
Abstract
Substantial evidence indicates that depression focuses attention on the problems that caused the episode, so much that it interferes with the ability to focus on other things. We hypothesized that depression evolved as a response to important, complex problems that could only be solved, if they could be solved at all, with an attentional state that was highly focused for sustained periods. Under this hypothesis, depression promotes analysis and problem-solving by focusing attention on the problem and reducing distractibility. This predicts that attentionally demanding problems will elicit depressed affect in subjects. We also propose two control-process mechanisms by which depression could focus attention and reduce distractibility. Under these mechanisms, depression exerts a force on attention like that of a spring when it is pulled or like a magnet on a steel ball. These mechanisms make different predictions about how depressed people respond emotionally to a task that pulls attention away from their problems. We tested these predictions in a sample of 115 undergraduate students. Consistent with our main prediction, initially non-depressed subjects experienced an increase in their depressed affect when exposed to an attentionally demanding task. Moreover, the overall pattern of results supported the magnet metaphor.
Keywords
Introduction
Organisms face multiple adaptive challenges, many of them simultaneously, and they must have adaptations that allocate attention and cognitive resources to them. Negative emotions are thought to have evolved, at least in part, for this purpose (Alexander, 1986; Barlow, 2002; Buss, 2000; Ohman, Flykt, and Esteves, 2001; Thornhill and Thornhill, 1989). Specifically, the effect of negative emotions on attention is thought to be analogous to the influence of physical pain on attention. Physical pain draws attention to problems that are causing, or threatening to cause, physical damage to the body, such as the pain that one feels when one inadvertently puts one's hand on a hot surface (Eccleston and Crombez, 1999; Wall, 2000). Similarly, negative emotions are thought to have evolved to draw attention to important problems in the environment (often of a social nature) that had an important impact on fitness and could be fixed or ameliorated with attention (Alexander, 1986; Thornhill and Thornhill, 1989).
Control-process views of emotion suggest that they are related to progress or frustration in finding solutions to problems or meeting goals (Carver, Lawrence, and Scheier, 1996; Carver and Scheier, 1990). Negative emotions are elicited when one has not found a solution to a problem or one is not making satisfactory progress towards a goal, and the emotion draws attention to the task of finding a solution. Conversely, positive emotions are elicited when one has found a solution or is making satisfactory progress towards a goal, and the emotion keeps attention focused on the adaptive course. For instance, courtship is emotionally painful when unrequited, and attention is directed to solving the problem of successfully wooing the desired partner. However, positive emotion is elicited when the partner responds positively to the courtship, and attention and behavior stays focused on the same course, at least until progress towards the mating goal becomes unsatisfactory. Thus, the valence of emotion reflects whether or not progress towards a goal or a solution is being frustrated (Carver et al., 1996; Carver and Scheier, 1990).
There are many different negative emotions—e.g., anger, anxiety, disgust, fear, jealousy—and they presumably evolved to influence attention in different ways. In this paper, we focus on the attentional function of depression or depressed affect, which is an emotion characterized by negative affect and low arousal.
Although clinical depression is often assumed to be qualitatively different than subclinical forms, explicit tests of this assumption have found that depressed affect is better characterized by a single dimension that varies continuously in intensity and duration (Aggen, Neale, and Kendler, 2005; Krueger and Markon, 2006). For instance, depressive symptoms vary continuously in epidemiological samples (Hankin, Fraley, Lahey, and Waldman, 2005), and the degree of psychosocial impairment covaries linearly with the number of depressive symptoms (Kessler, Zhao, Blazer, and Swartz, 1997; Sakashita, Slade, and Andrews, 2007). We therefore use the terms depressed affect and depression to refer to a single continuum that varies from transient sadness to chronic, severe, clinical depression.
There is abundant evidence that depression influences attention. People with clinical or subclinical depression tend to report persistent ruminations about important problems in their lives (Lyubomirsky, Tucker, Caldwell, and Berg, 1999). Indeed, people with greater levels of depression tend to ruminate more and are less easily distracted from their ruminations (Just and Alloy, 1997; Lam, Smith, Checkley, Rijsdijk, and Sham, 2003; Nolen-Hoeksema and Morrow, 1991; Schmaling, Dimidjian, Katon, and Sullivan, 2002). Attention is a limited resource (Kahneman, 1973), with one implication being that as attention becomes more focused on one problem, fewer cognitive resources are available for other problems. Further evidence of depression's influence on attention thus comes from the fact that depressives' ruminations interfere with their ability to concentrate on other things. For instance, when people come into a psychological testing situation with clinical or subclinical depression, their ruminations interfere with their ability to focus on cognitive tasks and reduce their performance (Lyubomirsky, Kasri, and Zehm, 2003; Watkins and Brown, 2002; Watkins and Teasdale, 2001; Watkins, Teasdale, and Williams, 2000). Such research suggests that depression focuses attention on the problems that caused the episode, so much so that it interferes with people's ability to focus on other things. Put another way, one of depression's effects is to focus attention and reduce distractibility.
Depressives' focused attentional state can affect how they process information. Research on pre-existing and experimentally induced mood indicates that depressed affect promotes an analytical processing style (Ambady and Gray, 2002; Au, Chan, Wang, and Vertinsky, 2003; Bless, Bohner, Schwarz, and Strack, 1990; Bless, Mackie, and Schwarz, 1992; Braverman, 2005; Edwards and Weary, 1993; Forgas, 1998; Gasper, 2004; Gasper and Clore, 2002; Hertel, Neuhof, Theuer, and Kerr, 2000; Schwarz and Bless, 1991; Semmler and Brewer, 2002; Sinclair, 1988; Sinclair and Mark, 1995; Storbeck and Clore, 2005; Yost and Weary, 1996). Analytical reasoning involves dividing a complex problem into smaller, more manageable components, where each is studied in turn. To arrive at the solution to the whole, the solution to each component must be maintained in memory while processing on the next component takes place. Analytical reasoning therefore requires the use of working memory, which holds information in a highly active state because it is crucial to ongoing processing (Baddeley, 1996).
The Raven's Advanced Progressive Matrices (RAPM) is considered one of the best measures of nonverbal analytical reasoning ability (Carroll, 1993). Each item is a spatial pattern completion task in which one of eight choices correctly completes a two-dimensional visual array, and test items become progressively more difficult. The difficulty of test items increases, in part, because the number of elements in the array increases and the rules for how they vary across the array can be different for each element (Carpenter, Just, and Shell, 1990). The rule for each element must be ascertained independently, so once subjects figure out the rule for how one element varies across the array, they must keep the solution in their working memory while they figure out the rules for the remaining elements. The number of elements that must be analyzed and held in working memory varies from 1 to 5, and the proportion of people getting a test item correct is negatively related to the number of elements that must be analyzed (Carpenter et al., 1990).
Current research indicates that analytical tasks with high working memory loads, such as the RAPM, are attentionally demanding because they leave little room for attention to wander (Kane and Engle, 2002). For instance, performance on the RAPM is highly correlated with the ability to resist distractions under attentionally demanding conditions, and the relationship is mediated by differential activity in areas of the brain known to be involved in attentional control (Gray, Chabris, and Braver, 2003).
In summary, depressed affect focuses attention on problems, and it promotes an analytical processing style. Because analytical reasoning requires focused attention, it seems reasonable to hypothesize that depressed affect may promote an analytical processing style by its attention-focusing effects.
We suggest that depressed affect evolved as a response to important, analytically challenging problems that could only be solved, if they could be solved at all, with an attentional state that was highly focused for a sustained period of time (Watson and Andrews, 2002). Under this hypothesis, depressed affect promotes analysis and problem-solving by focusing attention on the problem and reducing distractibility.
If depressed affect is a response to analytically challenging problems, then a task such as the RAPM should be able to induce depressed affect in people with low levels of depression. Established methods for inducing depressed mood involve having subjects listen to sad music or watch sad movies, giving them negative feedback about their performance on tasks, having them apply self-referent statements to themselves (e.g., “I feel a little down today”, “I wish I could be myself, but nobody likes me when I am”) (Seibert and Ellis, 1991), and so on (Westermann, Spies, Stahl, and Hesse, 1996). There is also substantial evidence that stressful life events can induce depression (Kendler, Karkowski, and Prescott, 1999). While cognitively effortful tasks are often used in methods that rely on negative feedback, the feedback is almost always fixed (i.e., even people who perform well on the task are given negative feedback) (Westermann et al., 1996). Moreover, it is failure itself, and not the nature of the task, that is assumed to elicit depressed affect. Our prediction that an analytically and attentionally challenging task can induce depressed affect, and not failure per se, is, to our knowledge, novel and untested.
There are two potential control-process mechanisms by which depressed affect could focus attention and reduce distractibility. First, depressed affect may keep attention focused on a problem in a way that is similar to the force exerted by a spring. In this analogy, the problem could be thought of as being attached to one end of the spring and attention to the other end. When the spring is compressed and relaxed, attention is focused on the problem, and the force exerted by the spring is minimized. When the spring is pulled, attention is pulled away from the problem, and the spring's force increases. If depression's mode of action is like the force exerted by a spring, then depressed affect should increase as attention is pulled from a focal problem, which would tend to draw attention back to the problem. Validation of the spring metaphor would suggest that, at the time of measurement, depressed affect is a marker of the degree to which attention is diverted from the problem that elicited the episode.
Alternatively, depression's influence on attention could be more like the attractive force on a steel ball produced by a magnet. In this analogy, the “magnet” is a difficult problem (e.g., marital troubles). The attractive force that the problem generates is depressed affect, and it draws attention to the problem just as the magnetic force draws a steel ball to the magnet. Since the magnetic force is greatest when the steel ball is closest to the magnet, depressed affect should be greatest when attention is fully focused on the problem, where it tends to keep attention focused. When attention is diverted to some other problem, depressed affect will decrease, just as the attractive force on the steel ball lessens as it is pulled from the magnet. Validation of the magnet metaphor would therefore suggest that, at the time of measurement, depressed affect is a marker of the degree to which attention is focused and distractibility is reduced.
We stress that the terms magnet and spring are merely metaphors to describe the possible ways depressed affect could exert force on attention. However, we use them because they help describe the different mechanisms of action that we are hypothesizing.
According to the hypothesis, depressed affect is a response to analytically and attentionally demanding problems that may take a long time to solve. Consequently, the organism might occasionally need to interrupt processing to deal with pressing issues that require immediate attention (e.g., predators, important social problems). After the issue has been dealt with, attention must return to the core problem that caused the depressive episode. Since attention must be pulled from the core problem to be focused on the pressing issue, processing the pressing problem would be very difficult with a spring-like mechanism because a great deal of force must be expended to keep attention focused there. However, under a magnet-like mechanism, once attention was pulled away from the core problem and focused on the pressing problem, less force would be needed to keep it there. Thus, a magnet-like mechanism would be better from an engineering perspective.
To test between these two mechanisms, we measured subjects' level of depressed affect twice. The first assessment (T1) was a baseline measure to assess the level of depression that they brought with them into the laboratory. Since depressed affect is continuously distributed in populations, people come into a psychological testing situation with varying levels of depressed affect unless pre-screening takes place. The causes of their depressive symptoms are assumed to reflect important pre-existing life issues, and we refer to this as their pre-existing depression.
Subjects completed the second assessment (T2) of depressed affect after they had been given intervention—in this case, practice questions from the RAPM. The hypothesis that depressed affect arises in response to an analytically and attentionally challenging problem predicts that subjects with low levels of pre-existing depression should experience an increase after exposure to the intervention. We were concerned that after the subjects had completed the attentionally demanding intervention, their attention would immediately relax and we would be unable to detect the emotional effect we were looking for when they took the T2 measure. So we devised the intervention's effect to be prolonged.
The intervention was also designed to get subjects with high levels of pre-existing depression to pull their attention away from their pre-existing problems. The spring and magnet mechanisms make different predictions about how they will respond emotionally to the intervention. According to the spring metaphor, this is like pulling a spring, and depressed affect should increase. Under the magnet metaphor, however, the intervention is like pulling a steel ball away from a magnet. This should cause the level of depressed affect to decrease just as the magnetic force exerted on the ball decreases.
Materials and Methods
Participants
The 115 participants were University of New Mexico students recruited from psychology courses and participated in exchange for extra credit. The intervention group had 65 participants (68% females, SD=.47, average age=21.9, SD=4.4), whereas the control group had 50 participants (88% females, SD=.33, average age=25.4, SD=10.2). One person in the control group did not provide information about their sex or age.
Instruments
Scale for assessing depressed affect. Since our two mood-state measures were to be completed within a few minutes of each other, we were concerned that subjects might remember their T1 answers when filling out the scales at T2. Moreover, we wanted to be able to detect subtle changes in affect. No existing instruments were adequate for these purposes.
To accomplish these goals, we constructed two parallel instruments (forms A and B) from a pool of 26 adjectives designed to assess state depression. The pool was composed of 16 negative and 10 positive affect adjectives, with each adjective having one synonym (i.e., there were 13 sets of synonyms). From each paired synonym set, one adjective was assigned to each scale so that there were 13 adjectives on each form (e.g., “sad” was on form A and “blue” was the form B synonym). Each adjective was rated on a 9-point Likert scale according to how one was feeling right then (1=extremely inaccurate as a self-description, 9=extremely accurate as a self-description). The construction of two different instruments that were roughly equivalent allowed us to reduce memory effects, and the use of multiple adjectives that were rated on Likert scales (as opposed to checklists) allowed us to detect subtle changes in affect.
To test for equivalence, we tested the factor structure of the forms on the control group. All subjects took both forms, counterbalanced for order. We used Mx (Neale, Boker, Xie, and Maes, 2003) to perform a series of latent variable analyses using structural equation modeling (SEM). In SEM, variables are connected by a series of arrows that represent the presumed direction of causation. The likelihood is the probability of obtaining the observed data under the assumptions of the model (e.g., a multivariate normal distribution), and it is influenced by the unknown parameters in the model (e.g., the regression coefficients of the variables connected by arrows). Mx searches through the parameter space for the regression coefficients that maximize the likelihood. The fit of the model is −2 times the natural logarithm of the likelihood (−2LL). For our latent variable models, the latent measure of state depression is assumed to influence the observed measure for each adjective, and Mx uses the variance that the observed measures share in common to estimate the regression coefficients to the latent factor. To our knowledge, this is the first attempt to use maximum likelihood estimation techniques to test the equivalence of two instruments for assessing affective states.
With maximum likelihood, significance testing is done by calculating the difference in the fits between nested models, −2ΔLL, which is asymptotically distributed as chi-square. (One model is “nested” inside another if the parameters to be estimated in the former are a subset of the parameters of the latter.) A common significance test is to compare the fit between a model and a submodel in which a parameter is dropped from the structural equation path or constrained in its value. For instance, in a latent factor model in which two parameters are constrained to have equal loadings onto the latent factor, an insignificant increase in fit is evidence that the parameters do not have significantly different loadings.
We first tested whether the 26 items were better described by one or two latent factors. The two-factor model fit significantly better (negative affect items loaded high on the first factor and positive affect items loaded high on the second factor), -2ΔLL=374.44, Δdf=27, p<.0001. We retained all the negative affect items from the first factor because they appeared to be more closely related to depressed affect (e.g., sad, cheerless, somber, lonely). This reduced the forms from 13 items each to eight each. Then, we conducted eight tests (one for each synonym pair), in which we tested whether the items in the pair had significantly different loadings on the latent factor. Based on these tests, we deleted two more pairs. The remaining six synonym pairs passed a strict test of factorial invariance in which each item and its synonym were simultaneously constrained to load equally onto the latent factor, -2ΔLL=10.76, Δdf =6, p=n.s. (see Table 1).
The forms for assessing depressed affect.

Items with the same number were synonyms that had equivalent factor loadings in the control group. Items with an asterisk (*) were eliminated from the analyses because the intervention influenced their loadings onto the latent measure (see text).
We also gave subjects in both groups the Beck Depression Inventory, which is a commonly used instrument for assessing depressed affect over the past two weeks (Beck, Ward, Mendelson, Mock, and Erbaugh, 1961). It is not state-like enough for our purposes, and so we only used it to validate our constructed scales.
Raven's Advanced Progressive Matrices. We gave subjects in the intervention group questions from the RAPM, which was described above. The full RAPM is considered one of the best measures of nonverbal analytical reasoning ability and fluid intelligence with an internal consistency reliability of about 0.90 and a validity of about 0.80 in measuring general intelligence (Carroll, 1993; Raven, Court, and Raven, 1994). The 12-item short form correlates 0.90 with the full 36-item RAPM (Arthur and Day, 1994).
Procedure
The protocols were completed in classroom settings. For the control protocol, each participant first read the instructions for either form A or form B (counterbalanced for order) for the T1 assessment of affect and then completed it. After completing the first form, they then read the instructions for the T2 assessment of affect and then completed it. Consequently, the time between the two measures was short. Subjects were also given the BDI and answered a short background questionnaire. After completing the protocol, the subjects were debriefed and thanked.
A key difference in the intervention protocol is that there was an intervention between the T1 and T2 measures of affect (Figure 1). At T1, subjects were also given the BDI, after which they were given the intervention. We were concerned that after the subjects had completed the attentionally demanding intervention, their attention would immediately relax and we would be unable to detect the emotional effect we were looking for when they took the T2 measure. So we devised an intervention that was intended to promote a prolonged focusing effect. Specifically, participants read that they were about to take a test, which involved questions that got progressively more difficult. They also read that they would first be given some practice questions to familiarize them with the rules of the test and give them some idea of the difficulty they would encounter in the test. Subjects were then given five practice questions taken from the remaining 24 questions from the RAPM that were not used in the short form. One easy question was given to familiarize participants with the rules of the test, and the other four had high working memory loads to help them understand the difficult nature of the test they would be taking. After they had answered each practice question, participants were given the correct answer and told to analyze the question until they had satisfied themselves that they knew why it was the correct answer. This feature was deemed necessary because, without knowing the correct answer, subjects might not have understood that the questions were difficult. The use of analytically challenging questions for the intervention should have helped subjects focus their attention, and the fact that they were practice questions should have helped subjects remain in the focused state so that they were psychologically and emotionally prepared for taking the test. Thus, the intervention was designed to prolong the focusing effect so we could measure affect after subjects had completed the intervention. After the intervention, participants completed the T2 assessment of affect. Then, subjects completed the short-form of the RAPM, which was administered under a 15-minute time limit. Finally, subjects filled out a short background questionnaire, and then were debriefed and thanked.

Time-line for the intervention group.
Results
The latent depressed affect constructs
The intervention could have influenced the measurement properties of the state depression constructs. We ran a series of models in which we compared the fully saturated model to one in which a particular synonym pair was constrained to have equal loadings across forms and times. Doing this for each of the six pairs, we found that one pair (miserable-awful) had a significantly worse fit across the two times, -2ΔLL=18.973, Δdf=3, p<0.0005, so we deleted it from our constructs. The remaining five pairs passed a test of factorial invariance in which each item and its synonym was simultaneously constrained to load equally onto the latent factor across T1 and T2, -2ΔLL=13.049, Δdf=15, p=n.s.
From the remaining adjectives, we used Mx to estimate factor scores for the latent T1 and T2 measures of state depression and then imported them into SAS. Both variables exhibited good spread, had roughly bell-shaped distributions and passed Shapiro-Wilk tests of normality. We therefore had no evidence that our population was emotionally unusual.
To test the validity of our instruments, we explored the relationship between the T1 measures of depressed affect of both forms, which are state measures of pre-existing depression, with the BDI, which is a more trait-like measure of pre-existing depression. Across both the control and intervention groups, the baseline (T1) score on form A was significantly correlated with the BDI, r(61)=0.56, p<0.001. The baseline (T1) score on form B was also significantly correlated with the BDI, r(54)=0.73, p<0.001. Despite being state measures of depressed affect, both forms were moderately good predictors of the BDI, which supports their validity as measures of depressed affect.
The effects of age, sex, and order
Age was not significantly correlated with the T1 depression score, the T2 depression score, or the RAPM score in either the control group or the intervention group. These variables also were not affected by the sex of subjects or the order in which they took the two forms.
The baseline measure of depressed affect at T1 in the control and intervention groups
The control group's mean level of pre-existing depression at T1 was 0.29, SD=1.03 (range=−1.77 to 3.01), whereas the mean T1 score for the intervention group was −0.04, SD=0.86 (range=−1.97 to 1.58). The control group was marginally more depressed, t=1.90, df=113, p=0.06. When an outlier in the control group was removed, the groups were not significantly different from each other in their baseline level of depression, t=1.64, df=112, p>0.10. Put simply, save for the outlier in the control group, the groups were similar in their baseline level of depression. All subsequent results that we report include the outlier, but they do not change substantively if the outlier is excluded.
The change in depressed affect from T1 to T2
We predicted that the analytically challenging intervention would elicit depressed affect in subjects with low levels of pre-existing depression. We divided the control and intervention groups into three approximately equally sized subgroups, based on their T1 depression. Consistent with our prediction, intervention subjects in the low pre-existing depression group tended to increase in depression at T2, mean change=+0.12, SD=0.22, p=0.02, whereas control subjects with low pre-existing depression tended to decrease at T2, mean change=−0.03, SD=0.03, p<0.001 (see Figure 2).
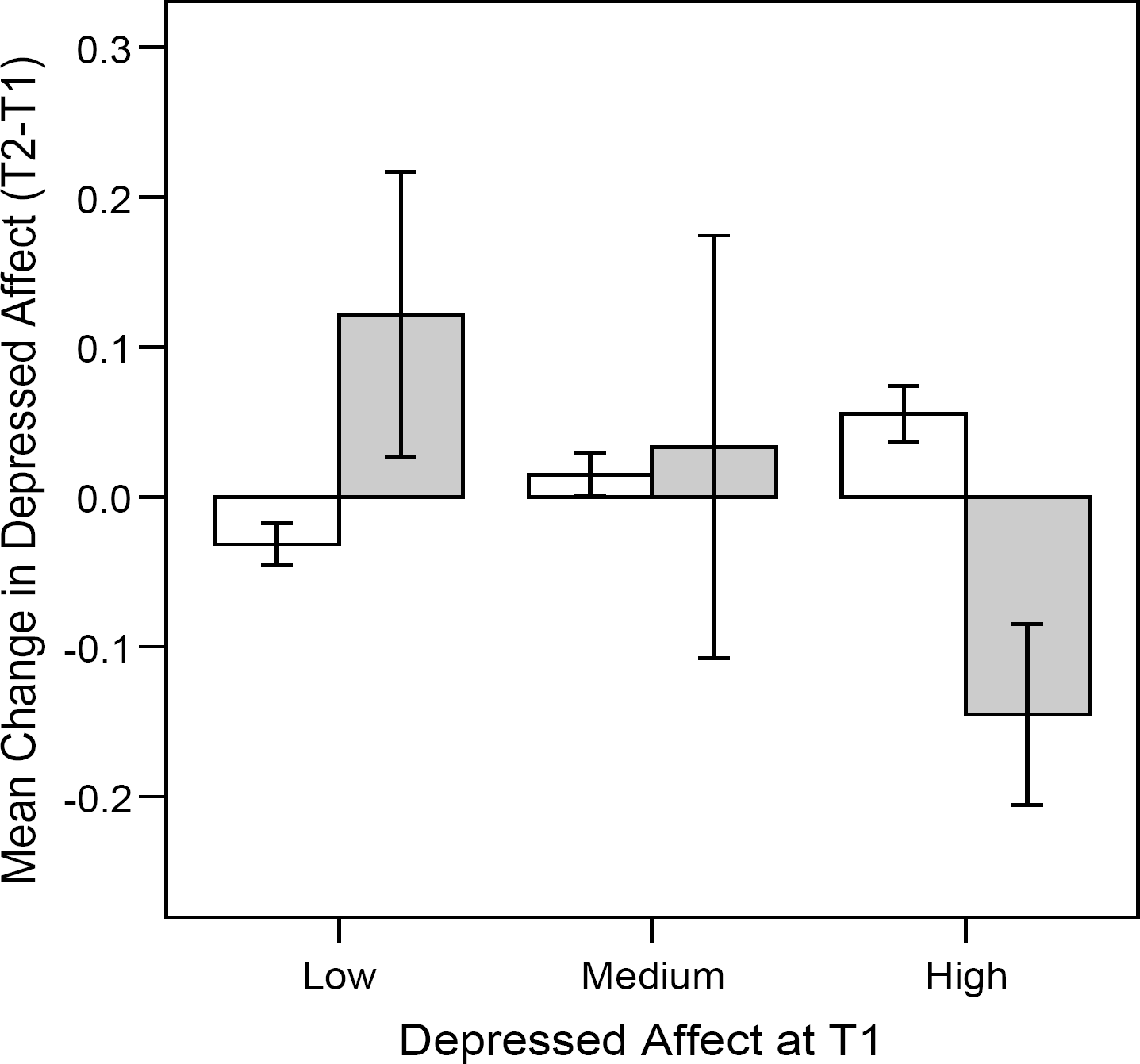
The white bars represent the control groups, whereas the gray bars represent the intervention groups. The error bars represent twice the standard error of the mean.
The spring and magnet metaphors made different predictions about how subjects with high levels of pre-existing depression would respond emotionally to the intervention. Consistent with the magnet metaphor, subjects with high levels of pre-existing depression showed a significant decrease in depressed affect after exposure to the intervention, mean change=−0.14, SD=0.14, p<0.001, whereas those in the control group showed a slight, but significant increase, mean change=+0.06, SD=0.04, p<0.001.
We get qualitatively similar results if pre-existing depression is treated as a continuous variable. Graphically, the depressive response (T2-T1) is positively related to baseline depression at T1 in the control group and negatively related in the intervention group. (see Figure 3). To formally test for an interaction, we analyzed both groups using linear regression in SAS, with the depressive response as the dependent variable. Depression at T1 was and group status were included as main effects, as well as their interaction. The interaction term was significant, β=−0.17, SE=0.04, p<0.0001, which shows that the depressive response pattern was different for the two groups. When the interaction was dropped and the regression model was applied to each group separately, depression at T1 was a positive predictor of the depressive response in the control group, β=+0.04, SE=0.003, p<0.0001, but it was a negative predictor of the depressive response in the intervention group, β=−0.13, SE=0.03, p=0.0004. (Because there were more females in the control group, we reran these analyses controlling for sex. The substantive results did not change, and sex did not emerge as a significant predictor.) When standardized, the correlation between the depressive responses and the baseline (T1) depression score is 0.91 for the control group and −0.43 for the intervention group.
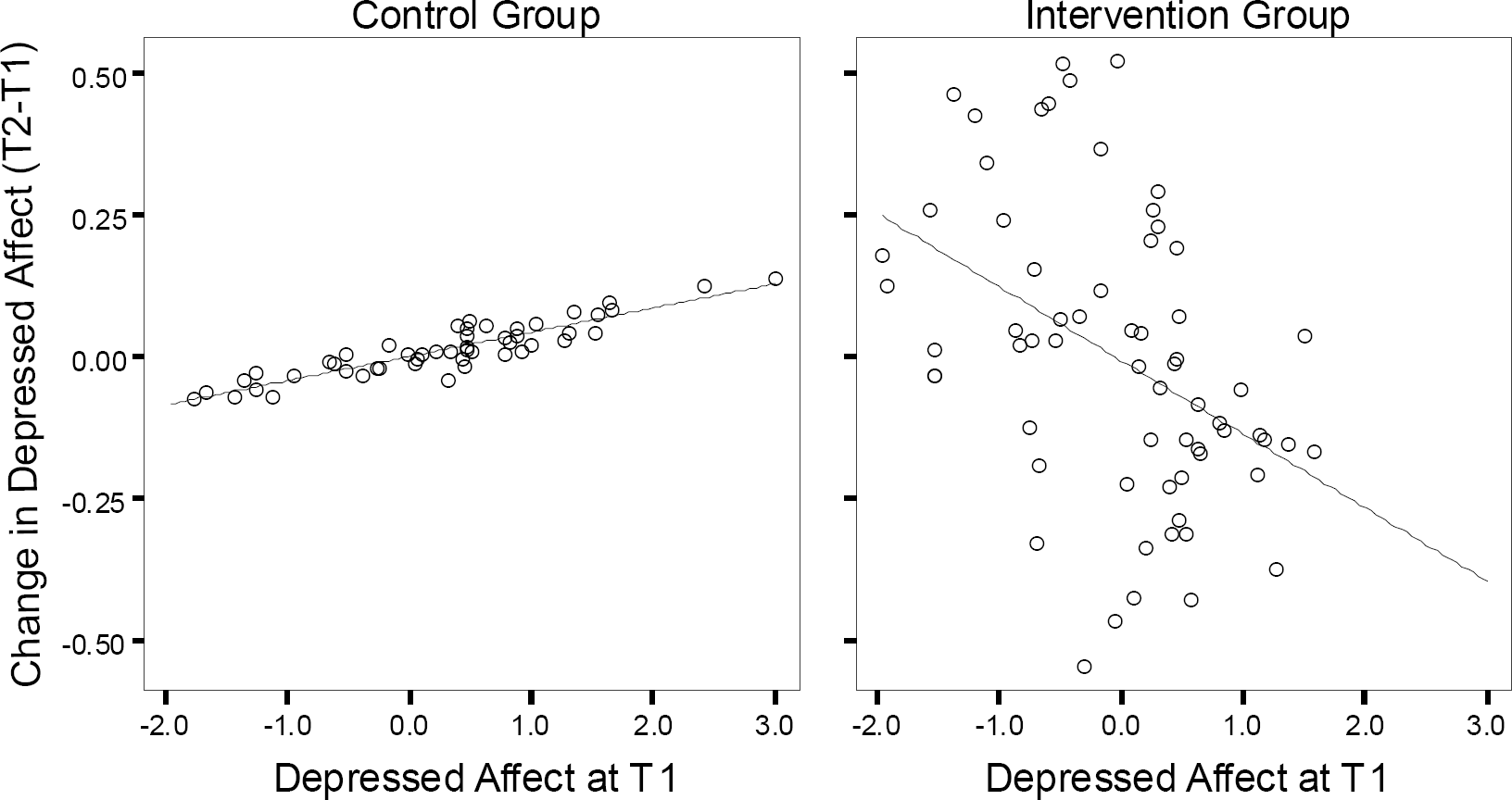
Control and intervention group best-fit regression lines between the change in depression from T1 to T2 and pre-existing (T1) depression.
Depressed affect and analytical reasoning ability
Finally, for the intervention group, we explored the relationship between emotional response to the intervention and subsequent performance on the RAPM. Bivariate correlational analyses yielded no significant relationships between RAPM score and the T1 or T2 depression scores. We then calculated the depressive response as the difference between the T2 and T1 depression scores. Since the depressive response tended to negatively covary with the pre-existing measure at T1, we regressed RAPM on the depressive response (T2-T1) as well as the T1 measure to control for differences in the baseline. The emotional response was a positive predictor of RAPM score, unstandardized β=+4.02, SE=1.54, p=0.01, and the T1 measure was marginally significant, unstandardized β=+0.78, SE=0.46, p=0.10. However, the interpretation of the T1 measure is difficult under these circumstances because it is also used to calculate the difference.
It can be shown that a mathematically equivalent model is to regress RAPM score on the T1 and T2 measures of depression. But the interpretation of the terms is more straightforward. When depression at T1 and T2 are both included in the regression model, each represents the effect of the non-shared (i.e., unique) variance on RAPM score. Thus, after the variance shared in common with depression at T1 is regressed out, depression at T2 represents the effect of participants' emotional response to the intervention on RAPM score. It is conceptually similar to the difference score, and it is also positively related to RAPM score, unstandardized β=+4.02, SE=1.54, p=0.01. When the variance shared in common with depression at T2 is regressed out, the T1 measure represents the effect of participants' pre-existing depression on their RAPM score, controlling for differences in their emotional response to the intervention. It is negatively related to RAPM score, unstandardized β=−3.24, SE=1.40, p=0.02.
Discussion
We hypothesized that depression evolved, at least in part, as a response to important, analytically challenging problems in people's lives that focuses attention on the problem and reduces distractibility. We suggested two control-process mechanisms by which depressed affect could focus attention and reduce distractibility. According to one metaphor, depressed affect exerts a force on attention much like that produced by a spring when it is pulled. The spring metaphor predicts that as attention is pulled from the focal problem, depressed affect increases and has the effect of drawing attention back to the problem. The magnet metaphor, on the other hand, supposes that depressed affect exerts a force on attention much like that produced by a magnet on a steel ball. As attention is pulled from the focal problem, depressed affect decreases, just as the attractive force on the ball decreases as it is pulled away from the magnet. The results of our experiment support the magnet metaphor, and we organize our discussion around it.
Both metaphors predict that an analytically challenging problem will induce depressed affect in subjects with low levels of pre-existing depression. To test this, we devised an analytically challenging intervention—the practice questions from the RAPM that were designed to help subjects prepare themselves for the short form of the RAPM. The prediction was supported (see Figure 2). Subjects with low levels of pre-existing depression showed an increase in depressed affect in the intervention group, but not in the control group.
Both the spring and magnet metaphors assume that people with high levels of pre-existing depression have important, analytically challenging problems in their lives. For these subjects, the intervention was designed to pull their attention away from their pre-existing problems, and the two mechanisms made different predictions about how they would respond emotionally. According to the spring metaphor, people with high levels of pre-existing depression should have experienced an increase in their depressed affect just as the force exerted by a spring increases as it is pulled. The magnet metaphor, in contrast, predicts that depressed affect will decrease just as the magnetic force on a steel ball decreases as it is pulled away from the magnet. The results supported the magnet metaphor (see Figure 2).
The overall depressive response pattern in the intervention group looks like regression to the mean (see Figure 3), with subjects with low levels of pre-existing depression increasing in depressed affect and those with high levels of pre-existing depression decreasing. However, if it were regression to the mean, the same pattern would have been found in the control group. We conducted a formal test, and the interaction term was significant, indicating that the response patterns were different in the two groups. In contrast to the intervention group, the depressive response in the control group was positively related to the T1 measure (see Figure 3). Regression to the mean is not an adequate explanation for the results.
The response pattern of the control group also supports the magnet metaphor. Control subjects who came into the testing with substantial levels of depressed affect experienced an intensification of their depression over the course of the experiment. Lacking any intervention that would pull their attention away from their ruminations, the magnet metaphor suggests that their attention would become increasingly focused on their pre-existing life issues and intensifying their depression, just as the force on a steel ball increases as it comes closer to the magnet. This interpretation is supported by other research. When people with pre-existing depression are experimentally induced to ruminate about their depression and its causes, their level of depressed affect tends to increase (Park, Goodyer, and Teasdale, 2004; Vickers and Vogeltanz-Holm, 2003). According to the magnet metaphor, depressed affect should increase as attention focuses more tightly on the problem that elicited the episode, just as the magnetic force on the steel ball increases as it gets closer to the magnet.
Other research supports the magnet metaphor as well. For instance, people with pre-existing depression experience an alleviation of depressed affect when they are given tasks that are designed to distract them from their ruminations (Nolen-Hoeksema and Morrow, 1993). A distracting task pulls attention away from the core problem that elicited the episode, and it is akin to pulling the steel ball away from the magnet. In short, depressed affect decreases as attention is pulled away from the problems that depressed people ruminate about just as the force on the ball decreases as it is pulled from the magnet.
A crucial point about the magnet metaphor is that the force exerted on a steel ball decreases as it is pulled away from the magnet, but it is not eliminated. There is always some residual magnetic force that will draw the ball back to the magnet unless some countervailing force, such as friction, prevents it from doing so. If the magnet metaphor holds, then depressed affect will decrease when attention is pulled away from the core problem that elicited the depressive episode. But there should be some residual level of depressed affect that eventually draws attention back to the core problem. Depressed affect can only be completely eliminated by solving the problem that elicited the episode, or by disengaging from the goal represented by the problem. We did not explicitly test this in the present experiment, but other evidence in the literature supports this prediction. People with pre-existing depression who systematically try to cope with their depression by trying to distract themselves from their ruminative thoughts either do not have shorter episodes (Kuehner and Weber, 1999; Nolen-Hoeksema, Morrow, and Fredrickson, 1993) or they have longer episodes (Schmaling et al., 2002). Similarly, a recent longitudinal study suggests that people who attempt to suppress the ruminative thoughts that they have in response to stress have longer or more severe depressive episodes, and their attempts to reduce their ruminations are unsuccessful (Wenzlaff and Luxton, 2003). Thus, attempts to pull attention away from depressive ruminations may temporarily alleviate depressive symptoms, but they do not make the symptoms go away. If anything, such attempts appear to lengthen depressive episodes, not shorten them.
A magnet-like control process mechanism may be better designed than a spring-like mechanism for dealing with the inherent tradeoffs that organisms face when managing multiple adaptive problems. Analytically challenging problems, by their very nature, require sustained processing, so the ability to resist distractions is very functional. At the same time, the organism must be able to temporarily divert attention from the core analytical problems that caused the depressive episode to attend to pressing matters that require immediate attention (e.g., predators, important social problems). The magnet metaphor suggests that it may take some initial effort to pull attention away from the core problem, but after it has been pulled away, it takes less effort to keep it away. The spring metaphor, in contrast, suggests that increasingly greater effort is required to resist the spring's force as attention is pulled further away from the core problem, which would make it difficult to attend to anything other than the core problem, no matter how pressing other problems are.
The magnet metaphor may seem paradoxical in the sense that depressed affect increases as attention is focused more on the problem, and people should do things that avoid causing them pain. However, analogous findings exist in the literature on physical pain. Pain draws attention to an injury, or the threat of injury, and when attention is drawn away from an injury by a more pressing problem, pain alleviates (Eccleston and Crombez, 1999; Wall, 2000). Thus, one may want to avoid pain by avoiding a wound. Or, given a wound, one may wish the pain to go away and take pain killers for that reason. But the reason for the pain is to focus attention on caring for the wound, which will happen in the absence of distractions or pain killers. By analogy, it is the pain of depression that makes one attend to the underlying problem that caused the episode. And the more pain that one feels, the more one attends to the problem. In terms of the magnet metaphor, even if attention is focused on other things, residual depression will tend to keep drawing attention to the problem. As attention begins to focus on the problem, the depression increases and attention focuses even more.
The magnet metaphor leads to an important conclusion—depressed affect is a marker of the degree to which attention is focused on a difficult problem. When depressed affect is high, attention is highly focused, just as the magnetic force on a steel ball is greatest when it is closest to the magnet; when depressed affect is low, attention is unfocused, distracted, or divided between multiple problems.
The idea that depression is a marker of the degree to which attention is focused may help interpret the RAPM findings. The nature of this part of the discussion is necessarily more speculative, but it could form the basis for future experiments. The RAPM is an analytically and attentionally demanding task (Carpenter et al., 1990), and performance on the RAPM is positively associated with the ability to maintain a focused attentional state in the presence of distracting stimuli (Gray et al., 2003). High performers on the RAPM tended to have high T2 depression scores, after controlling for differences in their pre-existing depression at T1. For high performers, the intervention may have made the RAPM a salient problem that generated depressed affect and drew attention to it like a magnet.
This suggests that people with higher levels of pre-existing depression should have had more difficulty performing well on the RAPM. The personal life problems that caused their depression served as a magnet that drew on their attention. They had to pull their attention away from their pre-existing life problems long enough for the RAPM to become another magnet that could gain traction on their attention. But the higher their pre-existing depression, the stronger the magnetic force exerted by their personal life problems, and the more difficult it should be to pull attention away from them. This may explain why the T1 measure of depressed affect was a significant negative predictor of RAPM score, after controlling for differences in the T2 measure.
As a single experiment, this is a preliminary test of our hypothesis that depressed affect evolved as a response to analytically challenging problems, and it needs to be replicated.
The fact that subjects with low pre-existing depression in the intervention group experienced a post-intervention increase in depression, but those in the control group did not, suggests that the increase was attributable to something about the intervention. We used an evolutionarily novel intervention, which might be viewed as a limitation of the experiment. However, people in modern, industrialized societies perform evolutionarily novel tasks frequently, and they must do so with evolved mechanisms. The use of evolutionarily novel tasks to help determine the functional design of evolved mechanisms can be very useful. In this case, we chose an analytically demanding task that was devoid of other evolutionarily important content. For instance, complex social problems often have an analytical component to them, but they might also have other content to them. The RAPM is a well-established test of analytical reasoning that lacks social content.
At the same time, the intervention's design is still not specific enough to isolate the precise properties of the intervention that made it depressogenic. For instance, subjects not only tried to answer the practice questions, they also read instructions about the practice questions. We have no empirical or theoretical reason to believe that the instructions were capable of eliciting depressed affect on their own. Still, we acknowledge this limitation in the design.
Another possibility is that the intervention elicited depressed affect because it caused subjects to be fatigued or frustrated by the practice questions, which were difficult and challenging. However, if the task was depressogenic because it was fatiguing or frustrating, then we would have expected subjects who got more depressed in response to the practice questions to perform worse on the subsequent RAPM. But subjects who got more depressed in response to the practice questions actually performed better on the test. The enhancement of performance suggests that depressed affect was not a response to fatigue or frustration.
Finally, we consider the possibility that depressed affect was elicited by the intervention because subjects failed to correctly answer the practice questions. This would make the intervention similar to negative feedback methods for eliciting depressed affect. But, again, subjects who showed a higher depressive response to the intervention scored better on the RAPM short form that they took after the intervention, not worse. If failure was a complete explanation for the elicitation of depressed affect, then who got the practice questions correct would have come out of the intervention with lower levels of depressed affect, which would have made them do worse on the RAPM. But it seems unlikely that people who got the intervention practice questions correct would systematically do worse on the actual test. A more plausible explanation is that the intervention elicited depressed affect because the questions were analytically difficult and attentionally demanding.
Even if failure did play a role in eliciting depressed affect, one can always ask why failure elicits depressed affect. The usual explanation is that failure elicits depressed affect because it creates the perception of helplessness. But if some subjects did get more depressed because they failed the practice questions, their better subsequent performance on the RAPM short form means that they did not give up (i.e., they did not become helpless). Indeed, failure might elicit depressed affect because it indicates that there is a problem that requires more focused attention, which is consistent with our hypothesis.
In short, we don't think it likely that fatigue, frustration, failure, or the practice question instructions were responsible for the elicitation of depressed affect. The results are consistent with our hypothesis that it was the analytically and attentionally demanding nature of the practice questions that elicited depressed affect. We therefore view the results as preliminary support for our hypothesis. Still, our ability to draw inferences about the precise aspects of the intervention that elicited depressed affect, and why they did so, are somewhat limited. This should be explored in future work.
Another limitation in our design is that the time between the two depression assessments was unequal for the control and intervention groups. While we did not measure the intervening time, it is clear to us the time was shorter for the control group than the intervention group. This may partly explain why the depressive response was highly correlated with the measure of pre-existing depression at T1 in the control group. There are two potential problems with this. First, the time between the two measurements could have been so short that subjects remembered what they reported at T1 when filling out their T2 assessment. We guarded against this problem by using two different, but roughly equivalent, instruments. It shouldn't matter if subjects remembered how they filled out the first instrument at T1 because the instrument at T2 used different adjectives. Subjects would still have to read and think about how each adjective applied to them at the time they were filling it out.
Second, the control group might have shown a different emotional response pattern if they had as much time between the T1 and T2 measurements as the intervention group. The control group's emotional response was positively correlated with their baseline (T1) score (Figure 3). In contrast, the intervention group's emotional response was negatively correlated with their baseline (T1) score (Figure 3). To say that the control group was inadequate for this reason is to argue that somehow their emotional response would have been more like that of the intervention group if they had been given more time between the T1 and T2 measurements. This would require time to have a non-linear effect on the emotional response of the control group: first showing a positive correlation with the baseline shortly after the baseline was taken, and then changing to a negative correlation with the baseline later on. In principle, this is possible, but we see no reason to believe that additional time would have had such an unusual effect. Still, we recognize it as a limitation in our design.
Conclusion
We elicited depressed affect in subjects with low levels of pre-existing depression by giving them an analytically and attentionally challenging intervention. Moreover, the overall pattern of subjects' response to the intervention supports the idea that depressed affect exerts a force on attention much like a magnet does on a steel ball, which, in turn, suggests that depressed affect is a marker of the degree to which attention is focused. Finally, subjects' depressive response to the intervention positively predicted their subsequent performance on the RAPM, which provides further support for the idea that depressed affect promotes an analytical processing style.
Footnotes
Acknowledgements
PWA was supported by a National Research Service Award from the National Institutes of Health, P32 MH-20030 (PI: Michael C. Neale). We thank Ed Hagen and two anonymous reviewers for their comments, and Chuck Gardner for statistical advice.