
Abstract
The purpose of the study was to develop a new ethogram for the assessment of children and adolescents with autism spectrum disorders (ASD) and intellectual developmental disorder (IDD) and to test whether this instrument accurately distinguishes ASD participants (n = 61) from IDD participants (n = 61). An ethogram with 88 behavior elements was generated, including body postures, verbalizations, facial expressions, motor stereotypies, head postures, gaze behavior, gestures, and interpersonal distance. Significant differences were detected between both groups in classic ASD behaviors; in behaviors that are deficient in ASD according to established theoretical models, such as symbolic play, gaze direction, gaze following, and use of mental state language; in atypical behaviors that have also been described previously in ethological studies with ASD; and in the nonspecific behaviors of ASD, such as walk, look own body, explore, and cry. The predictive success of a diagnosis of ASD in the logistic regression model with the ethogram's factors was 98.4%. The results suggest that this ethogram is a powerful and useful tool for both the detailed study of the social behaviors of autistic children and adolescents, and for discriminating ASD and IDD.
Introduction
Modern ethology - that is, the science specialized in the evolutionary study of animal behavior - was founded by Lorenz, Tinbergen, and von Frisch (e.g., Lorenz, 1974; Tinbergen 1974). It was subsequently expanded and elaborated with regard to human behavior by Eibl-Eibesfeldt (1989). In this paper, we aim to show how the methodology of ethologists can be successfully employed to autism spectrum disorders. Autism spectrum disorders (ASD) are characterized by marked deficits in social reciprocity, social use of communication, and by the presence of repetitive and stereotyped behaviors or interests (American Psychiatry Association, 2013). The diagnosis of ASD is based on direct behavioral observation or on information about patterns of behavior and symptoms described by caregivers (Huerta and Lord, 2012). Often, the distinction between ASD and other developmental disorders, such as Intellectual Developmental Disorder (IDD), seems vague and ill-defined (Nazeer and Ghaziuddin, 2012). As children with ASD frequently have severe verbal communication deficits, the powerful and non-invasive observation methods of ethology may contribute significantly to the development of a more accurate and valid strategy for measuring the behavior of children with ASD (Klein, 2000).
A starting point in many ethological studies is the compilation of a detailed ethogram, which is a thorough descriptive catalog of the behavior patterns that form the basic behavioral repertoire of the study subjects (Troisi, 1999). Observed behaviors may differ in duration. Brief behaviors are called point-events (e.g., show, point, sit down). Lasting-events are behaviors of longer, but varying, duration (e.g., current status, interpersonal distance) (van Engeland, Bodnàr, and Bolhuis, 1985).
Autism spectrum disorders have drawn the attention both of ethologists and evolutionary psychologists due to their complexity and severe impact on the social life of affected individuals (e.g., Baron-Cohen, 2009; Reser, 2011; Tinbergen and Tinbergen, 1972; Zabel and Zabel, 1982). Elisabeth Tinbergen and Niko Tinbergen, for example, formulated a theory of the etiology of ASD couched in ethological terms (Tinbergen and Tinbergen, 1972), but the absence of evidence for their claims and the lack of precision with which they used the terms “autism” and “Kanner's syndrome” prevented their theory from having subsequent influence (Wing and Ricks, 1976). Ethological studies of ASD have focused on: systematic behavioral observations, i.e., recordings of preselected, well-defined behaviors cataloged on a timed sampling schedule; quantitative measurements of the frequencies of point events or relative durations of the behaviors (e.g., lasting-event categories); and detailed descriptions of behavior (Castell, 1970; Churchill and Bryson, 1972; Hutt and Ounsted, 1970; O'Connor and Hermelin, 1967; Pedersen and Schelde, 1997; Richer and Coss, 1976; Richer and Richards, 1975; van Engeland et al., 1985). Nevertheless, in the majority of these studies, the sample was relatively small and/or there were no comparison groups with other mental disorders, weakening their validity and specificity. Therefore, the aims of this study were to develop a new, detailed, valid, and useful ethogram with a large sample of children and adolescents with ASD, according to DSM-5 criteria, and to test whether this instrument accurately distinguishes ASD from IDD, another developmental disorder that is usually diagnosed in childhood.
Materials and Methods
Participants
All of the children and adolescents with ASD and IDD enrolled in this study were patients of the Child and Adolescent Psychiatry outpatient clinics of the Hospital of the University of Campinas (Unicamp) located in Campinas, São Paulo, Brazil. The initial sample consisted of 146 participants (69 with ASD and 77 with IDD) between the ages of 3 and 18 years (M = 10.8, SD = 4.1). The sample was composed predominantly of males (n = 113; 77.4%) and of children (n = 76; 52.1%). Clinical psychiatrists with an average of 20 years of experience treating patients diagnosed the participants using DSM-IV-TR (American Psychiatric Association, 2000) criteria for ASD and IDD. Both groups also met the proposed revised diagnostic criteria for ASD and IDD in the DSM-5 (American Psychiatric Association, 2013). The ASD participants comprised 69 children and adolescents diagnosed with ASD between the ages of 3 and 18 years (M = 9.4, SD = 4.6). The 77 IDD participants were children and adolescents between the ages of 4 and 16 years (M = 12.0, SD = 3.1). Sixty-seven participants were receiving psychotropic medication, among which antipsychotics and serotonin reuptake inhibitors were the most frequently prescribed substances.
After the participants' entry into the study, the diagnosis of ASD was confirmed by the Brazilian version of the Childhood Autism Rating Scale (CARS-BR; Pereira, Riesgo, and Wagner, 2008), which is a behaviorally-based rating scale used to evaluate the severity of autistic symptoms. Also following their entrance into the study, all participants with IDD between the ages of 6 and 16 years completed the Wechsler Intelligence Scale for Children or Adults, 3rd edition, Brazilian version (Wechsler, 2002, 2004), to determine their full-scale IQ (FSIQ). Participants with IDD aged less than 6 years were intellectually assessed with the Columbia Mental Maturity Scale (CMMS; Burgemeister, Blum, and Lorge, 2011). The two groups were matched in chronological age. Table 1 presents the results of the comparison between the ASD and IDD groups regarding age, gender, and CARS-BR total score.
Sample characteristics (n = 122)

Notes: ASD = Autism Spectrum Disorders; IDD = Intellectual Developmental Disorder; Significant values in bold
A group of 24 participants (16.4%) was excluded from the main analyses as they could not be unequivocally categorized as either ASD or IDD, according to the CARS-BR cutoff score (< 30) for ASD and the WISC-III/ WAIS-III or CMMS cutoff score for IDD (IQ < 70 or Age Deviation Score below two standard deviations in CMMS). This group was analyzed separately, in order to verify if these individuals could also be categorized based on the ethogram. Parents signed consent forms approved by the Institutional Review Board of Unicamp.
Measures
Video recorder. A high-definition hidden camera pen (by Brickhouse) with a digital video recorder (1280 × 720 pixels, 30 frames per second, 8 gigabytes), audio video interleaved format (AVI), and high speed universal serial bus (USB) 2.0 interface was used to record each participant during their regular psychiatric assessment.
Ethogram. We developed an ethogram from observations of the study participants' social behaviors in outpatient clinics of the Unicamp Hospital. This ethogram also incorporates measures from the literature of social behaviors of children with ASD in naturalistic settings, such as gaze and physical aversion, interpersonal distance, joint attention, mental state language, and other communication skills (Chiang, 2008, 2009; Hutt and Ounsted, 1970; Jones and Schwartz, 2009; Macintosh and Dissanayake, 2006; Perdersen and Schelde, 1997; Richer and Coss, 1976; van Engeland et al., 1985). To compose the categories and subcategories of the ethogram, we selected the first 10 recordings from ASD and IDD participants, for a total of 20 recordings. The All Occurrences Sampling method was used to analyze the video recordings. In this method, all behaviors observed within a period of time are included in the ethogram (Altmann, 1974; Setz, 1991). The final categories of the ethogram included body postures, verbalizations, motor stereotypies, head postures, gaze behavior, gestures, current status, and interpersonal distance (see Appendix I). Additionally, we developed two scoring sheets to facilitate the count of point- and lasting-event categories during the video recording analyses (see Appendices II and III).
Procedure
All the participants were videotaped in the outpatient clinics of the Unicamp Hospital during a follow-up psychiatric assessment in the company of their mothers, in a 343 cm × 230 cm room containing one table, four chairs, one gurney, one trash can, and one sink. Video recordings of each patient generally lasted 15 minutes, and the participants were inside the room for the duration of the recording. The parents knew about the recording, but the patients did not. The first author of the present study operated the video recorder pen but avoided interaction with the participants, caregivers, and psychiatrist.
Video recordings of each participant were analyzed using the All Occurrences Sampling method (Altmann, 1974; Setz, 1991), with a time interval of 2 minutes for point-events (e.g., point, look, talk), resulting in five periods of continuous analysis (i.e., measurements at 0–1, 3–4, 6–7, 9–10, and 12–13 minutes; see Appendix II), as well as the Scan Sampling method (Altmann, 1974; Setz, 1991), with intervals of 1 minute for lasting-event categories, totaling 15 distinct instantaneous scans (see Appendix III). In the Scan Sampling method, one records the lasting-event categories (e.g., an individual's current activity or interpersonal distance) at preselected moments in time. The first author of the present study analyzed the video recordings and was not blind to the diagnosis of the participants during the video recording and the coding process.
Statistical analysis
The data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 17.0. The variables were tested for normality using the Kolmogorov-Smirnov test. An arcsine square root transformation (ASRT) for lasting-event categories was performed. The ARST has long been a standard procedure when analyzing proportional data in ethology (Sokal and Rohlf, 1995; Zar, 1998). The frequency of each behavior element (i.e., the subcategories of our ethogram) was computed for each participant, and the frequencies in the experimental group (ASD) were compared with those in the control group (IDD). Mann-Whitney's test was used to compare age and the frequencies of behavioral elements between participants with ASD and IDD. A Chi-square test was used for the comparison of gender.
In order to reduce the subcategories of the ethogram to a small set of variables, a principal components factor analysis (eigenvalues ≥ 1) with Varimax rotation and Kaiser Normalization was performed on the total sample. The subcategories of the ethogram were standardized for the analysis due to differences in the variables. Factors with eigenvalues larger than 1 were initially extracted using principal components. The scree plot was then examined using Cattell's (1966) point of inflection criterion to determine factor numbers. Only behavior elements with a factor value in excess of 0.40 were used in this analysis, and elements that loaded on two different factors with a difference of factor loadings less than 0.20 were eliminated. The reliability analysis was performed on the final ethogram to assess the internal consistency as measured by Cronbach's alpha.
Two binary multivariate logistic regression analyses, with backward likelihood ratio selection method, were conducted with the ethogram's new factors and with 10 main ethogram categories (i.e., the sum of the frequencies of each subcategory) to explore the predictors of the ASD diagnosis.
Results
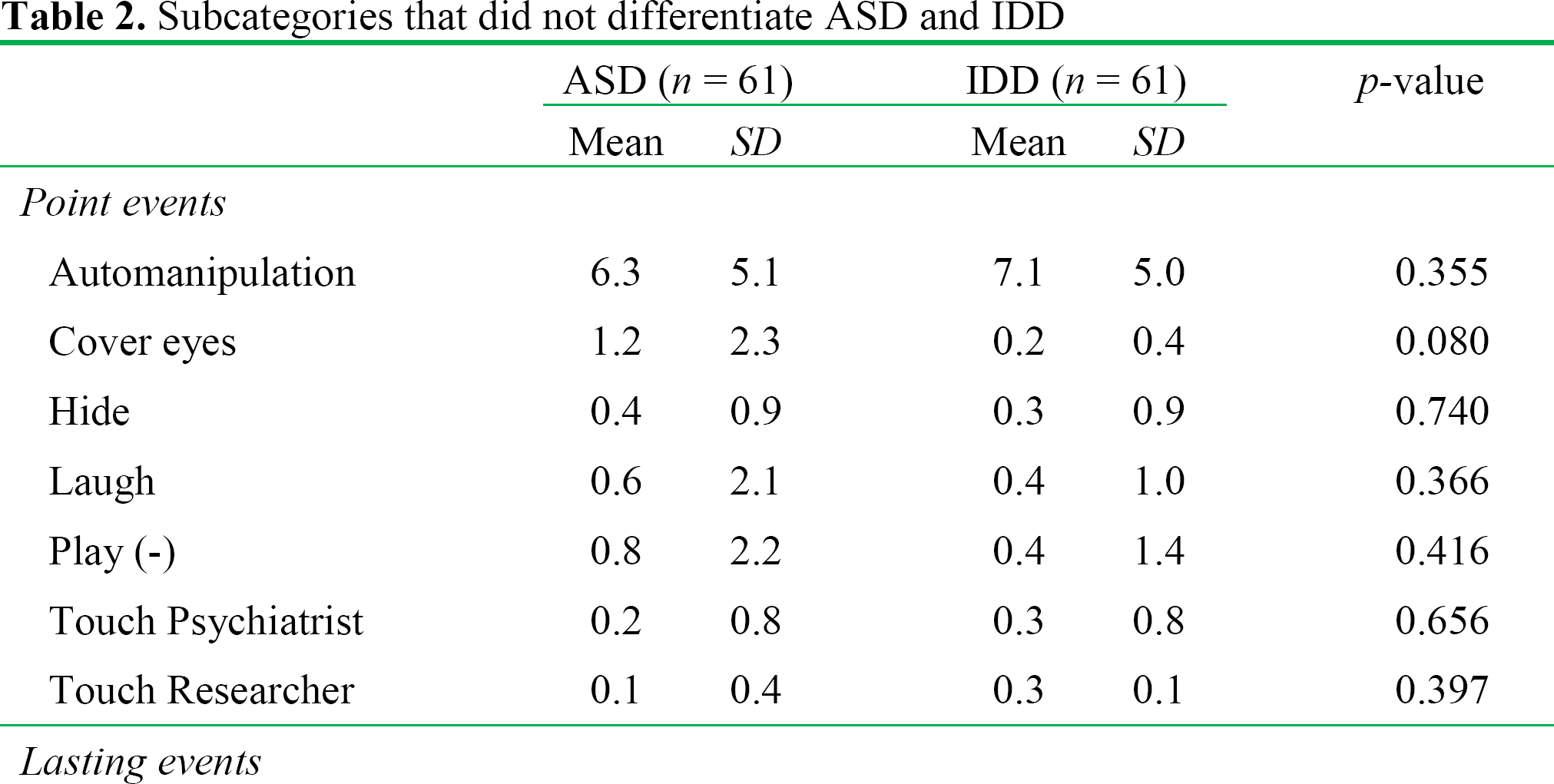
We collected 2,190 minutes (36.5 hours) of video recordings for the total sample. The full analysis of the 2,190 minutes of recording took 13,140 minutes, or 219 hours - 90 minutes per participant. The final ethogram comprised 10 major categories divided into 88 subcategories, 67 of which described point-events, and 21 of which described lasting-event categories (see Appendix I for an overview of the main categories, their behavioral elements, and a brief description of each element). Of the 88 subcategories in the ethogram, participants with ASD and IDD showed significant differences in 77 subcategories. Eleven subcategories did not differentiate between ASD and IDD (see Table 2). This could be related to the large variation within the samples, and not necessarily a lack of difference between ASD and IDD. Children and adolescents that were excluded from the main analyses, based on difficulties in categorizing them according to standard diagnostic checklists for ASD and IDD, exhibited significant differences in 20 subcategories of the ethogram (see Table 3). The subcategories of echolalia, rock, and spin were observed only in the ASD group (n = 8).
Subcategories that did not differentiate ASD and IDD
Subcategories that differentiate ASD and IDD in the unclassified group (n = 24)

The factor analysis of the ethogram's behavioral elements yielded a model with 24 factors, accounting for 79.3% of the variance. Table 4 gives an overview of the factor values and explains the variance and the internal consistency of the instrument. Four factors were identified based on eigenvalues and on the scree plot test, and these accounted for 37.6% of the variance. Thirty behavioral elements were excluded as they showed communalities below 0.4 or presented high factor loadings on two or more factors. Each of the four factors was named according to recognizable common features of the highest-loading behavioral elements. The factors were named as follows: Factor 1, General Movements (GM); Factor 2, Functional Communication (FC); Factor 3, Interpersonal Discomfort (ID); Factor 4, Stereotyped Behaviors (SB). Significant differences were found between the ASD and IDD patients in all four factors (p > .01). In relation to the IDD group, the ASD group had significantly higher scores on General Movements, Interpersonal Discomfort and Stereotyped Behaviors and presented significantly lower scores on Functional Communication.
Principal components analysis after Varimax rotation (n = 122)

Note: GM = General Movements; FC = Functional Communication; ID = Interpersonal Discomfort; SB = Stereotyped Behaviors
The binary logistic regression with the ethogram's factors showed that Functional Communication and Interpersonal Discomfort were significant predictors of ASD (see Table 5). A second logistic regression with the ethogram's main categories showed that Head Postures, Stare, and Look were significant predictors of the ASD (see Table 6). The predictive success of a diagnosis of ASD in the two logistic regression models was 98.4% and 95.9%, respectively. Due to problems of multicollinearity or singularity, lasting-event categories were removed from logistic regression analyses. The Hosmer-Lemeshow goodness-of-fit statistic (Hosmer and Lemeshow, 2000) was p > 0.05 in all steps of both logistic regression analyses.
Stepwise binary logistic regression analysis of the ethogram's factors predicting ASD (n = 122)

Notes: B = Partial regression coefficient; SE = Standard Error; OR = Odds ratio; 95% CI = 95% Confidence interval; Significant values in bold.
Stepwise binary logistic regression analysis of the ethogram's major categories predicting ASD (n = 122)

Notes: B = Partial regression coefficient; SE = Standard Error; OR = Odds ratio; 95% CI = 95% Confidence interval; Significant values in bold.
Discussion
The primary goal of this study was to develop a new ethogram describing behavioral elements that emerge in the psychiatric assessment of children and adolescents with ASD and IDD. Other objectives were to verify that this ethogram could differentiate the ASD group from the IDD group and that it could reliably predict the ASD according to the new DSM-5 criteria. The results of this study should be regarded with some prudence as to their generalizability. After all, the observation time per participant was relatively brief (15 minutes). Moreover, video recordings were performed only in one context of social interaction, they were coded by one observer who was not blind to the children's diagnoses, the participants received psychotropic medication, and there was no direct comparison with regard to predictive power between the ethogram and standard ratings. Nevertheless, the data presented here are sufficiently robust for an exploratory study.
We developed an ethogram covering a broad range of verbal and nonverbal behaviors of ASD and IDD, comprising earlier findings in classical ethological studies, and covering contemporary models of social behavior in mental disorders. Our ethogram not only precisely described the signs and symptoms of ASD, but also correctly classified ASD in most cases and clearly distinguished it from IDD, a developmental disorder that is common in childhood and adolescence. Furthermore, some subcategories of the ethogram that were related to gaze behavior, interpersonal distance, and avoidance behavior were able to differentiate children and adolescents with ASD and IDD who could not be categorized according to standard diagnostic checklists. A comparison between ASD and IDD on the behavioral elements of the ethogram revealed significant differences in: classic ASD behaviors, such as motor stereotypies (e.g., rock, hand-flapping), language stereotypies (e.g., echolalia), social interaction deficit (e.g., withdrawal, turn around), and gaze aversion (e.g., face away) (American Psychiatry Association, 2000; Kanner, 1943, 1971; World Health Organization, 1992); behaviors that are deficient in ASD according to established theoretical models, such as symbolic play, gaze following, pointing (i.e., joint attention), and use of mental-state language (Baron-Cohen, 1989, 1994; Baron-Cohen, Leslie, and Frith, 1985; Mundy, Sigman, and Kasari, 1990; Tager-Flusberg, 1981; Wing, Gould, Yeates, and Brierly, 1977); atypical behaviors that have also been described in ethological studies with ASD, such as gaze and physical aversion, echolalia, and motor stereotypies (Hutt and Ounsted, 1970; Pedersen, Livoir-Petersen, and Schelde, 1989; Pedersen and Schelde, 1997; Richer and Coss 1976; van Engeland et al., 1985); and in the nonspecific behaviors of ASD, such as walk, climb, explore, take, give, look own body, vocalization, and cry. Although children with ASD differed from IDD, it is not certain that the same would be true for contrasts between ASD and other mental disorders (e.g., childhood-onset schizophrenia), since the observed pattern of nonverbal behavior may not be specific to ASD. Future studies could use this ethogram to distinguish ASD from other mental disorders, to detect ASD in the general population, or even to study other behavioral conditions - analogous to previous ethological research with obsessive compulsive disorder (Eilam, Zor, Fineberg, and Hermesh, 2012; Zor et al., 2009; Zor, Szechtman, Hermesh, Fineberg, and Eilam, 2011).
The observation method of children and adolescents with ASD by means of discrete video recording devices and further analysis with an ethogram is minimally invasive, inexpensive, affordable, requires only a few minutes of video recording, and it is potentially more accurate than the typical clinical diagnostic procedures. Another advantage of this method in relation to standard ratings is that it does not depend on the parents' report, on the language development of the child or adolescent with the ASD, or on direct observation of behaviors, which are all methods that may suffer due to their lack of accuracy, especially in contexts where socioeconomic and sociocultural deprivation is common, such as in developing countries. On the other hand, the retrospective analysis of video recordings is time-consuming, may demand more training than just consulting DSM-5, may require multiple coders for behaviors that are difficult to identify (e.g., gaze following, mental state language), and perhaps may not be practical in clinical settings. Nevertheless, there are various computer programs that facilitate work with ethograms (e.g., the commercial “Observer” by Noldus, and the freeware “J-Watcher”). For research purposes, it may be an objective and very powerful tool for the detailed study of the social behaviors of autistic children and adolescents.
Footnotes
Acknowledgements
We would like to thank our patients and their families for their participation. We also thank Valerie Miller, MD, for constructive and valuable comments that helped improve an earlier version of the manuscript.
Ethogram

|
|
|
| Walk | Locomotion not directed to another person |
| Sit Down | Self-explanatory |
| Stand Up | Self-explanatory |
| Lie Down | Self-explanatory |
| Climb | The arms pull, and the legs push the body up. The child may also climb onto large chairs, tables, etc |
| Bow | To bend forward with the upper part of the body |
| Approach | The child walks toward a person (to be distinguished from accidental movements in the direction of a person) |
| Withdrawal | The child walks away from some person (to be distinguished from accidental movements away) |
| Turn Around | Turns whole body around its axis for at least 90° |
|
|
|
|
|
|
|
|
|
| Ask | Posing questions to somebody |
| Answer | Verbal reaction to a question from somebody |
| Echolalia | Repeating part of sentence spoken by somebody |
| Vocalization | Producing an unintelligible sound with mouth |
| Laugh | Self-explanatory |
| Cry | Self-explanatory |
| Scream | Self-explanatory |
| Mental State Language | Use of words such as “think”, “know”, “believe”, “wish”, “mean”, “pretend”, “forget”, “guess”, “want”, “believe”, “feel”, etc. (See Tager-Flusberg, 1981) |
| Talk | Using speech, loudly or quietly, other than as described |
|
|
|
|
|
|
|
|
|
| Smile (−) | The corners of the mouth are drawn back. The mouth is closed or slightly open. Does not establish eye contact |
| Smile (+) | The corners of the mouth are drawn back. The mouth is closed or slightly open. Establishes eye contact |
| Grimace | A sharp contortion of the face expressive of pain, contempt or disgust |
|
|
|
|
|
|
|
|
|
| Rock | Rhythmic up-and-down movements, either in a lateral or dorsal-ventral way |
| Flapping | Stereotyped hand-flapping |
| Jump | Abruptly raises body with or without feet leaving the floor. Does not include skipping, galloping or dancing |
| Tiptoe | The child walks on toes |
| Clap | Claps hands repetitively out-of-context |
| Finger | Moves fingers in a flicking motion, often near the head |
| Spin | Rotating the body around its own axis repetitively and out-of-context |
|
|
|
|
|
|
|
|
|
| Nod | Moves head up and down, once or several times, quickly or slowly |
| Shake | Rotates head from side to side, between once and several times |
| Tilt | Tilts head forward, backwards, or sideways |
| Face Away | Turns face away from the partner more than 90° |
| Head Spin | Rotates the head around its own axis repetitively and out of context |
|
|
|
|
|
|
|
|
|
| Stare Mother | Looks towards eyes of mother |
| Stare Psychiatrist | Looks towards eyes of psychiatrist |
| Stare Researcher | Looks towards eyes of researcher |
|
|
|
|
|
|
|
|
|
| Look Mother | Gaze directed to the mother's body |
| Look Psychiatrist | Gaze directed to the psychiatrist's body |
| Look Researcher | Gaze directed to the researcher's body |
| Look Body | Gaze directed to own body |
| Look Own Object | Looks at an object that is being manipulated by self |
| Look Other Object | Looks at an object that is being manipulated by another person |
| Look Away | Gaze directed away from the other person. This category includes looking at the wall, floor, door, table, window, and chair |
| Gaze Following | Follows the direction of gaze, head posture, or gestures of other people, and consequently shares a common social point of visual reference |
|
|
|
|
|
|
|
|
|
| Automanipulation | Manipulates own body, e.g. finger against teeth, picking nose or teeth, fumbling with fingers |
| Autoagression | Hurts own body, e.g., scratching skin, pulling the hair, biting hand, banging head against something |
| Heteroagression | Physically assaults another person, e.g., hair pulling, kicking, punching, biting, scratching |
| Point (−) | Indicates something discrete with fingers, hands or arm gestures. Does not establish eye contact |
| Point (+) | Indication of something discrete by mean of fingers, hand or arm gestures. Establishes eye contact |
| Show (−) | Shows objects. Does not establish eye contact |
| Show (+) | Shows objects. Establishes eye contact |
| Give (−) | Gives an object to another person. Does not establish eye contact |
| Give (+) | Gives an object to another person. Establishes eye contact |
| Take (−) | Picks up an object from another person. Does not establish eye contact |
| Take (+) | Picks up an object from another person. Establishes eye contact |
| Manipulate (−) | Extensive handling of objects in any way, exclusive of play. Does not establish eye contact |
| Manipulate (+) | Extensive handling of objects in any way, exclusive of play. Establishes eye contact |
| Play (−) | Handling objects, toys in a constructive or symbolic way. Does not establish eye contact |
| Play (+) | Handling objects, toys in a constructive or symbolic way. Establishes eye contact |
| Explore (−) | Explores the room without making eye contact, e.g., opens and closes the door and the window, pushes the wall, beats the floor with hands |
| Explore (+) | Explores the room while establishing eye contact, e.g., opens and closes the door and the window, pushes the wall, beats the floor with hands |
| Touch Mother | Touches the mother's body |
| Touch Psychiatrist | Touches the psychiatrist's body |
| Touch Researcher | Touches the researcher's body |
| Cover Eyes | Covers eyes with own hands |
| Cover Ears | Covers ears with own hands |
| Hide | Hides behind a chair, under the table, behind the gurney |
|
|
|
|
|
|
|
|
|
| Sit | Self-explanatory |
| Stand | Self-explanatory |
| Lying | Self-explanatory |
| Facing Mother | The child is facing the mother |
| Facing Psychiatrist | The child is facing the psychiatrist |
| Facing Researcher | The child is facing the researcher |
| Side Mother | The child is beside the mother |
| Side Psychiatrist | The child is beside the psychiatrist |
| Side Researcher | The child is beside the researcher |
| Backs Turned Mother | The child has his back to the mother |
| Backs Turned | The child has his back to the psychiatrist |
| Psychiatrist | |
| Backs Turned | The child has his back to the researcher |
| Researcher | |
|
|
|
|
|
|
|
|
|
| Near Mother | Distance between child and mother is between 0 and 0.5 meters |
| Near Psychiatrist | Distance between child and psychiatrist is between 0 and 0.5 meters |
| Near Researcher | Distance between child and researcher is between 0 and 0.5 meters |
| Medium Mother | Distance between child and mother is between 0.5 and 1.5 meters |
| Medium Psychiatrist | Distance between child and psychiatrist is between 0.5 and 1.5 meters |
| Medium Researcher | Distance between child and researcher is between 0.5 and 1.5 meters |
| Far Away Mother | Distance between child and mother is more than 1.5 meters |
| Far Away Psychiatrist | Distance between child and psychiatrist is more than 1.5 meters |
| Far Away Researcher | Distance between child and researcher is more than 1.5 meters |
Ethogram's scoring sheet for point events

| ALL OCCURRENCES (Intervals in minutes) | ||||||
|
|
0–1 | 3–4 | 6–7 | 9–10 | 12–13 | Total |
| Walk | ||||||
| Sit Down | ||||||
| Stand Up | ||||||
| Lie Down | ||||||
| Climb | ||||||
| Bow | ||||||
| Approach | ||||||
| Withdrawal | ||||||
| Turn Around | ||||||
| BODY POSTURES | - | - | - | - | - | |
| Ask | ||||||
| Answer | ||||||
| Echolalia | ||||||
| Vocalization | ||||||
| Laugh | ||||||
| Cry | ||||||
| Scream | ||||||
| MS Language | ||||||
| Talk | ||||||
| VERBALIZATIONS | - | - | - | - | - | |
| Smile (−) | ||||||
| Smile (+) | ||||||
| Grimace | ||||||
|
FACIAL
|
- | - | - | - | - | |
| Rock | ||||||
| Flapping | ||||||
| Jump | ||||||
| Tiptoe | ||||||
| Clap | ||||||
| Finger | ||||||
| Spin | ||||||
|
MOTOR
|
- | - | - | - | - | |
| Nod | ||||||
| Shake | ||||||
| Tilt | ||||||
| Face Away | ||||||
| Head Spin | ||||||
| HEAD POSTURES | - | - | - | - | - | |
| Stare Parents | ||||||
| Stare Psychiatrist | ||||||
| Stare Researcher | ||||||
| STARE | ||||||
| Look Parents | ||||||
| Look Psychiatrist | ||||||
| Look Researcher | ||||||
| Look Body | ||||||
| Look Own Object | ||||||
| Look Other Object | ||||||
| Look Away | ||||||
| Gaze Following | ||||||
| LOOK | - | - | - | - | - | |
| Automanipulation | ||||||
| Autoagression | ||||||
| Heteroagression | ||||||
| Point (−) | ||||||
| Point (+) | ||||||
| Show (−) | ||||||
| Show (+) | ||||||
| Give (−) | ||||||
| Give (+) | ||||||
| Take (−) | ||||||
| Take (+) | ||||||
| Manipulate (−) | ||||||
| Manipulate (+) | ||||||
| Play (−) | ||||||
| Play (+) | ||||||
| Explore (−) | ||||||
| Explore (+) | ||||||
| Touch Parents | ||||||
| Touch Psychiatrist | ||||||
| Touch Researcher | ||||||
| Cover Eyes | ||||||
| Cover Ears | ||||||
| Hide | ||||||
| GESTURES | - | - | - | - | - | |
Ethogram's scoring sheet for lasting-event categories

| SCAN SAMPLING (Intervals in minutes) | ||||||||||||||||
|
|
1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | Total |
| Sit | ||||||||||||||||
| Stand | ||||||||||||||||
| Lying | ||||||||||||||||
| Facing Mother | ||||||||||||||||
| Facing Psychiatrist | ||||||||||||||||
| Facing Researcher | ||||||||||||||||
| Side Mother | ||||||||||||||||
| Side Psychiatrist | ||||||||||||||||
| Side Researcher | ||||||||||||||||
| Backs Turned Mother | ||||||||||||||||
| Backs Turned |
||||||||||||||||
| Backs Turned Researcher | ||||||||||||||||
| CURRENT STATUS | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Near Mother | ||||||||||||||||
| Near Psychiatrist | ||||||||||||||||
| Near Researcher | ||||||||||||||||
| Medium Mother | ||||||||||||||||
| Medium Psychiatrist | ||||||||||||||||
| Medium Researcher | ||||||||||||||||
| Far Away Mother | ||||||||||||||||
| Far Away Psychiatrist | ||||||||||||||||
| Far Away Researcher | ||||||||||||||||
|
INTERPERSONAL
|
- | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |