
Abstract
Zahavi's handicap principle suggests that only organisms with good genetic quality can afford to engage in costly behaviors. Recreational drug use can be harmful to one's health and therefore might be viewed as a costly signal of one's genetic quality. One of the measurements of genetic quality is bodily symmetry assessed by fluctuating asymmetry. If unhealthy drug use is a behavioral example of Zahavi's handicap principle, then men who use different stimulants or recreational drugs should be more symmetrical than men who do not use them at all or use them only in low quantity. The aim of this study was to examine the relationships between drug use and fluctuating asymmetry. The subjects were 190 young women and 202 young men. Six bilaterally symmetrical traits were measured: length of II–V digits, wrist breadth, and ear height. Questionnaires included questions about smoking, alcohol drinking, drug use, and designer drug use. There was no relationship between bodily symmetry and smoking frequency, alcohol drinking frequency, drug or designer drug use, total substance use, age of smoking initiation, or reason of this initiation. The results indicate that drug use does not reflect genetic quality and does not necessarily relate to the handicap hypothesis.
Introduction
The most common addictions in western countries are related to smoking, alcohol drinking, and drugs (including marijuana) (Substance Abuse and Mental Health Services Administration, 2011; World Health Organization [WHO], 2004). All of these are unhealthy and might cause serious health problems and shorten the longevity of heavy users. Smoking increases the risk of death from cancers, heart disease, stroke, or chronic respiratory disease (WHO, 2009). Even low nicotine intake is risky. Smoking 1–4 cigarettes per day correlates positively with the risk of death from ischaemic heart disease (Bjartveit and Tverdal, 2005); also, even occasional smokers have a higher risk of developing smoking-related cancers (Bjerregaard et al., 2006). Alcohol causes oesophageal cancer, liver disease, epilepsy, and motor vehicle accidents (WHO, 2002). Using cannabis causes an epithelial injury of the trachea and major bronchi and increases the risk of chronic bronchitis, acute bronchitis, and possibly schizophrenia (WHO, 1997). New psychoactive substances—so-called designer drugs—may also pose serious public health problem, and they are difficult to monitor (European Monitoring Centre for Drugs and Drug Addiction [EMCDDA], 2009).
People use recreational drugs for a variety of reasons (Boys et al., 2001; Labouvie and Bates, 2002; Meyer et al., 2002), but since all drugs pose some health risk, it can be supposed that those who decide to use are more prone to take risks.
For young people (particularly boys or young men), drug use is often related to showing off and making an impression on others (Abolfotouh et al., 1998; Al-Naggar, Al-Dubai, Al-Naggar, Chen, and Al-Jashamy, 2011; EMCDDA, 2000; Hall and Nelson, 1995; Husseini, 2010; Percy, Wilson, McCartan, and McCrystal, 2011). The problem is that any drug may produce unpleasant side effects. However, the intensity of such effects may differ between individuals, and it is therefore likely that some people can more easily bear these side effects or can otherwise afford to engage in such risky behavior. According to the handicap principle (HP) of Zahavi (1975), the ability to risk one's health in this way can be classified as a handicap that might impress peers or potential mates. It has already been postulated that drug use might be related to sexual selection. It has been shown, for instance, that smoking by 13–15 years boys (but not girls) might increase their attractiveness (The Global Youth Tobacco Survey Collaborative Group, 2002). Smoking also lowers voice pitch, and studies show that lower voices are perceived as more attractive in men (Collins, 2000; Feinberg, Jones, Little, Burt, and Perrett, 2005) but not in women (Borkowska and Pawlowski, 2011; Collins and Missing, 2003). It is therefore possible that in the case of men, one might expect a trade-off between health-risking behavior and the potential increase of attractiveness. Might cigarette smoking or binge drinking have an advertising purpose? It has been proposed that by using these toxic substances, individuals show that they are genetically well equipped to be able to overcome the harmful effects of drugs (Diamond, 1996). However, if such sexual selection still takes place, regular smoking or drinking should be an honest signal of biological quality. It is possible that those individuals who use drugs can better cope with metabolizing different stimulants and/or have less painful discomfort in the case of overdosing. As it is postulated in the HP, only those individuals who have good genetic quality can afford either the costly morphological structures (Zahavi and Zahavi, 1999), high level of immunosuppressive sex steroid hormones that influence sexual dimorphic traits (Folstad and Karter, 1992), or risky behavior. It is then possible that those people who use recreational drugs can biologically afford such health risks; in other words, they have a better biological condition (or better genetic quality) on average.
The widely accepted and often used method of measuring biological condition is measuring bodily fluctuating asymmetry (FA) (Tomkins and Kotiaho, 2001, but see Van Dongen and Gangestad, 2011). FA is a random deviation from the ideal bilateral symmetry. It is supposed that despite possible factors affecting development and growth, organisms with good genes are able to secure enough energy that can be spent on body symmetry (Møller and Swaddle, 1997). This means that more symmetrical individuals (with lower FA) might have better genetic quality. This presumption has been confirmed in the morbidity of men (e.g., mentally disabled men have higher FA) (see Kowner, 2001) or by the frequency of male health problems (men with higher FA get ill more frequently than men with lower FA) (Waynforth, 1998). A meta-analysis of the relationship between FA and health and genetic quality (Van Dongen and Gangestad, 2011) has confirmed a robust association, although it has also demonstrated unexplained large variation across studies and overestimations of the strength of association, which is driven by publication bias.
Apart from drug use, there are other behaviors that are related to health risk, such as tattooing and piercing. A considerable percentage of people who have had body scarification have suffered health complications as a result: bacterial and viral infections, allergic reactions, and transmission of blood borne diseases (see Huxley and Grogan, 2005). In this case, Koziel, Kretschmer, and Pawlowski (2010) showed that in comparison to the control group, men who had tattoos or non conventional piercings were more symmetrical (had lower FA).
To our knowledge, drug use in the context of biological quality—assessed as developmental stability measured by FA—has not been studied in the context of the handicap principle.
Materials and Methods
Participants
The subjects were Polish students of the University of Wrocław and students of the Wrocław University of Technology, comprising 190 women aged 19.3–27.6 years (M = 22.56, SD = 1.63) and 202 men aged 18.8–29.1 years (M = 22.44, SD = 1.97). Our subjects were from the same ethnic group, had the same education, and were similar in age.
Fluctuating asymmetry measurements
Six bilaterally symmetrical traits were measured: length of II – V digits (from the tip of the finger to the ventral proximal crease), wrist breadth, and ear height (from the anterior to the posterior tip of the pinna). This combination of traits has been used in previous studies of (Martin, Manning, and Dowrick, 1999; Manning, Gage, Diver, Scutt, and Fraser, 2002).
Measures were taken using digital calipers of 0.01 mm accuracy and recorded onto a dictaphone. Each trait was measured three times and averaged. The reliability of the measurements was calculated using intra-class correlation coefficient (ICC) (Müller and Büttner, 1994, as cited in Kornhuber et al., 2011); their values ranged from 0.963 to 0.996 (left side – II digit: 0.993, III: 0.996, IV: 0.994, V: 0.991, wrist: 0.992, ear: 0.964, right side – II digit: 0.991, III: 0.995, IV: 0.994, V: 0.992, wrist: 0.991, ear: 0.963).
In order to check for directional asymmetry (DA), for each trait we calculated the difference between the right and left (Palmer and Strobeck, 1992) and then conducted one-sample t-tests with the mean set at zero. Three traits showed DA: III digit (left longer), IV digit (right longer) and the wrist (right wider) (see Table 1). Although according to Palmer and Strobeck (1992) directional asymmetry is genetically programmed and does not reflect developmental noise, Leamy (1999) suggested that directional asymmetry can also be used as an indicator of developmental stability. Lalumière, Harris, and Rice (1999) made use of two versions of FA indices—the first one with all measured traits and the second one without the traits showing DA—and they obtained comparable results.
Results of one-sample t-tests for the difference between the right and left side of each trait
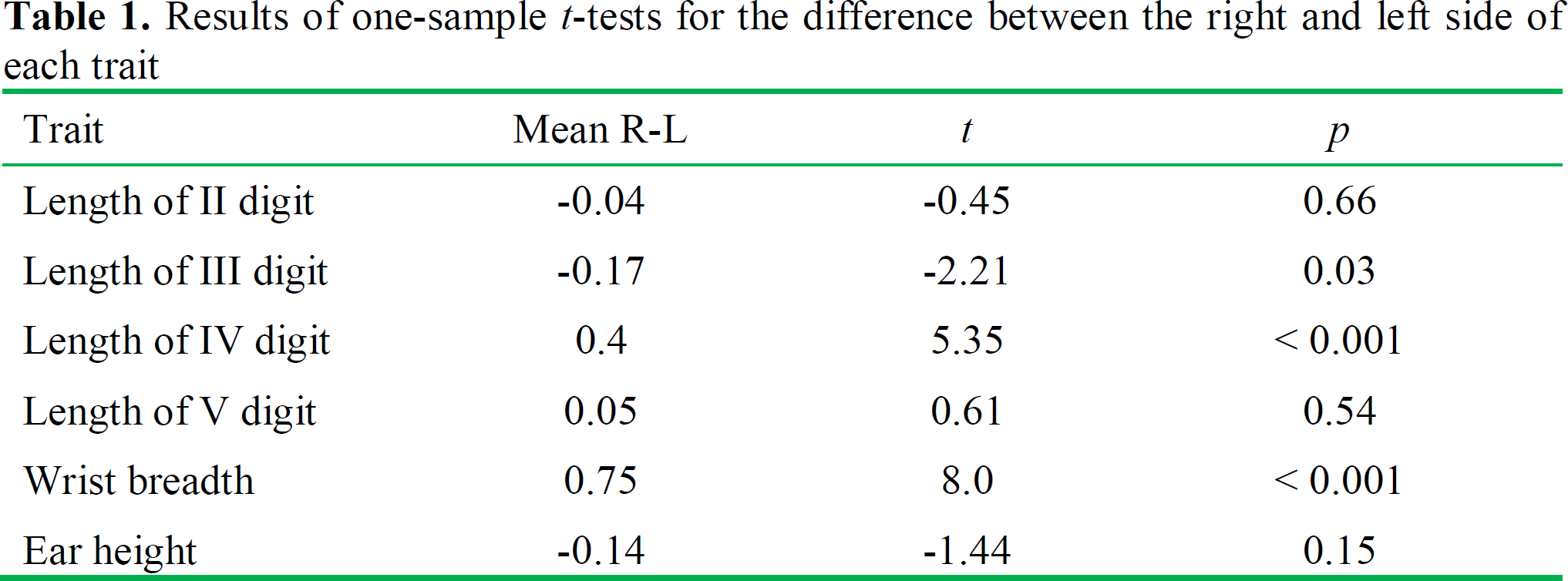
For each trait, the distribution of signed asymmetry was tested for skewness and kurtosis (Palmer and Strobeck 1992). No value departed from normality (skewness: range from -0.16 to 0.41; kurtosis: range from 0.06 to 0.7) (Kim, 2013).
We calculated the absolute value of each difference between the right and left side and divided it by the mean size of a given trait; relative asymmetry obtained in this way was also multiplied by 100:

Since the combined FA of several traits is a better indicator of developmental instability than the FA of a single trait (Dufour and Weatherhead, 1996; Gangestad and Thornhill, 1999), we calculated the arithmetic mean of relative FA for all the traits. In this way we obtained a total fluctuating asymmetry (tFA) for each person. In a similar way to Lalumiere et al. (1999), we used two versions of tFA: the first one included all six traits, and the second one excluded the traits that showed directional asymmetry. The results did not differ between these measures, so we present only the results obtained for the second type of tFA (without directionally asymmetrical traits). In some cases we obtained measures of five bilateral traits instead of six. This was the case for 19 women and 30 men who either declared injuries, had deformed ears by piercing, or the proximal crease of a digit was reduced. Similar methods have been used by Milne et al. (2003).
Intra-class correlation coefficients for FA amounted to the following: II digit: 0.87; III digit: 0.75; IV digit: 0.87; V digit: 0.88; wrist: 0.90; ear: 0.72; first version of tFA: 0.86; second version of tFA: 0.83.
Questionnaires
Questionnaires included questions about birth date, height and weight, smoking, alcohol drinking frequency, and use of other drugs (e.g., cannabis, amphetamine, or designer drugs). Current and former regular smokers were asked about age and reason of smoking initiation, and current regular smokers also declared the number of cigarettes smoked per day.
Self-reported data on height and weight were included in order to control for BMI, which may correlate with FA, at least in females (Milne et al., 2003). There is good evidence that younger adults report their height and weight accurately (e.g., Großschädl, Haditsch, and Stronegger, 2012; Kuczmarski, Kuczmarski, and Najjar, 2001). Participants were given the opportunity to weigh themselves on a digital scale if they did not know their own weight. We used values with accuracy to 1 cm (height) and 1 kg (weight).
To analyze smoking, we divided participants into the groups non-smokers, occasional smokers, and regular smokers (see Table 2). Only participants who had never smoked were treated as non-smokers, former smokers (13 women, 23 men) were not compared with the other groups, but they were included in the analyses of age and reason of smoking initiation.
Descriptive statistics for tFA indices in the various groups of participants
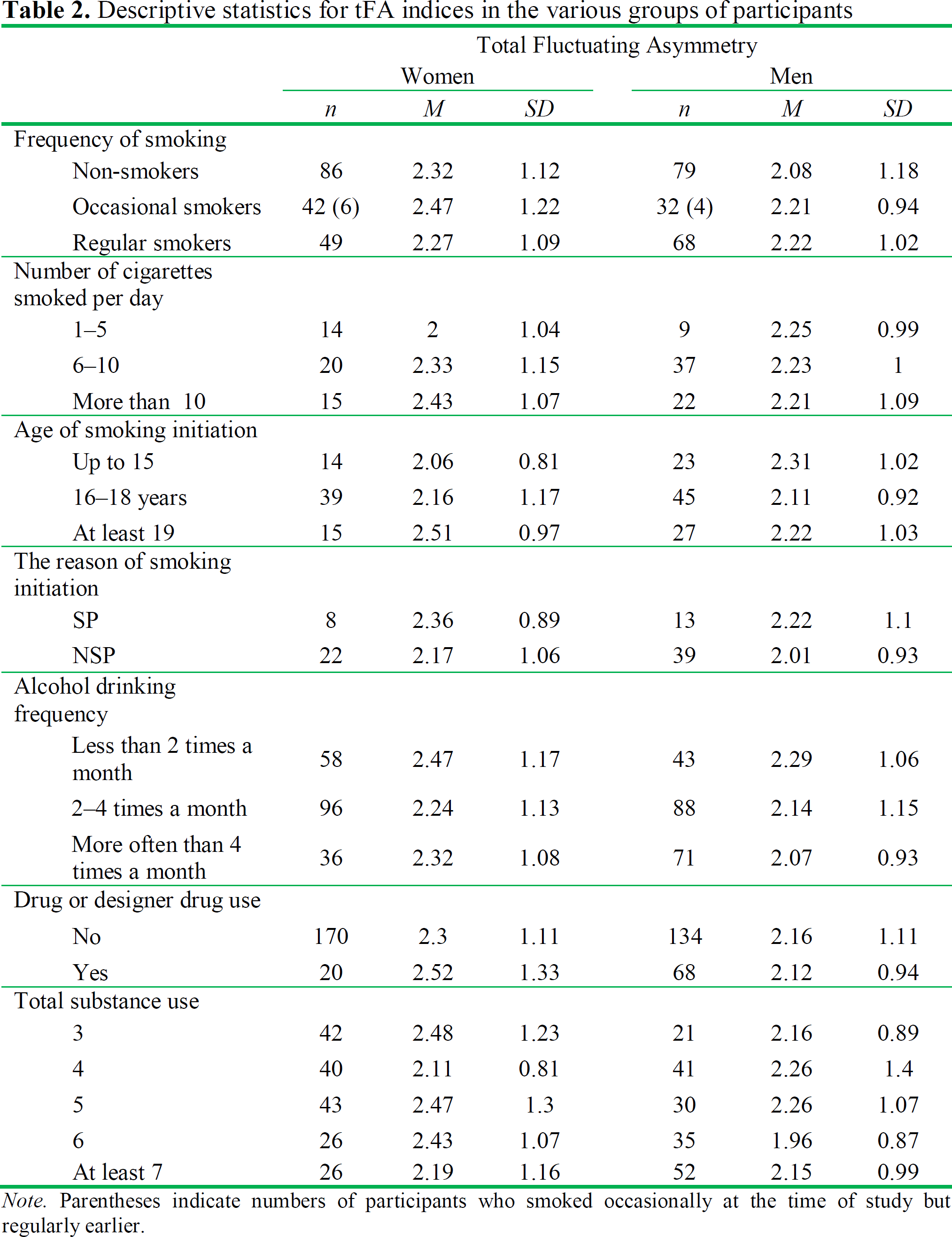
Note. Parentheses indicate numbers of participants who smoked occasionally at the time of study but regularly earlier.
The question about number of cigarettes smoked per day was open-ended, and we created three categories on the basis of the answers provided: 1–5, 6–10 and more than 10 cigarettes per day (a similar classification was used by Jones, Kann, and Pechacek [2011]) (see Table 2). Regarding the age of smoking initiation, we also created three categories (see Table 2) related to the likely peer context (secondary school, high school, and university).
Participants who smoked regularly and used to smoke in the past were also asked to indicate the main reason for smoking initiation (because of stress, to not stand out, and to show off in order to be perceived as an adult) or wrote their own answers. The responses to this question that suggested the influence of the other people were collected into the category under social pressure or stress (SP; n = 8 women, 13 men), whereas responses such as out of curiosity, for pleasure, or for fun were classified as non-related to social pressure (NSP; n = 22 women, 39 men) (see Table 2). Unfortunately, 38 women and 43 men either did not remember the specific reason for smoking initiation or it was difficult to distinguish between SP and NSP reasons. We assumed that susceptibility to interpersonal influence as an aspect of social conformity may not reflect high biological quality compared to someone's own decision-making about smoking. We also presumed that smoking because of stress is a sign of weakness rather than strength; therefore we connected this option together with interpersonal influence as a combined group of the factors unrelated with potential high biological quality.
Alcohol drinking frequency was studied using the same five categories as in Babor, Higging-Biddle, Saunders, and Monteiro (2001): never, monthly or less, 2-4 times a month, 2-3 times a week, and 4 or more times a week. Because of the small number of participants in the extreme groups, we combined the first two categories (not more than once a month), and we did the same with the two categories of the most frequent alcohol consumption (more often than 4 times a month). In this way we obtained 3 categories (see Table 2). Similarly, we distinguished three answers about drug or designer drug use: never, occasionally, and regularly, but since no woman declared regular intake, we compared only two categories: not taking and taking any drugs (see Table 2).
We also calculated the total amount of substance use. In order to obtain equal importance for each kind of substance (cigarettes, alcohol, and drug or designer drug), we divided every group into the three categories: cigarettes: non-smokers (1 point), occasional smokers (2 points), and regular smokers (3 points); alcohol: no more than one time a month (1 pt.), 2-4 times a month (2 pts.), and more often than 4 times a month (3 pts.); drug or designer drug: not taking (1 pt.), taking occasionally (2 pts.), and taking regularly (3 pts.). Scores were summed for each participant, and we obtained seven ranks from 3 to 9 points. Since no woman obtained 9 points and only four women scored 8 points, the last three categories were combined into one category: at least 7 points (see Table 2).
Statistical methods
Intra-class correlation coefficients were calculated using the two-way random effects mode (Müller and Büttner, 1994, as cited in Kornhuber et al., 2011), which was performed in SPSS Statistics 17.0.0. The other analyses were carried out in Statistica 9. Differences in tFA between groups and sexes were tested by two-way analysis of variance.
Results
BMI did not differ between all compared subgroups of recreational drug users (p > 0.07); therefore, we did not control for this factor in further analyses. We compared tFA indices in all categories of the studied addiction habits (i.e., smoking frequency, alcohol drinking frequency, drug or designer drug use, and total substance use) (see Table 2). We did not find any significant relationship, nor was there any significant interaction between tFA in these groups and sex (see Table 3). There was also no relationship between smoking initiation age or the cause of this initiation and FA (see Table 3). Men and women did not differ from each other in terms of tFA (women: M = 2.32, SD = 1.13; men: M = 2.15, SD = 1.05), F(1,390) = 2.55, p = 0.11.
Results of two-way ANOVA with sex and group as independent factors and recreational drug use as dependent variable

Discussion
Our results do not confirm that drug use can be a good indicator of biological quality measured by fluctuating asymmetry. This also means that we found no support for drug use as an example of Zahavi's (1975) handicap principle. We also did not find any significant relationship with the age of smoking initiation and the causes of this initiation. In this case, however, the results should be treated very cautiously, because many participants could not remember the circumstances and the causes of smoking initiation, and those who specified the cause of smoking initiation were very often not precise enough in this respect. Even when specified, given the time lag, such self-reported, subjective information should be also treated cautiously.
We should also take into account that fluctuating asymmetry is a result of two opposing influences: developmental noise and developmental stability (see Lens, Van Dongen, Kark, and Matthysen, 2002). Thus, FA in our study is not an ideal measure of genetic quality. An example of environmental stressors during prenatal development may be exposure to alcohol and nicotine. There is evidence that alcohol consumption by a pregnant woman increases the asymmetry of children's heads (Żądzińska, 2003), faces (Klingenberg et al., 2010), and dentition (Kieser, 1992), and tobacco smoking by a father also disturbs the head symmetry of a child (Żądzińska, 2003). Furthermore, alcohol use (Hayes, Smart, Toumbourou, and Sanson, 2004; Hung, Yen, and Wu, 2009) and smoking (Eaton, 2008; Gilman et al., 2009) are influenced by parental drinking and smoking habits. Hypothetically, subjects who use recreational drugs relatively often might have been exposed to alcohol and nicotine during intrauterine growth, and such a stressful environment would reduce their bodily symmetry. The fact that we did not control for parental drinking and smoking habits is a limitation of our study.
The other potential limitation of our study is related to the data on alcohol consumption. Our subjects responded to the question of how many occasions they consumed alcohol and did not indicate what amount of alcohol they consumed in each episode. Consuming small quantities of alcohol (particularly by older people) is not necessarily harmful to one's health (Abramson, Williams, and Krumholz, 2001; Rimm, Williams, Fosher, Criqui, and Stampfer, 1999). Although we do not have data regarding the quantity of alcohol consumed, considering the cultural habits of alcohol consumption by young people (mainly students) in the studied population, we may reasonably presume that drinking sessions (usually in the social contexts) mentioned by our subjects were related with at least moderate (if not heavy) alcohol consumption and, therefore, posed some health risk. Nevertheless, due to the lack of precise information about the amount of alcohol consumed, our results on alcohol drinking and FA should be treated cautiously. Since even occasional smoking and small amounts of drugs are harmful, there is no doubt that our results for smoking and drugs consumption are related to health-risk behavior.
The obtained results indicate that genes related to biological quality are not a better predictor of substance use than already well-known predicting factors, such as genes not directly related to biological condition (Kendler and Prescott, 1998; Madden, Bucholz, Martin, and Heath, 2000) and environmental or psychological factors: e.g., life stress (Castro, 2004; Enoch, 2011) and cultural influences (Shuster, 2004; SIRC, 1998; ter Bogt, Schmid, Gabhainn, Fotiou, and Volleberg, 2006). However, it is possible that in the modern western society, easy access to different substances and a more stressful lifestyle precludes detecting a relationship between biological quality (measured with FA) and proneness to substance use. It would be interesting to study this relationship in traditional societies where the handicap hypothesis related to drug use may be detected, at least in young men. The possibility that in our evolutionary past “recreational substances” may not have been used at all or were different from those used in modern western countries does not necessarily undermine our evolutionary reasoning, because we focus on risk-taking behavior and not on the mental mechanisms related to specific types of recreational substances. It is well known that the recreational substances mentioned here are usually unhealthy and, therefore, using them poses some health risk. Furthermore, studies indicate that there is a moderate positive correlation (rs between 0.4 and 0.5) between health and proneness to recreational risk-taking behavior (Johnson, Wilke, and Weber, 2004; Weber, Blais, and Betz, 2002). This means that health risk itself can be studied as an estimation of proneness to risk-taking in all situations that are related to health and, therefore, fitness problems.
There are studies showing that taking health risks is more likely by young men in the context of sexual selection, e.g., attracting short-term partners (Burriss, Rowland, and Little, 2009). Men, for instance, disdain health risks more than women (Wilson, Daly, Gordon, and Pratt, 1996). The potential example of showing off a readiness to take health risks by men is tattooing and non-conventional piercing (Koziel et al., 2010). On the other hand, drug taking (Farthing, 2005) and health–risk taking in general appeared to be unattractive in potential partners by both sexes (Wilke, Hutchinson, Todd, and Kruger, 2006). This, however, does not mean that health risk cannot be considered a potential attractor in intersexual selection. Firstly, it has been shown that the attractiveness of taking a physical risk may depend on sexual strategy. Although both men and women prefer risk-avoiding partners for long-term relationships, they seem to accept risk-takers in short-term relationships (Sylwester and Pawlowski, 2011). It has also been shown that women under the influence of alcohol and drugs engage in short-term liaisons more often than sober women (Grello, Welsh, and Harper, 2006). Furthermore, the amount of money spent on alcohol is a good predictor of unrestrictiveness in sexual behavior (Clark, 2004). Using health-risking drugs might play some role in intra-male competition and hierarchy, which to our knowledge has not been studied. It can be hypothesized that stronger and more dominant young men are more prone to take health risks and start using stimulants earlier.
In summary, we did not find support for the hypothesis that smoking, drinking, or using drugs serve as a signal of biological quality or are related to the handicap principle hypothesis.
Footnotes
Acknowledgements
We would like to thank Michael Stirrat for all his suggestions and proof reading, and two anonymous reviewers for their valuable suggestions.