
Abstract
Background:
Hypertension and cognitive impairment often coexist in older people. Office blood pressure measurement is a poor indicator for diagnosing hypertension in the general population. However, its diagnostic accuracy has not been substantially studied in patients with cognitive impairment.
Aim:
The aim of this study was to determine the proportion of misdiagnosis of hypertension in patients with mild cognitive impairment and dementia compared to no cognitive impairment, by comparing office blood pressure measurement with home blood pressure measurement.
Methods:
A cross-sectional study including consecutive patients visiting a memory clinic between 2014 and 2017. Home blood pressure was measured for one week according to the European guidelines. Office blood pressure was assessed during routine clinical practice. Using guideline definitions for normal blood pressure and hypertension, we investigated the proportion of disagreement between office blood pressure measurement and home blood pressure measurement. Univariable and multivariable logistic regression compared disagreement in diagnosis between patients with dementia, mild cognitive impairment and no cognitive impairment.
Results:
Of 213 patients (aged 73.4±9.0 years, 42% women) 82 had dementia, 65 had mild cognitive impairment and 66 had no cognitive impairment. Mean office blood pressure was 156/84±23/11 mmHg and mean home blood pressure was 139/79±16/10 mmHg. In 31% of patients, there was disagreement in hypertension diagnosis. This proportion was higher for mild cognitive impairment (38.5%) and dementia (35.4%) compared to no cognitive impairment (18.2%), with adjusted odds ratios of 3.7 (95% confidence interval 1.5–9.0), P=0.005 for mild cognitive impairment and 3.4 (1.3–8.6), P=0.011 for dementia.
Conclusions:
In memory clinic patients with dementia and mild cognitive impairment, the diagnostic accuracy of office blood pressure measurement is lower compared to patients without cognitive impairment. To avoid the risk of making improper treatment decisions in this vulnerable group, a diagnosis of hypertension should be based on home blood pressure measurement, not office blood pressure measurement.
Introduction
Hypertension is the most prevalent treatable risk factor for cardiovascular diseases, affecting ±75% of people aged over 70 years.1, 2 There is controversy regarding hypertension management in older people with cognitive impairment, 3 despite these morbidities often coexisting in this group. 4 This group has been excluded from randomised controlled trials estimating the benefit-to-risk ratio of antihypertensive treatment. Based on observational evidence, it is postulated that people with cognitive impairment are more prone to side-effects of treatment (such as hypotension and falls) and might even show a more rapid cognitive decline with hypertension treatment.5, 6 Considering this ongoing discussion, the current clinical advice is to assess blood pressure (BP) carefully and accurately in this group, 7 because treatment decisions based on an incorrect diagnosis of hypertension may expose people with cognitive impairment to greater risks than older people with normal cognitive function.
It has generally been acknowledged that the accuracy of an office blood pressure measurement (OBPM) is low and hence out-of-office measurements are now recommended by guidelines.8, 9 Ambulatory blood pressure monitoring over 24 hours (ABPM) has been accepted internationally as the gold standard for hypertension diagnosis, 10 but can be experienced as invasive, 11 and may result in lifestyle disruption, especially in people with cognitive impairment, which reduces its representability for daily life. In addition, it comes with considerable costs. Home blood pressure monitoring (HBPM) has been shown to be a feasible and reliable alternative for ABPM in several populations, 12 including patients with dementia. 13 Not unexpectedly, the majority of dementia patients also indicated that they preferred HBPM over ABPM.
In a general older population (mean age 70 years) the prevalence of a misdiagnosis of hypertension with OBPM, compared with HBPM, was 22%. 14 This percentage consisted of false positives (i.e. white-coat hypertension, 13%) and false negatives (i.e. masked hypertension, 9%). It is unknown whether these findings can be extrapolated to a population of older people with cognitive impairment. Therefore, the aim of this study was to investigate the proportion of misdiagnosis of hypertension with OBPM, when compared to HBPM, in older people with mild cognitive impairment (MCI) and dementia.
Methods
Participants
This cross-sectional study included consecutive patients referred to the memory clinic at a university teaching hospital between 2014 and 2017. Patients who agreed to perform HBPM were eligible for this study. The study was approved by the medical ethics committee and used an opt-out consent approach for the use of medical records. The investigation conforms with the principles outlined in the Declaration of Helsinki.
Of 1159 referred patients, 261 agreed to perform HBPM and did not opt out. Patients who received HBPM had higher systolic office blood pressure (SBP; 155.9±22.8 vs. 150.9±23.4 mmHg, P=0.005), were less often women (40.7% vs. 53.0%, P=0.001), and less frequently had a diagnosis of dementia (39.5% vs. 58.8%, P<0.001). For details see Supplementary Table 1 and Supplementary Figure 1.
Clinical measurements
Clinical information was collected during a comprehensive geriatric assessment by a geriatric medicine registrar. This included information on sociodemographics, psychosocial abilities, functional abilities, cardiovascular history, medication use and cognitive screening. Cardiovascular history was marked as present if one of the following conditions was identified in the medical history: chronic heart failure, coronary heart disease, arrhythmia, cerebrovascular disease, or peripheral artery disease. Cognitive screening included the Mini-Mental State Examination (MMSE; 01/2014–04/2016) or the Montreal cognitive assessment (MoCA; 05/2016–12/2017).15, 16 Functional abilities were assessed with the Barthel index for activities of daily living and the Lawton–Brody scale for instrumental activities of daily living.17, 18 Supine OBPM was taken using a manual sphygmomanometer according to standard clinical practice. Cognitive diagnoses were established in a multidisciplinary meeting with geriatricians and neuropsychologists, based on all information from the geriatric assessment and when necessary after additional diagnostic testing (i.e. neuropsychological testing or neuro-imaging), using international diagnostic criteria.19, 20 Based on this assessment we categorised patients into three cognitive groups: dementia (any type), MCI and cognitively normal (CN; i.e. subjective cognitive complaints).
Home BP measurement
HBPM involved a validated, memory equipped, automatic oscillometric device (Microlife WatchBP Home, Microlife, Heerbrugg, Switzerland), following recommendations of the European Society of Hypertension.21, 22 This comprised duplicate measurements in the morning (06:00–10:00 hours) and evening (17:00–21:00 hours) for 7 consecutive days, resulting in a maximum of 28 measurements. As recommended, measurements for day 1 were discarded and mean BP was not calculated if patients performed fewer than 12 measurements. 22 Patients and (when applicable) their caregiver received a demonstration and written instructions on how to measure home BP. Patients were instructed to sit in a straight chair with the arm supported by a table for at least 5 minutes before starting a measurement.
Outcomes
The main outcome of interest was the presence of disagreement in hypertension diagnosis between OBPM and HBPM. Disagreement in diagnosis was defined as either hypertension on OBPM, but normal HBPM (i.e. white-coat hypertension) or as normal OBPM, but hypertension on HBPM (i.e. masked hypertension). The cut-off point for hypertension on OBPM was SBP ⩾140 mmHg and/or diastolic blood pressure (DBP) ⩾90 mmHg. The cut-off point for hypertension on HBPM was SBP ⩾135 mmHg and/or DBP ⩾85 mmHg. 8 To explore these results further, the presence of white-coat hypertension and masked hypertension were also analysed separately and an analysis with only morning or evening HBPM was performed.
Statistical analysis
Continuous and categorical variables were presented as mean (SD) or median (interquartile range) and % (n), respectively. Descriptive variables were compared between patients with dementia, MCI and CN with analysis of variance, chi-squared test or the Kruskal–Wallis test, as appropriate.
Univariable and multivariable logistic regression models were used to examine the association between disagreement in hypertension diagnosis and cognitive groups. The group of CN patients was used as a reference. In the multivariable model we adjusted for age, sex, level of education (low/medium/high), 23 cardiovascular history (present/absent), use of BP-lowering medication (yes/no) and living situation (alone or with spouse). Unadjusted and adjusted odds ratios with 95% confidence intervals were reported. All analyses were performed using IBM SPSS Statistics 25.0 (SPSS, Inc., Chicago, IL, USA). In order to detect a difference in the proportion of misdiagnosis of 18%, with a power of 80% and alpha set at 0.05, a sample size of 209 patients was required. For details of the sample size calculation see the Supplementary material.
Results
Ninety per cent (236/261) of the patients who agreed to perform HBPM reached the minimum threshold of 12 measurements. There were no relevant differences in characteristics between those with successful and unsuccessful HBPM, as described in Supplementary Table 2. For 9.7% (23/236) of the patients OBPM was missing in the medical record, leading to a final study sample of 213.
Table 1 shows the characteristics of the final study sample. More than two-third (69%) of the patients in the study had a diagnosis of dementia or MCI. Patients with dementia or MCI were significantly older compared to CN patients. Mean home BP was on average −16.8/–5.0 mmHg lower than office BP. This difference was similar across the groups.
Descriptive characteristics of memory clinic patients by cognitive group.
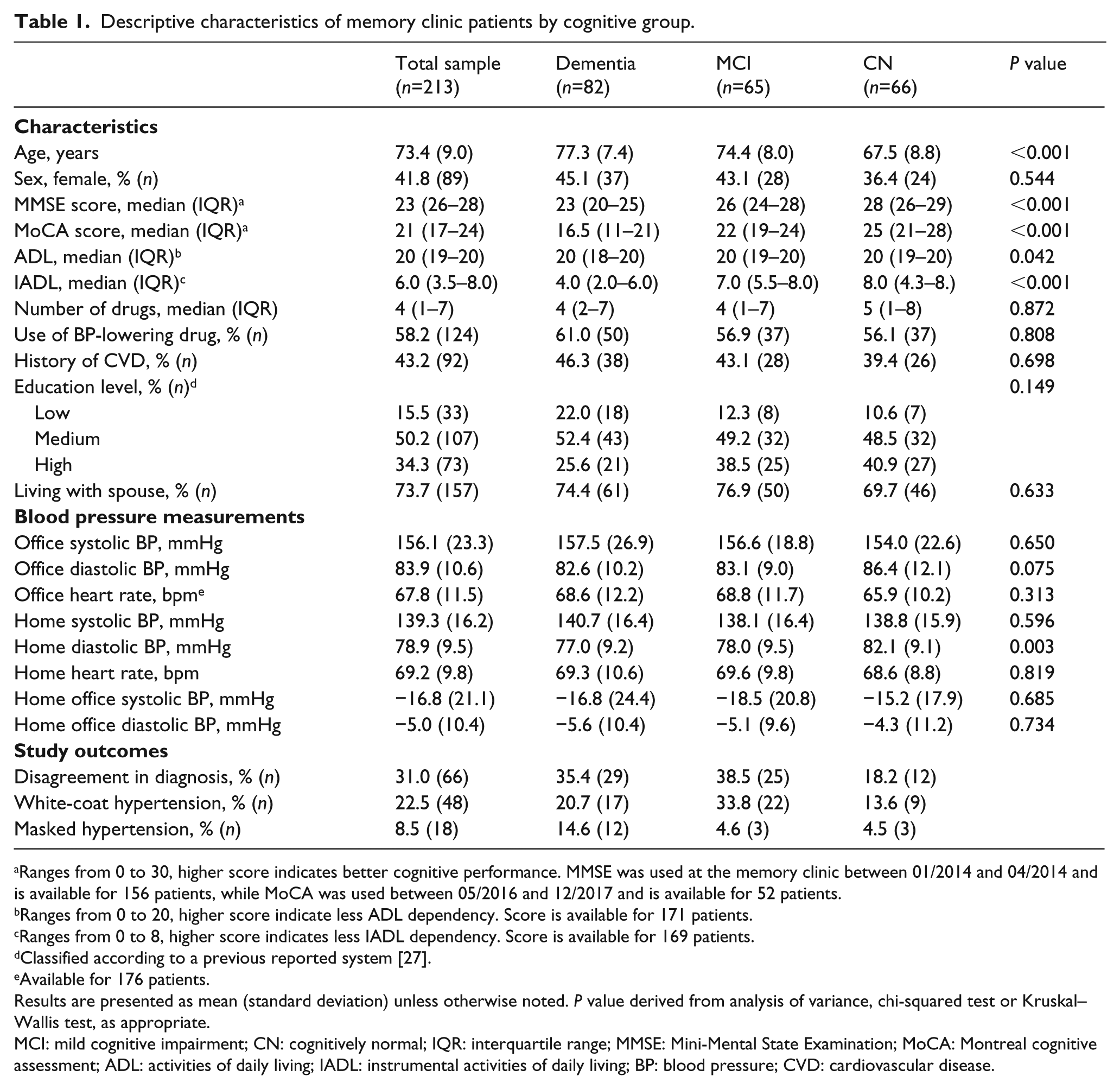
Ranges from 0 to 30, higher score indicates better cognitive performance. MMSE was used at the memory clinic between 01/2014 and 04/2014 and is available for 156 patients, while MoCA was used between 05/2016 and 12/2017 and is available for 52 patients.
Ranges from 0 to 20, higher score indicate less ADL dependency. Score is available for 171 patients.
Ranges from 0 to 8, higher score indicates less IADL dependency. Score is available for 169 patients.
Classified according to a previous reported system [27].
Available for 176 patients.
Results are presented as mean (standard deviation) unless otherwise noted. P value derived from analysis of variance, chi-squared test or Kruskal–Wallis test, as appropriate.
MCI: mild cognitive impairment; CN: cognitively normal; IQR: interquartile range; MMSE: Mini-Mental State Examination; MoCA: Montreal cognitive assessment; ADL: activities of daily living; IADL: instrumental activities of daily living; BP: blood pressure; CVD: cardiovascular disease.
In 31% of patients, there was disagreement in hypertension diagnosis between OBPM and HBPM. This proportion was 35.4% for dementia patients, 38.5% for MCI patients and 18.2% for CN patients (Figure 1). The unadjusted and adjusted odds ratios and 95% confidence intervals are presented in Table 2. Compared to the CN patients, the adjusted odds ratios of disagreement in diagnosis were 3.4 (1.3–8.6) for dementia and 3.7 (1.5–9.0) for MCI.
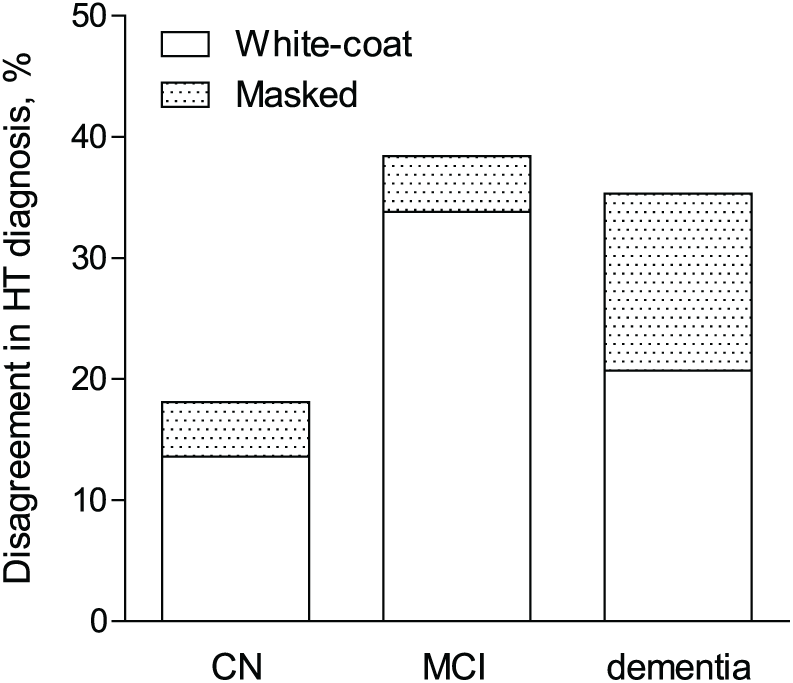
Proportion of disagreement in hypertension diagnosis by cognitive group, split in proportion due to white-coat hypertension and due to masked hypertension.
Univariable and multivariable logistic regression models.

The adjusted model is corrected for age, sex, educational level, use of blood pressure-lowering medication, history of cardiovascular history and living situation.
HT: hypertension; OR: odds ratio; CI: confidence interval; CN: cognitively normal; MCI: mild cognitive impairment.
In additional analyses we analysed the two types of disagreement in hypertension diagnosis separately. We observed a similar pattern for white-coat hypertension, but not for masked hypertension (Table 2). When morning and evening HBPM were analysed separately, similar results were obtained (Supplementary Tables 3 and 4).
Discussion
We investigated the diagnostic accuracy of OBPM compared to HBPM in a memory clinic population. Using recommended cut-offs for hypertension diagnosis, 31% of patients showed disagreement between OBPM and HBPM. The proportion of disagreement was doubled in patients with dementia and MCI compared to CN patients. Even after adjusting for several demographic factors, we found that having dementia or MCI was associated with an increased risk of incorrect hypertension diagnosis. This was mainly driven by a higher prevalence of white-coat hypertension in dementia and MCI and in a smaller extent to a higher prevalence of masked hypertension in dementia.
Previous research showed that the proportion of disagreement between OBPM and HBPM in a cohort of treated hypertensive patients (mean age 70 years) was 22%, 14 which is comparable to our observation in the CN group. Our results now indicate that in older people with cognitive impairment, OBPM is even less accurate. Given previous observations that HBPM is well tolerated and reliable in patients with dementia, 13 this advocates for the use of HBPM before any decisions regarding BP management are made.
Several concepts can be proposed to explain this observation. First, patients with MCI or dementia visiting the clinic might experience more stress or anxiety, resulting in a higher proportion of white-coat hypertension. 24 More speculatively, the seemingly higher prevalence of masked hypertension in dementia patients might be an expression of reduced compliance to antihypertensive treatment in daily life, 25 while patients are reminded to take their medication on the morning of a planned doctor’s visit. Of note here is that 10/12 dementia patients with masked hypertension were indeed prescribed antihypertensive medication. Finally, increased BP variability has been suggested to be involved in the pathophysiology of dementia and can result in a less reliable measurement with only one observation, as is the case with OBPM. 26 In these interpretations we refer to HBPM as the reference standard, which is supported by ample evidence. However, it cannot be completely ruled out that HBPM is responsible for the observed disagreement between groups.
Strengths and limitations
In this study, HBPM was measured according to the European guidelines using a validated device equipped with a memory function and set at fixed time windows. Measurement of OBPM was part of the routine clinical practice, and as a result was assessed by different physicians, which could have introduced observer bias. 27 Nevertheless, it does represent normal clinical practice for OBPM. Also, OBPM was performed manually and HBPM was automated. While it would have been a good extension of this work also to study automated OBPM, it was recently shown that only unattended automated OBPM is comparable to HBPM and attended automated OBPM is as discrepant from HBPM as manual OBPM. 28
Patients who agreed to perform HBPM were biased towards cognitively healthier patients with a higher OBPM. Still, the studied sample included a large diversity of age, cognitive function and BP. We compared our dementia and MCI patients to memory clinic patients without objectively diagnosed cognitive impairment and not to a group of healthy controls. The generalisability of this group has been questioned, 29 although it was recently shown that cognitive function in this group is mostly stable in the long term. 30 In addition, the proportion of misdiagnosis (18.5%) in our CN group compares well with the 22% observed in the general population of older people. As the study had a cross-sectional study design, we were not able to study the prognostic value of HBPM compared to OBPM. Finally, despite giving oral and written instructions not to measure within one hour after food or drug intake and to have 5 minutes rest before measuring, we cannot ensure adherence to these instructions.
Conclusion
We found that in memory clinic patients with dementia and MCI the proportion of disagreement between OBPM and HBPM was high, indicating a lower diagnostic accuracy of OBPM compared to older memory clinic patients with no cognitive impairment. For clinical practice, this advocates the use of HBPM in this group before any decisions regarding BP management are made. In view of the new guideline advice for lower thresholds for treatment of hypertension in older patients, a diagnosis of hypertension should be based on reliable BP measurements. For one-third of patients with MCI and dementia, OBPM leads to an inaccurate diagnosis. In these patients, the benefit-to-risk ratio of hypertension treatment remains uncertain and an individualised approach based on accurate BP measurements is therefore highly desirable.
Supplemental Material
Supplementary_material – Supplemental material for Diagnostic accuracy of office blood pressure compared to home blood pressure in patients with mild cognitive impairment and dementia
Supplemental material, Supplementary_material for Diagnostic accuracy of office blood pressure compared to home blood pressure in patients with mild cognitive impairment and dementia by Rianne AA de Heus, Maxime V Tumelaire, Marcel GM Olde Rikkert and Jurgen AHR Claassen in European Journal of Cardiovascular Nursing
Footnotes
Acknowledgements
The authors would like to thank all study participants and their caregivers for their time and effort. They also thank the secretary and all involved residents of the Radboudumc Alzheimer Center for their support with the recruitment and are grateful to Jeannette Bronk-van Hoorn, Anne Lieke Meendering, Lotte van den Ingh, Faize Önen and Emma Peters for their role in data capture.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: this work was supported by the Dutch Alzheimer Society (grant number WE.09-2015-03).
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.