
Abstract
The population of older adults is growing rapidly and there will be an increased need for psychological services for this population. Current estimates indicate a significant workforce gap such that all psychologists, regardless of specialty area, will likely be called upon to work with older adults. Education and experience in the care of older adults has been consistently connected with improved competence and interest in working with this population. Further, the APA requires that training programmes adequately cover aspects of individual diversity, though age-related education and training may be largely lacking and/or minimally addressed. The present study explores age-related training within a sample of psychology doctoral students. Participants (n = 85) consisted of doctoral trainees recruited via email (listserv) to complete an anonymous online survey as part of a larger study. Results indicate that (1) training in aging varies and is inadequate in some programmes; (2) knowledge in aging varies and is associated with training opportunities; (3) training in aging is less than training in race/ ethnic diversity; and (4) attitudes toward older clients are most strongly predicted by extent of training in aging. The authors offer suggestions for expanding age-related aspects into generalist training.
Introduction
The population is aging world-wide. In 2019, there were an estimated 703 million older adults globally, with the greatest numbers living in Eastern and South-Eastern Asia, Europe, and North America, respectively (United Nations, 2019). In the United States of America, recent estimates indicate there are approximately 56 million older adults, with this expected to rise to 73 million (20% of the population) by 2030 (Federal Interagency Forum on Aging-Related Statistics, 2020). These demographic changes will have profound effects on the services needed to support this population's physical and emotional health and well-being (see Carpenter et al., 2021).
A study exploring the prevalence of a wide range of mental health disorders in older adults across several European countries found that 25% of older adults currently had a mental health disorder, with 1 in 3 reporting a mental health diagnosis in the past year (Andreas et al., 2017). Older adults who do not have a clinical disorder may also benefit from mental health interventions, especially those experiencing physical health problems including chronic pain and disability - a common occurrence in older adulthood (Qualls & Benight, 2007). And, despite common misconception, older adults can and do benefit from mental health treatment (Cuijpers et al., 2014). Although the rate of mental health disorders and subclinical mental health difficulties will likely remain steady, the increase in the total population over 65 years of age will ultimately increase the total number of older adults in need of mental health services.
Psychology, unfortunately, is not prepared to meet the demand for practitioners to work with older adults (Institute of Medicine, 2012). Only 1 percent of psychologists in the U.S. specialize in aging (Moye et al., 2019), falling far short of the need. By 2030, the need for psychologists prepared to work with older adults is expected to increase to 5,940 full time equivalent (American Psychological Association, 2017). The shortage of mental health providers ready and willing to work with older adults is also present worldwide. Specifically, service-delivery gaps have been noted in Australia (Snowdon et al., 1995), New Zealand (Melding, 2005), Europe (Fernandez-Ballesteros et al., 2007), and China (Chiu & Chiu, 2005). Unfortunately, negative attitudes toward older adults are often found amongst mental health professionals (see Bodner et al., 2018 for review of literature) and have been connected with provider hesitance to work with this population (e.g., Caskie et al., 2022; Tomko & Munley, 2013). These may be particularly pronounced toward individuals 85 + (Kessler & Blachetta, 2020). The presence of biases toward older adults has also been linked to poorer health outcomes for older individuals (see Chang et al., 2020 for review), which makes this an issue of client care as well as a contributing factor to the workforce gap.
The projected workforce gap in psychology is believed to be attributable to factors such as the lack of inclusion of training opportunities at the graduate, intern, and post-doctoral level. Education and training in the care of older adults is important to enhance a sense of competence as well as to address negative attitudes (Levy & Macdonald, 2016; Lytle & Levy, 2019) and foster interest (Merz et al., 2017). Though there are unique challenges to working with older adult clients, particularly amongst young psychotherapists, supportive training and supervision may help to facilitate increased competence and comfort working with this population (Boschann et al., 2022). Educational interventions are often geared toward improving attitudes toward older adults, with positive clinical interactions seemingly the most influential (see systematic reviews by Chonody, 2015; Ross et al., 2018). Unfortunately, training opportunities seem to be quite limited across different countries (i.e., USA, Canada, Australia; (Pachana et al., 2010). Of note, clinical placements seem to represent the most common method of incorporating aging whereas a lack of encouragement from faculty mentors acts as a barrier to experience working with older adults (Pachana et al., 2010). Training opportunities can be guided by efforts generated within psychology (Hoge et al., 2015), such as the delineation of attitudes, knowledge, and skill competencies for the entry-level geropsychologist, entitled the Pikes Peak Model for Training in Professional Geropsychology (Knight et al., 2009), as well as foundational competencies for all psychologists working with older adults (Hinrichsen et al., 2018).
The American Psychological Association (APA) requires that graduate, internship, and fellowship programmes address issues of cultural and individual diversity, defined as “age, disability, ethnicity, gender, gender identity, language, national origin, race, religion, culture, sexual orientation, and socioeconomic status” (APA, 2015). However, there is concern that most programmes leave age out of diversity education and training (Yeo et al., 2017). Beyond a deficit in training, the lack of attention given to aging topics may also send the message that it is not important, thus breeding a social norm of ignoring or avoiding this population. Social norms have been found to be predictive of student intention to work with older adults (Graham & Rosén, 2020; Graham & King, 2022) and thus may be an additional piece of the service-gap puzzle.
In this context, the goal of the present study is to understand age-related training within a sample of psychology doctoral students. Specifically, this paper reports on (1) the reported extent of training in aging according to the student sample and a review of programme training materials; (2) doctoral students’ ratings of their knowledge in aging and its association with training opportunities; (3) how training in aging compares to training in race/ ethnicity; and (4) doctoral student attitudes toward older clients and its association with training opportunities and knowledge. In the discussion section, we return to explore the implications of education and training at the doctoral level in the context of the psychology workforce.
Method
Procedure
To recruit participants, the first author sent an email to the Counseling Psychology trainee (APA Division 17, Student Affiliates of Seventeen) and Directors of Clinical Training listservs (Council of Counseling Psychology Training Programs, Council of University Directors of Clinical Psychology). The recruitment email briefly described the study as relating to training and competency, contained IRB information, and the survey link with informed consent. Of note, this data was collected as part of a larger thesis study conducted in 2015. Additional data about the inclusion of age in counselling psychology Ph.D. programme training materials was gathered in 2022.
Measures
Demographic Information
Participants provided information about their age, race/ethnicity, type of doctoral programme (counselling or clinical; PhD or PsyD), and years of clinical experience.
Training in Aging and Race/Ethnicity
Training in aging and in race/ethnicity during graduate school was assessed via an adapted version of Tomko and Munley's (2013) Training and Experience Questionnaire (TEQ), which contained three items rating the extent of predoctoral training related to aging and three items rating the extent of predoctoral training related to racial/ethnic diversity. Items were rated on a seven-point Likert-scale (1 = none, 7 = very extensive) and summed to create a total score for training in aging and a total score for training in racial/ethnic diversity. Reliability in the current study sample for the aging scale (α = .83) and the racial/ethnic scale (α = .85) was acceptable (Nunnally, 1978). An additional item assessed the extent that diversity courses during graduate school included aging topics on a 7-point Likert scale (1 = None to 7 = Very Extensive). Participants were also asked to indicate which aging topics were covered in their programme coursework and in which clinical settings they gained clinical experience working with older adults.
Self-Rated Knowledge in Aging
Participants were asked to provide a self-assessment of aging-related knowledge competencies using the Pikes Peak Geropsychology Knowledge and Skill Assessment Tool, version 1.4 (Karel et al., 2010). Given that the participants were doctoral students, they received only the knowledge domain of the Pikes Peak tool: General Knowledge about Adult Development, Aging, and the Older Adult Population. This larger domain consists of four subdomains (Models of Aging, Demographics, Normal Aging, and Diversity in Aging). Items within each subdomain were rated on a five-point Likert-scale from 1 = Novice to 5 = Expert (see Table 1). This measurement also allowed for a rating of “0 = N/A.” A total score for each subscale score was calculated by averaging, with this standardization allowing for comparison across sub-domains. A total, full scale, score was derived by averaging all items. Reliability for subdomain scales was as follows: Models of Aging (α = .87), Demographics (α = .85), Normal Aging subscale (α = .96), and Diversity in Aging (α = .88), and for total score General Knowledge scale (α = .96). These reliability coefficients are all considered to be acceptable (Nunnally, 1978).
Knowledge Ratings in Aging Content Areas on the Pikes Peak Assessment Tool.
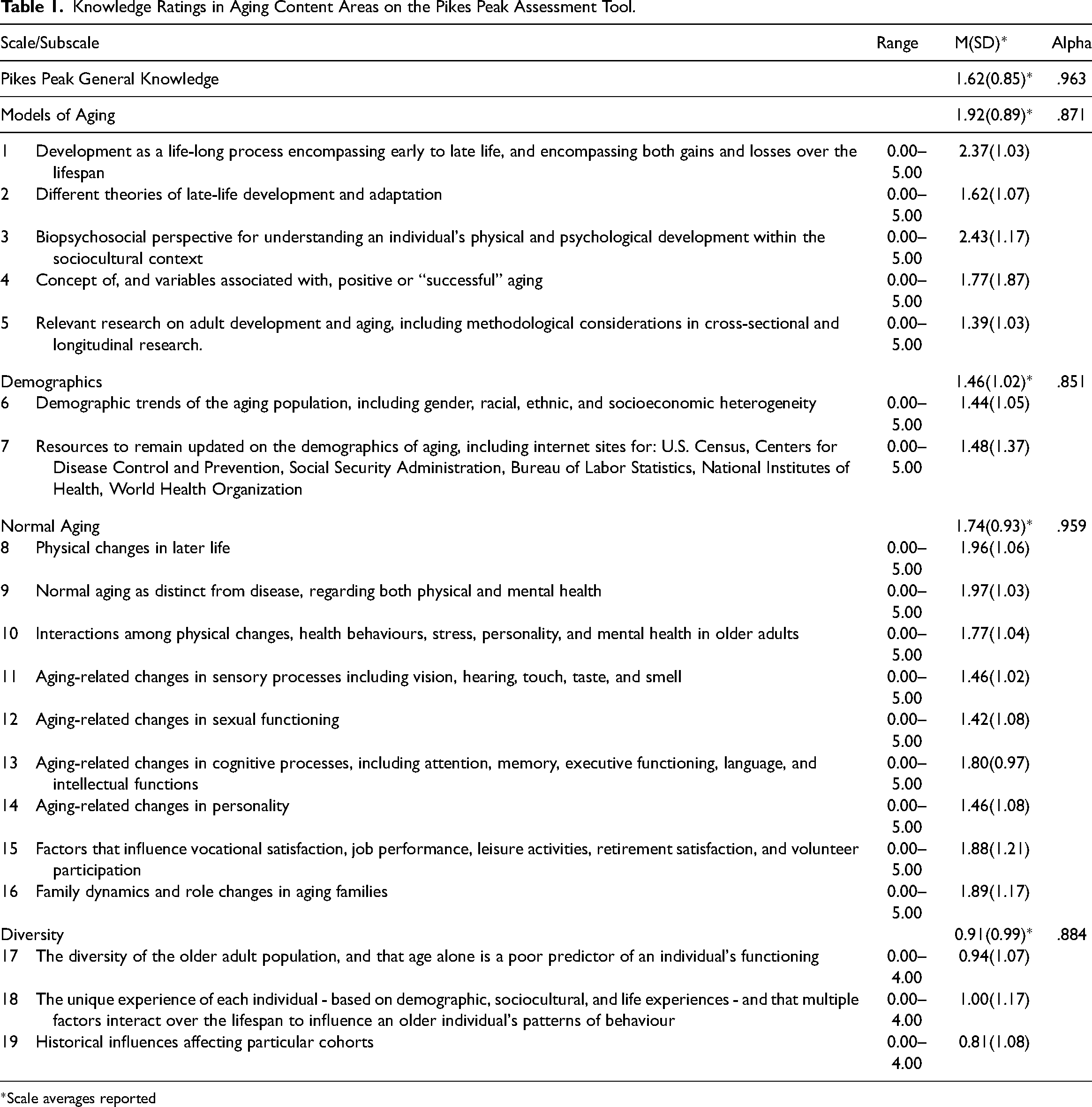
*Scale averages reported
Attitudes Toward Older Clients
Attitudes toward older clients were assessed via an adapted version of a scale by Happell and Taylor's (2001), originally developed to assess nurses’ perceptions of clients with drug and alcohol problems by substituting language referring to older clients. The scale was adapted to contain 15 items. Example items include: “I consider working with older adults to be fulfilling”, “I feel comfortable working with older adults”, and “I believe therapy is an effective means of treatment for older adults.” Items were rated on a six -point Likert-scale (1 = strongly disagree, 6 = strongly agree). A total score was created by summing item scores, with a higher score indicating more positive attitudes. Reliability in the current study (α = .91) was acceptable (Nunnally, 1978).
Programme Review
Additional data was collected in March of 2022 to supplement the survey data described above. Since the large majority of participants were from Counseling Psychology Ph.D. programmes (87%), a list of APA accredited Counseling Psychology Ph.D. programmes was acquired using the APA search tool (https://accreditation.apa.org/accredited-programs). Combined programmes (e.g., Counseling-School, Counseling-Clinical) were not included on this list. All of the APA accredited Counseling Psychology Ph.D. programmes listed are located in the United States of America.
Websites for each programme were searched using key terms “handbook,” “program,” or “manual.” If the key terms yielded no results, a visual/manual search was instituted to find the programme handbook. If a handbook was accessible, a search using the key terms “aging,” “age,” “adult,” “older adult,” and “diversity” was conducted. The number of mentions for each key term was recorded as well as additional information about the context in which it was mentioned. If faculty interests or specialties were included in the handbook, these were also included in the search for key terms and calculated in the final evaluation of the results.
Data Analysis
Frequencies and averages were used to describe levels of training, attitudes, and self-perceived knowledge. Comparisons were made across knowledge and training areas, with paired t-tests used to assess for significant differences between subscale means. A multiple linear regression was conducted to explore the association of participant age, self-reported knowledge in aging, and training in aging on attitudes toward older clients. Given the multiple bivariate analyses, a significance value of p < .01 was adopted to reduce experiment-wise error. Missing data existed on an item level and were not imputed. Missing data was less than 10% across variables, ranging from 3.4% to 9.4%.
Results
Sample
The 85 participants ranged in age from 24 to 66 with an average age of 29 years old (M = 28.67; SD = 6.05). The majority (71%) of the sample was female (n = 61), with the remainder of the sample identifying as male. The majority (69%) of the participants identified as Caucasian (n = 59), with the remaining participants identifying as belonging to a minority group (i.e., Hispanic, Black/African American, Asian, Pacific Islander). The sample of trainees consisted of current doctoral students, with the majority (87%) currently enrolled in a Counseling Ph.D. programme (n = 74). The remaining participants were from Clinical Ph.D. (n = 3), Clinical Psy.D. (n = 6), Counseling Ed.D (n = 1), and Combined (n = 1) programmes. Participant years of clinical training ranged from one to over five years, with the majority (84%) reporting between one and four years (n = 71). Based on a large report on student demographics in 500 + graduate programmes conducted at the same time as this study (Cope et al., 2016), the participants in the present study had similar demographics to the broader population of graduate students in terms of being predominantly female (72.1%) and Caucasion/White (72.4%). Although geographic location was not explicitly reported, exploration of latitude and longitude indicated that all participants were in the United States at the time the survey was completed. Locations were diverse and included Washington, California, Colorado, New Mexico, Kansas, Nebraska, Texas, Illinois, Ohios, Florida, Georgia, Virginia, New Jersey, Pennsylvania, Massachusetts, and New York.
Training in Aging
Participant ratings on the total training in aging scale (TEQ-A) ranged from 3 to 16 (M = 7.70, SD = 3.74). Participants ratings of three items on the training in aging scale averaged between 2 and 3 on a 7 point scale in the areas of coursework (M = 2.74, SD = 1.43), training in counselling/psychotherapy with older adults (M = 2.58, SD = 1.47), and training in intakes/diagnostics with older adults (M = 2.39, SD = 1.44). Levels of training reported in these three areas were not statistically different from one another in paired t-tests (e.g., coursework vs. counselling/psychotherapy; coursework vs. intakes/diagnostics; counselling/psychotherapy vs. intakes/diagnostics).
Regarding aging topics covered, the majority (64%) of participants reported learning about the developmental stages of aging whereas a smaller percentage (33%) reported learning about the neuropsychology of aging. Most participants (80%) indicated that they did not receive any training on clinical skills with older adults and a quarter of the trainees (25%) reported that no topics related to older adults had been covered in their programmes.
Comparing Training in Aging with Race/Ethnicity
Participant ratings on the total training in race/ethnicity scale (TEQ-D; M = 15.28, SD = 3.65) was significantly greater than training in aging (M = 7.70, SD = 3.74; t(77) = 15.25, p < .001). Similarly, participant ratings on each of the three training in race and diversity items were significantly greater than training in aging for coursework (t(79) = 14.04, p < .001), counselling/psychotherapy (t(79) = 12.81, p < .001), and intakes/diagnostics (t(79) = 12.25, p < .001). See Figure 1. Participant ratings of the extent of aging topics covered within their diversity training averaged a 3 on a 7-point scale, with no ratings at 6 or 7 level (Range 1–5, M = 2.78, SD = 1.17). Further, about half of the participants (48%) said that their diversity training did not include older adults at all.
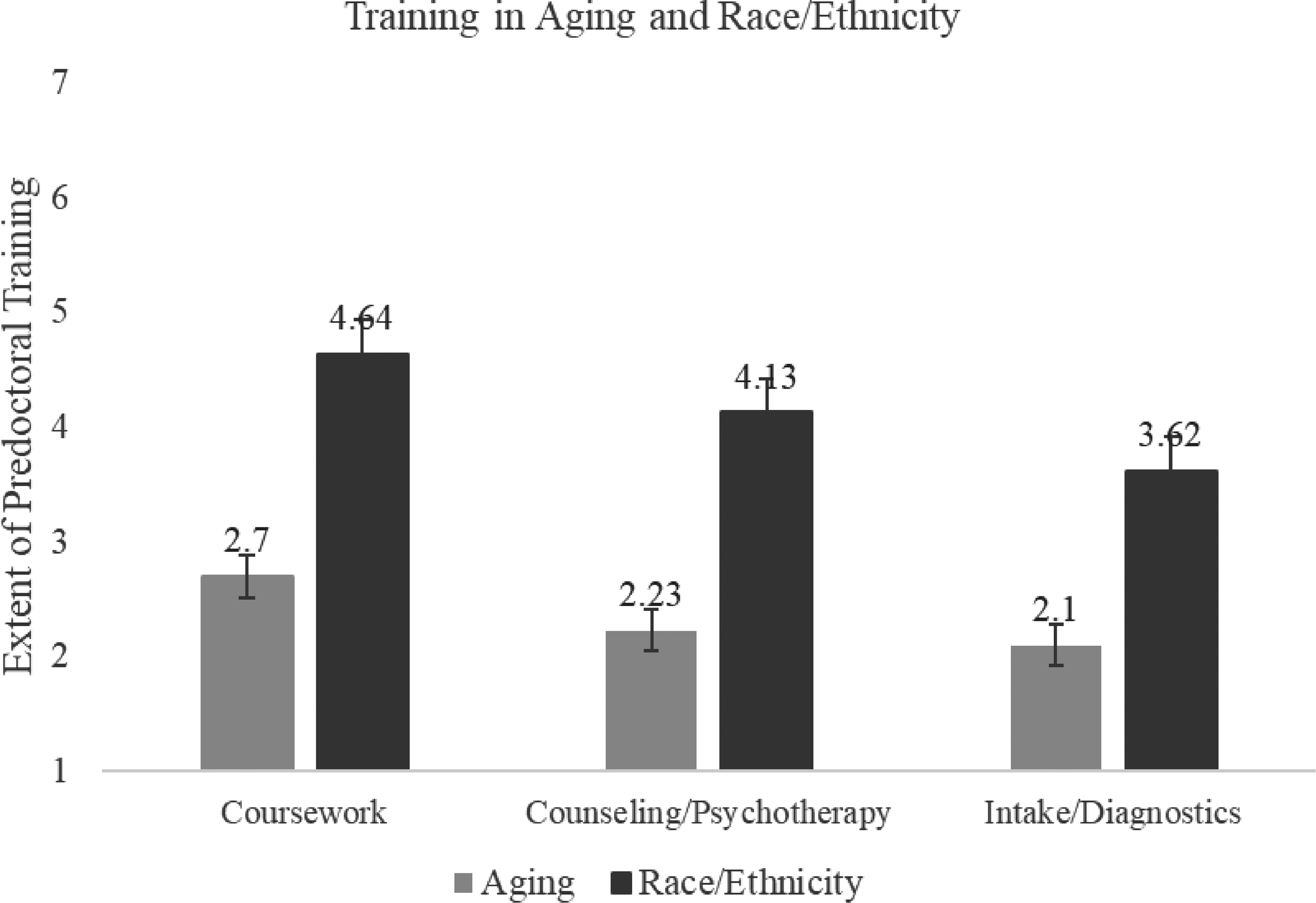
Training in aging and race/ethnicity. Note. Rated on a Likert scale from 1 = None to 7 = Very Extensive.
Self-Rated Knowledge in Aging
Participant ratings of General Knowledge in aging (Pikes Peak total score) fell between the Novice and Intermediate designations (M = 1.91, SD = 0.89). Subdomain mean scores were highest in Models of Aging (M = 1.92, SD = 0.89), followed by Normal Aging (M = 1.74, SD = 0.93), and Demographics (M = 1.46, SD = 1.02). Self-rated knowledge of Demographics was significantly lower than Models of Aging (t(77) = 5.66, p < .001) and Normal Aging (t(77) = −3.64, p < .001). The mean score for Diversity in Aging was the lowest of the four subscales (M = 0.91, SD = 0.99) and was significantly lower than Models of Aging (t(76) = 10.41, p < .001), Normal Aging (t(76) = 8.87, p < .001), and Demographics (t(76) = 4.84, p < .001). See Figure 2.
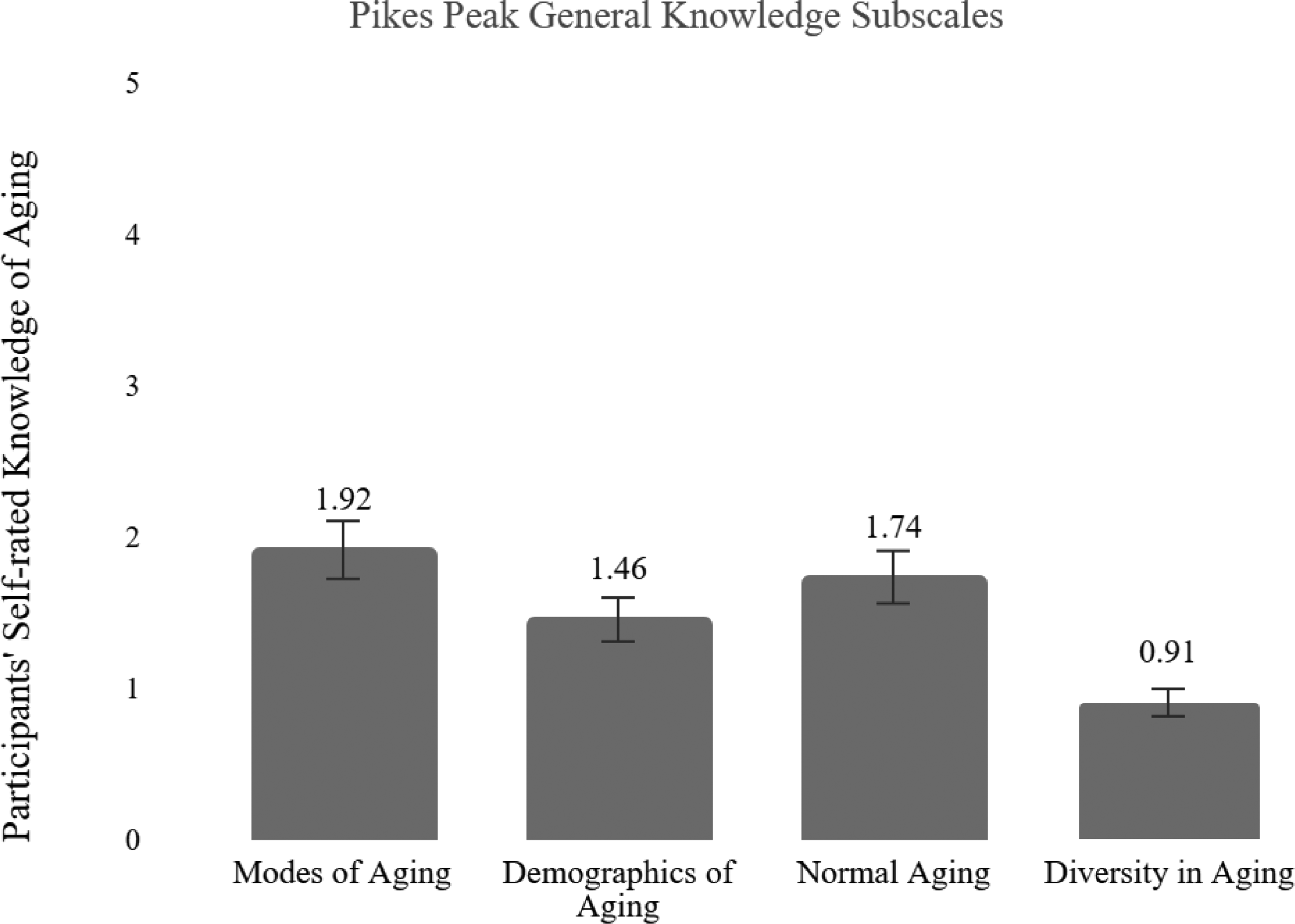
Participants’ self-rated knowledge of aging (pikes peak general knowledge). Note. Rated according to the following scale: 1 = Novice; 2 = Intermediate; 3 = Advanced; 4 = Proficient; 5 = Expert; 0 = N/A.
Attitudes Toward Older Clients
Participant ratings of attitudes toward older clients were skewed positive, with an average of 66.91 (SD = 9.8) out of a maximum scale score of 105. A non-statistical assessment of item means indicated that participants endorsed the most positive ratings on items related to clinical care for older adults and the least positive ratings on items related to perceived competency working with older adults. For example, the following two items had the highest average ratings: 1) “I deliver the same standard of care to older adult clients as I would to any other client” (M = 4.85, SD = .99), and 2) “I believe therapy is an effective means of treatment for older adults” (M = 5.18, SD = .63). Whereas, the following two items had the lowest average ratings: 1) “I do not believe I have the professional training required to work successfully with older adult clients” (M = 3.88, SD = 1.08; reverse coded); and 2) “I feel I know enough about aging and geropsychology to provide adequate therapy to older adult clients” (M = 3.68, SD = 1.09). Positive attitudes toward older adult clients was positively related to participant age (r(82) = .43, p < .001), but not participant gender or ethnicity. Additional correlations, means, and standard deviations are provided in Table 2. In a multiple regression analysis (F(3, 73) = 17.78, p < .001; R2 = .422), training and education in aging was a significant predictor of attitudes toward older clients (β = .34, p = .001), such that more training predicted more positive attitudes. Participant age (β = .26, p = .012) and self-reported General Knowledge (β = .25, p = .023) were not significantly associated with attitudes at the p < .01 cut off.
Correlations Amongst Knowledge, Experience, Attitudes, and Participant Age.
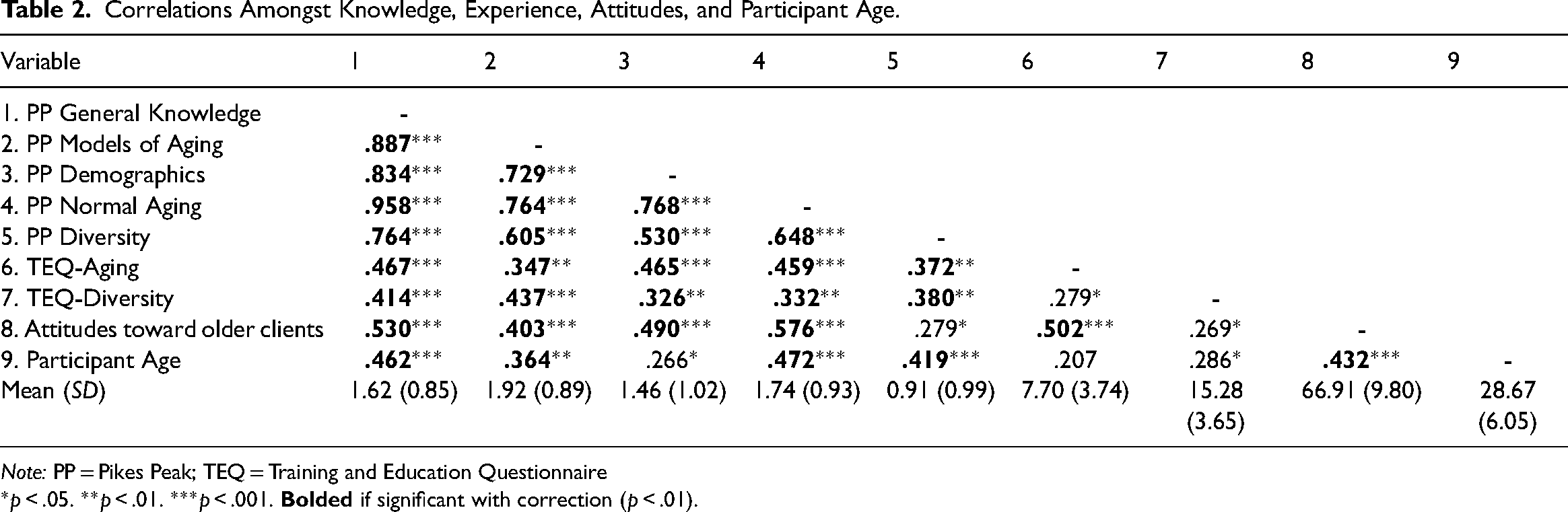
Note: PP = Pikes Peak; TEQ = Training and Education Questionnaire
*p < .05. **p < .01. ***p < .001.
Programme Review
There are a total of 63 APA accredited Counseling Psychology Ph.D. programmes, all located within the USA. Of these 63 programmes, 31 (49.2%) had accessible programme handbooks and 12 additional programmes (19%) contained aging-related keywords on their programme websites. Therefore a total of 43 of the 63 programmes (68%) included some reference to aging in either their programme materials or website. Twenty-six programmes (60.4%) included the term “age,” with 25 of those (96%) instances unrelated to training and merely including statements on discrimination and social justice. The keyword “Adult” was found in 29 (67.4%) of programme materials. These mentions included required courses on assessments of adults as well as statements on diversity unrelated to training and/or APA codes and guidelines included in the handbook. The keyword “Older Adult” was found in 14 (32.6%) handbooks, with 12 of those mentions coming from citations of APA guidelines. Seven programmes (16.3%) made mention of “aging,” two of which stated that additional training in aging and older adults is required upon completion of the programme whereas three of these programmes included required courses in the curriculum if previous lifespan classes had not been taken. The keyword “diversity” was found in 23 (36%) handbooks.
Discussion
In order to address the growing workforce crisis in aging, there is an urgent need to enhance the competencies of all psychologists for working with older adults. Further, aging-related knowledge may benefit the care of younger and middle aged clients through supporting “successful” aging and long-term development. The main findings of this paper are four-fold: (1) Training in aging varies and is inadequate in some programmes; (2) Knowledge in aging varies and is associated with training opportunities; (3) Training in aging is less than training in racial/ ethnic diversity; (4) attitudes toward older clients are most strongly predicted by extent of training in aging.
Participant ratings of aging-related training in coursework, psychotherapy, and diagnostics were modest and consistent across domains. This finding was supported by the programme content review of APA-accredited Counseling Psychology Ph.D. programmes and seems to be consistent with previous reports of a lack of aging-related education and training in programmes in the USA, Canada, and Australia (Pachana et al., 2010). The most reported area of coursework in which aging was included was within the context of human development. Unfortunately, the more clinically relevant areas such as neuropsychology and counselling skills related to aging were infrequently covered. This is concerning given the need to increase the clinical workforce to support a rapidly growing older population. Even more concerning is that one-quarter of the participants reported receiving no didactic education related to aging at all and the majority (80%) reported receiving no clinical training. Although a review of programme training materials found that aging was at least mentioned in the majority of programmes (68%), a review of the context revealed that only five programmes (11.6%) explicitly referenced clinical work and training with older adults. The growing population of older adults increases the likelihood that psychologists from all training backgrounds and across clinical settings will encounter older adults, making this an important aspect of generalist training.
Participant ratings of competency in General Knowledge of aging fell between the Novice and Intermediate designations, which was expected given their level of training. Of note, the knowledge ratings varied across subdomains. Specifically, knowledge on Models of Aging was rated the highest and most participants reported that developmental models were covered in their doctoral coursework. The significant relationship between level of training in aging and self-rated knowledge suggests some programmes are quite successful in offering training related to older adults and that this training is associated with greater knowledge. A deficit in knowledge related to aging and working with older adult clients could impact a psychologist's ability to successfully treat this population. For instance, treatment goals may vary according to age with older clients prioritizing functioning and well-being over personal growth goals often espoused by younger clients (Sittler et al., 2021). This knowledge applied in a clinical setting could support individualized treatment planning and care for older adult clients.
Following this line of reasoning does raise concerns, however, about the domains that are not being reliably covered across programmes. Specifically, diversity within aging was identified as least consistently and adequately covered knowledge area in the current sample. Students reported more training in diversity as defined by race/ethnicity than in diversity as defined by age, even though both factors are a component of diversity as defined by the APA. The emphasis on infusing diversity-related topics into training has been significant and in line with APA's values (APA, 2015). The current findings validate this effort, with students reporting significant training in diversity related to race and ethnicity. Unfortunately, age was not receiving adequate attention within the domain of diversity within the present sample. This is sadly in line with other research (Yeo et al., 2017) and may indicate a lack of intersectionality within diversity training. Intersectionality, the recognition that an individual's identities are interactive and cannot be addressed as separate from one another (see Crenshaw, 1989) has been identified as an important area of focus in clinical training (Rosenthal, 2016). This is not to say one identity factor is more or less important but rather that all are important and worthy of inclusion in training curricula.
Within the present study, attitudes toward older adults were skewed more positive on average. However, an item review revealed some variability such that students endorsed higher ratings on items toward clinical care and lower ratings on items related to their own competence levels. Given the consistent finding that ageism is present within healthcare settings (see São José et al., 2019) and the negative impact biases can have on healthcare (see Chang et al., 2020 for review), these differences may be an area of further explanation. Further, attitudes were positively associated with training and knowledge such that trainees who reported receiving more training and having more knowledge about older adults also reported more positive attitudes toward older adults. This finding is consistent with other research indicating that when exposure to older adults is offered positive attitudes tend to increase (Levy & Macdonald, 2016). It should be noted that the directionality of this relationship likely runs both ways, such that trainees with more positive attitudes toward older adults may be more likely to seek out aging-related training and experiences. Taken together, this supports the notion that increasing training can not only increase competence but can also combat ageist attitudes, potentially reducing the harmful differential treatment within healthcare settings.
Limitations and Future Directions
Although this study provides useful information and a platform for further inquiry, there were several limitations that should be noted. As previously described the data were taken from a thesis project and is a bit older (2015). It would be interesting to continue to explore the state of aging training over time to assess the potential impact of efforts to include aging as a diversity factor. The data was also cross-sectional and therefore conclusions cannot be drawn about causality. It would be useful to collect longitudinal and/or experimental data to further explore this area of study. The sample was also small and primarily of psychology students in Counseling Ph.D. Programs. Future research should seek to include a larger sample that includes more representation across programmes (e.g., Clinical/Counseling Psychology, PhD/PsyD) and countries.
Conclusion and Recommendations
Within the context of an ever-growing service gap, these findings can serve as a wake-up call to the need for further emphasis on incorporating aging-related training into graduate training. They may also serve to offer suggestions on potential areas where programmes should put their emphasis. Specifically, for those programmes that do not offer any aging-related training it will be important to adjust as soon as possible to best prepare students for careers in which they will likely interact with a growing aging population in various settings. Failure to include age related training may have consequences beyond knowledge/skill deficit such that a lack of acknowledgment altogether could send the message that age is not an important identity factor. Programmes that currently offer basic training related to aging (e.g., models of aging, neuroscience of aging) may want to focus on intersectionality of aging and other diversity factors. All programmes would likely benefit from including clinical skills training to best lay groundwork for the growing likelihood that trainees will encounter older adults in future clinical work. Relevant skills could be included within the context of general clinical skills training related to therapy and assessments.
Interested programmes can find helpful resources through APA's Division 20 and 12:2, GeroCentral (https://gerocentral.org/), the Council of Professional Geropsychology Training Programs (CoPGTP; http://copgtp.org/). Additionally, Zucchero et al. (2014) offer several nontraditional pedagogical suggestions for including geropsychology education and training at the undergraduate, masters, and doctoral level.
Footnotes
Acknowledgments
Portions of this paper were derived from the first author's dissertation submitted to Colorado State University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article