
Abstract
Simon Baron-Cohen pioneered the idea that different brain types evolved to process information in gender specific ways. Here we expand this approach to looking at eating disorders as a byproduct of the extreme female brain. The incidence of eating disorders is higher among females, and recent findings show that hormones may play a role in eating disorders. We present new evidence from four studies that both an empathizing bias and hyper-mentalizing (as measures of the extreme female brain; EFB) are related to disordered eating and negative evaluation anxiety in women. We also advance the novel hypothesis that concerns about animal welfare (a unique expression of the EFB) may account for the relationship between vegetarianism and eating disorders.
Introduction
Baron-Cohen (2002) proposed an inclusive theory of individual differences in cognitive style by creating a taxonomy of brain types based on the distinction between empathizing and systemizing. This theory, derived from observed sex differences in cognition, also provides a plausible account of the proximate and evolutionary mechanisms driving sex differences in psychopathology. The central argument is that males and females have evolved different brain-types each specialized to process information in different ways (Baron-Cohen, 2003). This may explain the female advantage on cognitive tasks that involve language and the male advantage on spatial tasks, in terms of broader cognitive styles that were selected because they provided a fitness advantage.
Systemizing is the drive to analyze and explore systems to discover their underlying governing principles (Baron-Cohen, 2002). Systems can be explained by ‘if-then’ correlational rules and can be deconstructed in terms of input and output. More males than females use a systemizing cognitive style (Baron-Cohen, 2002; 2003).
Empathizing, on the other hand, is the drive to identify someone else's emotional state and to respond appropriately (Baron-Cohen, 2002). Gallup (1998) has argued that empathizing relies upon self-awareness (i.e., awareness of one's own mental state), the ability to infer the mental states of others (i.e., theory of mind), and the ability to produce an appropriate emotional response to mental states in other people (i.e., empathy). More females than males use an empathic cognitive style and because effective communication relies upon making correct inferences, superior empathizing skills may explain the advantaged communication and language abilities of females (Baron-Cohen, 2002, 2003).
In the right situation, systemizing and empathizing are both adaptive responses to the complex social and physical environments that characterize human existence. But because selective pressures operated on males and females differently, females developed greater empathizing skills and males developed better systemizing skills. The different adaptive problems facing males (e.g., hunting, tracking, making weapons) and females (e.g., caring for offspring, recruiting and reciprocating help from others) have led to the sexual differentiation of the human brain.
Testosterone, Autism and the Extreme Male Brain
Autism spectrum disorders represent a class of neurodevelopmental disorders characterized by deficits in communication and language, social development, and the presence of self-stimulatory behaviors (APA, 2000). Research suggests certain features associated with autism spectrum conditions may provide a model of the extreme male brain (Baron-Cohen, 2002). The first line of evidence is that four times as many males are affected by autism than females (Fombonne, 2003; Wing, 1981). This sexual asymmetry in the prevalence of autism spectrum conditions (ASCs) stands out in even greater relief when looking at Asperger's syndrome, which shares two out of the three features of autism (social communication deficits and self-stimulatory behaviors, without accompanying language or intellectual deficits; APA, 2000). In Asperger's syndrome, the sex ratio is 10:1 male to female (Wing, 1981). These findings are consistent with a putative role for the sex hormone testosterone, produced in higher levels in males than in females.
Retrospective studies of amniocenteses in the first trimester of pregnancy show that testosterone levels are significantly elevated in the amniotic fluid of women whose offspring develop autistic characteristics (Baron-Cohen, Lutchmaya and Knickmeyer 2004). Amniotic fluid testosterone levels are negatively related to eye-contact in boys at 12 months of age, vocabulary development in 18- and 24-month olds, and the quality of social relationships and range of interests in 4 year olds (Baron-Cohen et al., 2004; Knickmeyer, Baron-Cohen, Raggatt and Taylor, 2005).
There is also evidence that 2D:4D ratios, a somatic marker negatively correlated with prenatal testosterone exposure, are lower in males than females and even lower among individuals with autism (Baker, 1888; Manning, Scutt, Wilson and Lewis-Jones, 1998). In addition, this ratio is negatively correlated with symptom severity (Manning, Baron-Cohen, Wheelright and Sanders, 2001). In a study of 95 families with autistic children, children with autism (and their parents and siblings) had lower 2D:4D ratios than controls, suggesting that families with lower digit ratios may be at higher risk for autism. In addition, children with the greatest language impairments had the lowest 2D:4D ratios (Manning et al., 2001).
Being a female with autism does not offer protection against the other side effects of heightened testosterone exposure. In fact, the rates of androgen-related medical problems, including polycystic ovary syndrome, irregular menstrual periods, excessive body hair, and severe acne are higher among females with ASC's (Ingudomnukul, Baron-Cohen, Wheelright and Knickmeyer, 2007). Females with autism spectrum conditions also experience a delayed onset of menarche compared to controls (Knickmeyer, Baron-Cohen, Hoekstra and Wheelright, 2006).
Collectively, these findings yield consistent, albeit indirect evidence supporting a model of elevated testosterone levels during prenatal development in autism which may persist across the lifespan. In addition to being associated with heightened levels of testosterone, the extreme male brain theory of autism rests on the idea that systemizing and empathizing are normally distributed, and that a small percentage of individuals will occupy the upper and lower ends of both these distributions. These individuals may manifest the pathological extremes of sexually differentiated brain-types. In support of this theory, people with autism have superior systemizing skills (Baron-Cohen et al., 2003) with deficits in empathizing and other aspects of social communication including language and theory of mind (Baron-Cohen, 2002, 2003).
Testosterone-Disordered Eating and the Extreme Female Brain
Baron-Cohen (2003) also proposed the existence of an ‘extreme female brain,’ but did not specify the form it would take. Indeed, he hypothesized that it might not be maladaptive at all. But given the far-reaching effects of autism and the specific patterns of neuropathology associated with it, this seems unlikely. At the very least, the EFB would have to affect more females than males, be sensitive to the organizational and activational effects of sex steroids, and be associated with superior empathizing at the expense of systemizing.
Eating disorders, including anorexia and bulimia, are characterized by aberrant patterns of eating behavior, a preoccupation with weight, an intense fear of becoming fat or gaining weight, and a disturbance in the way one's body weight or shape is perceived (APA, 2000). Arguably, there may be more similarities than differences between anorexia and bulimia. For instance, 20% of anorexics display bulimic behavior such as recurrent episodes of binge eating and compensatory behaviors in order to prevent weight gain, including self-induced vomiting, misuse of laxatives and/or excessive exercise. There is also growing evidence to suggest that disordered eating exists on a continuum, much like the autism spectrum (Södersten, Bergh and Zandian, 2006).
The sex ratio in the prevalence of eating disorders is highly skewed. Women are ten times more likely to experience eating disorders than males (APA, 2000). Similar to ASC's they are also considered chronic conditions because more than fifty percent of patients receiving treatment relapse within a year, and even after ten years less than fifty percent of patients fully recover. Mortality rates among people with anorexia are twelve times higher than all other causes of death among females aged 15–24, making it one of the most lethal forms of mental illness (Sullivan, 1995).
There is increasing evidence that hormones may play an important role in the development and maintenance of eating disorders (Klump, Gobrogge, Perkins, Thorne, Sisk and Breedlove, 2006). In addition to the female bias in the prevalence of eating disorders, eating disorder symptoms typically appear at puberty and tend to remit later in life when hormone levels decline (Strober, Freeman and Morrell, 1997). Early puberty is a risk factor for eating disorders in both men and women (Zehr, Culbert, Sisk and Klump, 2007) and salivary estradiol is positively correlated with disordered eating during the follicular phase of the menstrual cycle (Klump et al., 2006). Furthermore, in animal studies estrogen is negatively related to food intake and positively related to activity levels (Eckel, 2004).
Whereas heightened serum levels of testosterone have been implicated in autism, several recent studies have shown that prenatal testosterone exposure protects against the development of disordered eating later in life. Klump et al. (2006) examined 2D:4D ratios as a function of disordered eating and found that lower levels of prenatal testosterone exposure were associated with higher levels of disordered eating. In the same study, circulating estrogen levels were positively correlated with disordered eating. Quinton, Smith and Joiner (2011) investigated 2D:4D ratios in females with eating disorders and found significant differences between those diagnosed with anorexia and bulimia. Participants with anorexia displayed a “low masculinized” digit ratio, whereas participants with bulimia displayed a “high feminized” digit ratio, with non-clinical controls falling between the two. In addition, among women with eating disorders, 2D:4D was associated with participants' current and lowest weight. Consistent with previous research, a study from the same lab showed that 2D:4D ratios in males were positively correlated with disordered eating (Smith, Hawkeswood and Joiner, 2010).
A unique way to assess the relationship between fetal testosterone and disordered eating is to look at twins. Because twins share the same prenatal environment, females with a male co-twin are exposed to higher levels of prenatal androgens, including testosterone. Culbert and colleagues (2008) found that the risk of disordered eating was higher among females who shared a female co-twin than among females who shared a male co-twin. Conversely, another study showed that the risk of developing anorexia was highest for males who shared a female co-twin (Procopio and Marriott, 2007). Thus, the idea that prenatal testosterone has a protective effect against the development of eating disorders may be overly simplistic. Instead, it may be a combination of protective androgens and pathogenic estrogens that result in a sex-specific hormonal profile that increases susceptibility to eating disorders later in life (Procopio and Marriott, 2007). Clearly, the links between prenatal testosterone exposure, autism and eating disorders warrant further investigation, particularly in light of Baron-Cohen's extreme male brain theory of autism and the absence of a plausible EFB counterpart.
Demands of Group Living and Brain Type
The increasing complexity of our social lives is another adaptive problem faced by humans over the course of evolution. It is likely that as social interaction among humans became more complex there was considerable variation in proficiency in social domains. Thus, if sociability was represented on a continuum, the lower end of the distribution could be anchored by social apathy (a characteristic of autism), whereas the high end could be represented in the form of social anxiety (a common co-occurrence in eating disorders).
The prevalence of anxiety disorders, including social phobia, is high among individuals with eating disorders and not surprisingly is more prevalent in women than men (Turk et al., 1998). A study looking at co-morbidity of anxiety disorders in anorexia and bulimia found that two thirds of those who met the criteria for eating disorders reported experiencing an anxiety disorder, with twenty percent reporting the experience of social phobia. In most cases, the anxiety disorders preceded the development of eating disorders and co-morbidity of anxiety served as a risk factor contributing to a less favorable outcome (Kaye et. al., 2004; Steinhausen, 2002).
Negative evaluation anxiety is a specific form of social anxiety that involves intolerance toward disparaging or hostile judgment by others toward the self (Watson and Friend, 1969). This form of social anxiety is not only more prevalent among women; the content and experience of women's social anxieties also differ from men. Women report greater fear while talking to authority figures, working while being observed, entering a room while others are already seated, and expressing disagreement or disapproval to people they do not know well (Turk et al., 1998). Collectively these findings suggest a more general fear of negative evaluation by others. In addition, negative evaluation anxiety is positively associated with disordered eating (Gilbert and Meyer, 2005). The sex differences observed in the prevalence of negative evaluation anxiety and its relationship to disordered eating suggests that there may be affective mechanisms, such as the experience of anxiety, in addition to the cognitive biases that differentiate male and female brain types.
In this paper we present a series of four studies investigating the hypothesis that disordered eating and negative evaluation anxiety provide a candidate model for the EFB.
Materials and Methods
The methods used in the series of studies that follow were approved by local Institutional Review Boards and conformed to guidelines for the ethical treatment of human subjects. All participants gave informed consent. Participants volunteered or received course credit in exchange for their participation. Due to the anonymous nature of this study, participants with high levels of disordered eating could not be identified for referral to appropriate medical professionals, so a packet of local resources for treatment and support for those with concerns about eating disorders was made available to all participants.
Measures
Eating Attitudes Test. The Eating Attitudes Test (EAT) is the most widely used standardized measure of the characteristics associated with eating disorders (Garfinkel and Newman, 2001). The 40-item full version of the EAT was developed to identify people with severe eating disorders. The EAT-26, developed by Garner, Olmstead, Bohr and Garfinkel (1982), is the short form of the original test. It consists of 26 items taken from the full version. The EAT-26 distinguishes between three factors of disordered eating including dieting, bulimia and food preoccupation, and oral control. It has strong psychometric properties including good test-retest reliability (r = .84; Carter and Moss, 1984) and criterion validity (Koslowsky et al., 1992).
Fear of Negative Evaluation Scale. The Fear of Negative Evaluation Scale (FNE) is a self-report measure of social-evaluative anxiety developed by Watson and Friend (1969). Participants respond to 30 true or false statements. It was designed to assess apprehension and distress over negative evaluations by others, the avoidance of evaluative social situations, and the expectation that others would evaluate one negatively. The FNE is correlated with other measures of social anxiety including the State-Trait Anxiety Inventory (STAI; Spielberger, Gorsuch and Lushene, 1971) and is associated with eating disorder pathology, specifically the drive for thinness and level of body dissatisfaction. (Turner, McCanna and Beidel, 1987; Gilbert and Meyer, 2005) The brief form includes 12 questions and correlates highly (.96) with the original scale items (Leary, 1983).
The Empathizing Quotient. The Empathizing Quotient (EQ) is a forced-choice, self-administered questionnaire created by Baron Cohen and Wheelright (2004), designed to assess empathy. Structurally, it is comprised of 60 items, with 40 items assessing empathy and 20 filler items. Responses are given on a four-point scale depending on how strongly participants agree or disagree with statements related to empathy, and scoring direction is counterbalanced. Females score significantly higher than males on this instrument and it can be used to identify individuals with Asperger's syndrome. Scores on the EQ range from 0–80. The instrument has high internal consistency with a Cronbach's alpha of .852 and is considered a valid measure of empathy components (Muncer and Ling, 2006). Empathizing appears to be mostly, but not completely independent of systemizing (Wheelwright et al., 2006).
The Systemizing Quotient. The Systemizing Quotient Revised (SQ-R) is a 75-item forced choice, self-administered questionnaire that measures individual differences in systemizing by assessing a person's interest in a broad range of systems (Wheelwright et al., 2006; see Baron-Cohen, Richler, Bisarya, Gurunathan and Wheelright, 2002 for original version). Responses are given on a four-point scale depending on how strongly participants agree or disagree with statements related to systemizing. Half the items are reverse coded, to reduce response bias. Males score higher than females on the SQ-R, but these sex differences disappear among individuals with autism spectrum conditions. The finding that physical scientists score higher than biological or social scientists on this measure supports the ecological validity of this measure. Within the general population, the relationship between SQ-R scores and EQ scores is weak, suggesting that most individuals possess a balanced brain type, where there is only a slight tradeoff between dimensions of empathizing and systemizing (Wheelwright et al., 2006).
Reading the Mind in the Eyes Test. The Reading the Mind in the Eyes Test (RME; Baron-Cohen, Wheelright, Hill, Raste and Plumb, 2001) tests participants' accuracy in the attribution of relevant mental states. Participants are presented with 36 partial face photographs, showing only the eye region of different actors and actresses. The participant is asked to choose which mental state (one target embedded within 3 foils with the same emotional valence) best describes what the actor in the photograph is feeling or thinking. This test measures how well the participant can infer the mental state of another person, which is a cognitive component of empathy (Muncer and Ling, 2006). We used a modified version of this test in which the photographs were presented on a computer screen instead of paper. Participants were provided with a glossary of all the mental state terms used in the test, and encouraged to consult these when necessary. Normative data on the RME suggests a slight, but non-significant female advantage on the task and is inversely correlated with scores on the autism spectrum quotient (Baron-Cohen et al., 2001).
Intuitive Physics Test. The Intuitive Physics Test (Baron-Cohen, Wheelright, Spong, Scahill and Lawson, 2001) is based on the philosopher Daniel Dennett's claim that humans have an intuitive understanding of physics from infancy onwards and use this knowledge to understand the causal forces that act on inanimate objects (Dennett, 1987). The test is a 20-item, multiple-choice task that involves visual problem solving related to the perception of physical causality. It is a test of intuitive physics because all problems on the test can be solved from everyday, real-world experience and are not problems that were taught as part of the curriculum in any of the schools where the test was piloted (Baron-Cohen, et al., 2001).
Schizotypal Personality Questionnaire. The Schizotypal Personality Questionnaire (SPQ) is a 72 item, forced-choice self-report scale of schizotypal personality characteristics (Raine, 1991). It provides an overall measure of individual differences in schizotypal characteristics and includes subscales for all nine schizotypal traits identified in the DSM-III-R criteria for schizotypal personality disorder.
Redrawn Vandenburg and Kuse Mental Rotations Test (Version-A). The Redrawn Vandenburg and Kuse Mental Rotations Test Version A (MRT-A) is a 24-item test that involves mental rotation around a vertical axis. Participants have to choose which two out of four rotated figures accurately represent a target. This significantly reduces the probability of success when a participant uses guessing as a strategy and increases the validity of the measure. Sizable sex differences on this task may reflect underlying differences in systemizing abilities. Gender accounts for a significant proportion of variance in performance on this test and task performance is positively correlated with other measures of visuospatial ability (Hegarty and Waller, 2004; Peters et al., 1995).
Study 1
Using self-report measures of disordered eating, negative evaluation anxiety and measures of cognitive style (systemizing and empathizing), the first study investigated the hypothesis that individuals with high levels of disordered eating and negative evaluation anxiety may represent a model of the EFB by showing a cognitive advantage in empathizing and disadvantage in systemizing.
Materials and Methods
Participants
One hundred and twenty-two undergraduate students (52 males; 70 females) at the State University of New York at Albany were recruited from psychology courses. Participants' were aged between 18 and 30 (Mean age = 19.4; SD = 1.9) and all were fluent in English.
Measures
Participants filled out the following self-report measures: EAT-26, FNE, EQ and SQ-R, as well as a brief demographic survey in a group setting. Participants were instructed to sit at least one seat apart from each other in a classroom setting.
Results
Data from each participant were entered into a spreadsheet and analyzed using SPSS/PAWS version 18.0. An exploratory analysis revealed that the distribution of scores were normal for every variable except disordered eating. The distribution for scores on the EAT-26 was positively skewed (Kolmogorov-Smirnov Z = 2.006, p = .001). In order to correct for skew, this was corrected by computing the natural logarithmic transformation for this variable [ln(EAT+1)], which resulted in a distribution that did not differ significantly from normality (Kolmogorov-Smirnov Z = .813, p = .523). Consistent with Watson and Friend (1969), the distribution of scores on the FNE was rectangular, therefore a Spearman rank order correlation was used to analyze the relationships between these variables. In addition to examining associations between disordered eating, negative evaluation anxiety and participant raw scores on the EQ and SQ-R, a composite variable identified as Empathizing Bias was created for each participant by obtaining the z-scores of EQ and SQ-R variables, and subtracting the participants' SQ-R z-score from the EQ z-score (z-EQ – z-SQ-R = empathizing bias). Empathizing bias reflects the tendency to utilize a cognitive style that favors empathizing over systemizing and its use has been supported in other studies examining possible candidates for the EFB (Brosnan, Ashwin, Walker and Donahue, 2010). One outlier scoring more than 4 standard deviations away from the mean (X = −.0413, SD = 1.1) was removed from the subsequent analyses. Sex differences on all variables were examined using multiple t-tests and the alpha level was adjusted accordingly using a Bonferroni correction (.05/6 = .008). As some participants did not complete all portions of the questionnaire battery, any missing values were excluded pairwise.
Mean values for each variable are displayed in Table 1. Consistent with the EFB theory, levels of disordered eating, negative evaluation anxiety, empathizing and empathizing bias were significantly higher among females. Mean scores and sex differences are reported in Table 2. Table 3 depicts the correlations among these variables. There was a significant positive correlation between disordered eating and negative evaluation anxiety (r = .329, p ≤ .001) and the bulimia subscale of the EAT-26 and negative evaluation anxiety (r = .310, p ≤ .001), which is consistent with a substantial body of previous research demonstrating comorbidity between eating disorders and social anxiety (Kaye, Bulik, Thorton, Barbarich and Masters, 2004). There was also a significant positive correlation between disordered eating and scores on the EQ (r = .272, p ≤ .001), but not the SQ-R. A similar relationship was discovered for negative evaluation anxiety. Participants' responses on the FNE were positively associated with empathizing and negatively associated with systemizing, albeit not significantly. However, both disordered eating and negative evaluation anxiety were positively correlated with an empathizing bias (r = .173, p ≤ .05 and r = .157, p ≤ .05, respectively).
Descriptive statistics for disordered eating, negative evaluation anxiety, and cognitive style.

Note. EAT-26=Eating Attitudes Test; FNE=Fear of Negative Evaluation; EQ=Empathizing Quotient; SQ-R=Systemizing Quotient-Revised; EB=Empathizing Bias
Sex differences in levels of disordered eating, negative evaluation anxiety and cognitive style.

Note. EAT-26 = Eating Attitudes Test; FNE = Fear of Negative Evaluation; EQ= Empathizing Quotient; SQ-R = Systemizing Quotient-Revised; EB= Empathizing Bias
p ≤ .05; reflecting significant sex differences
Spearmans rhoa and Pearson correlations between disordered eating, negative evaluation anxiety and cognitive style.

Note. EAT-26=Eating Attitudes Test; FNE=Fear of Negative Evaluation; EQ=Empathizing Quotient; SQ-R=Systemizing Quotient-Revised; EB=Empathizing Bias
p ≤ .05
p ≤ .001
Discussion
In the present study females who scored significantly higher on measures of disordered eating also scored higher on measures of negative evaluation anxiety, empathizing, and empathizing bias. Males only outperformed females on measures of systemizing. These results are consistent with previous research examining sex differences in cognitive styles.
Among male and female participants, disordered eating and negative evaluation anxiety were significantly correlated with a cognitive style that favors empathizing over systemizing, providing preliminary evidence that the EFB phenotype displays both high levels of disordered eating and negative evaluation anxiety. In addition, disordered eating accounted for a small, but significant proportion of the variance in empathizing scores.
Study 2
The purpose of Study 2 was to replicate the findings from Study 1, using objective measures of systemizing and empathizing, and to investigate whether patterns of disordered eating are affected differently in males and females.
Methods and Materials
Participants
One hundred and sixty undergraduate students (74 males; 86 females) at the State University of New York at Albany were recruited from psychology courses. Participants' age ranged from 18–30 years (Mean Age = 19.5; SD = 1.9) and all were fluent in English.
Measures
Participants completed the EAT-26, FNE, EQ and Systemizing SQ-R and a brief demographic survey in a group setting. Each participant completed a modified paper and pencil version of the Reading the Mind in the Eyes Test (RME; glossary provided) and the paper and pencil version of the Intuitive Physics Test. Participants were instructed to sit at least one seat apart from each other in a classroom setting.
Results
Data from each participant were entered into a spreadsheet and analyzed using SPSS/PAWS version 18.0. An exploratory data analysis revealed that the distribution for scores were normal for every variable with the exception of EAT-26 scores which were significantly positively skewed (Kolmogorov-Smirnov Z(EAT) = 2.499 p ≤ .001). This was corrected by transforming EAT-26 scores into their natural logarithm (Kolmogorov-Smirnov Z(nlEAT+1) = 1.03, p = .239). In the following analyses, Pearson product correlations were computed to analyze relationships between variables for the entire sample. Significant relationships were further explored using regression analyses and scatterplots. Sex differences on all variables were examined using multiple t-tests and the alpha level was adjusted accordingly using a Bonferroni correction (.05/8 = .006). General linear model (GLM) univariate analysis of variance procedures were used to explore the differential effects of disordered eating upon gender.
Mean scores and sex differences are reported in Table 4. Table 5 depicts the correlations among these variables. The significant positive correlation between disordered eating and negative evaluation anxiety was replicated (r = .379, p ≤ .001). Disordered eating was significantly correlated with scores on the empathy quotient (r = .275, p ≤ .001), but not the systemizing quotient (r = .115, p = .073). For the total sample, performance on the Reading the Mind in the Eyes Test and performance on the Intuitive Physics test was not significantly related to disordered eating. Scores on the empathizing quotient were positively correlated with performance on the Reading the Mind in Eyes Test (r = .179, p ≤ .05), and surprisingly, the Systemizing Quotient-Revised (r = .292, p ≤ .001).
Descriptive statistics for Study 2: Measures of disordered eating, social anxiety and cognitive style.

Note. EAT-26=Eating Attitudes Test; FNE =Fear of Negative Evaluation; INPH=Intuitive Physics Test; EYES=Reading the Mind in the Eyes test; EQ=Empathizing Quotient; SQ-R=Systemizing Quotient-Revised; EB=Empathizing Bias
p ≤ .05
p ≤ .001
Pearson correlations between disordered eating, negative evaluation anxiety and cognitive style in males and females.
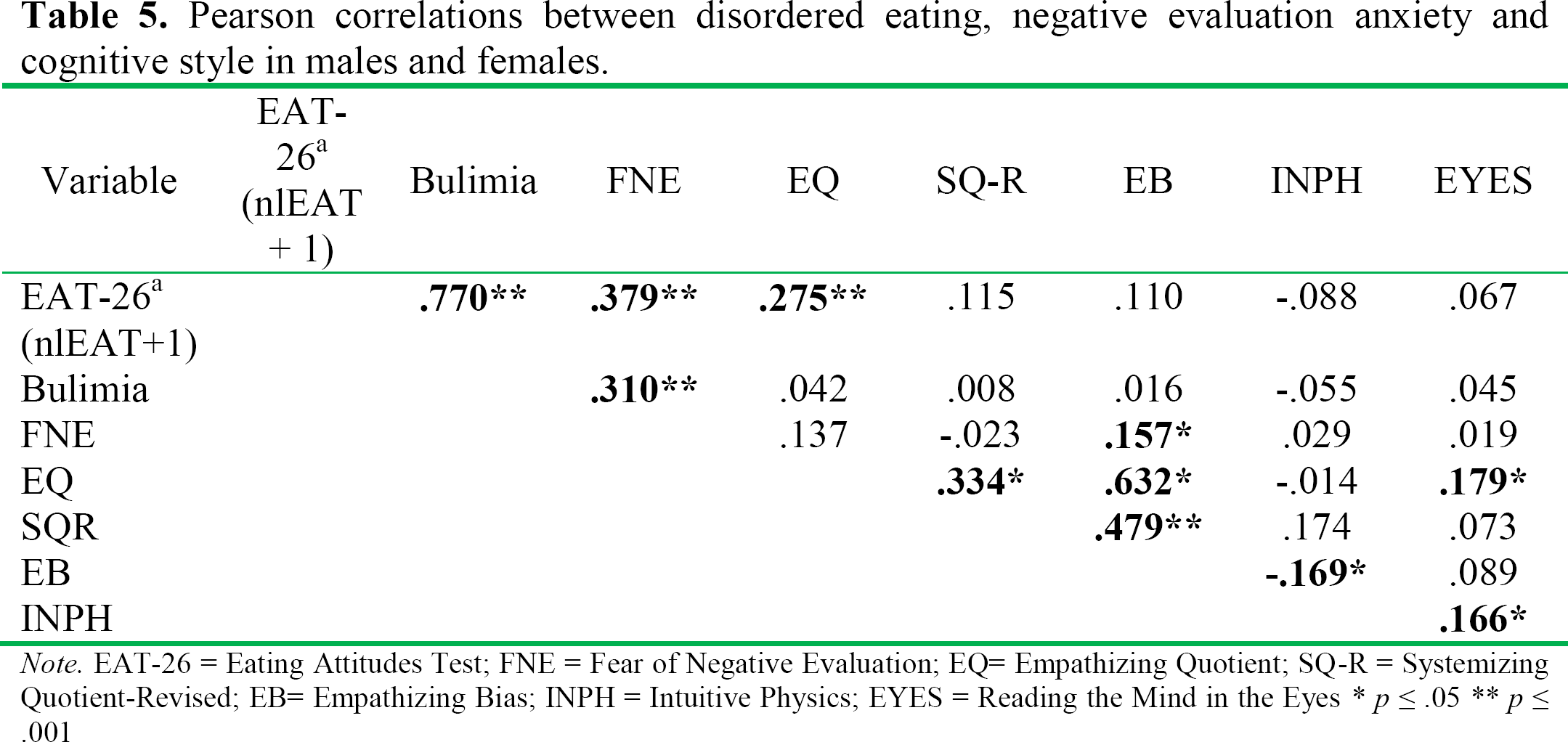
Note. EAT-26 = Eating Attitudes Test; FNE = Fear of Negative Evaluation; EQ= Empathizing Quotient; SQ-R = Systemizing Quotient-Revised; EB= Empathizing Bias; INPH = Intuitive Physics; EYES = Reading the Mind in the Eyes
p ≤ .05
p ≤ .001
GLM procedures were utilized to further investigate the relationship between disordered eating, gender and measures of empathizing. Gender and level of disordered eating were entered as fixed factors with performance on the Reading the Mind in the Eyes Test entered as the dependent variable with high and low scores determined by scoring at least one standard deviation above the mean for each gender. A two-way analysis of variance revealed a significant interaction between gender and level of disordered eating (F = 9.86, p ≤ .01). A similar result was obtained when empathizing quotient scores were entered as the dependent variable (F = 5.513, p ≤ .05) revealing that the effects of disordered eating on both objective and self-reported measures of empathizing depended upon gender (see Figures 1 and 2).

Interaction between gender, disordered eating and theory of mind.

Interaction between gender disordered eating and empathizing.
Discussion
The previously reported association between disordered eating and empathizing was replicated in the second study. Here, empathizing was significantly correlated with negative evaluation anxiety, although we did not observe a significant relationship between systemizing and disordered eating or negative evaluation anxiety. A possible explanation for the absence of a systemizing deficit is because the items on the Intuitive Physics Test are taken from everyday experience, and, therefore may not be as sensitive to individual variation in systemizing ability. However, this would not explain why performance on the SQ-R was correlated with empathizing scores. Future research should investigate performance on other plausible systemizing tasks as a function of disordered eating.
There was a significant interaction between gender, disordered eating and theory of mind. Females with high levels of disordered eating performed better on the Reading the Mind in the Eyes test, whereas males with high levels of disordered eating performed worse. There was also a significant interaction between disordered eating, gender, and empathizing. In females, levels of disordered eating were not related to empathizing scores, but males with high levels of disordered eating displayed greater empathizing. The data from males are consistent with the idea that disordered eating is associated with the hyper-empathizing that characterizes the EFB type. As previously stated, the capacity to empathize relies on the ability to make inferences about mental states in others, but at the extreme of the empathizing/systemizing continuum, these mental state attributions do not necessarily have to be accurate. It is possible that the hyper-mentalizing associated with the EFB may manifest as faulty inferences about mental states, include paranoia or suspiciousness, or even manifest as beliefs in telepathy or other types of magic. Interestingly, these characteristics are typically associated with psychosis or schizophrenia. This observation has lead Bronsan, Aschwin, Walker and Donahue (2010) to suggest a model of the EFB that is characterized by psychosis. An issue with this hypothesis is that rates of schizophrenia affect males and females equally, although females display higher rates of certain schizotypal characteristics, including ideas of reference, suspiciousness, and odd beliefs and magical thinking (Gur, Petty, Turetsky and Gur, 1996; Raine, 1991). Therefore, psychosis, in and of itself, may not completely capture the EFB type. However, an examination of schizotypal characteristics in the context of disordered eating and negative evaluation anxiety may provide a more complete picture of the EFB counterpart.
Study 3
A striking characteristic of eating disorders is the aberrant patterns of thoughts and related distortions in one's body image, which appear to parallel the hyper-mentalizing that has been associated with schizotypal personality characteristics. Therefore, the goal of the third study was to examine schizotypal personality characteristics as a function of disordered eating and negative evaluation anxiety as candidates for the EFB. According to our hypothesis, the EFB profile ought to be associated with symptoms of schizotypy, such as ideas of reference, suspiciousness, and odd beliefs or magical thinking.
Materials and Methods
Participants
Forty-two undergraduate students (20 males; 22 females) at the State University of New York at Albany were recruited from psychology courses. Participants' age ranged from 18–22 (Mean age = 19.2; SD = 1.2) and all participants were fluent in English.
Measures
Participants filled out the following self-report measures independently: EAT-26, FNE, Empathizing Quotient (EQ) and the Schizotypal Personality Questionnaire (SPQ).
Results
Data from each participant were entered into a spreadsheet and analyzed using SPSS/PAWS version 18.0. An exploratory analysis revealed that the distribution for scores were normal for every variable with the exception of the bulimia subscale of the EAT-26 which was positively skewed for males only (Kolmogorov-Smirnov Z(bulimia) = 1.514, p ≤ .05). Therefore a Spearman rank order correlation was used for this variable in the following analyses. For all other analyses, Pearson product correlations were used. Significant correlations were investigated further using regression analyses and scatterplots.
Mean scores are reported in Table 6. Table 7 depicts the correlations among these variables. Negative evaluation anxiety was significantly correlated with total SPQ scores (r = .388, p ≤ .01; see Figure 3). In addition, negative evaluation anxiety was correlated with disordered eating (r = .280, p ≤ .05) and five of the nine SPQ subscales including: Ideas of Reference, Social Anxiety, Odd Beliefs and Magical Thinking, Constricted Affect, and Suspiciousness.
Descriptive statistics for Study 3: Disordered eating, negative evaluation anxiety and schizotypal personality characteristics.

Note:
n = 42 EAT-26=Eating Attitudes Test; FNE=Fear of Negative Evaluation; EQ=Empathizing Quotient; SPQ-Total=Total scores on the Schizotypal Personality Questionnaire
Study 3: Significant correlations between disordered eating, social anxiety, and schizotypal personality characteristics.

Note: EAT-26=Eating Attitudes Test; FNE=Fear of Negative Evaluation; EQ=Empathizing Quotient; SPQ-Total=Total scores on the Schizotypal Personality Questionnaire
p ≤ .05
p ≤ .01

Positive correlation between negative evaluation anxiety and schizotypy.
Disordered eating was positively correlated with three of the nine subscales including: Ideas of Reference, Odd beliefs and Magical Thinking, and Suspiciousness. In addition, there was a significant positive correlation between scores on the bulimia subscale and schizotypal traits including Ideas of reference (r = .280 p ≤ .05) and Suspiciousness (r = .391, p ≤ .01). Moreover, the correlation between empathizing scores and disordered eating obtained in the first two studies was replicated (r = .321, p ≤ .05). There was also a significant positive correlation between the bulimic subscale and the empathizing quotient (r = .258 p ≤ .05, respectively). In males, but not females, there was a significant negative correlation between scores on the EAT-26 and Constricted Affect (r = −.455, p ≤ .05).
Schizotypal personality traits were not correlated with empathizing. In fact, the only subscale of the SPQ significantly correlated with empathizing was constricted affect (r = −.286, p ≤ .05).
Discussion
Schizotypy was significantly associated with negative evaluation anxiety and disordered eating. Total SPQ scores and five of the nine subscales were associated with negative evaluation anxiety. Three SPQ subscales were significantly associated with disordered eating: ideas of reference, suspiciousness and odd beliefs and magical thinking. Ideas of reference involve mistaken attributions that causal incidents and external events have direct reference to oneself (APA, 2000). The tendency to over-attribute relevance to external events, specifically the thoughts or beliefs of another person, may represent a type of hyper-mentalizing associated with the EFB.
Suspiciousness is the belief that one is being persecuted or treated unfairly (APA, 2000). The nature of the relationship between suspiciousness, disordered eating, and negative evaluation may represent another example of mental state attribution in which neutral social interactions are misinterpreted. In addition, the tendency to infer that one is being targeted or treated unfairly may closely approximate negative evaluation fears.
The final subscale that was associated with both disordered eating and negative evaluation anxiety was the odd beliefs and magical thinking subscale, which measures how odd beliefs (e.g., belief in telepathy) and magical thinking influence behavior. Since telepathy relates to the ability to “read” another person's mind, this belief may be a prime example of the hyper-mentalizing expected to be associated with the EFB.
For males, disordered eating was negatively related to constricted affect. Constricted affect is characterized by blunted emotional reactivity. Consistent with our predictions about disordered eating and the EFB, males with higher levels of disorder eating were more emotionally reactive than males with lower levels of disordered eating. There are gender differences in emotional reactivity that show females are more reactive than males (Muncer and Ling, 2006). Greater emotional reactivity may also be a significant component of empathy. Garnering the appropriate emotional response to other people's experiences hinges upon being able to relate to or identify with what another person is feeling. This is also supported in the present study by the finding that constricted affect was the only schizotypy variable that correlated significantly with empathizing. Thus, the fact that males responded in a more characteristically feminine way as a function of disordered eating provides further evidence of the relationship between disordered eating and negative evaluation anxiety as potential candidates for the EFB.
Study 4
The purpose of the last study was to replicate the results observed between hyper-mentalizing as indexed by schizotypal characteristics, disordered eating and negative evaluation anxiety, and to further investigate the relationship of these variables to systemizing using an objective measure of spatial reasoning as an alternative to the Intuitive Physics Test and self-report measures of systemizing.
Materials and Methods
Participants
Thirty-seven undergraduate students (16 males and 21 females) were recruited from classes at Alfred State College and Alfred University. Participants' age ranged from 19–53 years (Mean age = 23.1; SD = 7.8) and all were fluent in English.
Measures
Participants completed the EAT-26, the FNE-brief, the SPQ and the MRT-A in small groups.
Results
Data from each participant were entered into a spreadsheet and analyzed using SPSS/PAWS version 18.0. An exploratory data analysis revealed that the distribution for scores were normal for every variable. The significant correlations between negative evaluation anxiety, schizotypal characteristics, and disordered eating were replicated. Significant correlations were investigated further using regression analyses and scatterplots.
Negative evaluation anxiety was correlated with total SPQ scores (r = .412, p ≤ .01). In addition, negative evaluation anxiety was correlated with disordered eating (r = .601, p ≤ .001) and five of the nine SPQ subscales including: Ideas of Reference, Social Anxiety, Odd Beliefs and Magical Thinking, Constricted Affect, and Suspiciousness.
Mean scores are reported in Tables 8 and Table 9 depicts the correlations among these variables. Disordered eating was positively correlated with total scores on the SPQ (r = .514, p ≤ .001; see Figure 4) and four of the nine subscales including: Ideas of Reference, Odd beliefs and Magical Thinking, Perceptual Disturbances, and Suspiciousness.
Descriptive statistics for Study 4: Disordered eating, negative evaluation anxiety and schizotypal personality characteristics.
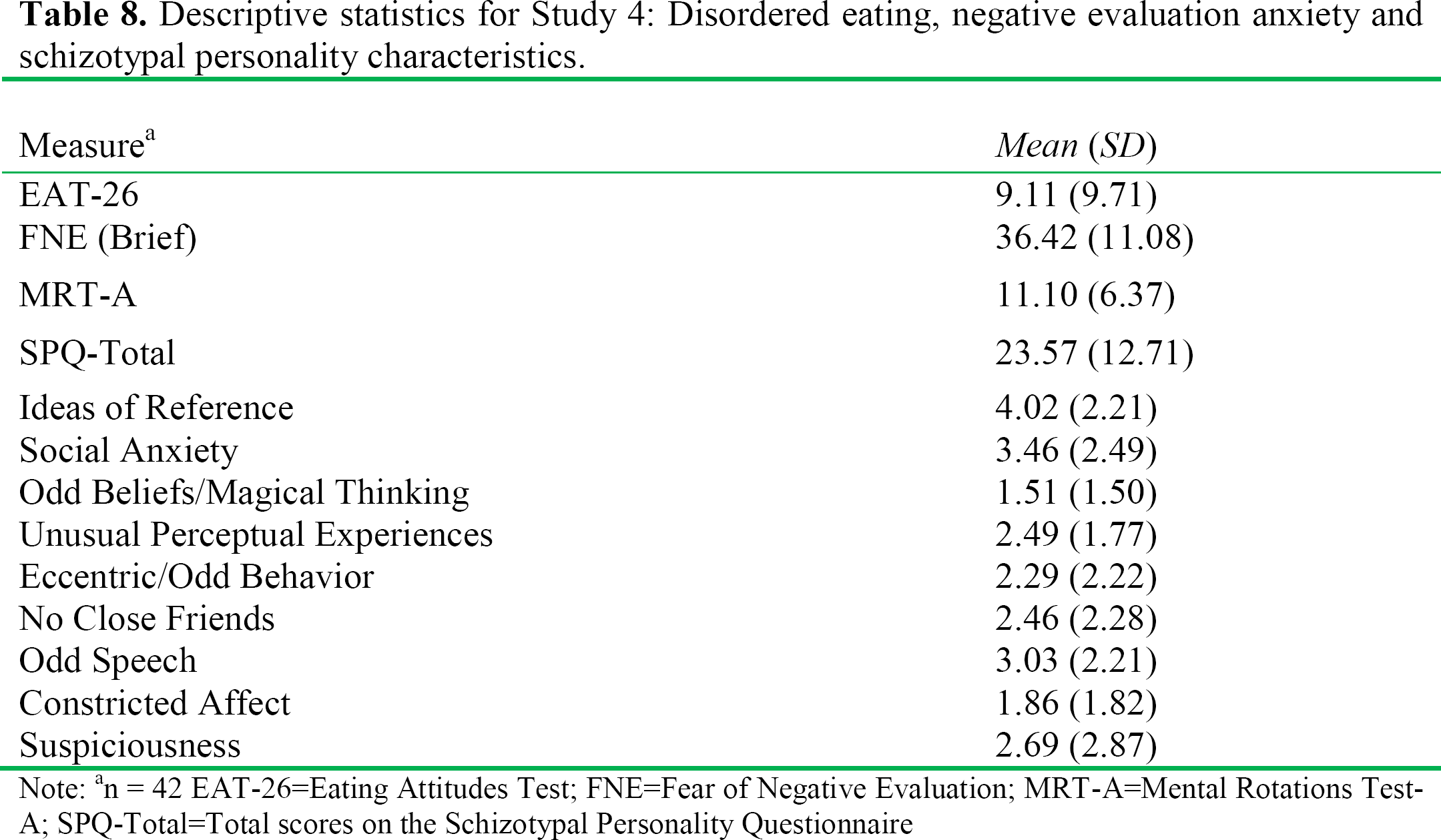
Note:
n = 42 EAT-26=Eating Attitudes Test; FNE=Fear of Negative Evaluation; MRT-A=Mental Rotations Test-A; SPQ-Total=Total scores on the Schizotypal Personality Questionnaire
Study 4: Significant correlations between disordered eating, social anxiety, and schizotypal personality characteristics and performance on the mental rotations test.

Note: EAT-26=Eating Attitudes Test; FNE=Fear of Negative Evaluation; SPQ-Total=Total scores on the Schizotypal Personality Questionnaire
p ≤ .05
p ≤ .01

Positive correlation between disordered eating and schizotypy.
Consistent with a deficit in systematizing ability, there was a significant negative correlation between scores on the EAT-26 and the Mental Rotations Test-A (r = −.313, p ≤ .032), but not negative evaluation anxiety (r = .121, p > .05).
Discussion
The previously reported association between hyper-mentalizing, as measured by positive schizotypal personality characteristics, and disordered eating and negative evaluation anxiety was replicated. In addition, performance on the mental rotation test was negatively correlated with disordered eating, suggesting a deficit in systemizing abilities as scores on the EAT-26 increase. One of the most widely documented sex differences in cognition is found on tests that measure spatial reasoning skills. These tests require good systemizing because they involve the application of correlational rules that govern the movement of an object around a vertical access. In order to successfully perform these tasks, a person has to utilize the “if-then” correlational rules that govern the movement of objects around a vertical axis in three-dimensional space and mentally represent these different perspectives. In a sample that included both male and female participants, we showed that excessive mentalizing and impaired systemizing were associated with disordered eating.
General Discussion
Evidence from all four studies converge to show that a combination of disordered eating and negative evaluation anxiety are associated with a cognitive style that Baron-Cohen (2002) predicted for the EFB. Social anxiety, particularly negative evaluation anxiety, appears to represent a salient feature of the EFB. The intense fear of becoming fat, a defining feature of eating disorders, may not be the fear of fat itself, but a fear that arises from the potential to be evaluated disparagingly by others. Disordered eating may be a predominant way in which negative evaluation fears manifest.
An interesting consequence of eating disorders is the profound decrease in levels of estrogen (Sharp and Freeman, 1993). The changes in estrogen levels are responsible for amenorrhea, a defining characteristic in anorexic women. A significant drop in estrogen levels may also produce changes in empathizing and theory of mind performance.
Comparable to the heightened sensitivity to sensory stimuli (auditory, visual and tactile) common among people with autism, individuals with the EFB may be hypersensitive to social stimuli. Disordered eating may ameliorate the experience of negative evaluation anxiety that results from heightened sensitivity to social stimulation.
Consistent with this idea, emotional processing deficits have been linked with eating disorders including the inability to recognize, label and describe emotions in detail and to link feelings with bodily correlates (Bourke, Taylor, Parker and Bagby, 1992; Eizaguirre, de Cabezon, de Alda, Olariaga and Juaniz, 2004; Garner, Olmsted and Polivy, 1983). Also, compared to healthy controls, women with anorexia had difficulty recognizing emotions from facial expressions and vocal tones (Jansch, Harmer and Cooper, 2009; Kucharska-Pietura, Masiak, and Treasure, 2003).
Jones, Harmer, Cowen and Cooper (2008) investigated emotional face processing in female undergraduates with high and low levels of disordered eating. Participants completed the Eating Attitudes Test-26 and the Facial Expression Recognition Task, a computer task in which participants view faces depicting 7 different expressions (anger, disgust, fear, happiness, sadness, surprise, and neutral) at different intensities. The participants with higher levels of disordered eating were less accurate in identifying happy and neutral faces. Among participants with high-levels of disordered eating, there was a tendency to classify more happy faces as neutral, and more neutral faces as either angry or sad. In addition, there was evidence that reaction times to recognize disgust were longer, while reaction times to recognize fear were faster than participants with low-levels of disordered eating. When disordered eating reaches clinical levels, the effects of hyper-mentalizing may manifest as mental state misattributions. This may be because they are using their own experience to model the experience of others, and their bias to classify emotions with a negative bias may influence their attributions. For instance, when shown pictures of women who are said to have overeaten, females with high levels of disordered eating ascribed more negative emotional states to these women than control participants do. Thus, women with higher levels of disordered eating appeared to use their own experience of overeating to describe how the other women would feel (Beebe, Holmbeck Schober, Lane, Rosa, 1996).
It is also possible that the physiological and cognitive effects of starvation produce deficits in performance. In a study looking at performance on the Reading the Mind in the Eyes Test, individuals with anorexia performed worse compared to healthy controls (Russell, Schmidt, Doherty, Young and Tchanturia, 2009).
An alternative interpretation is that is low scores on the Reading the Mind in the Eyes task does not represent a deficit in theory of mind ability, but rather an excess that reflects hyper-mentalizing. Abu-Akel (2003) suggests that theory of mind dysfunctions range from the complete absence of the ability to represent other people's mental states (as shown in severe autism) to having the representational understanding of mental states, but a deficit in the ability to apply this understanding (as in Asperger's syndrome) to the abnormal or excessive attribution of mental states (represented by schizotypy). It may be that this third class of dysfunction is misconstrued as a deficit, rather than an excess. Consistent with this interpretation, the RME is one of the most widely used instruments to investigate theory of mind performance in adults; however, scores on the RME depend only on accuracy. The test does not identify the nature of the errors that impede performance. For example, there can be errors of absence (failing to detect a mental state when it is present) and errors of excess (wrongly inferring a mental state in its absence). We suspect the second class of errors (errors of excess) account for most of the lower scores on this test among individuals with anorexia.
Another area for future research is the role of self-awareness in theory of mind and psychopathology. Most models of theory of mind and empathizing view self-awareness as a closely related construct because we use our own experience to model the experiences of others. There is evidence that individuals with eating disorders and autism spectrum conditions show deficits in self-awareness. For example, mirror self-recognition, a proxy for self-awareness, is often developmentally delayed or absent among people with autism (Dawson and McKissick, 1984; Spiker and Ricks, 1984). Similarly, a study of individuals with anorexia found that self-awareness may be suppressed in patients with eating disorders. Sachdev, Mondraty, Wen and Gulliford (2009) used fMRI to examine how self-image and non-self images are processed in individuals with anorexia and healthy controls. They found that processing of non-self images was similar in both groups, but compared to healthy controls, who showed activation in the insula and prefrontal cortex, processing of self-images in the anorexic group led to no activation of these brain regions. The almost complete absence of activation to self-images suggests that cognitive, emotional, and perceptual processing may be suppressed in patients with anorexia and that this may contribute to the body image distortion that characterizes this disorder.
In addition, Heatherton and Baumeister (1991) proposed that binge eating could be motivated by the desire to escape self-awareness. They argue that individuals who engage in binge eating are acutely sensitive to the demands of others and set extremely high expectations for themselves. When they fail to meet their own expectations, they develop a pattern of high self-awareness, concern over how they appear to others and emotional distress. Binge eating and the loss of inhibition associated with it may provide temporary relief from self-awareness.
Theory of mind dysfunction does not preclude eating disorders from representing the EFB. Rather, it warrants closer examination of the source of the dysfunction. In autism spectrum conditions, theory of mind deficits may be driven by an aberrant pattern of brain development that is rooted in excess early testosterone exposure. The theory of mind dysfunction observed in eating disorders may reflect the absence of testosterone which alters development during critical periods later in life (i.e., puberty). Further examination of the role of self-awareness and theory of mind as a function of disordered eating may elucidate the neurocognitive and developmental mechanisms involved. The results of the present studies provide evidence that supports disordered eating and negative evaluation anxiety as a candidate model of the EFB, and incorporating the knowledge of empathizing/systemizing distinctions may help guide the development of effective interventions for disorders that fall on the extremes of these variables.
As shown in Study 1 and replicated in Studies 2, and 3 it is important to reiterate that as scores on the empathizing quotient increase, levels of disordered eating also rise. People with greater empathizing skills would be expected to be more sensitive to the pain and suffering of others. An interesting interpretation of these data involves the disproportionate rates of vegetarianism among individuals with eating disorders. For example, numerous studies have found a positive association between vegetarianism and eating disorders (e.g., Bas, Karabudak and Kiziltan, 2005; Robinson-O'Brien, Perry, Wall, Story, Neumark-Sztainer, 2009; Yackobovitch-Gavan et al., 2009). Most investigators interpret this relationship as evidence confirming health-conscious, restrictive eating patterns among people with eating disorders. However, an alternative hypothesis consistent with the data presented here is that individual differences in empathizing may affect dietary choices as a consequence of heightened concerns about animal cruelty and animal welfare. Rather than being used as a method to reduce caloric intake, vegetarianism may actually be a by-product of the greater empathizing capacities among individuals with EFBs. A study by Yackobovitch–Gavan et al. (2009) showed that vegetarianism is not only associated with disordered eating, but it can be thought of as a pre-morbid condition that affects the course and outcome of anorexia. In their study, vegetarianism reduced the probability of symptom remission by a factor of over 12 times. If vegetarianism is viewed as an expression of greater empathizing capacities, the corollary hypothesis would be that heightened levels of empathizing may function as a prelude to eating disorders, as well as an important risk factor for its development. Future research should explore empathizing and mental state attributions as variables that may influence both the onset and outcome of eating disorders.
Footnotes
Acknowledgements
Authors thank Steven Platek, Jeremy Atkinson, Nate Pipitone, Melvin Phillip, Iara Mantenuto and Debra Tomm for their assistance and comments.