
Abstract
There is considerable literature describing the use of Change Laboratory as a simultaneous research and intervention methodology in workplace settings. However, there is limited literature describing Change Laboratory from the researcher-facilitator perspective. This paper examines the ethical dimensions of Change Laboratory from this perspective and specifically how a ‘rule of care’ became a conscious rule. The context is a series of Change Laboratories implemented with Centre Directors and Educational Leaders from early childhood education and care centres in Darwin and Melbourne, Australia. Based on our analysis we attribute the emergence of this rule to a particular vulnerability of the participants: that they were all recruited from centres that had been publicly designated as Working Towards National Quality Standard requirements for quality early childhood education and care practices. We present evidence of this ‘rule of care’ in our work as researcher-facilitators from our data. We conclude that attention to a ‘rule of care’ is necessary to support transformation, particularly for vulnerable participants such as Educational Leaders.
Keywords
Introduction
There is now a considerable body of literature describing the use of Change Laboratories (Engeström, 2007, 2015) as a simultaneous research and intervention methodology in workplace settings. Researchers using Change Laboratory have worked with groups as various as librarians (Engeström et al., 2012), architects and engineers (Kerosuo et al., 2012), homeless people (Sannino, 2020) and inter-professional groups (Edwards, 2011) to expand and renew local work practices. Although there are good sources that explain the principles and practices of Change Laboratory (Edwards, 2012, 2016; Engeström, 1994, 2015; Vikkunen and Newnham, 2013), there is only a limited literature that describes Change Laboratory from the research-facilitator point of view in the context of actual interventions. This may be because one of the principles of Change Laboratory is that the researcher-facilitators, with the workplace participants, together form a collective ‘subject’ in the Change Laboratory, sharing the object of expanding the meanings and implementation of valued practices. However, as Nuttall (2022) has argued, researcher-facilitators have particular responsibilities within Change Laboratories, including attending to ethical dimensions of research and practice that may not be immediately obvious to the workplace participants or facilitators.
This paper explores one such responsibility, related to how care is conceptualised and enacted by researcher-facilitators as a mediating ‘rule’ as an aspect of Change Laboratory methodology. The context for the study is a series of Change Laboratories implemented with Centre Directors and Educational Leaders from early childhood education and care centres in Darwin and Melbourne, Australia. Although the rule that ‘Change Laboratories provide a caring environment for learning and development’ was implicit, rather than explicit, for us at the commencement of the intervention, it rapidly became a conscious guideline in our work. In the paper we attribute this to a particular vulnerability of the participants: that they were all recruited from centres that had been publicly designated as Working Towards National Quality Standard requirements for quality early childhood education and care practices. This designation meant that the participants had been subjected to public judgement of their early childhood centre and received a rating less than the required Meeting National Quality Standard or higher. They sought to change this rating so were eager to engage in the Change Laboratories. However, they were simultaneously concerned about their capacity to lead innovative practice change in their respective centres.
We begin the paper by outlining the policy context that has brought about this exposure to public judgement for Australian early childhood education and care services, and touch on literature that has attended to questions of quality, quality assessment and the role of leadership in these settings. We then provide a description of the research design, including the implementation of the Change Laboratories and our approach to data analysis. Before turning to data that illustrate the methodological significance of a ‘rule of care’ in Change Laboratory facilitation, we expand on the concept of care as we came to understand it in our work, drawing on Tronto (1994, 1998) and Puig de la Bellacasa’s (2017) ‘matters of care’. We conclude by reflecting on how one of our research questions – What effects does the project methodology have on leaders and on their leadership practices in centres rated ‘working towards’ against the National Quality Standards? – came to be complemented by the methodological question: How can researcher-facilitators contribute to the effectiveness of Change Laboratory methodology by attending to a ‘rule of care’?
Public judgement of Australian early childhood education and care services
The Australian context for the study is a set of policy reforms that has increased the focus on the quality of early childhood education and care services (Nuttall et al., 2022). Behind these reforms are a set of policy rationales that connect high quality early childhood education and care with ameliorating the effects of early deprivation and building human capital (Garcia et al., 2016). In this context, the National Quality Framework (NQF) (Australian Children’s Education and Care Quality Authority [ACECQA], 2023), introduced in Australia in 2012, saw new quality standards introduced to improve early childhood education and care services. The NQF brought, what was a complex and multi-jurisdiction regulation and quality assurance system of ECEC, into a national approach and includes four key components:
(1) the National Law and National Regulations (NSW Government, 2011)
(2) the National Quality Standard (NQS)
(3) an Assessment and Rating process (A&R)
(4) Belonging, being and becoming: The Early Years Learning Framework for Australia (Department of Education, Employment and Workplace Relations [DEEWR], 2009)
The NQS defines ‘quality’ through seven quality areas: Educational program and practice; Children’s health and safety; Physical environment; Staffing arrangements; Relationships with children; Collaborative partnerships with families and communities; and Leadership and service management. Each quality area consists of standards (totalling 15), with each standard having a number of elements (totalling 40). ACECQA is the statutory body supporting the implementation of the NQF, and regulatory authorities in each state and territory of Australia are responsible for the A&R of services against the NQS. Following the A&R process, a centre receives a rating against each standard as well as an overall rating based on these standard-level ratings. Rating descriptions are provided in Table 1. Centres who receive a rating of Working Towards National Quality Standard or Significant Improvement Needed will be rated again sooner than centres that have achieved Meeting National Quality Standard or higher.
NQS ratings.
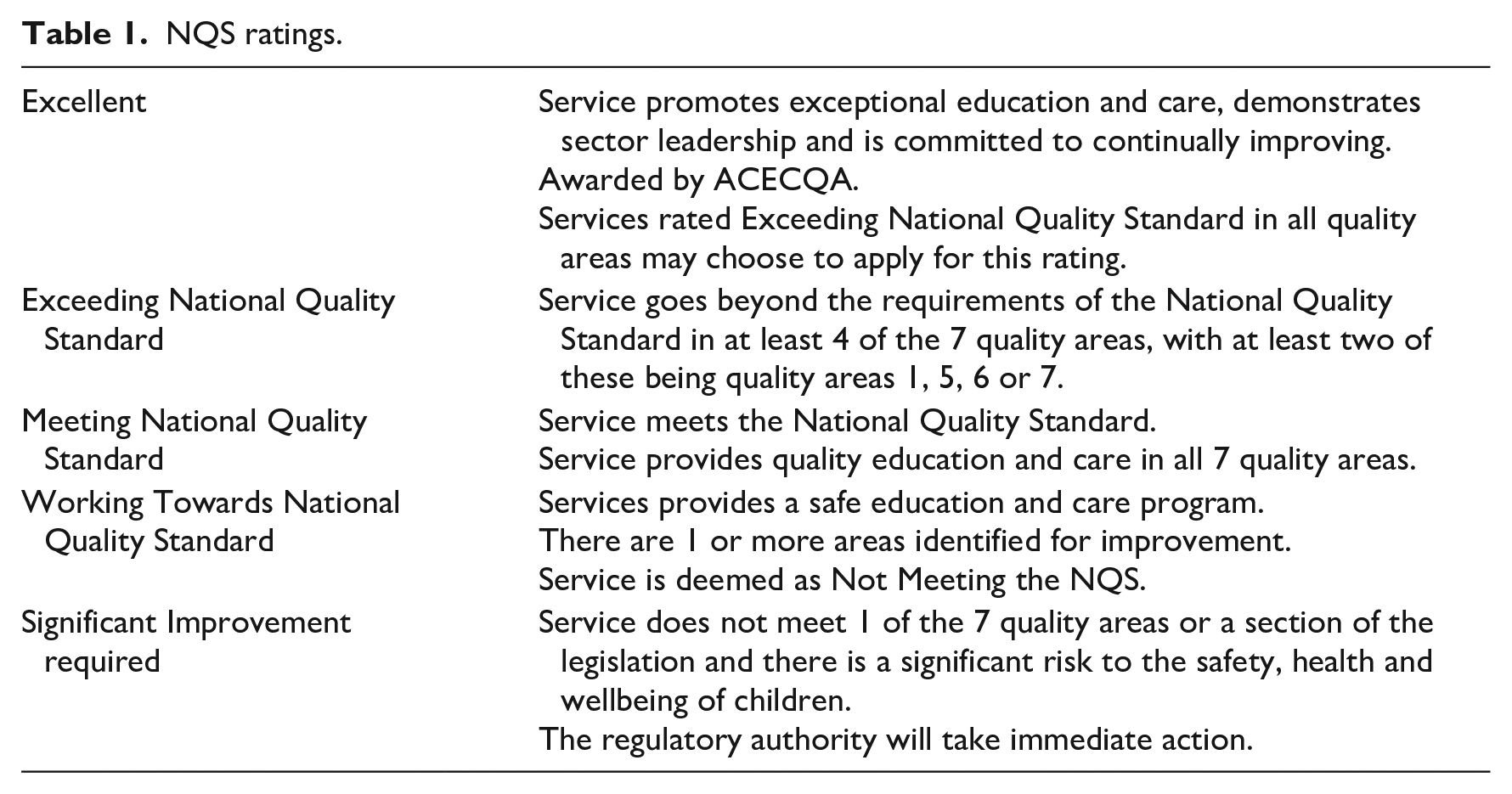
However, in this A&R context we note that ‘quality’ is a contested term in the early childhood education and care literature. It has been discussed and debated extensively with no agreed definition, alongside vigorous debate about the ‘rating’ of quality (e.g. Dahlberg et al., 1999; Hunkin, 2019; Siraj et al., 2019). It is not our intention to enter this debate in this paper. For the purpose of this paper, we define ‘quality’ in the way it is conceptualised in the National Quality Standards (NQS) as well as the National Law and Regulations (NSW Government, 2011) because this is the definition to which the participants were subject. All participants worked in centres rated as Working Towards National Quality Standard, a rating that publicly positioned the centres involved in this project as not meeting the NQS. This rating is public because centre providers are mandated to display their rating outcome in a position that is visible from the main entrance of their service, and ratings are also published on Starting Blocks and Child Care Finder websites. These websites were established to help parents find ‘the best service for their child’ (Starting Blocks, no date).
Togher and Fenech (2020) argue that centre leadership plays a critical role in how centres perceive the A&R process and their centre’s outcome. This connection with leadership aligns with one of the key policy drivers of the NQF: the role of the Educational Leader in lifting quality. This role is mandated in the NQF under the National Law and Regulations (NSW Government, 2011) and is reflected in NQS Quality Area 7.2: Leadership which states, ‘effective leadership builds and promotes a positive organisational culture and professional learning community’ (Australian Children’s Education and Care Quality Authority [ACECQA], 2020: 91). Element 7.2.2 requires that: ‘The educational leader is supported and leads the development and implementation of the educational program and assessment and planning cycle’ (Australian Children’s Education and Care Quality Authority [ACECQA], 2020: 91). In this way the NQS claims a correlation between educational leadership and NQS Quality Area One: Educational program and practice. This correlation draws on research showing that leadership influences the quality of educational program planning, and in turn, children’s learning outcomes (Douglass, 2019). In a systematic literature review, Douglass (2019) notes:
. . .effective leaders have greater knowledge and skills to develop staff leadership, a positive workplace climate, and an organisational culture of learning and improvement. They possess the skills to support curriculum development, implementation and pedagogy. Effective leaders may also establish alignment and coherence in the centre’s educational program across curriculum teaching and assessment. Together, these can result in high levels of process quality. In addition, when staff leadership is supported, staff can positively impact process quality, and can contribute to a positive organisational climate that supports positive staff-child interactions. A positive workplace climate and culture of continuous improvement, as well as educational program coherence, are associated with process quality. (p. 21)
In effect, leadership has been positioned as a key policy strategy for raising quality (Nuttall et al., 2022) and this is reflected in NQF policy implementation texts that state:
The Educational Leader has an influential role in inspiring, motivating, affirming and also challenging or extending the practice and pedagogy of educators. It is a joint endeavour involving inquiry and reflection, which can significantly impact on the important work educators do with children and families. (ACECQA, n.d.: 1)
Nuttall et al. (2022) argue this policy strategy has worked to responsibilise the Educational Leader, and in turn, make them accountable for program quality at their centre. Rogers’ (2021) research also highlights the effects of prescribed notions of quality on educational leaders arguing that ‘the effect of over-regulation in ECEC can result in a reduction in creativity and confidence’ (p. 553). There is also the risk that innovation in practices for quality improvement decreases, replaced by the feeling that policy is prescriptive and authoritarian (Maloney et al., 2019; Rogers, 2021). Questions must therefore be asked of the A&R process for quality improvement and what this means for those positioned as responsible for the centre’s rating and for ongoing quality improvement. In particular, it is important to understand the impact on Educational Leaders of receiving a Working Towards National Quality Standard rating, since they are positioned as responsible for leading centres publicly identified as operating at a level below the mandated standard. In this paper, we focus on one aspect of our work with the participants in our study, who were experiencing the vulnerability of being publicly positioned as not yet leading centre practice at acceptable standards of quality: the significance of care in the facilitation of practice-developing interventions.
Research design
Change Laboratory methodology
Change Laboratories support participants to systematically map workplace practices and identify tensions in workplace systems that are limiting achievement of important goals. Researcher-facilitators participate in the Change Laboratories alongside participants and introduce concepts and artefacts with the potential to support workplace participants in transforming workplace practices at a systemic level. A total of six 2-hour Change Laboratories were conducted with participants in Darwin and the same in Melbourne, over a period of 9 months. All Change Laboratories were video recorded, supplemented by fieldnotes and photographs of artefacts (posters, note-taking, diagrams) produced by the participants. As per Change Laboratory methodology (Engeström et al., 1996), in the first two sessions participants were supported to analyse current workplace practices and identify relationships between aspects of these practices that were limiting ongoing quality improvement in their service. In subsequent sessions, participants identified leadership practices they could implement with their teams to design (or redesign) important concepts and/or artefacts for quality improvement. Some examples of these changes during the project included changes to the allocation of educator tasks, new approaches to recording and assessing children’s learning, and shifts in important concepts such as ‘sustainability’ and ‘documentation’ and related practices. Between Change Laboratories the participants and their teams implemented these new concepts and/or artefacts, and examined their effects, as evidenced through changes in practice. Progress with these changes was reviewed and leadership activities redesigned in the later Change Laboratory sessions. Interviews with the pairs before and after the Change Laboratories allowed for pre-and post-comparison of participant perspectives on their leadership and engagement with quality improvement, including their understandings of the A&R process.
Participant recruitment
Following the approved ethical procedures by Henderson and Nuttall’s respective university Human Research Ethics Committees 1 , 20 Australian participants were recruited through emails to ECEC services rated as Working Towards National Quality Standard. Pairs of leaders from 10 services (usually the centre Director and Educational Leader) participated in the Change Laboratories (Engeström, 2007). Of the 10 centres, 4 were located in the city of Melbourne, in the Australian state of Victoria, and 6 in the city of Darwin, in Australia’s Northern Territory. The findings presented in this paper are drawn from the project data set as a whole but, for reasons of keeping within the permitted word length whilst maintaining coherence within the accounts of Change Laboratory sessions, data for this paper are taken from the Melbourne cohort only.
Approach to data analysis
Our analysis of the intervention data set (pre- and post-intervention interview transcripts; video records, field notes, photographs and research diary records of the Change Laboratories) proceeded as a series of ‘passes’ across the data set as a whole. Data pertaining to individual centres were aggregated into case records that allowed us to track change over time on a centre-by-centre basis. Cross-data analysis was also undertaken to identify commonalities as well as examples of unanticipated phenomena.
Our initial analysis was deductive, drawing on key concepts from cultural historical activity theory (CHAT). CHAT is an object-oriented activity system approach to understanding how collective systems (e.g. an early childhood centre) can be conceived as a series of networks of sociocultural relations and activity (Engeström, 2000). CHAT contends that an activity system’s goal-oriented actions are mediated by tools, shaped by sociocultural norms, rules, divisions of labour within a community (see Figure 1). Our deductive analyses were initially undertaken by individual members of the team, then reviewed by a second member of the team. Insights from this phase were then aggregated and re-analysed for the purposes of theory-building and findings from this work will be reported on in a future book publication. Inductive analysis was also undertaken mainly after the deductive analytic phase (but not exclusively, as some important unanticipated and therefore inductive concepts were identified from the outset) and have been reported elsewhere (Henderson et al., 2022; Martin et al., 2020). Our inductive analysis relied both on basic interpretive principles (Klien and Myers, 1999), such as identification of repetition of key words and phrases. We also conducted inductive analysis at the level of overall meaning, using discourse analytic advice offered by Willig (1999) to attend critically to the meaning and substance of participant talk. Again, these analyses were initially individual, then shared across the team to check the credibility of interpretations. Using this inductive approach, we noticed how ‘care-full’ practices on the part of the researcher-facilitators were evident over the course of the Change Laboratories. This led us to engage in methodological triangulation whereby we brought deductive analysis of ‘care’ according to how it was operating within a CHAT framework together with speech and vignettes in the data we had identified inductively as ‘care-full’. This allowed us to conceptualise how a ‘rule of care’ was mediating researcher-facilitator practices within the Change Laboratory itself.
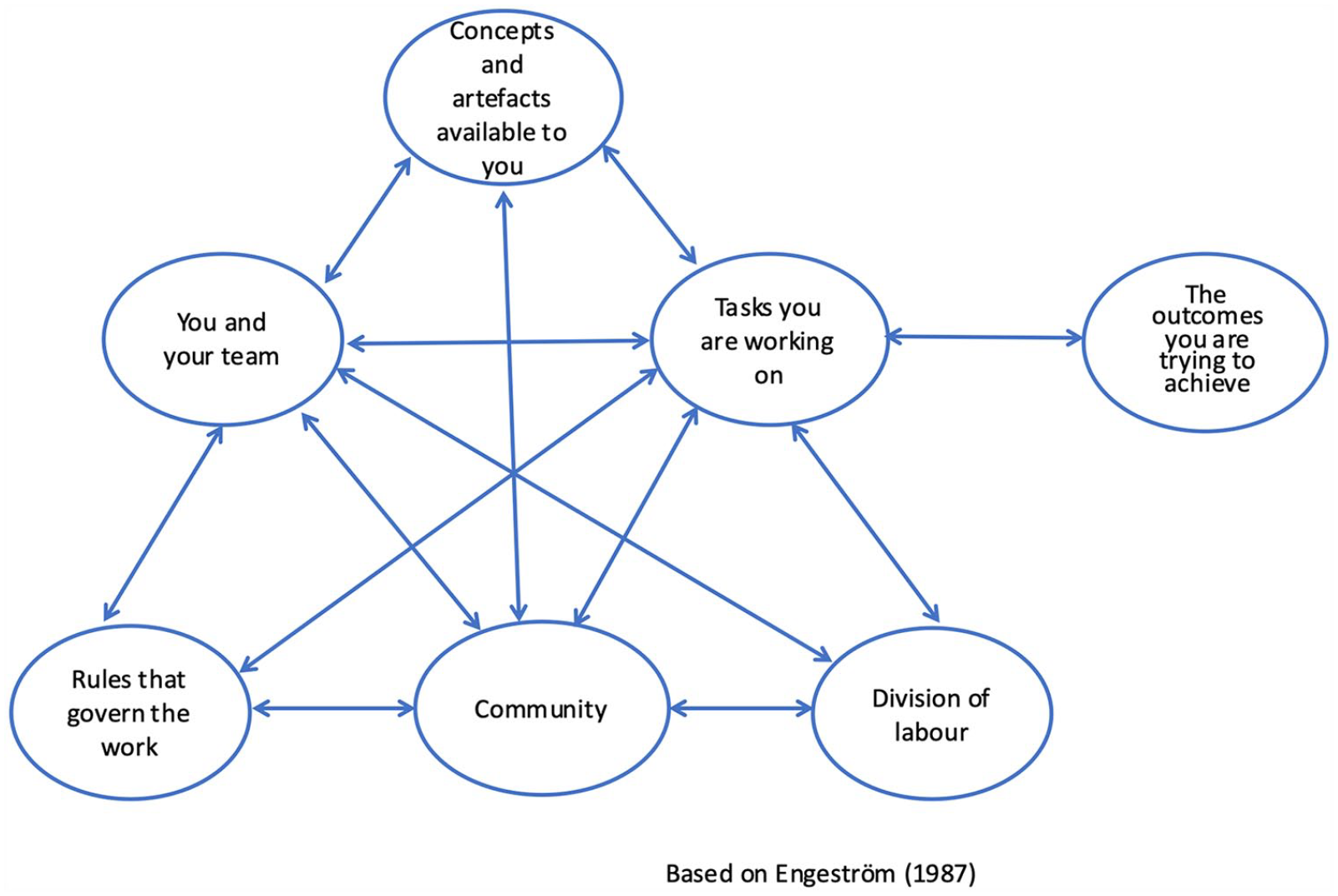
Graphical representation of an activity system.
In other words, we realised (but only retrospectively) that ‘caring about’ the participants as subjects of the A&R system that had rated them as Working Towards National Quality Standard was an implicit rule being applied by us as researcher-facilitators.
We were cognisant of what underpinned a Change Laboratory methodology: a process that aims to ‘bring to consciousness the prevailing contradictions within systems of activity’ (Nuttall, 2022: 5). We were aware of ‘the ethics of attempts to change the practices of others’ through Change Laboratories (Nuttall, 2022: 14). We knew this could be perceived as risky work for a centre that had been publicly judged as Working Towards National Quality Standard. We also understood the burden of responsibility they carried for this rating as ‘leaders’ of their centre, and their sense of responsibility to move this rating to Meeting National Quality Standard or higher (Nuttall et al., 2022). Therefore, we were conscious as researcher-facilitators that in this research context asking the participants to engage in change through innovation could potentially be perceived as risky work. As our analysis progressed, and we asked the question ‘What effects does the project methodology have on leaders and on their leadership practices in centres?’ We also began to see how the vulnerability of the participants had had an effect on the facilitation of the Change Laboratories. This led us to the methodological question that forms the focus of this paper: ‘How can researcher-facilitators contribute to the effectiveness of Change Laboratory methodology by attending to a “rule of care”?’
Conceptualising care
A rule of care within the activity system of a Change Laboratory means that this rule will regulate behaviours as well as conventions, and in this instance, how we interacted with our participants as the researchers-facilitators of the Change Laboratories, and how they, in turn, interacted with us. Rules can therefore either sustain power and positionality in a Change Laboratory or recognise the need to shift power and status to support participants’ agency (or some combination of these). To better understand how the dynamic of a ‘rule of care’ might have been mediating care-full practices by us as researcher-facilitators, we turned to Tronto’s (1998) work on care, which argues that care is crucial to the maintaining of all of life. For Tronto (1998), care is both a ‘mental disposition’ as well as a set of ‘practices’ that can critically examine notions of care that create positions of power and powerlessness. She suggests there are four phases to caring: caring about, taking care of, care-giving and care-receiving (Tronto, 1994). Caring about involves recognising the need to care that can see beyond one’s own life experiences. Taking care involves assuming responsibility for caring and understanding how that care can facilitate the flourishing of life. Care-giving is about directly meeting the needs of care that requires action beyond just tokenistic measures. Care-receiving is about recognising that the one receiving care ‘will respond to the care it receives’ (Tronto, 1994: 107). This final phase Tronto (1994) argues is important as it provides us with the ‘only way to know that caring needs have actually been met’ (p. 108). These four phases, Tronto (1998) argues, provide a more complex understanding of what care involves and to recognise it as ‘an integrated holistic process in which those who cared about a problem take responsibility, provide care, and receive thanks when all goes well’ (p. 17).
Adding to this we drew on Puig de la Bellacasa (2017) who argues that to ‘care for’ is an ethical practice, and as such, to think with care you must ‘probe further into imagining how a style of thought can contribute to caring thinking in living with other than humans’ (p. 19, original emphasis). This means a rule of care must be able to generate questions around issues of responsiveness, responsibility and attentiveness to our participants. Specifically, it meant that we needed to be able to create a secure, supportive environment for the Change Laboratory participants, knowing they had been publicly judged as Working Towards National Quality Standards, and therefore, publicly deemed as Not Meeting the National Quality Standards. In sum, it was about being able to meet their needs whilst also asking them to engage in a process of innovative change for the purpose of quality improvement. Although care for participants might seem an obvious and necessary feature of any practice intervention, we had not appreciated the extent to which care-full facilitation was necessary to the process of transformation being undertaken by the participants.
The rule of care
We now present our analyses that identified our rule of care in the Change Laboratories. Data are the video transcripts from the Change Laboratories conducted with the Melbourne cohort. We present three time points in the project that we have identified in the analyses as critical to the establishment and expansion of this ‘rule of care’. Time point one is Change Laboratory One, time point two is Change Laboratory Two through to Five and time point three is Change Laboratory Six. Our aim is to illustrate how the rule developed, and then, further expanded across our facilitation of the project.
Time point one: Caring about . . . positioning
As we commenced the project, we were conscious of the participants’ perspectives on their assessment and rating process and outcome. In the pre-Change Laboratory interviews some participants had openly shared their sense of frustration and resentment towards the rating awarded. In this talk, a strong theme in our inductive analysis was concerned with how the rating had publicly positioned them and their centre with a rating that said their centre was not a quality centre. One participant reflected this positioning when she stated: ‘I think everyone was just like “you’ve got to be kidding me, like seriously.” Do you know what I mean. . .very demoralising’ (Maisie – Director). There was a sense of disbelief they were awarded this rating because they believed strongly that the centre was a quality centre: ‘We feel quite confident that we are a quality service. What we do. . .It’s a quality service. All our families say that. Anyone who walks in the door says that. So, its frustrating. . .very disappointing’ (Lisa – Educational Leader).
Commencing in Change Laboratory One, participants were provided with an overview of the Change Laboratory methodology as well as given time to share details of their centres. It was during this discussion that Maisie asked about the sampling method of the project:
. . .I’ve just noticed a common theme between us. So when you picked the centres did you have a common denominator? Joce: We can tell you the sampling method we used. . .
Joce continued to openly share the sampling methodology that included using ACECQA’s National Registers to identify centres who had an overall rating Working Towards National Quality Standard and, from that sample, further narrowing down by identifying centres that received Working Towards National Quality Standard ratings on Quality Area One and Seven, followed by identifying centres by location as the final sample of centres to be invited to participate. Maisie responds:
Yes it’s interesting because it’s not like anyone here has said, you know, from a 200 place multi-national corporation centre. . .we all have something in common in our size and location. Its very interesting to me because it makes me wonder what [the assessors] are really looking at when they come out to look. Because I bet you all have [pointing to all the participants] really good centres. Do you know what I mean?
Maisie continued to outline her concerns about the assessment and rating process, noting that not one participant had talked about issues such as high staff turnover or poor quality care. In response to this Joce confirmed Maisie’s observations:
It’s interesting, this [Melbourne] group compared to our Darwin cohort, who do have high staff turnover and some of them are from multi-national corporate owned centres. Whereas here, you all do have stability. So it will give us a comparison. . .help us identify what are the contextual issues where the policy touches down. So we’ll be unpacking this lots with you and working with you through these contextual issues.
Maisie thanked Joce for this information noting the support offered to unpack the contextual issues. She was then reassured that her question was ‘a great question, a really important question. We need to talk about these things’.
Maisie had been consistently questioning the rating her centre received and her talk indicated a kind of mistrust towards the assessment and rating process. She was confused how quality was being determined in this process and indicated that, from her perspective, she could not see how her centre or the other participants’ centres could be rated as Working Towards National Quality Standard. Joce responded with acknowledgement of Maisie’s concerns. Maisie was provided with information that she sought and was given permission to openly question the assessment and rating process, whilst also not further adding to Maisie’s questioning of the A&R process.
Evident in this exchange are acts of caring about Maisie’s lived experiences of the A&R system that has publicly judged her centre. This is consistent with Tronto’s (1998) first phase of care, caring about, which is the recognition of a need to care that can see beyond one’s own life experiences. The research team have never personally experienced this A&R process; rather, they can only understand it from their research position. We could have responded with information on the training of the Authorised Officers who go out to centres to conduct the A&R, including both reliability and drift testing, to clarify for Maisie the checks in place to ensure the robustness of the A&R process 2 . If this was the approach, we would have established our authority and power over the participants. Instead, we remained attentive to their positioning both in the Change Laboratory and within the A&R process that has publicly judged them. We would argue our attentiveness was what signalled, at this time point, an implicit ‘rule of care’. We understood our positioning and their positioning. We were cognisant that we were asking them to trust us as we asked them to engage in examining their practices for the purpose of creating change, and we understood this would demand some risk taking on their behalf. The participants needed a safe place in which to do this work. We suggest this shows we were already taking care (Tronto, 1998) of our participants by assuming the responsibility for a ‘rule of care’ as the researchers-facilitators of the Change Laboratories.
Time point two: Caring giving. . .as an exchange
In this section, we present our analyses of the ‘rule of care’ in the light of Tronto’s (1998) notion of care giving, which is about directly meeting the needs of care that require action beyond tokenistic measures. Our analysis identified this ‘rule of care’ as care giving across Change Laboratories Two to Five. In Change Laboratories Two and Three each centre started the process of analysing their centre’s activity system. Contradictions between aspects of centre practice were surfaced in this process and with this came realisations that these contradictions were currently operating to inhibit each centre from realising their desired practices and outcomes. For example, analysis of practices at Violets Early Childhood Centre (all centre names are pseudonyms) identified a contradiction between a rule which allowed staff to choose shifts on the staff roster and a division of labour that positioned the second in charge staff member as responsible for achieving the object of continuity of care (see Figure 2). Similarly, Kokomo Childcare identified that a rule that said staff did not have to attend staff meetings was contradicting a motive object of fostering professional conversations (see Figure 3).
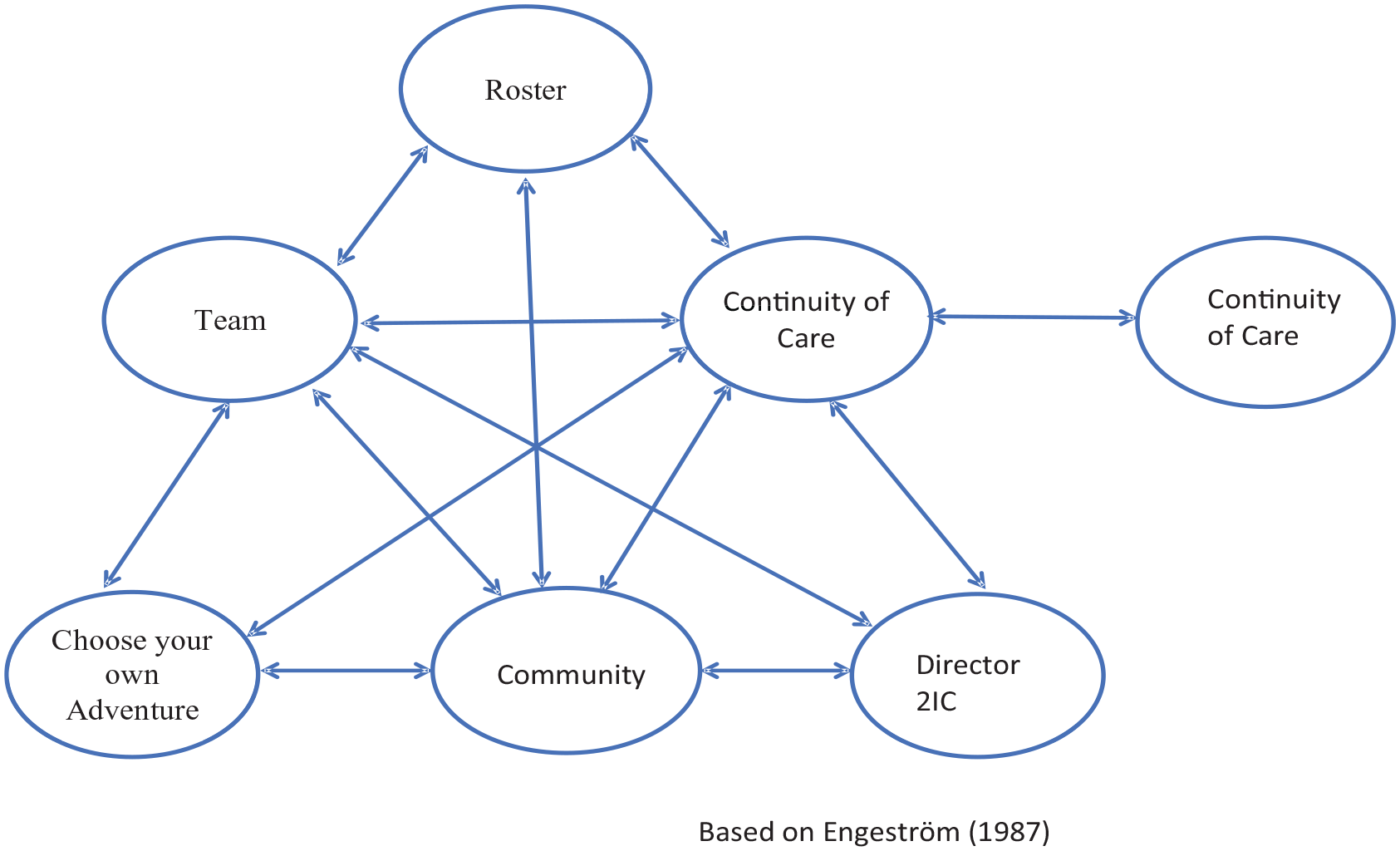
Violets Early Childhood Centre: Rule and division of labour contradiction.
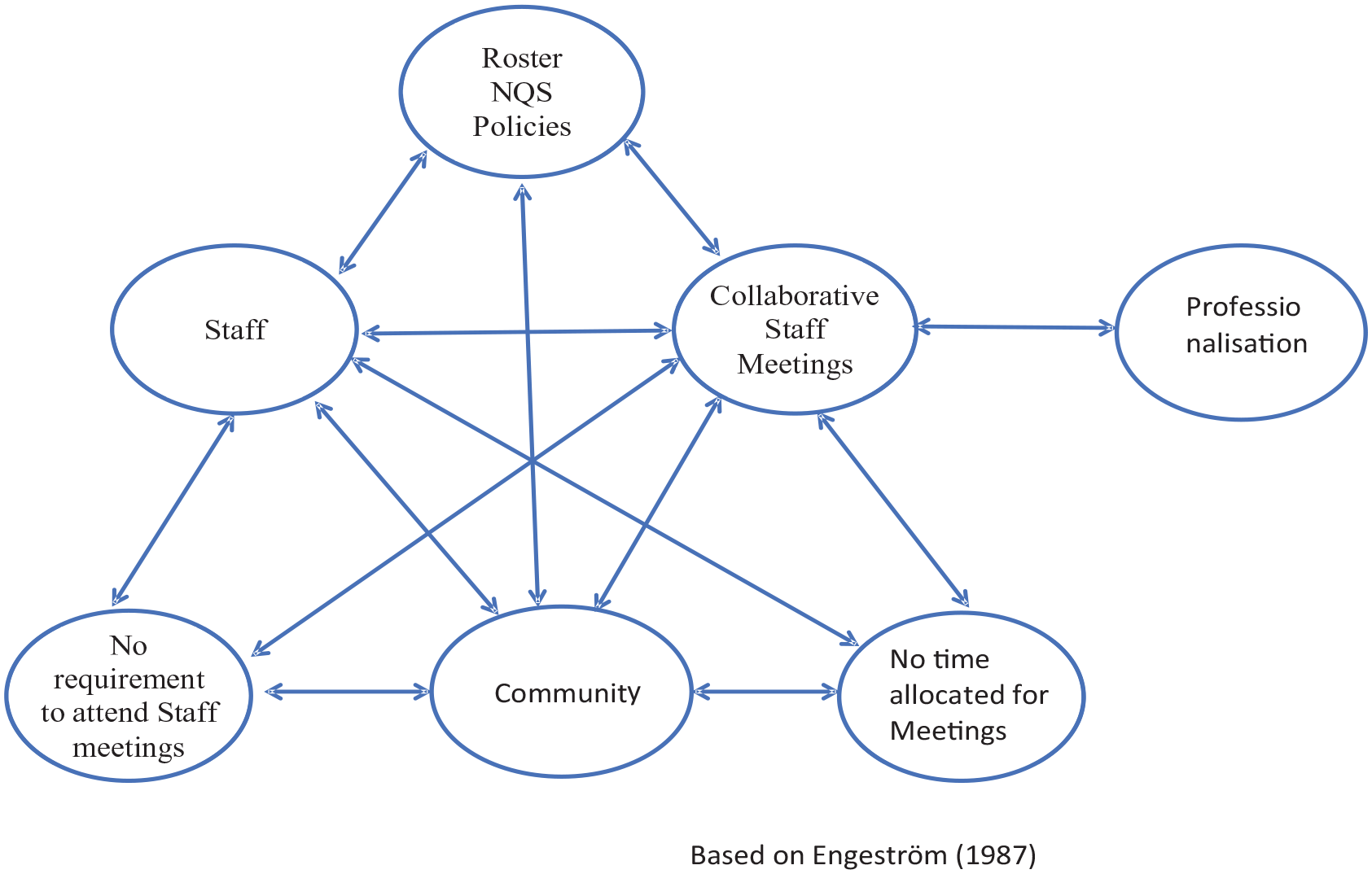
Kokoma: Rule, division of labour and object contradiction.
Templetons was experiencing what we named as a ‘crisis’ in their system, having just had a change of management which introduced significant change, including new rules, tools and divisions of labour. Analysing this change, the Kokomo participants noted:
Ellie: . . .the staff do not like the change . . . [they] are still currently doing what they were doing beforehand . . . they are saying ‘well I don’t want to do this, this is not how we do it. . . and I’m getting a lot of bite back . . . and before with the old company . . . all staff were accommodating into planning even though they were not off the floor programming, they were taking down jottings, assisting team leaders. [Name of researcher-facilitator]: They were feeding into the plan? Ellie: Yeah, and I personally don’t like that ‘you’re the team leader and I’m the assistant’. I hate it. I’ve never worked like that. I like it more ‘no we are all co-educators’. . .I guess since the new company’s come in they are very much like ‘everyone needs to do it, everyone needs to be on the planning’ and there’s that little bit more push towards it. Whereas before . . . it was very relaxed. Kristy: So now they’re getting pulled up on their accountability. Ellie: Correct Linda: So the rule has become explicit from management? Ellie: Yes Joce: What you are describing is the classic contradiction in a workplace which is between rules and division of labour. So the rule is, certainly the rule from you as the leader, is that. . .we’re co-educators. . .The division of labour though is quite hierarchical, because [management] are going, there’s the leadership team and then there’s the room leader and then there’s assistants and so on. . . .and having hierarchy cannot co-exist and so that’s creating tension. . . Ellie: Yes Joce: Is this making sense? . . . Its very disruptive when new rules and tools get dropped in from above. Kristy: Yeah and it causes you to feel like you are just getting on top of one. . .[and] you just get another one thrown at you and your like (puts hands to head) Ellie: . . .it’s a debate with staff. . .why do we have to do this? You know? That sort of mindset. And I said to [the staff] they are just trying to implement things to be compliant. They are not asking us to go above and beyond. . .does this make sense? . . .Sorry. Joce: No, its good. This is really important. Its really disruptive.
In the vignette above, the response to Ellie’s felt need to say ‘sorry’ is mediated by a ‘rule of care’ that acknowledges the importance of all she has shared. Linda and Joce then turned to Elaine and Rita from Junipers, who had recently bought their centre, asking them about staff experiences of a change in management. Rita explained that staff did not trust them at first and this resulted in both staff resistance and resignations. Ellie responded by reflecting on her own personal style of leading people, noting that she feels she is sometimes ‘too lenient. . .I get beaten down’. Turning back to Ellie, Joce responded by noting that the objects motivating practice ‘always have a strong emotional component. . .hidden but it’s in there. And keeping things smooth always feels more comfortable, people will be happier. But being object oriented is what we are here to do not how to keep people happy. That will not let you realise your motive object’. Joce added to this by then providing Ellie with examples from previous Change Laboratory projects to further illustrate this point and the power of contradictions in systems in achieving quality improvement.
Focusing on the object of activity is critical in Change Laboratories in supporting participants in both analysing and changing workplace systems. CHAT, as a systems approach, see the unit of analysis as the system rather than individuals, allowing for workplaces to be examined through the elements of the system rather than the impact of individual behaviours. We would argue that, through a ‘rule of care’, we were able to acknowledge Ellie’s emotional labour then re-orient Ellie back to a system orientation. Mediated by a ‘rule of care’ we were then able to directly meet her needs with tangible measures, a practice that is central to care giving as defined by Tronto. In providing care-full attention to the ‘crisis’ Ellie was experiencing, new tools to support her were also provided, which in turn, would lead to tangible change taking place in her centre, as we outline in the next section.
Time point three: Care receiving . . . as relatedness
Care receiving is the response that arises from care giving. Tronto (1098) argues that care receiving requires both receiver and the giver to respond to the act of caring. Our analyses of data for the ‘rule of care’ as care receiving was most evident in the final Change Laboratory. In particular, the focus at this point in time had shifted from the impact of being rated Working Towards National Quality Standard to a responsiveness to care receiving as a form of relatedness between participants as well as the researchers-facilitators.
Introducing this workshop Linda noted how the Change Laboratory is a system itself, and how, within this system, the participants had been responsive to the methodology but also to each other’s journey. She talked about the rules of the Change Laboratories and that each one had seen participants demonstrate a deep moral commitment to supporting each other in the change process through such things as an attentiveness to the sharing of the lived realities of each participant. This was confirmed by the two educators from Junipers Early Childhood Centre who noted:
Elaine: Sometimes you go for PD and you see the barrier there . . . I mean its so easy. It comfortable . . . we’ve felt very comfortable. Rita: You are not there to dictate to us to do this, to get it right . . . it didn’t have that kind of approach. So, the way the workshops is done is good.
One key aspect of this final Change Laboratory was that participants created posters to represent, and then talk about, their change processes and outcomes. Rita shared at this time how the Change Laboratories opened up a space in which to engage critically with her own leadership practices and that ‘we had to work hard’ to do this but ‘your outside perspective has helped us see what we could not see’. In response, Rita was asked if it was also about giving herself permission to examine her own leadership practices for the purpose of quality improvement. Rita responded stating that ‘you have given us a space in which to do this though, to look at our leadership and make these changes’.
In a similar manner, Claire from Violets Early Learning Centre shared how the changes that they implemented were because they had learnt through the Change Laboratory work that they could implement change and that it was not something they needed to fear. She shared how she knew that with change there would be ‘resistance’ but when you are able to share with staff the reasons for introducing change through a system approach, there is less resistance and more support. She concluded that because of the Change Laboratories she knew that ‘we can change things’ and ‘when understood as a system and we are not changing individuals, we can change’.
Finally, Lisa and Maisie shared how the workshops facilitated a community in which they could feel a sense of belonging and support in which to engage in the work of change for quality improvement:
Lisa: I’ve quite enjoyed connecting with other educators from other places too Maisie: Yeah, and people I guess in the same position. That was probably the nice thing. . . Like I said on the very first day, no doubt everyone has a really nice centre or they wouldn’t be operating. That was quite a nice thing, . . . you talked to real people. Real people that we could relate to. Lisa: And that allowed you to connect and relate . . . to see things from different perspectives.
This is care receiving, where a ‘rule of care’ has been able to facilitate the development of a culture within the activity system of the Change Laboratories in which participants have been able to receive care as they engaged in the task of analysing their own centre’s systems, surfacing contradictions, and designing innovative change for the purpose of quality improvement.
Matters of care in Change Laboratories for early childhood leadership
Nuttall (2022) argues that Change Laboratory methodology demands ‘axiological responses’:
. . . considerations of what is valued and how this value will be represented. These questions include ‘Whose interests have been served historically by this contradiction? and ‘Who will benefit from the changes we design and implement?’ (p. 5)
Our formative intervention into the work of early childhood leaders commenced as a policy and practice problem that demanded an axiological response. We did not enter into this work without this understanding, but it was only through our post-project analyses we have been able to fully identify how our response took the form of a ‘rule of care’. Our ‘rule of care’ had us engaged in caregiving practices by paying attention to, and being responsive to, our participants as leaders who had all experienced the A&R system that determined their centres to be rated as Working Towards National Quality Standards. We noted in the introduction that there remains scant research into the enabling or constraining effects of receiving this rating. At Time Point One, we illustrated the material effects of this rating when raised by participants in the first Change Laboratory. It was something that was of concern and questions were asked of this rating process. Our response to this questioning was one of caregiving by being responsive and openly providing information and confirmation of the experiences of the A&R process and its outcome, and in particular, confirmation that ‘we need to talk about these things’.
We have shown that this ‘rule of care’ throughout the Change Laboratories was underpinned by a desire for transformation by our participants which is in keeping with Nuttall (2022) who raises the question ‘Who and what is being transformed?’ (p. 16). This question highlights the critical importance of being able to populate a ‘rule of care’ in Change Laboratories with care-full practices that support transformational processes for participants. Our participants came to us aware of their Working Towards rating and its material impact. In line with Tronto (1998) and Puig de la Bellacasa’s (2017) work on ‘care’, we were able to populate this ‘rule of care’ with practices that included: care-full listening and responding, care-full questioning; care-full holding of spaces for sharing; and care-full facilitation of relationships and relatedness that the participants told us made transformation of leadership practices possible in their centres. The analyses of Time Point Two and Three demonstrated this as the ‘rule of care’ moved from care giving as an exchange to care receiving as relatedness. The participants were able to explicitly identify and express this in the final Change Laboratory when they described how the Change Laboratories had become spaces that were ‘comfortable’ and where ‘connections’ and ‘relate(dness)’ were fostered, where seeing things ‘from different perspectives’ was permitted and encouraged, and where they were not told of one ‘right’ way of doing things. Indeed, experimentation was highly desirable within the Change Laboratory methodology. We argue this is a ‘rule of care’ at work making possible transformation of, and for, participants in Change Laboratory work.
On the matter of transformation, we return to our research question ‘What effect does the project methodology have on leaders and their leadership practices in centres rated ‘working towards’ against the National Quality Standards?’ and the methodological question that arose from this that has guided this paper: ‘How can the researcher-facilitator of Change Laboratories contribute to the effectiveness of Change Laboratory methodology by attending to a ‘rule of care’’? In answering this question, we first emphasise the point that we commenced this work with a deep sense of understanding that we were going to be working with participants who had been judged by an A&R system that positioned them publicly as Working Towards National Quality Standards. We intuitively understood the impact such a rating could have for leaders of these centres. Therefore, we argue that we entered into this work with an implicit ‘rule of care’ that brought with it an awareness and attentiveness to our participants and the impact of the rating even before commencing this work. We sensed it could impact their sense of agency in being able to make transformative change and that perhaps they would want to know how to better ‘comply’ with the standards in order to receive a Meeting National Quality Standards rating in their next A&R. Our attentiveness to the material conditions in which our participants were working, including the mandated definitions of quality that formed the basis of the A&R process, needed serious consideration when encouraging them to engage in transformative processes that asked them to take risks. In effect, we were intervening in their working lives. This is the ethical question that Nuttall (2022) raises, for if we are to intervene into the lives of those involved in Change Laboratories, then there must be serious consideration given to this question of who and what is being transformed. In this paper we have argued that a ‘rule of care’ (whether implicit or explicit) demands attention to the vulnerability of participants, such as those participating in this project. Our evidence suggests that incorporating a ‘rule of care’ can enhance the effectiveness of Change Laboratory methodology by creating an intervention environment where the risks of workplace transformations are reduced for participants.