
Abstract
Background:
There is a lack of knowledge about internet-based cognitive behavioural therapy in patients with cardiovascular disease, and its effects on depressive symptoms and physical activity.
Aim:
To examine trajectories of depressive symptoms and physical activity, and to explore if these trajectories are linked with the delivery of internet-based cognitive behavioural therapy.
Methods:
A secondary-analysis of data collected in a randomised controlled trial that evaluated the effects of a 9-week internet-based cognitive behavioural therapy programme compared to an online discussion forum on depressive symptoms in cardiovascular disease patients. Data were collected at baseline, once weekly during the 9-week intervention period and at the 9-week follow-up. The Montgomery Åsberg depression rating scale – self-rating (MADRS-S) was used to measure depressive symptoms. Two modified items from the physical activity questionnaire measuring frequency and length of physical activity were merged to form a physical activity factor.
Results:
After 2 weeks the internet-based cognitive behavioural therapy group had a temporary worsening in depressive symptoms. At 9-week follow-up, depressive symptoms (P<0.001) and physical activity (P=0.02) had improved more in the internet-based cognitive behavioural therapy group. Only in the internet-based cognitive behavioural therapy group, was a significant correlation (r=–0.39, P=0.002) between changes in depressive symptoms and changes in physical activity found. Structural equation analyses revealed that internet-based cognitive behavioural therapy decreased depressive symptoms, and that a decrease in depression, in turn, resulted in an increase in physical activity.
Conclusions:
Internet-based cognitive behavioural therapy was more effective than an online discussion forum to decrease depressive symptoms and increase physical activity. Importantly, a decrease in depressive symptoms needs to precede an increase in physical activity.
Background
In patients with cardiovascular disease (CVD) (i.e. atrial fibrillation/atrial flutter, ischaemic heart disease and heart failure), depressive symptoms are prevalent (20–40%) and constitute a health problem leading to a poorer quality of life and a worse prognosis, 1 which stresses the importance of intervening in depressive symptoms in CVD.1,2
Cognitive behavioural therapy (CBT) has been proposed as a treatment option for depressive symptoms in CVD patients. 3 However, there is poor access to CBT in clinical care and other treatment options are needed. 4 In non-CVD populations, physical activity has been reported as a treatment option for depressive symptoms, 5 whereas the evidence for patients with CVD is scarce. This could at least partly be due to the fact that a significant proportion of studies evaluating the effect of physical activity on depression in CVD has included patients irrespective of their levels of depressive symptoms. 6 There are other aspects that may act as barriers to the use of physical activity as treatment for depression in CVD, for instance lack of motivation, which can be seen as an inherent aspect of depression.7–9 Another barrier is a fear that physical activity might be harmful. 9 This is interesting, as depressive symptoms in CVD are associated with a decline in exercise confidence despite participation in a cardiac rehabilitation programme. 10 To conclude, simply recommending physical activity as a treatment option for depressive symptoms in CVD patients may not be feasible. Suggesting other treatment strategies is also warranted.
Studies of CVD patients with depressive symptoms have reported that psychological strategies can facilitate physical activity. 9 One suggestion could be to provide CBT, because it may improve both depressive symptoms and facilitate physical activity. To our knowledge, only one study has studied the impact of CBT on depression and physical activity. Gary et al. 11 showed that CBT combined with home-based exercise in patients with heart failure compared to CBT and exercise alone was most effective in reducing depression and increasing physical function. However, as access to CBT is scarce, a possible solution could be to use internet-based cognitive behavioural therapy (ICBT). ICBT has been found to be effective in patients with depression in many trials,12,13 but the number of studies of ICBT in CVD is limited. 3 Thus, there is currently a knowledge gap concerning whether ICBT in CVD can be used to reduce depressive symptoms and increase physical activity, and whether and how improvements in depressive symptoms are associated with, or affect, physical activity. We recently completed a study that included CVD patients with at least mild depressive symptoms (n=144). We found that ICBT (n=72) compared to an online discussion forum (ODF) (n=72) had a moderate to large effect on depressive symptoms. 14 In that study, data regarding the level of depressive symptoms and self-reported physical activity were collected weekly but not analysed in any detail. In this article we report a secondary analysis of the weekly collected data in order to examine the trajectory of depressive symptoms and associations with the trajectory of physical activity. We also report differential effects of ICBT and ODF in relation to trajectories of depressive symptoms and physical activity.
Methods
A secondary analysis of data collected in a randomised controlled trial (RCT) that evaluated the effect on depressive symptoms of a 9-week ICBT programme was performed. The study has been described in detail elsewhere. 14 In brief, 144 CVD patients with mild depression (i.e. patient health questionnaire score ⩾5) were recruited from medical and cardiology clinics at four hospitals in south-eastern Sweden. Potential participants were invited by letter. Patients interested in participating were instructed to register on the study website and were asked to complete a web-based screening form. Included patients were randomly allocated to 9 weeks of ICBT (n=72) or ODF (n=72). The ICBT programme consisted of seven modules: goal setting, psycho-education, problem-solving, behavioural activation and a summary module. All modules included home-work assignments and written feedback was provided on each assignment from a study nurse. In the ICBT programme, the psycho-education module also included information about physical activity. The ODF consisted of nine discussion topics moderated by a nurse. In the ODF, physical activity was one of the topics discussed. The regional ethical review board of Linköping Sweden approved the study (ref. no. 2011/166-31). The primary study is registered at clinical trials.gov (NCT01681771).
Data collection
Data for the present analysis were collected at baseline, once weekly during the 9-week intervention period, and at follow-up approximately one week after the 9-week intervention period.
Depressive symptoms
The Montgomery Åsberg depression rating scale – self-rating (MADRS-S) consists of nine items rated on a seven-point scale with a maximum score of 54. Scores between 0 and 12 have been proposed to indicate no depression, whereas scores between 13 and 19 and scores between 20 and 54 indicate mild, respectively, moderate/severe depression. 15 MARDS-S has been found to be sensitive to change in depression shorter time periods (i.e. 4 weeks), 16 and has also been found valid and reliable when administered by the internet. 17 Chronbach’s alpha in the present study for MADRS-S at baseline and follow-up was 0.77 and 0.93, respectively, indicating a good reliability.
Physical activity
Two modified items from the physical activity questionnaire 18 were used to measure the frequency and length of physical activity. Frequency was scored between ‘none of the days’ (0) to ‘often, 5–7 days’ (3). Length was scored from 0 (0 minutes) to 4 (more than 60 minutes). In the present analysis we used a physical activity factor, which was created by multiplying the two items. Self-reports and single response items have been reported to be reliable and valid estimates of physical activity.19,20
Reliability of the instruments
The mean inter-week correlation was 0.85 for the depression scale (MADRS-S) and 0.80 for the physical activity scale. This suggests that both instruments were stable and reliable to the same extent over the weeks.
Statistical analysis
Analysis of covariance (ANCOVA) adjusting for baseline scores and regression to the mean 21 was used to examine if there was a difference in depressive symptoms and physical activity between the ICBT and ODF groups at follow-up. These analyses were performed on original data. For the analysis of the trajectories of depressive symptoms and physical activity, we did not have complete data at each measurement point: baseline n=144; week 1 n=135; week 2 n=134; week 3 n=125; week 4 n=125; week 5 n=123; week 6 n=120; week 7 n=119; week 8 n=97; week 9 n=96; follow-up n=127. We therefore used mixed models based on imputed data. None of the variables in Table 1 had at least significant and moderate associations with depressive symptoms or physical activity at baseline or follow-up, thus imputation was based on the repeated outcome measurements (i.e. MADRS and physical activity) resulting in an imputation model using five iterations. Little’s missing completely at random (MCAR) test showed that data were not missing completely at random (Little’s MCAR P=0.038). After excluding week 8 and week 9 a new analysis revealed that data were missing completely at random (Little’s MCAR P=0.09). Therefore, to control for the robustness of the results we also performed mixed model analysis based on original data including and excluding weeks 8 and 9 as sensitivity analysis.
Description of the study population.
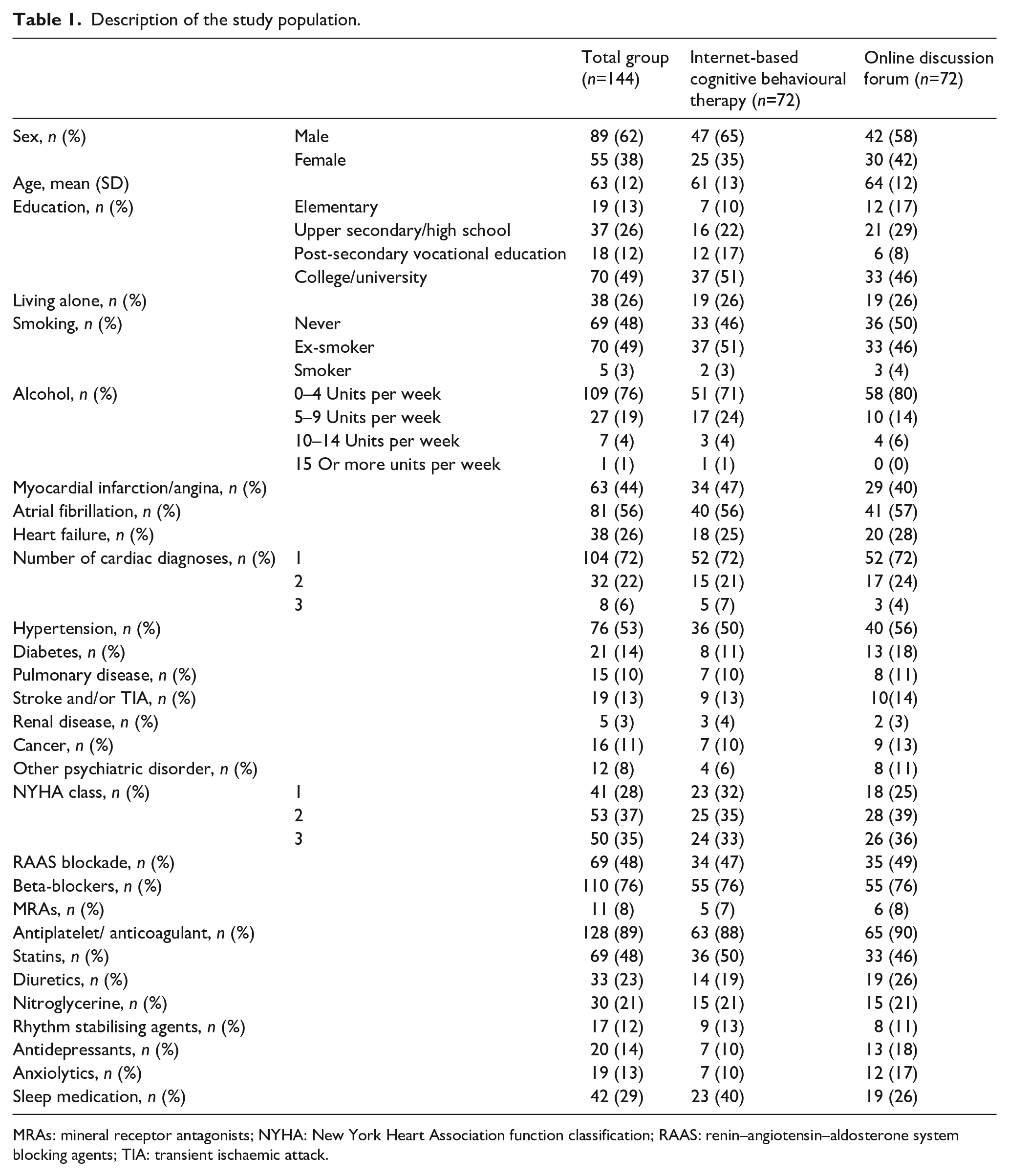
MRAs: mineral receptor antagonists; NYHA: New York Heart Association function classification; RAAS: renin–angiotensin–aldosterone system blocking agents; TIA: transient ischaemic attack.
To explore the appearance of the trajectory of depressive symptoms and the trajectory of physical activity, we first analysed the relationships between depression, physical activity and time by means of product-moment correlations based on the original individual scale values over the 9 weeks. In order to reduce the effects of initial differences between subjects, we also calculated scores representing changes in depressive symptoms and physical activity between the subjects’ first and follow-up measurements, these scores were also then analysed using product-moment correlations. We also analysed the associations between treatment, depressive symptoms and physical activity by using a dichotomous treatment variable (ICBT vs. ODF) labelled ICBT and the two variables based on the changes from baseline to follow-up in depressive symptoms (difference – MADRS-S) and physical activity (difference – physical activity) and labelled ‘change depressive symptoms’, and ‘change physical activity’. The associations between these manifest variables (ICBT, change depressive symptoms and change physical activity) were then analysed by means of structural equation modelling (SEM). Three alternative models were compared. In the first model we explored that ICBT decreases depressive symptoms and decreases in depression, in turn, lead to increases in physical activity. In the second model, ICBT increases physical activity and activity, in its turn, decreases depression. The third model is recursive with an interaction between depression and physical activity; that is, changes in depression cause changes in physical activity and changes in physical activity cause changes in depression. Different goodness of fit indices allow for comparison between the three SEM models. We used the chi-square value, the root mean square error of approximation (RMSEA) and comparative fit index (CFI). CFI indicates to what extent the co-variation in data can be explained by a given model in comparison to other models. For the chi-square test a significant value indicates a poor fit. A P value less than 0.05 indicates a significant value. Statistical analyses were performed with SPSS version 25.0 and the LISREL8 software. 22
Results
Participants
The two groups were similar at baseline (Table 1). The mean age was 63 years (standard deviation (SD) 12) and 38% (n=55) were women. Regarding the MADRS-S mean score at baseline, there was no significant difference between the groups, (ICBT 18.01 ± SD 7.25 vs. ODF 17.67 ± SD 6.19, P=0.76), and 14% (n=20) of the total sample had been prescribed antidepressant treatment and this was not significantly different between the groups. The physical activity mean score at baseline was not significantly different between the groups (baseline ICBT, 4.7 ± SD 3.4 vs. ODF 5.0 ± SD 3.7, P=0.62).
Trajectories of depressive symptoms and physical activity
ANCOVA analysis revealed a significant improvement in depressive symptoms at follow-up favouring ICBT (F=24.7, P<0.001, mean difference 5.8, 95% confidence interval (CI) 3.5–8.1). Mixed model analysis on imputed data on the trajectory of depressive symptoms from baseline to follow-up (Figure 1) also showed a significant improvement in the ICBT group at follow-up (t-value 3.2, P=0.01, estimated mean difference 5.7, 95% CI 2.2–9.1). Visual inspection of Figure 1 shows that the trajectory of depressive symptoms starts to deviate between ICBT and ODF at week 4 and to become significantly different at week 7 (t-value 2.1, P=0.035, estimated mean difference 4.0, 95% CI 0.3–7.6) and remains significant to the follow-up. Analysis of original data including and excluding week 8 and week 9 does not change these results. Figure 1 also indicates that the ICBT group at week 2 had a slight but not significant temporary worsening in their depressive symptoms.
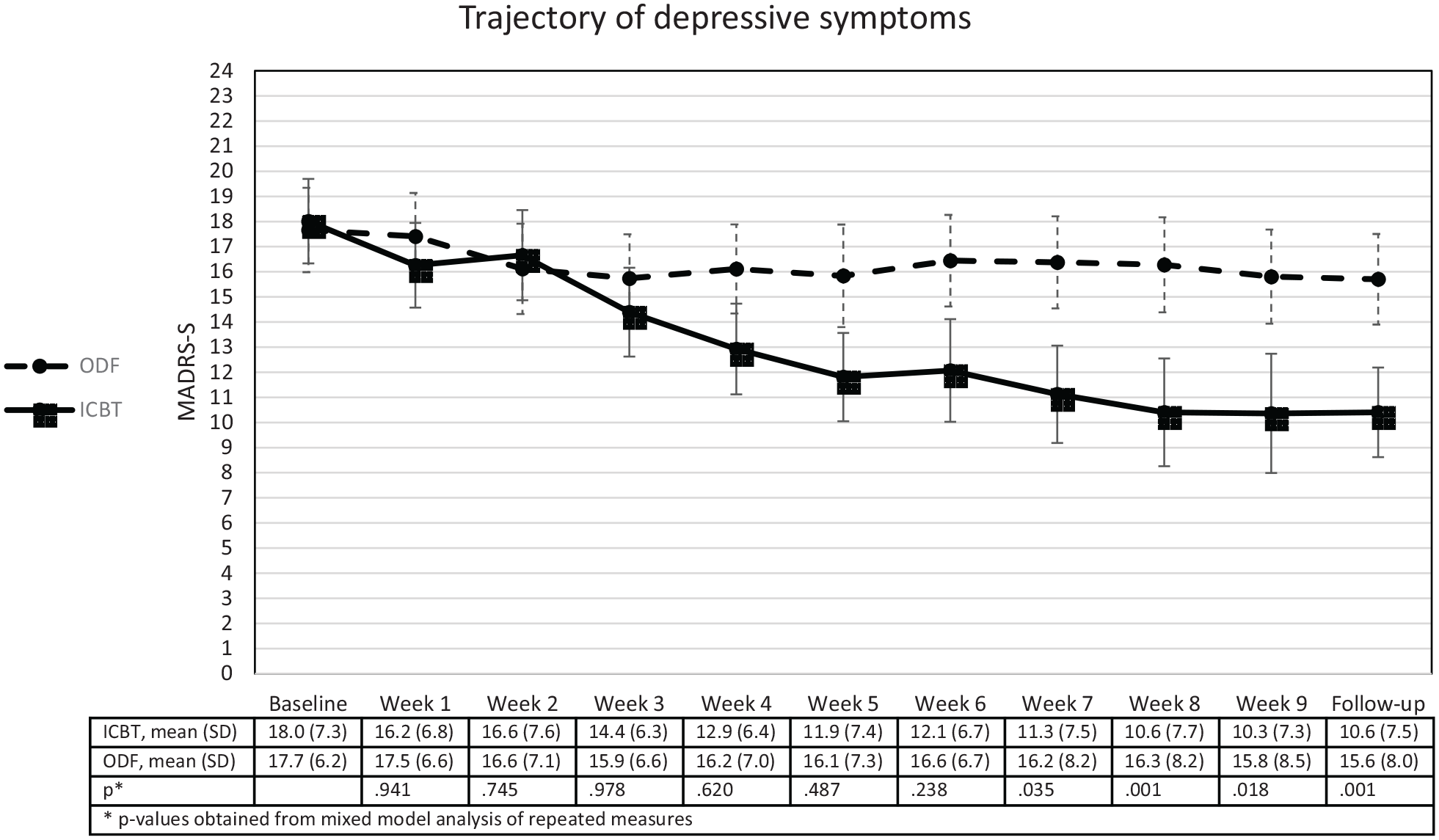
The trajectory of depressive symptoms, as measured by the Montgomery Åsberg depression rating scale – self rating (MADRS-S), in those who participated in an internet-based cognitive behavioural therapy programme (ICBT) and those in the on-line discussion forum (ODF).
For physical activity, the ANCOVA analysis showed a significant increase at follow-up favouring ICBT (F=5.9, P=0.02, mean difference 1.3, 95% CI 0.2–2.3). The mixed model analyses of the trajectory of physical activity revealed that the difference between ICBT and ODF at follow-up was not significant (t-value 1.5, P=0.13, estimated mean difference 1.3, 95% CI ‒0.4–3.0). Visual inspection of the trajectory of physical activity, as illustrated in Figure 2, indicates that the ICBT and ODF group starts to deviate at week 6 and remains to follow-up. However, none of these differences is significantly different. Analysis on original data excluding and including week 8 and week 9 did not change the results reported.
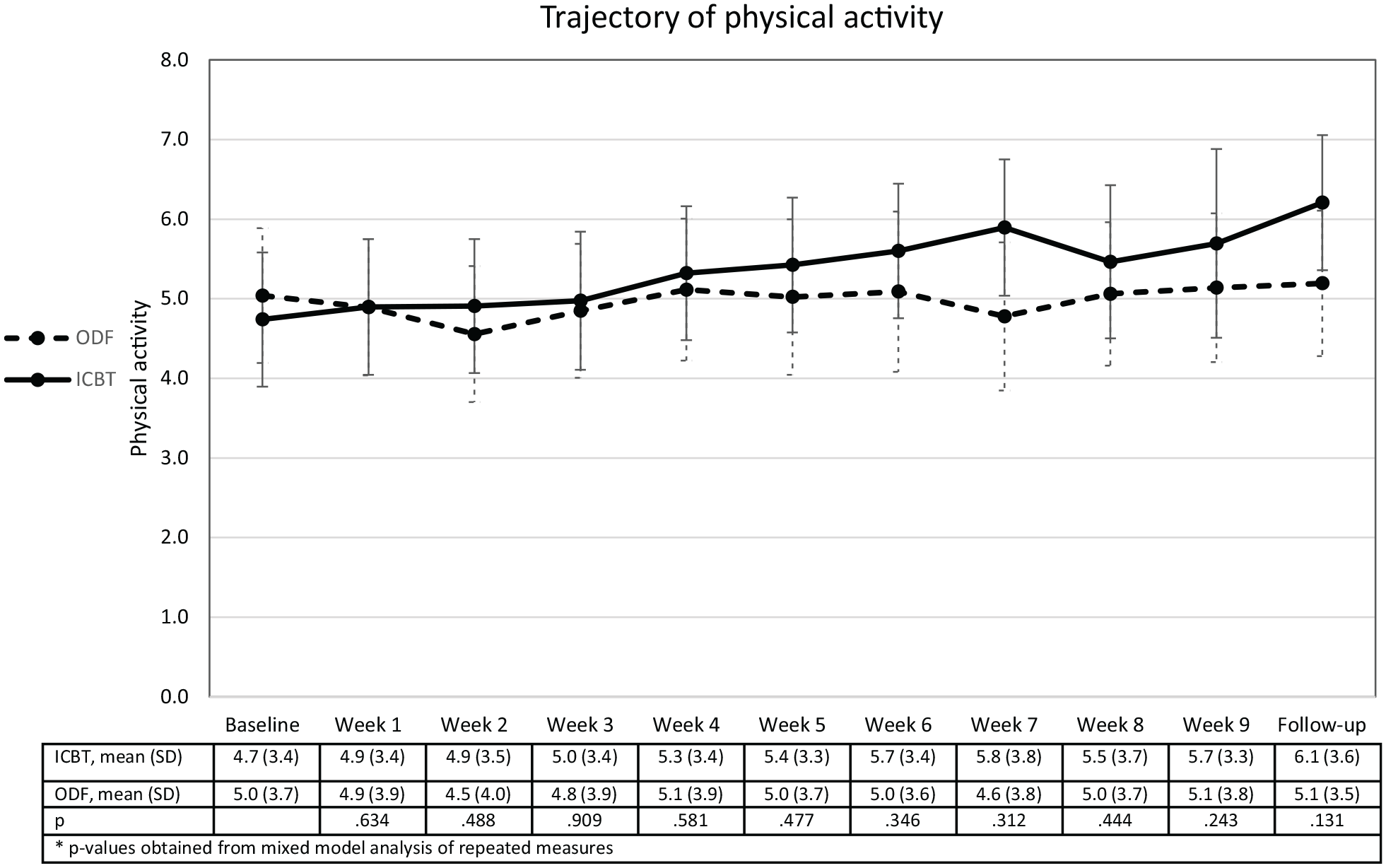
The trajectory of physical activity, in those who participated in an internet-based cognitive behavioural therapy (ICBT) programme and those in the on-line discussion forum (ODF).
The association between the trajectory of depressive symptoms and the trajectory of physical activity
Correlational analysis of the association between depressive symptoms and physical activity based on the original values showed a significant correlation for the ICBT group (r=–0.25, P<0.001). For the ODF group we found a significant but small correlation (r=–0.10, P<0.001). Analysing the association between depressive symtpoms and physical activity using the change scores showed a significant correlation (r=–0.39, P=0.002) for the ICBT group; that is, the larger the reductions in depression, the larger the increases in physical activity. The corresponding correlation for the ODF group was not statistically significant (r=–0.15, P=0.10).
In the SEM analyses of the assocations between ICBT, depressive symptoms and physical activitity, the first model (Figure 3, model 1) explored if ICBT led to decreases in depressive symptoms, and if decreases in depression would lead to increases in physical activity. The second model (Figure 3, model 2) explored if ICBT increased physical activity, and if physical activity would lead to decreases in depression. As seen in Figure 3, the fit of model 1 was perfect (chi-square 0.02, df=1, P=0.96, RMSEA 0.000, CFI 1.00); that is, the two direct effects between the three factors ICBT, depressive symptoms and physical activity, and the indirect effect of ICBT on physical activity (beta=–0.17, P<0.01) almost completely explained the co-variances between the variables. As seen in Figure 2, the fit for model 2 was not satisfactory (chi-square 9.58, df=1, P=0.002, RMSEA 0.264, CFI 0.70). In the third recursive model we tested if there was an interaction between depression and physical activity; that is, whether changes in depression cause changes in physical activity, and whether changes in physical activity in turn would cause changes in depression. As seen from model 3, there was no recursive effect of physical activity on depression (beta=0.01). Our conclusion is that the conditions for recursive effects or interactions between depression and physical activity are not fulfilled in model 3, but that the sequence of model 1 is confirmed. The results suggest that ICBT decreases depressive symptoms, and that decreases in depressive symptoms then lead to increases in physical activity. Furthermore, the indirect effect in model 2 indicates that depression is a mediating factor between treatment and physical activity.
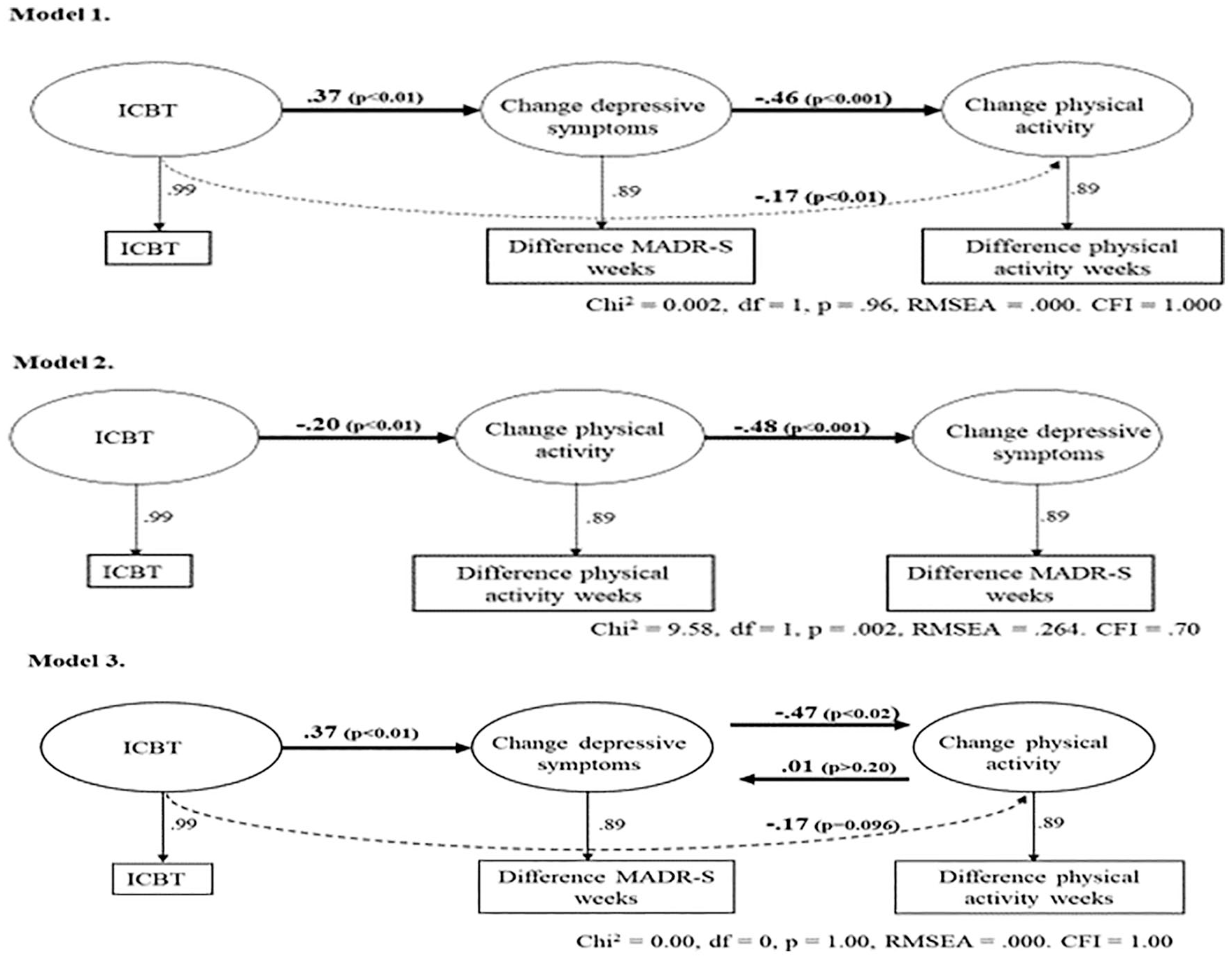
The three structural equation models exploring the causal relationship between treatment, depressive symptoms and physical activity. Model 1 explores if internet-based cognitive behavioural therapy (ICBT) treatment decreases depressive symptoms, and if a decrease, in its turn, produces an increase in physical activity. Model 2 explores if ICBT treatment increases physical activity, and if an increase in physical activity, in turn, decreases depressive symptoms. The recursive model 3 explores if ICBT treatment affects depression, and the interaction between depression and physical activity. Goodness of fit indices of the models are presented in the figure. MARDS-S: Montgomery Åsberg depression rating scale – self-rating; ODF: on-line discussion forum.
Discussion
The aim of this study was to examine trajectories of depressive symptoms and physical activity in relation to ICBT and ODF, and to investigate the associations between these trajectories to discern the temporal order of change. Over the study period we found that as depressive symptoms decreased, physical activity increased in both the ICBT and the ODF groups. However, in the ICBT group there was a stronger association between the decrease in depressive symptoms and physical activity. Of particular interest, our analysis suggested that depressive symptoms had to decrease before an increase in physical activity could be expected. Consequently, when ICBT reduces depressive symptoms, increased physical activity follows.
The analysis of the trajectory of depressive symptoms revealed that depressive symptoms started to improve in the ICBT group after 4 weeks and was significantly different from week 7. However, there was a temporary worsening of depressive symptoms in the beginning of the ICBT programme. Participation in ICBT has been reported to be perceived as stressful and demanding, which can initially trigger symptoms of anxiety.23,24 For example, ICBT requires engagement and may compete with other duties in daily life. Interestingly, the temporary worsening of depressive symptoms corresponded with the performance of the psycho-educative module about depression and how it can be associated with CVD. It could be that becoming aware of this association is perceived as stressful. However, more than 60% completed the full programme, and more than 80% completed more than 50% of the programme. 14 Staff support, and careful information about what to expect when participating in ICBT, has been mentioned by participants in ICBT studies as helpful to overcome and cope with perceived demands and stress.23,24 In our study all participants were given information about what to expect when working with the treatment programme and they also received feedback from nurses on home-work assignments. 25 Our results here inform us that a negative, but temporary, increase in depressive symptoms my be expected. But it is also possible that such negative reaction may be counteracted by support and feedback on homework assignments, which increases the chance of improvements in depressive symptoms with the ICBT programme.
Inherent in the symptomatology of depression is often the problem of staying active or becoming active again.6,26,27 The association found in this study between decreasing depressive symptoms and increasing levels of physical activity in both ICBT and ODF was expected.7,8 In the ANCOVA analysis we found a significant increase in physical activity in the ICBT group compared to ODF at follow-up. This difference was, however, not found in the mixed model analysis. We believe that this difference in the results depends on the fact that mixed models also include the effect of time in the analysis, compared to the ANCOVA that only analyses if there is a difference in the mean values between ICBT and ODF at follow-up. Although not statistically different, visual inspection of the trajectory of physical activity indicates that the ICBT group physical activity starts to increase between week 5 and week 6, whereas physical activity in the ODF group remained unchanged. However, when correlating the changes in depressive symptoms and physical activity, and after reducing the effects of initial differences between subjects, a significant correlation was found for the ICBT group but not for the ODF group. This suggests that the larger the reductions in depressive symptoms, the larger the increases in physical activity favouring ICBT. Interestingly, the SEM analysis showed that decreasing depressive symptoms was a mediator between ICBT and increasing physical activity, and not the other way around. Our study suggests that an ICBT programme targeted to decrease depressive symptoms in CVD patients may also result in an increase in physical activity.
A critical question is if physical activity protects against depression or if depression leads to decreased activity? It is also possible that there is a bidrectional association. A recent study 28 showed that objectively measured physical activity was associated with a reduced risk of depression. On the other hand, studies aimed at evaluating the effects of physical activity on depression show that the positive effects seem to diminsh after the end of the exercise intervention, 5 indicating that structured and supervised exercise programmes do not necessarily lead to a continuation of physical activity. It is also important to bear in mind that CVD patients with depressive symptoms may avoid physical activity due to reasons such as fear of provoking cardiac symptoms and/or being afraid that the heart is vulnerable and does not tolerate physical exercise.9,29 In clinical practice, this suggests that CVD patients with depressive symptoms need more than supervised exercise to learn to become physically active. Thus, CBT may help CVD patients with depressive symptoms to overcome such fears. Moreover, from our SEM analysis we found that a decrease in depressive symptoms led to an increase in physical activity and not the other way around. This suggests that physical activity may be ineffecive if it not is paralleled with another type of treatment, such as CBT, that can also help to decrease depressive symptoms. Combining exercise with psychotherapy such as CBT/ICBT has not been studied extensively. 5 However, in one of the few studies performed, Gary et al. 11 showed that patients with heart failure and depressive symptoms benefitted from CBT combined with home-based exercise, compared to only home-based exercise, or CBT only, or ordinary care. The combined intervention had the best effect in reducing depression, increasing physical function and improving health-related quality of life. In our study the CVD patients in the ICBT programme only received information about, and were encouraged to be, physically active. Thus, we need studies that specifically evaluate the efficacy of ICBT combined with a physical activity in CVD patients with depressive symptoms.
Exercise is the most studied and recommended treatment with beneficial effects on prognosis in CVD. To be effective, the recommendation is for at least 30 minutes per day, 5 days a week, of moderate activity, or at least 15 minutes per day, 5 days a week, of vigorous activity. 30 But are the recommendations for exercise as a secondary prevention in CVD the same as using exercise as a treatment for depression? A recent meta-analysis of 24 studies evaluating the effects of exercise on depressive symptoms in patients with different chronic diseases reported no differential effects on depressive symptoms with regard to the number of training days per week (2–3 days vs. four to five times) or the amount of time spent (⩽30 minutes or 31–60 minutes or >60 minutes). 31 This is in alignment with another study reporting that relatively small amounts of exericese (i.e. at least one hour or more per week), regardless of intensity, was protective against a future depression. 32 In CBT/ICBT or other types of programmes, aimed at decreasing depression in CVD patients, this suggests that the focus may be to stimulate the partcipant to start physical activity instead of primarily achieving the recommendations for exercise in the CVD guidelines.
A limitation of this secondary analysis is that the results relied only on the participants’ subjective reports of physical activity. A study suggests a 20% lower level of physical activity when self-reported physical activity is compared to objectively measured physical activity. 33 Thus, our measure may not be sensitive enough to capture changes in the participants’ physical activity during the study period, this may explain the non-signficant differences between ICBT and ODF in the mixed model analysis of the trajcetory of physical activity. However, the reliability of the physical measure was about the same as the well-established measure of depression. Collection of objective data using measures such as an actigraph would have been interesting and could in future research also be used to validate and expand the findings reported here. However, because of the general lack of research into ICBT in CVD patients’ programmes, we believe that these results provide interesting information regarding the trajectory of depressive symptoms and association with the trajectory of physical activity during a ICBT intervention in CVD patients.
In conclusion, in CVD patients a temporary worsening of depressive symptoms in the beginning a ICBT programme may be expected. In spite of this, ICBT was more effective than ODF in reducing depressive symptoms and increasing physical activity. Importantly, depressive symptoms served as a mediator between ICBT and physical activity, suggesting that in CVD patients a decrease in depressive symptoms needs to precede an increase in physical activity. More ICBT studies focusing on CVD are needed, to explore the associations between changes in depressive symptoms and physical activity. Such studies should be performed on patients with increased levels of depressive symptoms, and should also collect objective data regarding physical activity.
Footnotes
In patients with cardiovascular disease depressive symptoms were associated with physical activity. In patients with cardiovascular disease and depressive symptoms increased physical activity needs to be preceded by a reduction in depression. Internet-based cognitive behavioural therapy targeting depressive symptoms in cardiovascular disease could be used to reduce depressive symptoms and increase physical activity. It is important to be aware that cardiovascular disease patients may have a temporary worsening of depressive symptoms in the beginning of an internet-based cognitive behavioural therapy programme.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swedish Research Council (2015-02600); ALF grants Region Östergötland (LIO-600321 and LIO-687531); and Region Östergötland strategic fund (LIO-719561).