
Abstract
Strong professionals who influence the development of healthcare services have dominated healthcare organizations for many years. However, this dominance has been challenged recently through patient involvement. One method of achieving patient involvement is experience-based co-design (EBCD), in which patients and healthcare professionals work together to improve care. Patient involvement has considerable potential, but also presents certain challenges. This article addresses these challenges using experiences from patients and healthcare professionals who participated in two action research projects that aimed to improve patient experienced quality using EBCD in pediatric care. The paper shows that patient involvement in quality improvements can challenge the traditional roles of professionals and patients by new roles as co-designers. The role as co-designer embraces new perspectives for healthcare professionals that force them to step out of their comfort zone. Accordingly, healthcare professionals are able to view patients as equal partners in improvement work. Reflecting dialogues during the projects offered eye-opening stories for patients and healthcare professionals that enabled them to construct a common picture of care. The contribution of this study is strengthening earlier research that argues that an action research approach can strengthen important values for successful EBCD projects: equal partnerships, new roles, and dialogue. The findings show that the combination of EBCD and action research is a promising approach to address the challenges of patient involvement in healthcare improvement.
Keywords
Introduction
Healthcare professionals often think they have unique expert knowledge that will improve care processes and create value for patients (Bate & Robert, 2006). Based on experiences from joint improvement efforts in service industries in general (Carbonell, Rodríguez-Escudero, & Pujari, 2009; Witell, Kristensson, Gustafsson, & Löfgren, 2011), patients are also likely to be important resources in healthcare improvement by contributing knowledge from their personal experiences.
However, patient involvement practices are often problematic and have therefore not been widespread in healthcare (Luxford, Gelb Safran, & Delblanco, 2011). Strong professional dominance in healthcare has been the main explanation for difficulties in involving patients in ongoing care activities or improvements (Luxford et al., 2011). The presence of strong professionals such as physicians, nurses, etc. in healthcare is an advantage, in that they bring the benefit of their knowledge, but also a challenge because it can be hard for management to influence them (Freidson, 2001; Scott, Ruef, Mendel, & Caronna, 2000). The legitimacy of medical professions in society is based on trust that professionals always put the best interests of the patient first (Wilensky, 1964). However, researchers have also argued that professionals actively guard their arenas and positions by ensuring that they dominate their knowledge domain, precluding other actors from challenging their decisions (Abbott, 1988; Freidson, 2001). Allowing patients to access this knowledge domain challenge the status and identity of professionals (Andersson, 2015). Thus, a professional logic has two competing characteristics—service ideal and professional dominance (Freidson, 2001; Wilensky, 1964)—that are related, but have different implications. The service ideal means that a professional, acting altruistically, always works in the best interest of the client. Professional dominance is the egocentric belief that only a professional knows what is best for a client/patient (Liff & Andersson, 2011). These competing characteristics explain why joint improvement efforts involving patients and healthcare professionals are a natural evolution based on the altruistic service ideal in professional logic, but also challenge the very core of professional logic considering egocentric professional dominance.
Despite several examples of mutual gains with positive and sustainable improvement results, the clash between these logics entails inevitable challenges when healthcare professionals and patients are involved in joint improvements (Bate & Robert, 2006; Gustavsson, 2014; Iedema et al., 2010; Pickles, Hide, & Maher, 2008). New roles and approaches are required for both healthcare professionals and patients. Luxford, Gelb Safran, and Delblanco (2011, p. 513) argued that one barrier to moving from a “provider focus” to a “patient focus” is changing “the mindset of employees.” Staff may also feel that involving patients in improvements is time-consuming and competes with daily work tasks (Donetto, Tsinakas, & Robert, 2014; Larkin, Boden, & Newton, 2015).
One method of involving patients in healthcare improvement is experience-based co-design (EBCD), in which healthcare professionals and patients use their own experiences as pivotal points of departure for developmental efforts in order to improve care (Bate & Robert, 2006, 2007). Internationally, EBCD has been described as an action research (AR) method (Robert, 2013), even if it often is used as an improvement method without research ambitions. In Sweden, where the current study took place, EBCD has only been an improvement method. Combining EBCD and AR means adding a research part to EBCD and also taking advantage of AR’s ability to support conditions that enable development and change, such as equal power distribution between healthcare professionals and patients as they jointly contribute knowledge to the healthcare system (Hughes, 2008; Koch & Kralik, 2006; Lifvergren, Huzzard, & Hellström, 2015). However few studies have provided insight into the effects of combining EBCD and AR (Bate & Robert, 2007).
In the present article, we address the challenges of patient involvement in healthcare quality improvements by describing experiences from patients and healthcare professionals who collaborated in AR projects, by using EBCD in pediatric care settings at a Swedish hospital. Involving patients in the research process results in co-production of knowledge, sustainable change, and translation of knowledge (Gillard, Simons, Turner, Lucock, & Edwards, 2012). However, few research papers have explored the benefits of combining EBCD and AR, and studies on EBCD have mainly been case studies that report outcomes from improvement projects (see Bowen, Dearden, Wolstenholme, & Cobb, 2011; Boyd, McKernon, Mullin, & Old, 2012; Tsianakas et al., 2012).
Previous research
This section includes a brief overview of previous research in the field of patient involvement in improving healthcare and, more specifically, the EBCD method.
Patient involvement in healthcare improvements
Patient involvement is a central aspect of sustainable healthcare (Lifvergren et al., 2015; Williamson, 2014) and may occur in several different ways. For example, patients may take greater responsibility for their own care, for managing healthcare services, and for improving the quality of care.
One step towards patient involvement may entail using patient experiences to evaluate care as a basis for improvements executed by healthcare professionals (Coulter, Locock, Ziebland, & Calabrese, 2014). Healthcare organizations have gone a step further in recent years, emphasizing public and patient involvement in service development and participation in decisions around one’s own treatment (Tritter & McCallum, 2006), which implies a view of active patients as co-producers of healthcare quality (Bate & Robert, 2006; Lengnick-Hall, Claycomb, & Inks, 2000; Robert et al., 2015).
There is a lack of research about improvement projects that involve patients participating together with healthcare professionals. However, Crawford et al. (2002) described how the experience of participating in joint improvements can differ between patients and healthcare professionals. Patients welcomed the invitation to participate and their self-esteem often improved as a result of their contributions. However, they sometimes felt the process was unsatisfactory as it was not intended to devolve power to patients, but to legitimize decisions made by healthcare professionals. In an additional study (Engström & Elg, 2015) the following motives for patients to join were identified: restitution after poor treatment, desire for contact with others, volunteerism, desire to make a contribution, or the enjoyment of having a task to complete. Crawford et al. (2002) described that healthcare professionals found the experience rewarding, but also described difficulties in their relationship with patients; for instance, decision-making processes were slowed down. However, organizations became more open to involving patients and the projects had a general effect on organizational attitudes.
Bowen and Wright (2010) described further challenges, which included a conflict between patient involvement and professional values and daily habits. Furthermore, even when professionals were positive to patient involvement, there was a gap between values and practice (Lord & Gale, 2014). Because the experiences of healthcare professionals and patients can differ, a collaborative approach is needed in order to capture as many areas of improvement as possible (Gustavsson, 2014). In addition, if patients—who are the experts in their own experiences—are given the opportunity to be involved in the health service improvement and design, a shift may occur in expertise and, in turn, in the power relations between patients and professionals (cf. Tritter & McCallum, 2006).
Accordingly, patient involvement in improvement work needs careful management if it is to realize its full potential (Armstrong, Herbert, Aveling, Dixon-Woods, & Martin, 2013; Crawford et al., 2002). Managers are often willing to involve patients in improvement initiatives, but lack knowledge and experience of how to do it (Andersson & Olheden, 2012; Bate & Robert, 2006; Iedema et al., 2010). While it is important to use patients’ unique experiences when striving for higher healthcare quality, the challenges must be illuminated. Successful collaborative improvements in healthcare require courage to change the current roles for patients and healthcare professionals.
Experience-based co-design
Bate and Robert (2007) developed the EBCD method in collaboration with the NHS Institute for Innovation and Improvement. AR was used as an approach to test new methods of involving patients in improvement efforts on equal terms with healthcare professionals. The EBCD methodology was inspired by several research approaches: participatory action research, user-centered design, learning theories, and a narrative-based approach (Bate & Robert, 2007). In EBCD, healthcare professionals and patients work together in four steps: capturing experiences, understanding experiences, improvement, and follow-up (Bate & Robert, 2006, 2007; Tsianakas et al., 2012). During these phases, storytelling is a basic foundation for improvements, and there are opportunities to engage in dialogue that supports learning among individuals, groups, and organizations.
The first examples of EBCD in healthcare came from a head-and-neck cancer clinic (Bate & Robert, 2006, 2007; Pickles et al., 2008). The method was subsequently used elsewhere, such as emergency health services (Iedema et al., 2010), breast and lung cancer services (Boyd et al., 2012; Tsianakas et al., 2012), neonatal care (Gustavsson, 2014), outpatient services for the elderly (Bowen et al., 2011), and mental health (Larkin et al., 2015).
The results of such collaborative improvement projects included fast access to reliable health advice, effective treatment delivered by trusted professionals, involvement in decisions, respect for preferences, clear and comprehensible information and support for self-care, and attention to physical and environmental needs (Maher & Baxter, 2009). A collaborative approach can tackle both simple and complex problems (Gustavsson, 2014). Even if the accomplishments are small, several improvements simultaneously or within a relatively short time can produce a vast shift in the entire experience and may lead to deeper, longer-term changes in attitudes and behaviors (Robert et al., 2015).
According to Pickles, Hide, and Maher (2008), the EBCD methodology ensures that healthcare professionals draw upon the experiences of patients and their families in order to truly reflect on patient needs. These experiences help the participants see their care pathway from different perspectives with an emotional touch (Iedema et al., 2010). The EBCD methodology is a process in which people who have everyday experiential knowledge combine with people who have expert knowledge (specialist, discipline-based) and the two knowledge systems enrich one another (Bate & Robert, 2007). Hence, the dynamic process is a complex social intervention that has an impact that can be difficult to evaluate (Iedema et al., 2010). Furthermore, the process depends on the participants’ personal development; changes in the healthcare professionals’ motivation, skills, and self-confidence; and the development of trust and new relationships between the various participants (Donetto et al., 2014). The novelty of EBCD is that patients are involved in all phases, not only sharing their experiences, but also positioned as active partners with healthcare professionals (Tsianakas et al., 2012). If the improvement process leads to new understandings, relationships, and engagement, it can potentially support a more equal partnership between patients and healthcare professionals (Iedema et al., 2010).
Collaboration under these circumstances is challenging because few social or discursive rules for co-design processes currently exist. For instance, the role of improver has been reserved for healthcare professionals. Other challenges include engaging people’s commitment to the idea of collaborative improvements and talking about their experiences. EBCD is sometimes seen as impractical because the methodology (such as conducting interviews or making films) is time-consuming and the corresponding number of improvements made may be relatively small (Larkin et al., 2015; Robert, 2013).
Another challenge is that the EBCD approach shifts the focus from a strong management orientation to a more user-centric organizational approach, which may lead to promising future developmental directions (Bate & Robert, 2007).
EBCD as an AR approach
Similarities between EBCD steps and the AR cycle.
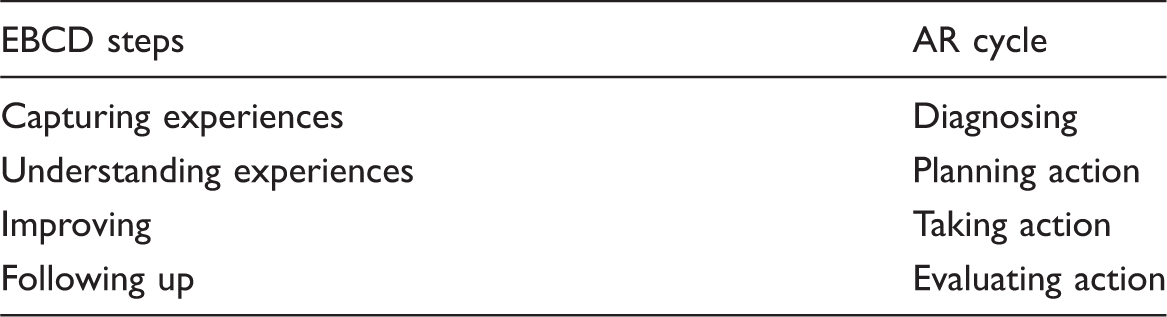
AR; action research; EBCD: experience-based co-design.
Even though there are similarities between EBCD and AR there are benefits of the combination. One is the reflection that occurs through AR that may not be found in ordinary improvement projects using EBCD. A reflection process that goes beyond the actual project, when the research process continues. In addition, each step in the EBCD process can be strengthened by the experiential learning cycle: experiencing, reflection, interpreting, and then taking action (Coghlan & Brannick, 2008). Reflective inquiry in AR can be from first-, second-, and third-person perspectives (Bradbury, 2013; Coghlan & Brannick, 2008; Reason & Bradbury, 2009; Reason & Torbert, 2001). First-person inquiry can be individual reflections on “… changing practices, ways of thinking and quality of attention” (Torbert & Taylor, 2008, p. 240) and is vital for developing critical subjectivity (Burgess, Pirkis, & Coombs, 2006). Second-person inquiry entails collective learning within a group of people, such as organizational learning, and third-person inquiry concerns the theoretical contributions to academia (Torbert & Taylor, 2008).
Method
The research approach was based on AR and the study design was inductive and qualitative. The authors sought to analyze and describe the experiences of researchers, healthcare professionals, and patients who participated in projects that combined EBCD and AR, and to address the challenges. Consequently, we chose a qualitative approach for its relevance for analyzing practical implications, social relations, and verbal and textual data, in an attempt to achieve an in-depth understanding of the phenomenon (Flick, 2009).
Insider action researcher
During the first part of the AR process, the first author functioned mainly as a method facilitator, guiding the teams through the EBCD phases. She had previously worked as a midwife in the organization, but here she took the role of an insider action researcher (IAR), which presented both advantages and challenges. On one hand, the author felt like an insider; someone who was familiar with the organization, the other people working there, and had experience of caring for children in neonatal care and children with diabetes. On the other hand, in her role as an IAR, she felt as though the participants viewed her as an outsider, someone who was no longer active in the workplace. She had to consider these different roles in the reflective process. The most difficult aspect of this process was abstracting the practical issues and experiences into theoretical reflections; however, as a doctoral student, she could turn to her university supervisors for assistance. It is not uncommon for someone conducting AR in his or her own organization to feel confused about his or her different roles (De Guerre, 2002; Coghlan & Brannick, 2008).
The second author participated in the diabetes project as the father of a daughter with diabetes, but then also took an active role during the writing of this paper. As a researcher in healthcare management, he has experience in healthcare organizations as an outsider, but has never worked in healthcare. He enrolled in the project with no research plans, but after the completion of the improvement project he was invited to participate in a joint writing project with the first author. The second author recognized that the different roles he had played during the process provided various perspectives. During the improvement project, the second author was an insider to some extent, as a participating, committed father with the goal of improving diabetes care for children. At the same time, he was an outsider in the organization compared to the first author. During the writing process, the second author was an insider in terms of parents’ experiences, but an outsider in leading the project compared to the first author. These various perspectives enhanced the reflective capacity of the AR process.
Context
This paper is based on two AR projects in pediatric care processes in a Swedish hospital. The pediatric division has worked with quality improvement processes for approximately 10 years, but has only had modest patient involvement.
The first project, the neo project, was located in the neonatal care department and involved healthcare professionals from the delivery, maternity, and neonatal wards. The participants in the neo project included nurses, midwives, and nursing assistants (n = 7); and parents (n = 5; two fathers and three mothers). The mothers had two perspectives: that of a patient giving birth and that of a parent of a child needing neonatal care.
The second project, the diabetes project, focused on care processes for children with diabetes and involved the children’s medical department and outpatient clinic. Four fathers and three mothers of diabetic children participated, together with seven healthcare professionals (three nurses, a physician, a psychologist, a social worker, and an improvement facilitator).
The term “patient” as used in the two projects includes mothers as patients when giving birth, their partners, and parents as spokespersons for their sick children.
Both projects lasted for about nine months and were inspired by EBCD, with four phases: capturing, understanding, improving, and following up experiences (Figure 1).
The EBCD/AR process. AR; action research; EBCD: experience-based co-design.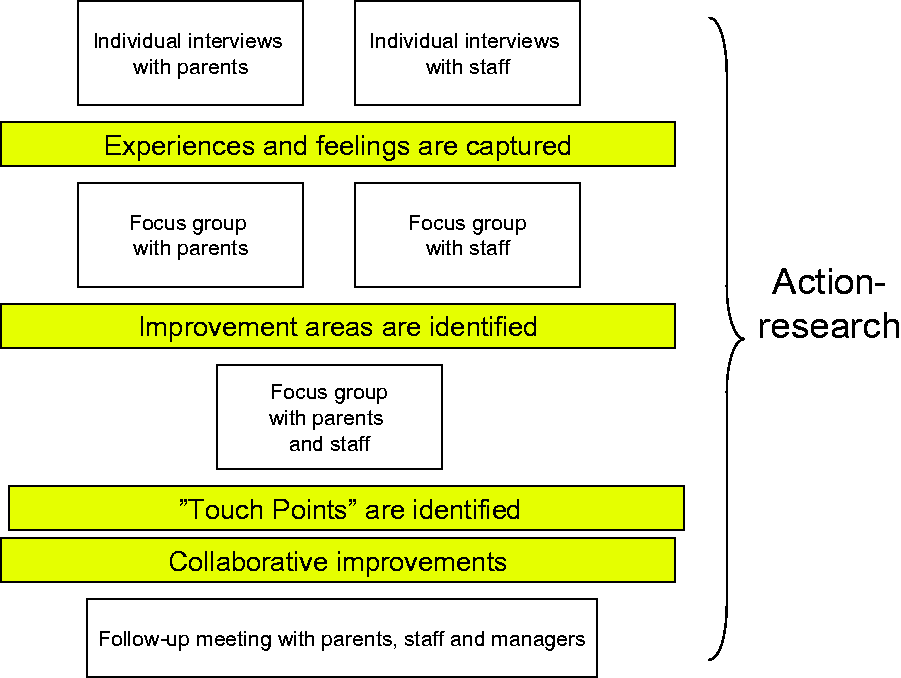
The outcomes, in the form of established improvements in the patient processes, have been described in earlier publications (Gustavsson, 2014; Gustavsson et al., 2016).
(1) Capturing experiences
The first phase was capturing the experiences, in which patients and healthcare professionals were interviewed individually. The interviews, which lasted approximately 60–90 minutes, were recorded and transcribed. One open-ended question was used: Can you describe your experiences of the care process, and how you felt in various situations? The first author documented the mentioned situations and related feelings in an “emotional map,” which consisted of a timeline that compiled patient processes with experiences from all individual interviews. One map consisted of patients’ experiences and another of the healthcare professionals’ experiences.
(2) Understanding experiences
The second phase was understanding the experiences. In this phase, all the patients/relatives met to agree on the contents of the map and to highlight common improvement areas. A similar meeting was held with all healthcare professionals. Thereafter, both groups met for a reflection dialogue in which the two groups listened to each other’s experiences and identified “touch points” of joint improvement areas. A list of prioritized improvement areas was developed collaboratively.
(3) Improving experiences
During the third phase—improving—the healthcare professionals and patients/relatives worked in groups or pairs to solve problems using the plan, do, study, act (PDSA) cycle (Deming, 1986). Some participants met during the improvement work and others met via telephone and/or e-mail. The improvement facilitator supported this phase.
(4) Follow-up meeting
Approximately three months after the improvement phase started, a follow-up meeting was held in which participants in the project groups presented the completed improvements. These meetings also included ward managers, who supported the accomplishment of some improvements that required managerial involvement. During the meeting, participants also reflected on the methodology and highlighted the challenges and advantages they had experienced in the combined EBCD/AR projects. After the meeting, the IAR distributed a questionnaire that captured the participants’ experiences of the EBCD/AR process in order to complement the joint reflections.
Overview of the projects.
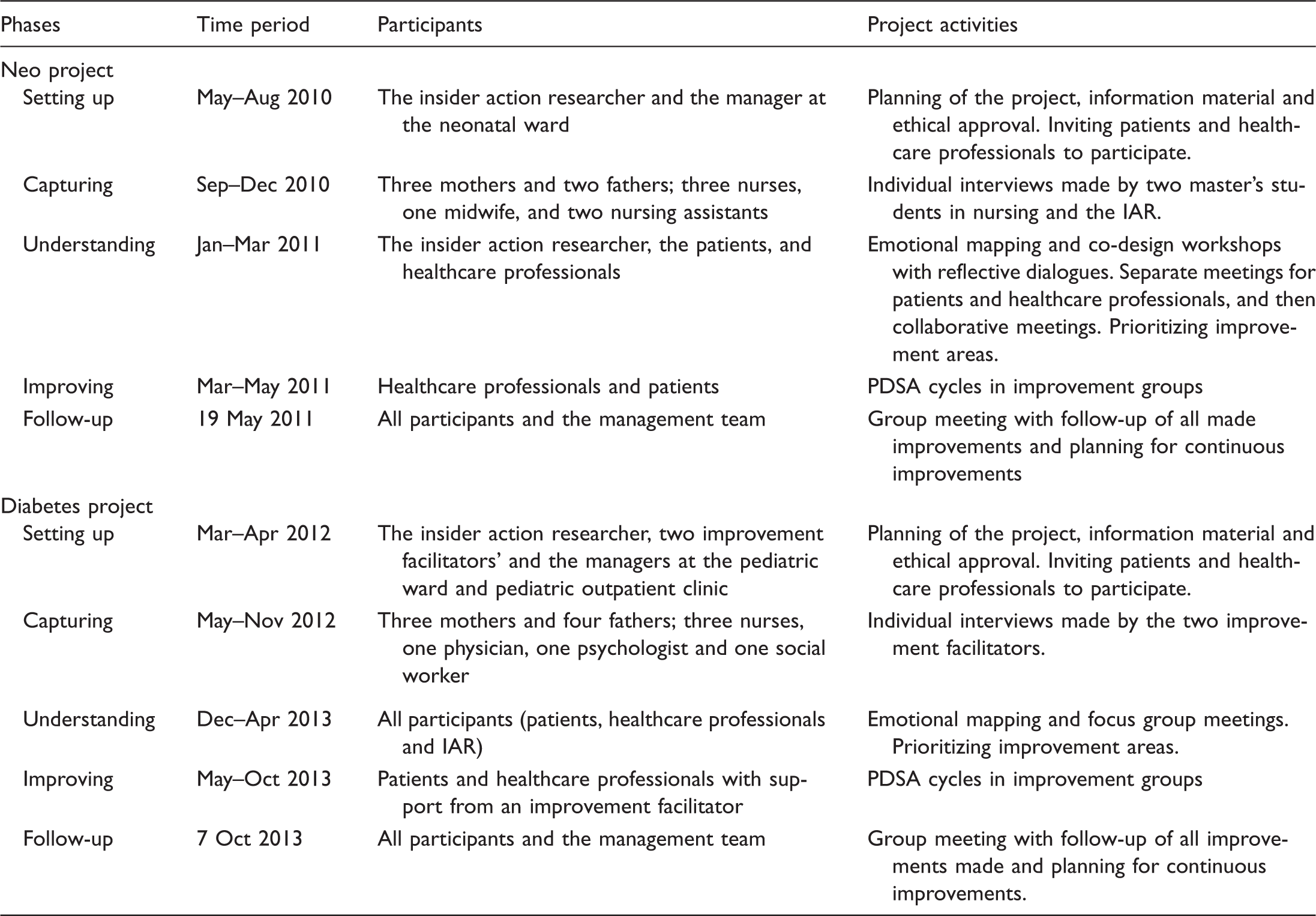
IAR: insider action researcher; PDSA: plan, do, study, act.
In each phase of the EBCD approach, the IAR supported the reflective process by asking questions to participating professionals and patients such as: What is going on? How do we move forward? What did we learn?
Data collection and analysis
This paper draws upon three sources of empirical material: recorded and transcribed reflective dialogues from all the group meetings in both projects, a questionnaire regarding the participants’ experiences after project completion, and the IAR’s field notes during the project. Each project had six or seven group meetings (see Table 2). The questionnaire was sent by mail to 28 recipients and had a response rate of 61 percent. The questions were open-ended. Examples of questions include: How was your experience of attending a project in which patients and healthcare professionals collaborated? How do you think that the improvement work was affected by the fact that patients and healthcare professionals collaborated?
Data were analyzed in three stages. First, we used first-person inquiry, based on the first author’s reflections of being an IAR. The first author kept a personal diary during the project. The notes in the diary contained different experiences during the process that contributed to learning, e.g. situations that felt difficult or positive. Second, we used qualitative analysis to examine transcripts of the group meetings and the questionnaires (Graneheim & Lundman, 2004) and perform a second-person inquiry of the project participants’ reflections and learning. The texts were read several times in order to capture, code, and translate units of meaning into categories and themes. The third-person inquiry stage of the analysis consisted of reflections on the theoretical contribution to research. The reflection was managed through dialogues between the IAR and other researchers. The reflection and analysis continued between the IAR and the co-author during the writing of this paper.
The validity of this study is based on the deliberate, conscious adoption of the AR cycle of planning, taking action, and evaluating the action, which in turn leads to further planning. Reliability was ensured by having different parties in both the academic and organizational settings triangulate data. For example, after the first author had analyzed interviews with patients and healthcare professionals, the result was brought back to them in an emotional map for confirmation. Such triangulation strengthens the trustworthiness of research (Bryman & Bell, 2007; Coghlan & Brannick, 2008). The generalizability of this study is analytical rather than statistical (Bryman & Bell, 2007) and the lessons learned during this project can support learning for others.
Collaboration on equal premises during the project provided a valuable ethical safeguard. Participants took part in the study voluntarily and were informed that they could withdraw at any time. Before starting the projects and the research, we received ethical approval from the ethical review board in Gothenburg (Dnr 135–10).
Experiential lessons from the combined EBCD/AR projects
The findings are based on reflections in first-, second- and third-person inquiry, compiled and presented as four themes (see Figure 2).
Four themes.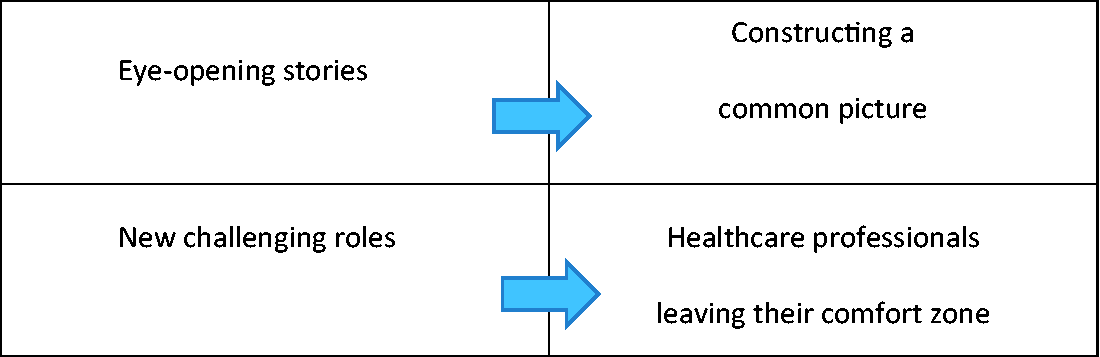
Eye-opening stories (A) is a theme that leads to the construction of a common picture (B). The third theme is new challenging roles (C), which leads to healthcare professionals leaving their comfort zone (D). The themes will be further presented with descriptive quotations from patients and healthcare professionals.
Eye-opening stories
During the improvement process, patients and healthcare professionals had the opportunity to speak about their own experiences and reflect collaboratively about the narratives. When they spoke about their own experiences they were able to reflect on their memories of the care process and they said they felt good about being able to recall situations that mattered to them. One parent said the experience reminded her of psychotherapy: It was so nice to talk with others who had the same, similar experiences—others who truly understand what you are going through. (Parent in the diabetes project) They [healthcare professionals] were shocked by our bad experiences, which also made it feel like we were “on the same side.” (Parent in the diabetes project) You can easily become “blind.” One thinks differently depending on whether one is a patient or a healthcare professional. It is great [to see] with fresh parent/patient eyes. (Nurse in the neo project) We understand each other better, now that we know a little more about each other’s activities. (Midwife in the neo project)
The IAR continually sought to reduce the gap between the experiences of professionals and patients and supported the creation of spaces for dialogues in which participants could co-construct a joint picture of the patient journey. For example, the IAR raised situations from the interviews that could be improvement areas, and suggested action.
Constructing a common picture
Healthcare professionals and patients increased their understanding of how various situations in the care process could be experienced. The reflective dialogues confirmed that the two groups took each other seriously. Professionals had to listen to the patients first, instead of giving directives and instructions. Patients highlighted the positive effects of “bouncing” their experiences off the professionals. The dialogue had synergistic effects, such as mutual understanding and development of improvement ideas. According to patients, this kind of dialogue felt rare in ordinary care meetings, which tend to focus on biomedical aspects. The collaborative reflections provided opportunities for seeing situations from different perspectives, and participants gained new understanding of the care process. For example, there were some situations that patients and healthcare professionals experienced in totally different ways. Both groups felt that a diversity of views came together during the projects in order to arrive at a more common perspective of patient processes. Participants said it felt good to share and listen to other people’s experiences. I learned that my “little banal” thoughts and experiences made a big difference in the care of other patients. It feels incredible and very beautiful. (Mother in the neo project) Very nice! Good to work with them (healthcare professionals) and nice to be taken seriously. (Parent in the diabetes project)
New challenging roles
Participants felt that the power relationship between professionals and patients was more equalized in the improvement/research process than in relationships in an ordinary care episode: As a patient you might not dare to give as much feedback to the healthcare professionals, but when you work together like this where everyone is on the same terms, it was very positive. (Mother in the neo project) It was also nice to learn about healthcare professionals behind the role. The collaboration became somehow more humane. (Parent in the diabetes project)
The patients’ new role was initially uncomfortable for most professionals, who did not know how to handle it. The patients initially showed a higher attendance and commitment than the professionals. One of the improvement facilitators in the diabetes project felt frustrated that the professionals did not show commitment from the beginning: It felt strange and frustrating that the healthcare professionals did not receive the input and offer of assistance to the same extent as the offers were given by parents. (Improvement facilitator in the diabetes project)
The healthcare professionals were initially anxious to take responsibility for all the improvements in the projects. The IAR had to suggest collaboration with patients and support joint improvement work. The IAR noted that the professionals appeared to be ashamed that they might not have provided good experiences for the patients. They felt motivated to improve because they thought it was their duty to do so, and the role of a patient/parent as an improver seemed odd.
Some patients’ suggestions for improvements and knowledge exceeded those of the professionals. This difference contrasted with normal practice, in which professionals are usually superior based on their professional medical competence.
Hence, in the final stages of the projects, the professionals expressed that the role of patients as co-designers was obvious and should always be considered in all healthcare improvement projects. Patients shared that expectation: I hope that you are satisfied and continue to use us patients for development purposes. (Parent in the neo project) It feels like the right way to do improvement work. We as healthcare professionals cannot know how patients experience different situations if we don’t ask them. (Ward manager in the neo project) We work as a team and I am probably a “team person” and believe in the synergy effect of more value, if we can have a stimulating dialogue. It is absolutely necessary to work in this way! Good improvements, not difficult to implement, but healthcare professionals do not find them by themselves. (Manager in the neonatal project)
Healthcare professionals leaving the comfort zone
The fourth emergent theme was stepping out of one’s comfort zone, which relates to established patterns of improvement work that were challenged in the projects. Initially, the healthcare professionals were not excited about the idea of working with patients in improvement projects. This attitude was particularly evident in the diabetes project because the patients and professionals still had a care relationship, whereas in the neonatal project the patients had ended their care episode. Parents initially found it strange to work collaboratively on improvements; they were unused to coming up with suggestions for how to improve their children’s care. The professionals also felt uncomfortable and feared being criticized or accused of not doing their work well. At the initial collaborative meetings, both parties felt nervous and tense. There was a certain excitement and anxiety in the air at the beginning, but it decreased later on. (Improvement facilitator in the diabetes project)
Patients and healthcare professionals believed that patients can help drive improvement projects and are an untapped resource for healthcare. Professionals alone cannot identify all the improvement areas that matter to patients. During the projects, healthcare professionals became aware of new information and collaboration between professionals and patients became a natural way of working with improvements. Patients expressed trust in the approach and sought increased use of EBCD in healthcare. It feels very good and natural as a patient to be involved and make suggestions for improvement through experiences. (Parent in the neo project)
Discussion
This section starts with a discussion of the findings in relation to earlier research and then discusses the benefits of combining AR and EBCD.
Strong professionals in healthcare have traditionally not allowed patients to be involved in improvement work (Andersson, 2015). The present paper shares experiences that may be of value when testing new approaches to develop healthcare that involve patients in collaboration with healthcare professionals.
One experience that the patients and healthcare professionals shared in the projects in this paper was that the variety of perspectives from participants stimulated different interpretations of the experiences and the findings that emerged. The patients had the whole picture of the process, whereas healthcare professionals saw only occasional episodes and were sometimes blind to the patient’s experience. Thus, the patients have important insights about how to make improvements. This information can be important for quality improvement work in healthcare, as argued in earlier research (Bate & Robert, 2006). Luxford et al. (2011) claimed that the most common barrier to an increased patient focus is the attitude of professionals. In the presented projects the professionals developed a “patient-focused” mindset during the reflective dialogues; in that way, the dialogues helped cross the above-mentioned barrier. Bate and Robert (2007) highlighted that EBCD can help to approach the shift from a strong management orientation to a more user-centric organizational approach. It is important for healthcare professionals to realize that the care they think they provide is not always the care that patients experience (Larkin et al., 2015). During the reflective dialogues, participants in the studies constructed a common picture of the care process. These dialogues helped reduce the gap between the experiences of patients and of healthcare professionals and helped to identify and prioritize improvement areas. Earlier research related to reflecting dialogues in AR aligns with these findings (Reason & Bradbury, 2009).
Participation in the projects challenged existing roles that had been assumed by professionals (Luxford et al., 2011) and patients, and challenged them to develop new roles as co-designers during the improvement process. The collaborative approach contributed to learning in the context of the professional–patient relationship and the patients in this study perceived an increase in equality between professionals and themselves. Patients highlighted the different role that the projects offered them, which was unlike what they were used to when meeting with healthcare professionals. These findings support earlier research related to new understanding, relationships, and a more equal partnership (Iedema et al., 2010). The AR approach supported reflections about patient involvement in improvements, and the IAR observed a decreased professional dominance and an empowered patient role. This finding aligns with earlier research that indicated a power structure shift between patients and healthcare professionals (Tritter & McCallum, 2006). In the diabetes project, a social network was funded to support a sustainable co-design relationship between healthcare professionals and patients. In the projects, the combination of EBCD and AR helped healthcare professionals to leave their comfort zone and venture into projects that entailed new roles and a new set of medical practices.
Previous work on EBCD has shown that patient involvement can leverage healthcare improvement (Bate & Robert 2006), but the present study shows four ways in which AR can enhance this effect: (1) reflective dialogue, (2) knowledge development beyond the actual project, (3) greater legitimacy, and (4) interplay between EBCD and AR enable results beyond each of the approaches:
EBCD is based on sharing experiences—mainly listening to others—while AR provides a reflective dialogue on these experiences, which promotes a common view of care practices (see Iedema et al., 2010). Reflective dialogues during the projects affected the outcomes in several ways. Both individual and collaborative reflections were stimulated by the preconditions for dialogue that AR brought to the EBCD process (Iedema et al., 2010; Reason & Torbert, 2001). Arenas for dialogues were provided several times during all steps of the project. Participants also engaged individually in reflective practice after the project, as first-person inquiry when completing the questionnaire. Knowledge development became more extensive because reflection goes beyond the actual improvement project to include patient involvement, general improvement work, and the quality of specific care processes (in this case, care for diabetic children and neonatal care). The research agenda lent greater legitimacy to the project and widened the impact of the results, which is also mentioned in earlier research (Payne et al., 2011). For example, the projects have been presented at conferences and in news articles, and the diabetes project has been included in films related to service design. It can be assumed that a research agenda also will improve sustainability, as there is a responsibility to report a result. The interplay between the EBCD methodology and the AR approach created value beyond each. This study illustrates that the AR approach can strengthen the conditions that previous research has shown to be important for successful EBCD projects: equal partnership, new roles, and dialogue. The collaborative power of dedicated healthcare professionals and patients resulted in collaborative learning and several accomplished improvements (Gustavsson, 2014; Gustavsson et al., 2016).
The dynamic processes of AR and EBCD strengthened the results of the actual improvement projects and generated knowledge about patient involvement in quality improvement for the organization. However, the AR element caused the results to extend beyond the organization and also reach other healthcare organizations and the research community. A traditional research project without the “action” part may not have supported knowledge development during the improvement work or the participants’ roles, as it did in this case.
Conclusion
Patient involvement in healthcare improvement is challenging in many ways, but this paper also shows the potential of AR and EBCD to influence both professionals and patients to develop new roles as co-designers. Leaving their comfort zones, examining new ways of interacting with each other and sharing experiences all serve to promote eye-opening situations that will encourage healthcare professionals to embrace new common pictures of care. Managers are often willing to involve patients in improvement work, but lack the knowledge and experience of how to do it (Andersson & Olheden, 2012; Bate & Robert, 2006; Iedema et al., 2010). This paper may help fill that gap of knowledge and practical experience. There is also a contribution in the area of shifting focus from healthcare professionals to patients in healthcare improvements. Accordingly, the findings strengthen earlier research and show that the combination of EBCD and AR is a promising approach with which to address the challenges of patient involvement in healthcare improvement.
Footnotes
Acknowledgements
This paper would not have been possible without the participants in the two pediatric improvement projects, and we are incredibly grateful to them for their contributions to our collaborative research. Also, we sincerely thank the management teams of the pediatric and obstetric clinics at Skaraborg Hospital, Sweden, for their support and engagement.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research and Development Centre, Skaraborg Hospital.