
Abstract
Background:
Although the implantable cardioverter defibrillator is successful in terminating life threatening arrhythmias, it might give unwanted shocks in the last phase of life if not deactivated in a timely manner.
Aims:
This integrated review aimed to provide an overview of studies reporting on implantable cardioverter defibrillator shock incidence and impact in the last phase of life.
Methods and results:
We systematically searched five electronic databases. Studies reporting on the incidence and/or impact of implantable cardioverter defibrillator shocks in the last month of life were included. Fifteen studies were included. Two American studies published in 1996 and 1998 reported on the incidence of shocks in patients who died non-suddenly: incidences were 24% and 33%, respectively, in the last 24 hours, and 7% and 14%, respectively, in the last hour of life. Six American studies and one Danish study published between 1991–1999 reported on patients dying suddenly: incidences were 41% and 68% in the last 24 hours and 22–66% in the last hour. Four American studies and two Swedish studies published between 2004–2015 did not distinguish the cause of death: incidences were 17–32% in the last month, 3–32% in the last 24 hours, and 8% and 31% in the last hour of life. Three American studies published between 2004–2011 reported that shocks in dying patients are painful and distressing for patients, and distressing for relatives and professional caregivers.
Conclusion:
If the implantable cardioverter defibrillator is not deactivated in a timely manner, a potentially significant proportion of implantable cardioverter defibrillator patients experience painful and distressing shocks in their last phase of life.
Introduction
During the last phase of life, goals of care usually shift from prolonging life to maintaining quality of life. 1 Many patients with heart failure eventually die due to progression of their underlying heart condition, despite the many treatments that are currently available. 2 Whether certain life-sustaining treatments are still appropriate in this last phase of life is an important topic of discussion. The implantable cardioverter defibrillator (ICD) is one of these life prolonging treatments that may pose difficult dilemmas in the last phase of life. The ICD is currently the treatment of choice in patients who are at risk of sudden cardiac death because of ventricular arrhythmias. 3 In Europe, more than 85.000 ICDs were implanted in 2013, based on 46 countries, mainly in Western Europe. 4 The number of new implants is still increasing, due to both an ageing population and expanding of the indication for ICD implantation, shifting from secondary prevention (implantation in patients that already have experienced life-threatening arrhythmias or aborted cardiac death) to primary prevention (implantation in patients with an elevated risk of arrhythmias or cardiac death who have not yet experienced such an episode). 5
Although the ICD is effective in prolonging life, it poses challenges to the patient, such as (fear of) experiencing painful shocks and feelings of helplessness, because of the unpredictable nature of the arrhythmia and subsequent shocks. 6 During the last phase of life, the benefits of the ICD may no longer outweigh these challenges and it may be important to discuss whether or not to deactivate the device. 1 However, such discussions can be challenging and complex for healthcare professionals, patients, and their relatives.
It is however unclear to what extend ICD patients experience shocks in the last phase of life, and what the impact of these shocks is, specifically at the end of life, on the patient, the patient’s relatives and the professional caregivers. Therefore, the following research questions will be addressed: (a) what is the incidence of appropriate and inappropriate ICD shocks in the last phase of life?; and (b) what is the impact of ICD shocks in the last phase of life on patients, their relatives, and their professional caregivers?
Methods
Data sources and search strategy
Research questions, search strategy and inclusion criteria were specified in advance and documented in a protocol. A search query was developed to identify relevant papers. In August 2016, we systematically searched five electronic scientific databases: Embase, Medline, Cochrane Central, Web of Science and Google Scholar. In order to find all relevant literature, we did not place a limitation on year of publication, all articles up to August 2016 were considered for inclusion. Studies were identified with the following keywords: defibrillator, defibrillator pacemaker, implantable cardioverter defibrillator, internal defibrillator, ICD, AICD; and shock, electric shock, electroshock, countershock, cardioversion, convulsive therapy; and terminal care, terminally ill patient, EOL, death, dying, palliative, hospice, last phase, last year, last month, last week, last day. Boolean operators were used in between key words. The detailed search queries can be found in Supplementary Material Appendix 1.
Study selection and eligibility criteria
Articles were reviewed by RS and AB via a stepwise procedure according to the PRISMA guidelines. 7 First, studies were screened on title and abstract. Selected studies were subsequently reviewed on full text and either included or excluded. In case of disagreement, consensus was sought and achieved. Table 1 describes the inclusion and exclusion criteria. Studies were included when they reported on deceased patients with an active ICD in the last phase of life, either on the incidence of ICD shocks or on the impact of shocks on patients, relatives or professional caregivers. The last phase of life was operationalised as the last month preceding death. This was based on a study that reported on shocks one month before death. 8 Relatives were not limited to family members but could also include others, such as close friends or other loved ones. Studies had to be written in English, and the full-text of the article had to be available. Studies were excluded when they reported on minors or were case reports. References lists from the included studies were examined to identify additional relevant studies.
Inclusion and exclusion criteria.
ICD: implantable cardioverter defibrillator.
Data extraction
Data of the studies that were included in the review were extracted via an extraction form. This form was developed by RS, AB and JR and piloted by RS and AB. The eventual data extraction was completed by RS.
The following data were extracted:
Shock incidence, where possible stratified by type of death. Type of death could be non-sudden death (NSD), defined as death occurring more than one hour after the onset of new symptoms, or sudden death (SD), defined as death that occurs less than one hour after the onset of new symptoms. 9 Shock incidence was calculated by dividing the number of patients in a specific group receiving shocks by the total number of patients in that group.
Timing of shocks, categorised in three time periods: the last month, the last 24 hours and the last hour preceding death. When a study reported on multiple time periods, patients who experienced shocks during the last hour or last 24 hours preceding death were also included in the incidence in the last 24 hours and last month before death.
Appropriateness of shocks. An appropriate shock was defined as a shock for ventricular tachycardia (VT) or ventricular fibrillation (VF). An inappropriate shock was defined as any shock not delivered for VT or VF.
Impact of shocks on either patients, relatives, or professional caregivers. All available data were extracted.
Characteristics of the study, such as year of publication, study design, aim, year of implantation, year of death, and characteristics of the participants.
Quality assessment
Methodological quality was assessed with the Quality Assessment Tool. 10 Via this tool, studies were evaluated regarding nine items: abstract and title, introduction and aims, methods and data, sampling, data analyses, ethics and bias, results, generalisability, and implications. Each criterion was scored on a four-point Likert scale, ranging from one (very poor) to four (good). In total, a summed score of 9–36 was calculated (9=very poor, 36=good). Studies with scores between 30–36 were assessed as high quality, studies with scores between 24–29 were assessed as moderate quality, and scores lower than 23 were assessed as low quality. Studies were not excluded based on their methodological quality.
Results
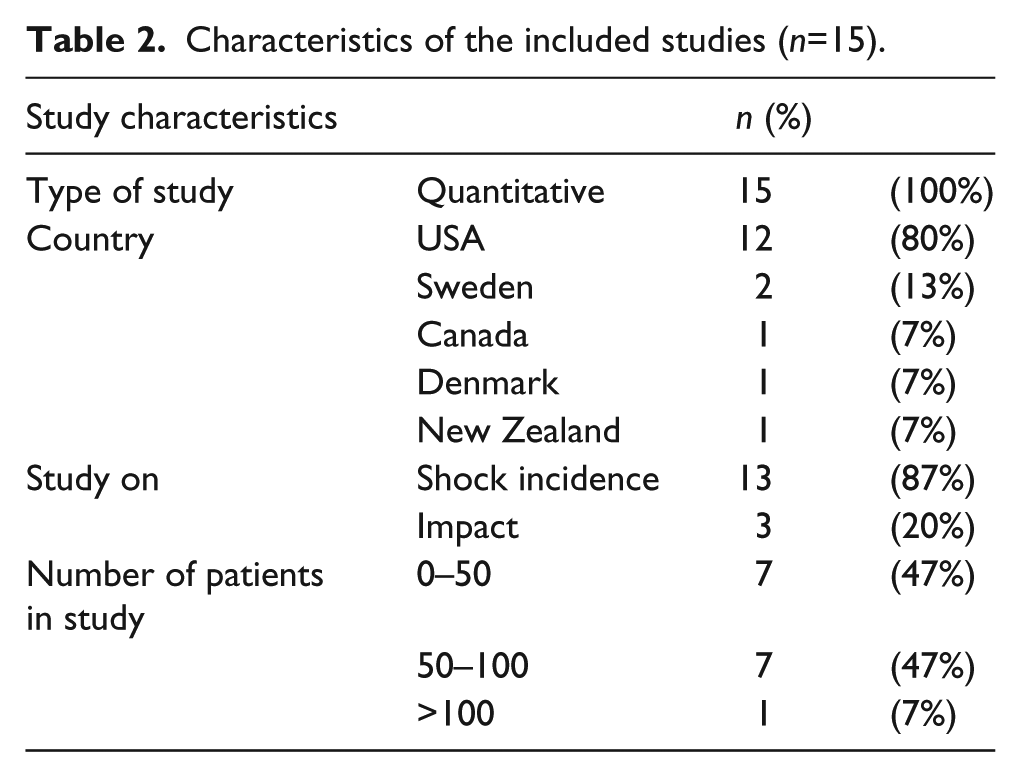
The search yielded a total of 4246 studies. We removed 1875 duplicates. All titles and abstracts were reviewed, after which 82 articles were available for full text assessment. Eventually, we included 15 studies (see Figure 1), comprising a total population of 1362 (range 4–558) patients. All studies were observational. The majority of the studies were conducted in the USA (12), the remainder in Europe (three). A total of 12 studies reported solely on shock incidence (80%), two solely on the impact of shocks (13%) and one on both the incidence and impact of shocks (7%) (see Table 2). Studies scored moderate to high on methodological quality (Tables 3 and 4). No additional studies were identified after examination of the reference lists of the included articles.
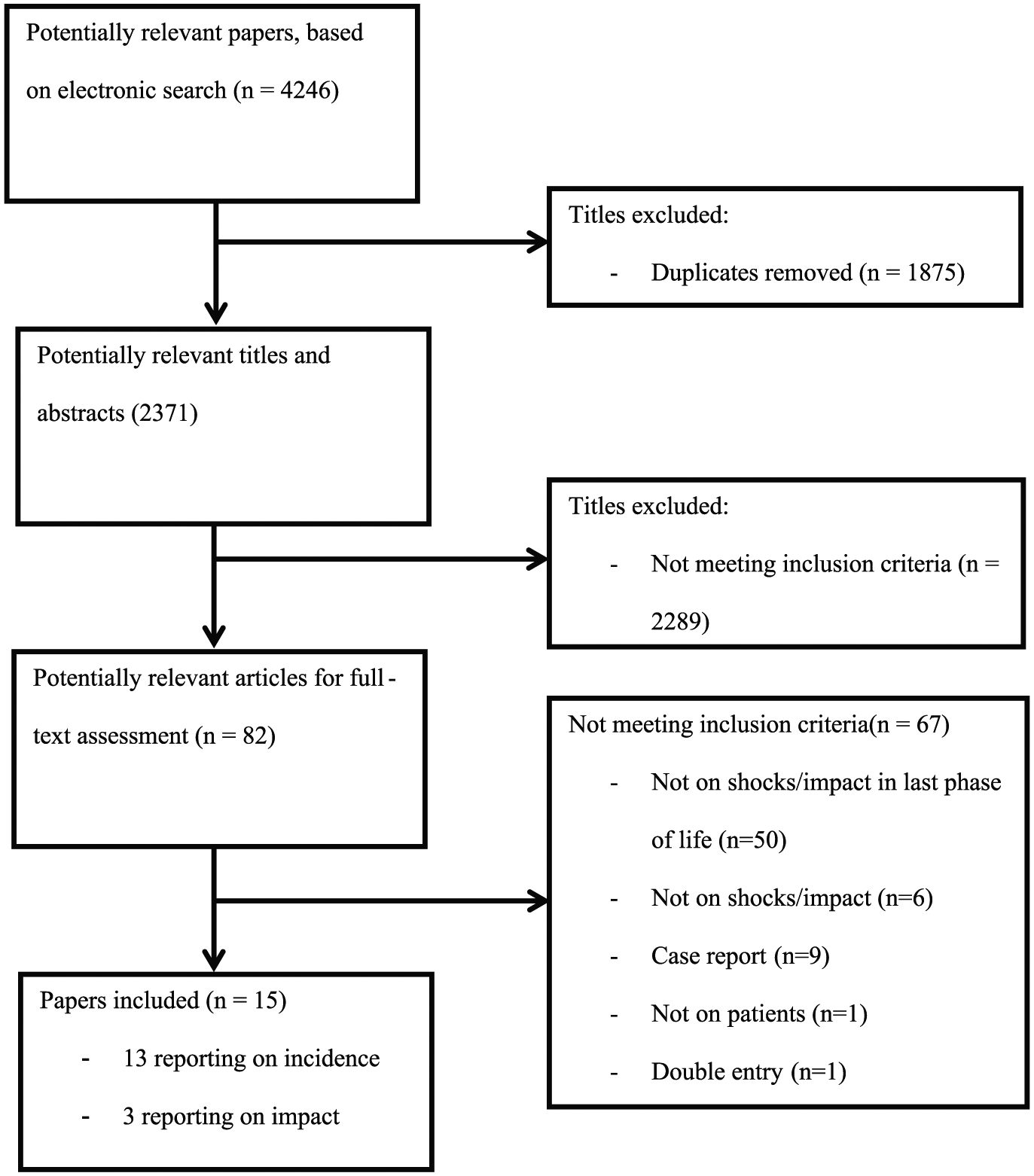
Flow diagram of literature search to identify articles reporting on the incidence and/or the impact of implantable cardioverter defibrillator (ICD) shocks in the last phase of life.
Characteristics of the included studies (n=15).
Information on studies reporting on implantable cardioverter defibrillator (ICD) shock incidence at the end of life.
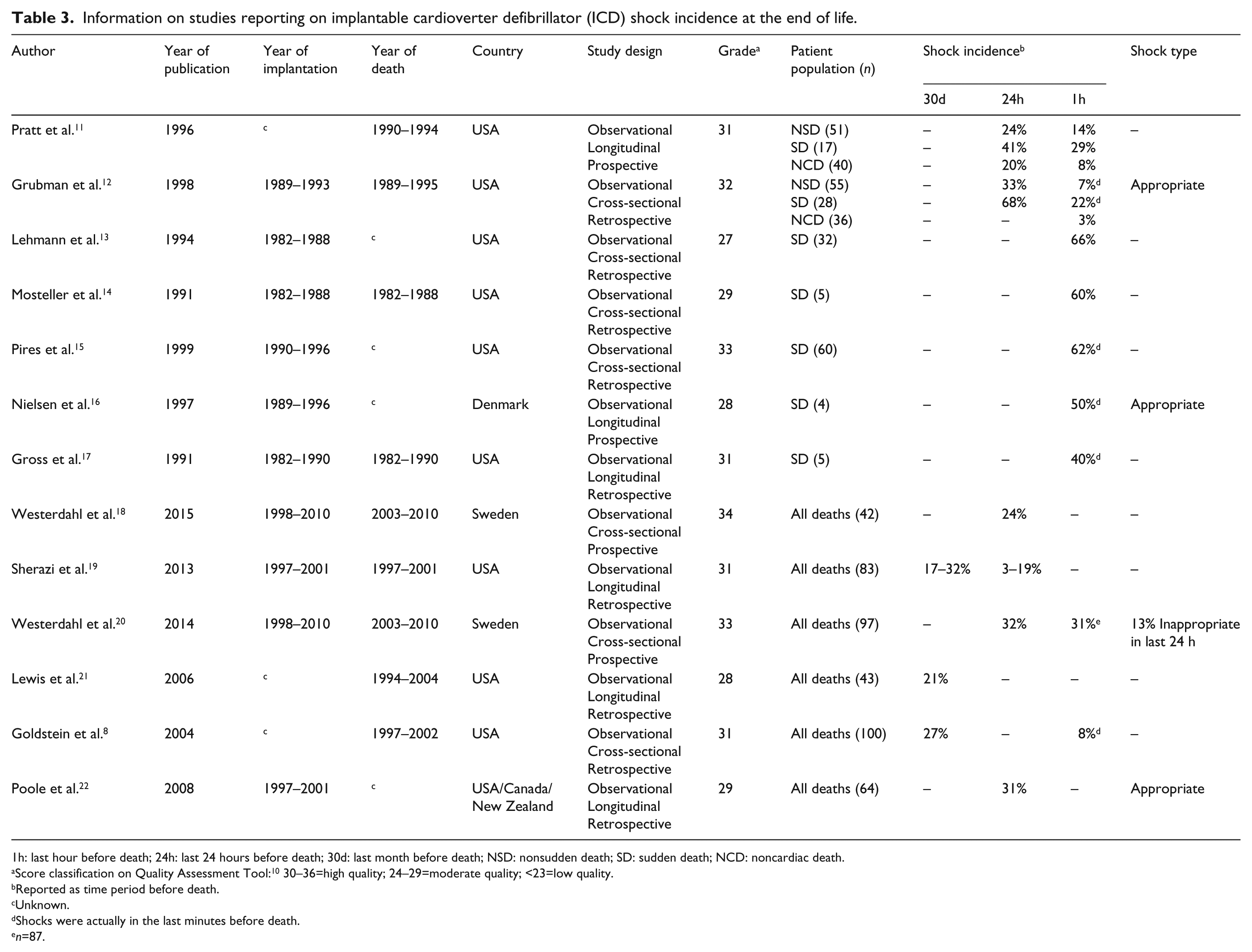
1h: last hour before death; 24h: last 24 hours before death; 30d: last month before death; NSD: nonsudden death; SD: sudden death; NCD: noncardiac death.
Score classification on Quality Assessment Tool: 10 30–36=high quality; 24–29=moderate quality; <23=low quality.
Reported as time period before death.
Unknown.
Shocks were actually in the last minutes before death.
n=87.
Information on studies reporting on implantable cardioverter defibrillator (ICD) shock impact at the end of life.
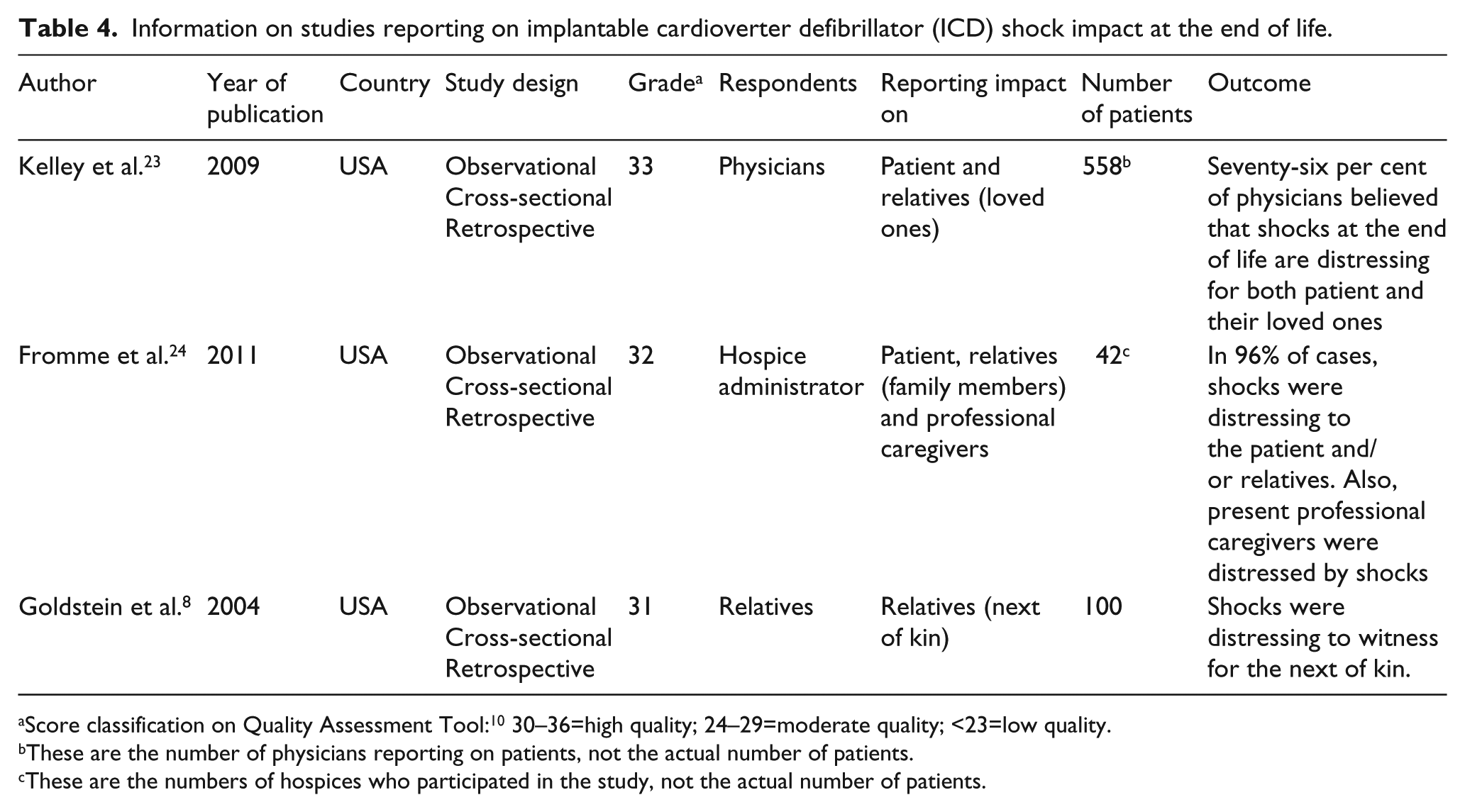
Score classification on Quality Assessment Tool: 10 30–36=high quality; 24–29=moderate quality; <23=low quality.
These are the number of physicians reporting on patients, not the actual number of patients.
These are the numbers of hospices who participated in the study, not the actual number of patients.
Incidence of ICD shocks
A total of 13 studies reported on shock incidence (Table 3). The year of publication ranged from 1991–2015. A prospective and a retrospective study, both high quality studies published in 1996 and 1998, reported on shock incidence in NSD patients.11,12 All deaths were of cardiac origin. In these studies, 24% and 33% of patients respectively experienced one or more shocks in the last 24 hours, and 14% and 7% experienced one or more shocks in the last hour preceding death. One study reported on the appropriateness of the shocks, 12 and found that all shocks were appropriate.
Seven studies reported on shock incidence in SD patients.11–17 Year of publication ranged from 1991–1999. Studies scored moderate to high on methodological quality. All deaths were cardiac of origin. Two studies reported on shock incidence in the last 24 hours preceding death,11,12 one prospective study showed an incidence of 41%, a retrospective study showed an incidence of 68%. All seven studies reported on shock incidence in the final hour of life, showing an incidence ranging from 22–66%. One study reported on the appropriateness of the shocks, 16 and found that all shocks were appropriate.
Two studies from 1996 and 1998 specifically reported on patients dying of noncardiac causes.11,12 The first study showed that 20% of patients dying of a noncardiac cause experienced shocks in the last 24 hours, and 8% experienced a shock in the last hour preceding death. 11 The second study showed that one out of 36 patients (3%) experienced a shock in the final hour of life. 12
In six studies, the type of death was not specified.8,18–22 Year of publication ranged from 2004–2015 and all studies scored moderate to high on methodological quality. Three of these studies reported that 17–32% of patients experienced shocks in the last month of life.8,19,21 Four studies showed that in the last 24 hours of life, 3–32% of patients experienced shocks.18–20,22 Two studies showed that in the last hour of life, 8% and 31% of patients experienced shocks.8,20 Two studies reported on the appropriateness of the shocks.20,22 In one study, all shocks were appropriate. 22 In the other study, 20 four of the 31 patients (13%) receiving shocks in the last 24 h were shocked inappropriately.
Impact of ICD shocks
A total of three studies reported on the impact of shocks in the last phase of life (Table 4). Date of publication ranged from 2004–2011. All studies were quantitative.8,23,24
Impact of shocks on patients
Two studies reported on the impact of shocks on patients in the last phase of life.23,24 In these studies, physicians and hospice administrators were surveyed. In the first study, physicians were asked whether they thought shocks are distressing to the patient. Seventy-six per cent agreed with this statement. 23 In the second study, hospice administrators reported that 74% of patients receiving shocks in the last phase of life were distressed by these shocks. 24
Impact of shocks on relatives
Three studies reported on the impact of shocks on relatives.8,23,24 In one study, 8 100 next of kin were surveyed. The next of kin who witnessed the patient being shocked at the end of life reported that this was distressing to see. One relative reported in an interview that the patient experienced shocks every 20 minutes at the end of life, and reported it was like seeing the patient wake up from a ‘really bad dream type of thing’, after which the patient lost consciousness again. In a survey study, 76% of physicians agreed with the statement that shocks in patients at the end of their lives are distressing for the patients’ loved ones. 23 A study in hospices reported that 92% of family members of patients receiving shocks found this distressing to witness. In one case, a patient experienced shocks during the dying process and, immediately after, the nurse had to wrap her body around the patient to stop the flailing of the body, which was distressing to witness. 24
Impact of shocks on professional caregivers
One survey study reported on the impact of shocks on professional caregivers. 24 Shocks were not only distressing for the hospice team to witness, but they must also deal with pain and panic induced by the shocks and loss of control in the patient and family. In the study, a situation was reported by a hospice administrator in which a patient was shocked multiple times during dying. The body was lifted off the bed due to the force of the shocks, which was disturbing for the nurse to witness. 24
Discussion
This review suggests that shocks in the last month of life are common in patients with active ICDs. An important finding of this review is that of patients dying non-suddenly, a quarter to a third experienced shocks in the last 24 hours of life. In patients dying suddenly, this was a third up to nearly 70%. The number of studies on the impact of shocks in the last month of life on patients, relatives and professional caregivers was limited, but they suggest that shocks are painful for the patient and distressing for patients, relatives and professional caregivers.
While the shock incidences found in this review are rather high, we found some variation between studies. There are several possible explanations for this variation. First, studies reporting on SD patients seem to report higher shock incidences than studies reporting on NSD patients.11–17 This is because patients in these studies mostly died of sudden cardiac causes, predominantly due to VT 14 or VF, 16 resulting in the ICD delivering shocks. In patients dying non-suddenly, death is less often the direct result of a tachyarrhythmia, but rather of the underlying heart disease or bleeding, resulting in the ICD intervening less often. Second, the indication for ICD implantation has shifted over time. Seven studies reported on patients who had their ICD implanted before the year 2000. In this period, ICDs were mainly implanted in patients for secondary prevention. These patients have a higher risk of recurrent VTs than patients with ICDs for primary prevention, leading to higher shock incidences. 20 From 2006 onwards, primary prevention was more often the indication for implantation than secondary prevention. 25 Only one study solely reported on patients with ICDs for primary prevention, showing that in the last 24 hours of life, 31% of patients experienced a shock. 22 This is still high, which might be due to the fact that in this particular study, patients with known sustained VT were excluded from the study, and only a single zone of therapy was used, so no antitachycardia pacing (ATP) was allowed. Third, in recent years, advances have been made to further optimise ICD programming to minimise inappropriate and appropriate therapy. 26 Developments such as ATP, longer detection times and high rate cut-offs all contribute to a reduction in shock therapy, by allowing more time for the arrhythmia to terminate spontaneously.26,27 These improvements in programming the ICD could mean that the current incidence of shocks might be lower than reported in the studies in this review. Fourth, studies we found were mainly concerned with patients dying of cardiac diseases, which might be an explanation for the high incidences as well. Only two studies specifically reported shock incidences on patients dying of noncardiac causes. Incidence in these populations seem to be lower than in the populations of NSD and SD patients.
Few studies were conducted on the impact of ICD shocks on patients in the last phase of life, their relatives and professional caregivers. From the literature on patients in earlier stages in their disease, it is known that shocks are painful and are associated with a diminished self-reported physical, emotional and social functioning, and symptoms of anxiety. 28 Although we found little detailed information on the impact of shocks in the last phase of life, this could also be the case in dying patients. In order to promote a peaceful death, quality of life should be pursued and the risk of developing symptoms of anxiety and depression should be reduced to a minimum. Timely deactivation of the ICD could help in promoting this peaceful death.
Communication between the professional caregiver and patient might be an important factor in preventing unwanted shocks at the end of life by deactivating the ICD. It has been shown that, when deactivation is discussed, a large proportion of patients decide to do so. 8 However, these conversations are rare.29,30 Professional caregivers often struggle with these conversations, because they feel they have insufficient knowledge about end of life care, 31 they feel uncomfortable discussing the topic, 32 or because they think talking about deactivation would take away hope from the patient. 33 A stronger collaboration with palliative care professionals might help professional caregivers to feel less uncomfortable initiating discussions about end of life.34,35 Also, policies can be developed for caregivers who do not frequently attend ICD patients, explaining the importance of discussing and deactivating the ICD, with specific opening questions to address the topic.1,36,37
More attention should be paid to inform the patient about the possibility of ICD deactivation, preferably starting before implantation of the device. Such discussions should be tailored to the patients’ health literacy, communication style and personal values. Physicians and nurses should be trained to obtain the necessary skills to discuss delicate end-of-life issues, such as possible deactivation of ICDs. 38
This study has some limitations. As with any review, it is possible that relevant studies were missed in conducting the search. In addition, publication bias is a possible limitation as well, leading to finding only articles which show notable results. 7 Also, included studies had relatively small study populations, only three included more than 100 participants.11,12,23 Further, seven of the 13 included studies on shock incidence were conducted 20 years or longer ago. Shock incidences might currently be lower than reported in this review, as described above. Finally, the majority of the studies were conducted in the USA, which might reduce the generalisability to a European population.
Future research on ICD management in the last phase of life should focus on determining shock incidences in both patients dying of noncardiac causes and patients dying with ICDs implanted for primary prevention, since these are not well known. Also, few studies are conducted on the impact of shocks at the end of life on patients, relatives and professional caregivers. This is a topic to be further examined. Also, it should be further examined what can be done to promote discussions before implantation and in early stages of the disease.
Conclusions
This is the first integrated review on the incidence and impact of ICD shocks in the last phase of life, providing a thorough overview of all the available evidence on these topics. Shocks were found to occur commonly, both in patients dying non-suddenly and patients dying suddenly. Shocks are painful and distressing for patients, but also distressing to witness for relatives and professional caregivers. The evidence summarised in this review should raise awareness among healthcare professionals of the negative consequences of having an active ICD at the end of life. Our findings emphasise that it is important for healthcare professionals to discuss ICD deactivation with the patient in an early stage of the disease. This can contribute to a timely deactivation of the ICD, and therefore can minimise possible suffering due to shocks and help promote a calm and peaceful death.
Supplementary Material
Supplementary_Material, Supplementary_Material – The incidence and impact of implantable cardioverter defibrillator shocks in the last phase of life: An integrated review
Supplementary_Material, Supplementary_Material for The incidence and impact of implantable cardioverter defibrillator shocks in the last phase of life: An integrated review by Rik Stoevelaar, Arianne Brinkman-Stoppelenburg, Rohit E Bhagwandien, Rozemarijn L van Bruchem-Visser, Dominic AMJ Theuns, Agnes van der Heide and Judith AC Rietjens in European Journal of Cardiovascular Nursing
Footnotes
Acknowledgements
The authors would like to thank GB de Jonge, biomedical information specialist at the Erasmus MC University Medical Center Rotterdam, for helping with developing and conducting the search strategy for this review.
At the end of life, a potentially significant proportion of implantable cardioverter defibrillator (ICD) patients experience shocks. ICD shocks are painful and distressing for patients. ICD shocks are distressing to witness for bystanders. The topic of deactivation should be discussed in a timely manner, and frequently, to promote a calm and peaceful death. Current incidence of shocks needs further study.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Netherlands Organization for Health Research and Development (grant number 80-84400-98-076).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.