
Abstract
Biases against the mentally ill are historically and cross-culturally pervasive, suggesting they may have an evolutionary basis. The prevailing view is that people seek to distance themselves from the mentally ill because they are perceived as dangerous, violent, and incompetent. However, because of similarities between sickness behaviors and symptoms of some mental disorders, it was hypothesized that mental illness stigma could be partially explained as a function of behavioral immune system biases designed to avoid potential sources of contagion. In two experiments, it was found that mental illness was implicitly associated more with disease than danger. In Experiment 1, this implicit association was exacerbated among people who have had their biological immune system activated by a recent illness. In Experiment 2, experimentally priming disease salience increased implicit association between mental illness and disease. Implications for the evolutionary origins of prejudice and the prevention of mental illness stigma are discussed.
Introduction
Mental illness has likely existed throughout human history. Stigma towards the mentally ill exists cross-culturally (Guimon, Fischer, and Sartorius, 1999) and is widespread and universal throughout history – suggesting an evolved bias to avoid the mentally ill (Kurzban and Leary, 2001). The prevailing view is that stigma exists because the mentally ill are perceived as dangerous, violent, and incompetent (Corrigan and Cooper, 2005; Jorm, Reavley, and Ross, 2012). Some evidence suggests that the mental disorders that are most stigmatized as dangerous are the ones believed to be due to organic causes, or “brain disease,” and include schizophrenia and bipolar disorder, among others (Dietrich, Matschinger, and Angermeyer, 2006; Furnham and Rees, 1988; Furnham and Wong, 2007; Jorm and Griffiths, 2008; Pescosolido et al., 2010). Yet, the psychological processes that drive behavioral avoidance toward the mentally ill remain unclear. Whereas avoidance may be driven by perceptions of the mentally ill as dangerous, it may also be due to the perception of the mentally ill as sick.
In response to the recurrent threat of infectious disease, a variety of species appear to have evolved behavioral adaptations to counter pathogen threat (Curtis, 2007). For example, grazing sheep avoid grasses infected with their own fecal matter (Cooper, Gordon, and Pike, 2000) and bullfrogs use chemical cues to avoid diseased conspecifics (Kiesecker, Skelly, Beard, and Preisser 1999). Among humans, it is believed that infectious disease was perhaps the single greatest contributor to morbidity and mortality ancestrally (e.g., Ewald, 1994; Wolfe, Dunavan, and Diamond, 2007). In response, there exists a behavioral immune system – a psychological system designed to promote the avoidance of potential pathogen carriers (Neuberg, Kenrick, and Schaller, 2011; Schaller and Park, 2011). When pathogen concerns are salient, people respond to heuristic disease cues with a range of affective (e.g., disgust), cognitive (e.g., attention), and behavioral (e.g., avoidance) reactions that ultimately serve to protect oneself from possible sources of infection (Ackerman et al., 2009; Curtis, Aunger, and Rabie, 2004; Miller and Maner, 2011; 2012; Schaller and Duncan, 2007).
The imperfect relationship between potential disease cues (e.g., facial discolorations, missing limbs) and actual infectious disease presents a signal detection problem. Overperceiving disease cues and frequently committing false-positive errors (Haselton and Nettle, 2006, Schaller and Park, 2011) is an adaptive response to ambiguous environmental threat (Nesse, 2005). This bias leads people to interpret any deviation from the norm to be evidence for parasitic infection, and has been used to explain prejudice towards immigrants and foreigners (Faulkner, Schaller, Park, and Duncan, 2004; Navarrete, Fessler, and Eng, 2007), the physically disabled (Park, Faulkner, and Schaller, 2003), the elderly (Duncan and Schaller, 2009), and the obese (Lund and Miller, 2014; Miller and Maner, 2012; Park and Isherwood, 2011; Park, Schaller, and Crandall, 2007). However, no study to date has tested whether the behavioral immune system is activated in response to a potential heuristic disease cue that is less visually obvious – mental illness.
Consideration of behavioral immune system processes leads to the prediction that biases towards the mentally ill may, in part, exist because mental illness may be taken as a heuristic cue to infectious disease. When humans and other animals are combating infectious disease, they exhibit a characteristic suite of responses that include lethargy, decreases in appetite, inability to concentrate, sleepiness and fatigue, and a loss of interest in activities they would otherwise find pleasurable (Dantzer et al., 1998; Hart, 1988; Raison, Capuron, and Miller, 2006). While these behaviors might be evolutionarily adaptive in that they allow the body to conserve enough energy to mount a healthy immune response, the symptoms of these sickness behaviors are similar to symptoms exhibited by those with mental disorders such as depression, some anxiety disorders, and sleep disorders, among others (see Kelley et al., 2003 for a review). Importantly, the biological basis of sickness behaviors include increases in proinflammatory cytokines that have been implicated in both healthy immune response to disease and in some psychological disorders such as depression (Raison et al., 2006). Given the physiological and behavioral similarities between normal immune responses and mental disorders, it is plausible that an oversensitive behavioral immune system would misperceive mental illness cues as physical illness.
Additionally, the overwhelming majority of research on perceptions of the mentally ill has focused on explicit measures – which are often confounded with social desirability (Stier and Hinshaw, 2007). A notable exception is a study by Teachman, Wilson, and Komarovskaya (2006) who found that the majority of their participants revealed negative implicit attitudes towards the mentally ill, associating them with the concepts of “bad”, “blameworthy”, and “helpless”. Importantly, Link and Cullen (1983) found a discrepancy between the relatively benign attitudes towards mental illness on self-report measures and the more negative attitudes evidenced among the same participants when assessed implicitly. Finally, because implicit measures also show predictive validity with behavioral measures of bias and discrimination that differ from patterns derived from explicit measures (e.g., Hofman, Gawronski, Gschwendner, Le, and Schmitt, 2005), we focused exclusively on implicit perceptions of mental illness in the present study.
Overview of Current Experiments
Despite a large body of evidence linking explicit mental illness stigma with danger (for review, see Jorm et al., 2012), we predicted that people would implicitly associate mental illness with disease over danger. Additionally, we hypothesized that people who are particularly concerned about disease will demonstrate a stronger implicit association between mental illness and disease. In Experiment 1, we capitalized on natural variance in the salience of disease caused by recent illness to evaluate participants' implicit perceptions. In Experiment 2, we manipulated contextual disease concerns using experimental priming methodology.
Experiment 1: Chronic Disease Concerns and Implicit Perceptions of Mental Illness
Research has shown that activation of the behavioral immune system (i.e., viewing photos of disease cues) can lead to activation of the biological immune system (i.e., stimulated production of cytokine interleukin-6; Schaller, Miller, Gervais, Yager, and Chen, 2010). Recent research has also demonstrated that activation of the biological immune system (i.e., by being recently ill and immunocompromised) can lead to compensatory heightened activation of behavioral immune system processes (Miller and Maner, 2011). In Experiment 1, we hypothesized that people would implicitly associate mental illness with disease over danger. We also hypothesized that being recently sick, an ecological context in which disease avoidance processes are particularly heightened, would lead to a stronger implicit association between mental illness and sickness.
Participants
One-hundred sixty-six University of Kentucky undergraduates participated by taking an online survey for course credit. Ten participants exited the survey before completing all measures, leaving complete data from 156 participants (100 women, 56 men; see Table 1 for complete demographics).
Summary of Descriptive Statistics Across Experiments

Procedure
This experiment was approved by and conducted in compliance with the guidelines of the University of Kentucky Institutional Review Board. Participants first provided informed consent. Participants then completed a modified Implicit Association Test (Greenwald, Nosek, and Banaji, 2003) called the Single-Target Implicit Association Test (ST-IAT, Wigboldus, Holland, and van Knippenberg, 2006). The advantage of the ST-IAT is that it allows for the evaluation of a single target object without needing to simultaneously contrast it with a counter-category. Whereas a typical IAT yields a preference index relative to a comparison concept, the ST-IAT yields a preference index solely for the target of interest (in our study, the term mentally ill).
While the ST-IAT is a relatively new and untested measure, a recent study demonstrated that it displayed sufficient discriminant validity, test-retest reliability, and convergent validity with explicit measures (Bluemke and Friese, 2008). This measure is also conceptually nearly identical to another recent alternative IAT, the Single Category Implicit Association Test (SC-IAT) which has demonstrated reliability and validity as an implicit individual difference measure (Karpinski and Steinman, 2006).
Participants began with 20 training trials for the evaluative attribute words prior to the first combined block (attribute words = danger: dangerous, unsafe, violent, aggressive; sick: sick, diseased, ill, unhealthy). Following the training trials participants were presented with four combined blocks (two blocks of mentally ill and danger then mentally ill and sick), introducing the target words: schizophrenia, bipolar disorder, depression, and obsessive-compulsive disorder.
Following the ST-IAT we assessed illness recency using an item from a previous study (Miller and Maner, 2012). Participants indicated their level of agreement (1 = Strongly Disagree to 7 = Strongly Agree) with the following statement: “I had a cold or flu recently.” We chose to use an item directly assessing the recency of the cold and flu because these are common ailments in participants' lives. We suspect that reactions to the use of items mentioning other short-term illnesses (e.g., bronchitis) would be similar, but these other illnesses are typically less common. We also felt that the use of an item too broad (e.g., “felt sick”) would capture other uncomfortable physical states (e.g., being hungover) that are not directly relevant to our hypotheses. Finally, participants completed general demographics and were debriefed.
Results and Discussion
Using the median to determine outliers has been proposed to be the best method for outlier detection (Leys, Ley, Klein, Bernard, and Licata, 2013). Six participants data were excluded for having error rates and/or average latencies greater than two interquartile ranges from the median on the IAT (error rate median: 8.6% of trials; error rate interquartile range: 12; average latency median: 642 ms; average latency interquartile range: 322 ms). For the remaining 150 participants, implicit associations were calculated using the D score measure with built-in error penalty, as recommended by Greenwald et al., (2003).
Positive D scores on the IAT reveal an implicit association between mental illness and disease, while negative D scores on the IAT reveal an implicit association between mental illness and danger. D scores (M = 0.07, SD = 0.27) were significantly above zero, t(149) = 3.139, p = .002, indicating that, overall, participants implicitly associated mental illness with sickness over danger. We then assessed how illness recency affected IAT D scores. Recent illness positively predicted D scores, β = 0.226, p = .005 (see Figure 1).

Scatterplot depicting the positive association between illness recency and IAT D scores.
Additionally, in an exploratory analysis we assessed the relationship between illness recency and IAT D scores separately by gender. We found that in men, recent illness and D scores were positively correlated r(52) = 0.364, p = .008. In women, recent illness and D scores were in the hypothesized direction but were not significantly correlated r(98) = 0.151, p = .137.
In summary, our prediction that people overall would implicitly associate mental illness with disease over danger was supported. Additionally, we found that those that had been recently ill (and thus had heightened behavioral immune system concerns) tended to implicitly associate mental illness with sickness to a greater degree, and that men might make a stronger implicit association between mental illness and disease than women.
Experiment 2: Situational Disease Concerns and Implicit Perceptions of Mental Illness
In Experiment 2, we again predicted that participants would implicitly associate mental illness with sickness over danger. We also aimed to determine whether situational disease salience, such as being warned about a recent epidemic disease threat, would affect the implicit association between mental illness and sickness. We predicted that priming pathogen concerns (i.e., bringing disease-relevant concepts into working-memory) would lead to a greater implicit association between mental illness and sickness.
Participants
Ninety-five University of Kentucky undergraduates participated by doing an in-lab experiment for course credit (52 women, 43 men; see Table 1 for complete demographics).
Materials and Procedure
This experiment was approved by and conducted in compliance with the guidelines of the University of Kentucky Institutional Review Board and participants first provided informed consent. Participants were then randomly assigned to read one of three articles on a computer screen in the laboratory, all used in previous studies (Miller and Maner, 2012). They were told that the experiment was ostensibly about “memory processes”, that they were going to read a “real” article that had been in the news recently, and that they were going to be tested on its contents later in the experiment. Participants were randomly assigned into one of three conditions: A disease condition designed to activate pathogen concerns, a control condition based on the extant research designed to prime danger, and a second control condition designed to prime a general non-pathogen and non-crime-related threat. In the disease salience condition, participants read a fictional news article about the threat of the H1N1 virus. In the first control condition (crime salience), participants read a fictional news article about the threat of violent crime. In the second control condition (economic salience), participants read a fictional news article about the threat of job losses. All three articles contained equivalent numbers of deaths or losses (i.e., 30-90,000 H1N1 deaths vs. 30-90,000 crime deaths vs. 30-90,000 job losses), and were similar in article length, style, and appearance.
Our contrast of interest was between the disease saliency prime and the average of the two control conditions. We predicted that those in the disease salience condition would exhibit a greater tendency to implicitly associate mental illness with sickness than those in the average of the control conditions. Following the article prime, participants completed the mental illness ST-IAT. All target and attribute terms as well as procedural aspects were identical to Experiment 1. Finally, participants completed general demographics and were debriefed.
Results and Discussion
Five participants were excluded for having error rates and/or average latency values greater than 2 interquartile ranges from the median on the IAT (error rate median: 7.1% of trials; error rate interquartile range: 7; average latency median: 625 ms; average latency interquartile range: 283 ms). For the remaining 90 participants, implicit perception scores were again calculated using the D measure with built-in error penalty. Participants' D scores (M = 0.10, SD = 0.24) were significantly above zero, t(89) = 3.916, p < .001, indicating again that, overall, participants implicitly associated mental illness with sickness over danger.
Consistent with our hypothesis, our planned contrast revealed that those in the disease salience condition (M = 0.18, SD = 0.21) implicitly associated mental illness with sickness to a significantly greater degree than those in the average of the crime salience (M = 0.04, SD = 0.25) and the economic salience (M = 0.09, SD = 0.25) conditions t(87) = 2.067, p = .042, ω2 = .234 (see Figure 2). We also assessed the strength of the implicit association between mental illness and sickness by condition. Participants in the economic condition had D scores marginally above zero t(28) = 1.96, p = .06. Participants' D scores in the crime condition did not differ from zero t(34) = 0.98, p = .33. Finally, as expected, participants' D scores in the disease condition were significantly above zero t(28) = 4.45, p < .001.
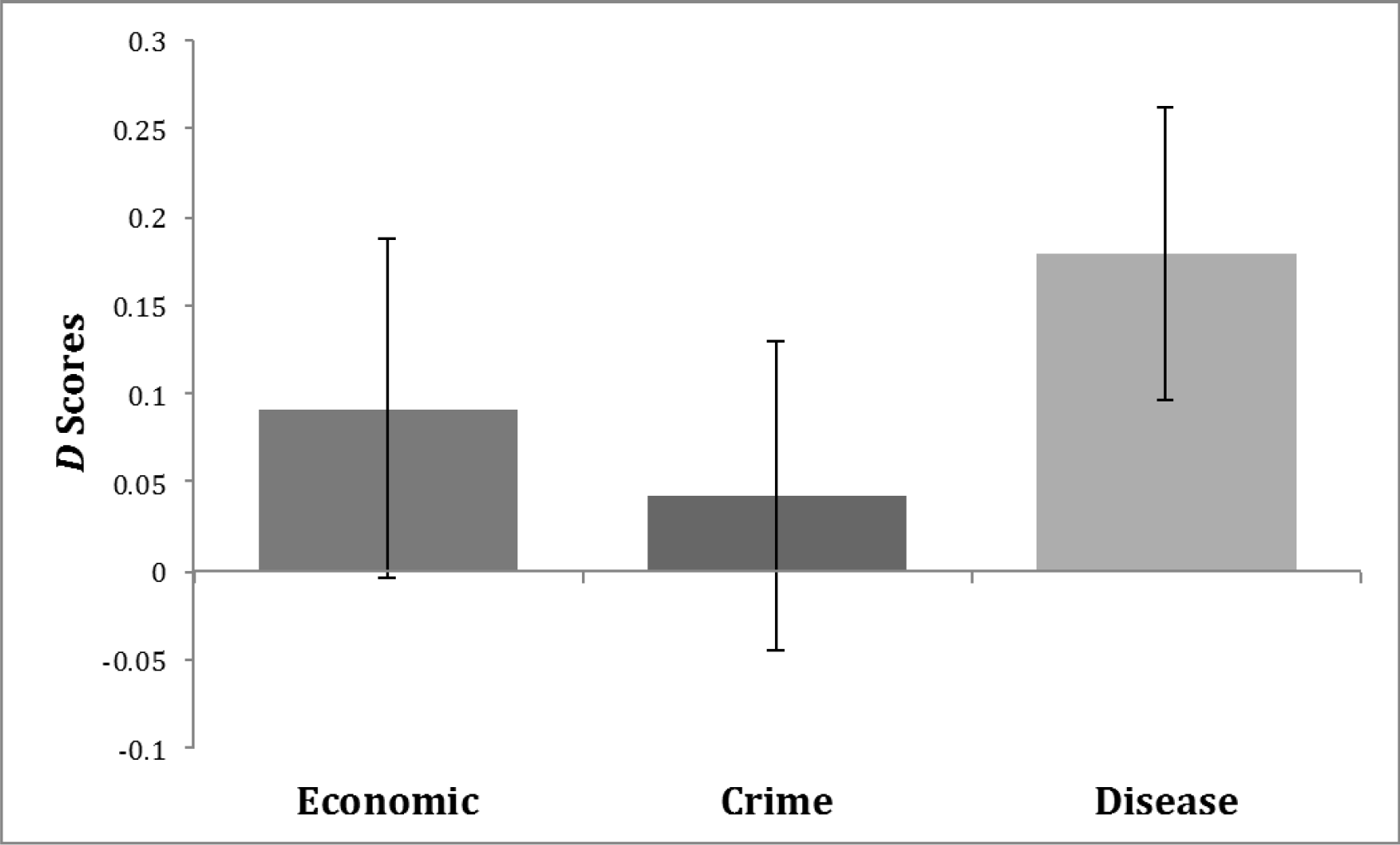
Experimental manipulation of disease salience increases the implicit association between mental illness and sickness.
As another exploratory analysis, we examined whether there were gender differences in D scores in response to the above three primes. The condition by gender interaction was not significant F(2,89) = .005, p =.93. Therefore, the gender difference in implicit perceptions of mental illness did not replicate in Experiment 2, and we address this inconsistent pattern further in the General Discussion.
In summary, in a second experiment it was found that people implicitly associate mental illness with disease over danger, an effect that is enhanced among those who are primed with disease concerns. Importantly, the results indicate that the association between mental illness and sickness appears to be more strongly elicited by pathogen concerns relative to the elevated arousal level of more general threats.
General Discussion
Across two experiments we found that people overall implicitly associate mental illness with disease over danger. Using different methodologies in both experiments, we also found that individuals that have heightened behavior immune system concerns – whether as a result of recent illness or a situational disease prime – are more likely to make this implicit link. Taken together, these findings accent the growing body of research on the behavioral immune system, and to our knowledge these experiments are the first to investigate whether mental illness may be taken as a heuristic pathogen cue.
The present findings may contribute to further research on the causes and consequences of – as well as the prevention of – mental illness stigma. Mental illness stigma has profound consequences, and affects how employers, neighbors, medical practitioners, family members, and the general public perceive those with mental illness (e.g., Corrigan and Miller, 2004; Link, Struening, Rahav, Phelan, and Nuttbrock, 1997). Further, stigma can become internalized and can be a significant obstacle for people seeking or continuing psychotherapy (Rüsch, Angermeyer, and Corrigan, 2005). Given the profound consequences of the stigma faced by people with mental illness, research seeking to understand the mechanisms of such stigma is of crucial importance. The present findings suggest that the stigma against the mentally ill is due, in part, to people associating mental illness with disease cues. Such knowledge could help those with mental disorders change their self-stigma and remove an important barrier from seeking treatment. Future research should investigate the mechanisms that would be most successful for changing self-stigma in those with mental illness.
Additionally, we assessed whether gender differences in implicit perceptions of mental illness existed in our study. In Experiment 1, we found that men made a stronger implicit association between mental illness and disease. However, in Experiment 2 we found no evidence for a gender difference in implicit perceptions. In previous studies, no consistent pattern has been found between gender and mental illness perceptions. Some studies have found that men expressed more negative attitudes, while other studies have found that women expressed more negative attitudes, and still other studies have found no gender difference (for review, see Angermeyer and Dietrich, 2006). We encourage further research in this area.
Limitations and Future Directions
First, these experiments only focused on implicit perceptions of mental illness. Future research should explore whether behavioral immune system processes affect explicit mental illness perceptions or stigma. Second, research suggests that language influences perceptions (e.g, Barrett, Lindquist, and Gendron, 2007); for example, the term by which we refer to those suffering from mental health problems may affect our perceptions of them (Byrne, 2000). Therefore, using the term ‘mental illness’ – versus, say, ‘mental disorder’ – may be leading to a stronger implicit association between mental illness and disease. However, in order to be consistent with the label often used by clinicians and the media (Stuart, 2006; Wahl, 1992) we chose to use the term ‘mental illness’ in this first set of experiments. Future research may want to investigate how behavioral immune system biases affect perceptions of other mental health labels.
Additionally, future research could assess whether the perceptions of mental illnesses may vary by disorder and by evolutionary concern. There is accumulating recent evidence that depression is linked to immune function (Raison and Miller, 2013). Researchers have proposed that depression specifically – with its suite of sickness behaviors – may be an evolutionary strategy for aiding the biological immune system's defense against infection (Anders, Tanaka, and Kinney, 2013; Raison and Miller, 2012). It is also likely that perceptions towards those with schizophrenia and its often associated unpredictable and violent behavior would be driven more by personal safety concerns than behavioral immune system concerns.
Conclusion
In response to the considerable fitness consequences posed by infectious pathogens, many animals (including humans) evolved a behavioral immune system as a first line of defense against disease threat. As the relationship between potential disease cues and the actual presence of disease is imperfect, people often commit false-positive errors, seeing disease cues where they may not exist. These biases have been used to explain prejudice and stereotyping towards a variety of groups, including the obese, the elderly, immigrants and foreigners (for review, see Schaller and Park, 2011). Because of the strong resemblance between healthy immune responses and the symptoms of some mental illnesses, it is not inconceivable that the threat of infectious pathogens influences perceptions of the mentally ill.
In the broader context, mental illness stigma and prejudice negatively affects thousands of people each year, leading to reluctance to seek treatment, ostracism, job discrimination, and other negative outcomes (Corrigan and O'Shaughnessy, 2007). In order to prevent stigma or aid those already suffering from it, it is immensely important to understand its origins from every angle. Therefore, we hope that future research investigating the evolutionary underpinnings of mental illness perceptions will lead to the reduction of stigma and prejudice.
Footnotes
Acknowledgements
The authors thank Saul L. Miller for early involvement in the study, as well as Will M. Gervais, Daniel R. Evans, and Mariah A. Macham for critical feedback on early versions of the manuscript.