participants themselves that assisted in their translation and not public contributors. Through reflection after Phase 1, I realized that it would be more appropriate for the findings to be translated into statements by participants themselves, to ensure a more accurate representation of the findings.
Action in FPAR during phase two
At the heart of participatory action research, is self-reflective enquiry that enables individuals to have increased control over their lives and this reflection is linked directly to action (Baum et al., 2006). When reflecting on the action borne from this phase, it was clear that actions had occurred on both individual and collective levels.
Individual action
The first example of this was when one woman expressed upset at the lack of family support in trying to cook healthy food to assist her weight loss. Other participants were empathetic and provided her with healthy recipes that they themselves used. The same woman participated in the ranking exercise in Phase 3, a year later and informed me that she had discussed the concerns she had raised during the focus group with her husband, and they had decided as a family, to modify their diet by no longer frying foods. Also, several of the healthy recipes that had been provided were now staple meals in her household, replacing the high calorific foods: “I bought an air-fryer, the one that Shazia recommended, and I make everything in there now instead of frying it. The peri chicken legs recipe that Ayesha gave me, and the veg bulghur thing is a hit with my husband and kids so I make that at least twice a week instead of getting chicken and chips from outdoors” (Shamim, aged 37, English speaking)
A further example of individual action borne from women’s involvement in Phase 2 is that it became clear that for many of the women, interacting with peers and hearing their perspectives increased their confidence and self-esteem and they became more assertive. For instance, during the focus groups, many women were initially quiet, not engaging with the process until others disclosed their concerns around obesity. This gave the reserved women the confidence to share their perspectives including their opposing views when they heard something that they disagreed with. They also disclosed that they did not know that others encountered similar problems to them until they heard other women express their concerns. One gatekeeper contacted me after the focus group, saying that those women who are normally very reserved in the group sessions, benefitted from their participation in that they contributed significantly to discussions, even debating with others.
Collective action
An example of collective action resulting from participation in this research project can be seen in women after participating in Phase 2. During the focus group, women learnt that all members of their group desired to engage in more physical activity yet felt uncomfortable walking alone in their local area. These discussions promoted feelings of togetherness and collective empowerment to initiate action by setting up a weekly walking group together. All five women continued participating in the study and a year later four of them were still going for weekly walks with other women who had joined the group. The group now ventures out of the city to go for long walks in scenic locations around Yorkshire. Prior to their participation in the focus groups, by their own admission, none of these four women engaged in leisurely walking for physical activity due to cultural and safety barriers and felt socially isolated and helpless by their circumstances at home. In both scenarios, women informed me that their lives, and the lives of their families, had improved by taking part in the research project, stating: “It’s funny because we met that one day but would never have thought we’d make lifelong friends just from that meeting” (Sobia, aged 42, English speaking)
Phase three, part two: Ranking exercise with Pakistani women (n = 32)
During the ranking or consensus seeking stage of research priority setting, it is common for multisectoral stakeholders to come together and decide, by consensus, a list of research priorities. As I was acutely aware of the prevalence of power imbalances in research priority setting exercises when bringing together patients and the public, and other stakeholders such as academics, researchers, health professionals and policy makers (Pratt, 2019) and the negative impact this could have on Pakistani women’s level of participation, it was decided that I would not bring together stakeholders but would instead solely include Pakistani women.
The purpose of the ranking session was for women to rank their top 10 most important statements from the list of 32 statements borne from the previous phases resulting in a top 10 list of prioritized statements. The ranking session was completed with women on a one-to-one basis, over video or voice call, to enable a wide range of Pakistani women to participate. Every effort was made to accommodate the wishes of participants to align with my FPAR methodology so that women’s needs were prioritised over my own. This included meeting at a time that was suitable for them which was frequently at 9pm as their children were asleep, enabling participants to talk freely. Working flexibly is essential to effectively coproduce with communities (Islam et al., 2022).
An important principle of FPAR is to share control of the research process with participants (Johnson and Flynn, 2020) to reduce researcher impact on the research. Up until this point of the research, Pakistani women themselves had not participated in collecting data, however during the ranking session, they did. Completing the ranking session one to one with women provided them with the opportunity to firstly experience the ranking process, and then support others with ranking. Nine women were trained by me on how to collect data. Published national standards on involvement in the UK stress the need to provide support and learning to enhance people’s confidence and skills for involvement (NIHR 2018). This is imperative for all stakeholders involved in research as they gain a better understanding of how involvement works (Horobin et al., 2017) and how to effectively work together (Staley et al., 2019).
Action in FPAR during phase two
The five women who had been initially been reserved in phase two expressed an interest in data collection in the ranking phase. This suggests that participation in this project was particularly empowering and for these five women who demonstrated increased confidence from when they initially participated in this research project, to becoming researchers themselves. Evidence indicates that individuals gain self-esteem and confidence by participating in peer research as researchers (Kelly et al., 2016). All the women involved in the project were asked if they would like be involved in further research pertaining to the health of South Asian women in Bradford. Interestingly these same five women without the pre-existing relationships asked to stay in touch. Recently, two of the women and myself were awarded grant funding, as co-investigators, from the National Institute for Health and Care Research to develop peer-led obesity support groups for South Asian, Muslim women across West Yorkshire (one of the recommendations from the research project reported in this article). Deploying FPAR as the research design underpinning the various phases of the research and being mindful to include strategies endorsed by FPAR meant that these women had increased in confidence and are now actively engaged in taking steps to conduct health research in their communities.
Developing the statements into an obesity research agenda
Once the data had been collected, I quantitatively analysed it, which resulted in a top 10 list of prioritised statements. At the final stage of research priority setting, statements are often translated into researchable questions and edited for clarity by a working or steering group that oversee the process. In this context, this would have been done by the researcher. This is referred to as external synthesis by Pratt (2019) when after the initial priorities have been identified, they are discussed by experts which gives power to the experts to interpret the findings. I would argue that when translating the statements into researchable questions or priorities, there is a real possibility that misrepresentations of statements can occur, thus failing to reflect the needs of those voices it intends to capture. This concern about losing specifics and preserving the authenticity of prioritised statements has been identified elsewhere (Madden and Morley, 2016). Those who have the power to synthesise the priorities and questions, may frame local knowledge in ways that highlight certain issues or solutions over others, leading to outputs reinforcing thinking about the world in a particular way over not from the perspectives of those with local knowledge (Pratt, 2019). To avoid this issue, a participant from phase four and ten public contributors assisted with translating the prioritised statements into a research agenda.
Lessons learnt
Many lessons were learnt during this project and have been discussed in the various phases of this paper. Two of the main learning points, however, are centred around being an insider researcher, and the time and effort required to coproduce research agendas with the public.
Being an insider researcher
My insider status assisted significantly in building rapport and eradicating barriers typically experienced by outsiders in research. It was clear throughout the study that this insider status enabled an environment to build trust with the women, enabling women to openly discuss their obesity related concerns and needs in my presence without fearing judgement or reprimand. Despite this, it was clear that during the research process, I was operating in a fluid capacity rather than possessing a fixed identity as an insider. For instance, two women were reluctant to participate yet part way into the sessions, asked if they could contribute to the discussions because they found them relevant and engaging yet did not agree with some of the perspectives and wanted to share their views on the topic. When probed afterwards about their changed stance, they stated that they had initially felt that they would be pressured to contribute and that because they did not know me, they were reluctant to share their views. This demonstrates that despite possessing insider status, I was deemed an outsider in some instances. Being mindful of the shifting identity of insider/outsider throughout the process is important so that insider researchers do not enter the process with certain expectations as this may lead to disappointment that they are not receiving the results they expected, or they may be less likely to be flexible and modify things if something is not working well.
Time and effort commitment requirement
A significant amount of time and effort was placed in ensuring that the project was designed in a way that facilitated women’s involvement throughout the research process. For instance, women were consulted with at various points during the project when they couldn’t directly be involved as co-researchers. I attended group sessions on many occasions to build relationships with the women, which also included returning to the groups for member checking of transcripts and for their assistance in data analysis. Data were collected at unconventional times to fit around women’s commitments and training women as researchers took a considerable time investment. Researchers need to be aware that good co-production requires considerable time commitment on the part of the researcher and participants.
Limitations
The study could have been more aligned to its underpinning participatory methodology. A project working group consisting of Pakistani women could have been established providing consistent input across the studies rather than ad hoc. Participants could have been involved earlier for example developing the interview topic guides, rather than women who reflected the target population.
Participants were asked whether they wanted to be named as authors on publications but declined and instead suggested that it would be more beneficial for me to disseminate the research findings to the community. I therefore delivered two presentations locally; one in a leisure centre, and one in the same community organisation in which I had conducted one of the focus groups. These were well attended by Pakistani women. It is important to note that communities not involved in research may have differing interests that do not align with academic researchers, such as publishing papers. Their interests lie more in how the research can benefit the community, hence their suggestion to disseminate the findings via community settings.
Concluding remarks
The use of FPAR as a conceptual and methodological framework to guide this research meant that the inclusion and participation of Pakistani women was key and a crucial focus throughout the study. This project demonstrated that researchers wanting to undertake this methodology must be committed to devoting significant time and effort in creating trusting relationships with participants. Possessing insider researcher status has many benefits, but insider researchers must be mindful that their identity is in constant flux within the research process which could influence the research process. Researchers who are keen to involve the community as active partners in research priority setting processes may benefit from adopting FPAR as a guiding methodology due to its ability to improve women’s lives and develop research agendas for women’s health.
Footnotes
Acknowledgements
I would like to extend my sincerest gratitude to all the research participants and public contributors for sharing their knowledge, and to my supervisors on this project
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute for Health Research (NIHR) under its Applied Research Collaboration (ARC) Yorkshire and Humber in the form of Ph.D. funding to HI [NIHR200166], the UK Prevention Research Partnership (UKPRP) in the form of funding to JW and RM [MR/S037527/1], the NIHR Clinical Research Network in the form of funding to JW, and the NIHR ARC Yorkshire and Humber in the form of funding to RM.