
Abstract
Background:
Although patients may experience a quick recovery followed by rapid discharge after percutaneous coronary interventions (PCIs), continuity of care from hospital to home can be particularly challenging. Despite this fact, little is known about the experiences of care across the interface between secondary and primary healthcare systems in patients undergoing PCI.
Aim:
To explore how patients undergoing PCI experience continuity of care between secondary and primary care settings after early discharge.
Methods:
The study used an inductive exploratory design by performing in-depth interviews of 22 patients at 6–8 weeks after PCI. Nine were women and 13 were men; 13 were older than 67 years of age. Eight lived remotely from the PCI centre. Patients were purposively recruited from the Norwegian Registry for Invasive Cardiology. Interviews were analysed by qualitative content analysis.
Findings:
Patients undergoing PCI were satisfied with the technical treatment. However, patients experienced an unplanned patient journey across care boundaries. They were not receiving adequate instruction and information on how to integrate health information. Patients also needed help to facilitate connections to community-based resources and to schedule clear follow-up appointments.
Conclusions and implications:
As high-technology treatment dramatically expands, healthcare organisations need to be concerned about all dimensions of continuity. Patients are witnessing their own processes of healthcare delivery and therefore their voices should be taken into greater account when discussing continuity of care. Nurse-led initiatives to improve continuity of care involve a range of interventions at different levels of the healthcare system.
Keywords
Introduction
Achieving continuity of care poses important challenges for healthcare systems due to rapid technological advances, new treatments, increased specialisation and shifts in care from institutional to community healthcare services. 1 Delivering good healthcare is consistent with an international effort to maintain and enhance continuity of care within the entire healthcare system. 2 Despite this fact, few studies have investigated cardiac patients’ experiences of care across the interface between secondary and primary healthcare systems.3,4
It is widely believed that continuity is essential for achieving high-quality patient care. 5 Continuity has been defined in numerous ways, yet there is no consensus on the definition of the concept. Haggerty et al. 6 identified three types of continuity: informational, management and relational continuity. Informational continuity refers to use of information (medical and personal) to provide appropriate client care over time. Management continuity refers to the measurement of the cohesiveness of care delivery from multiple healthcare providers. Relational continuity refers to the ongoing relationship between a patient and their healthcare providers.
Percutaneous coronary intervention (PCI) involves opening stenotic or occluded arteries by expanding a balloon in the stenotic artery, usually followed by insertion of a stent. It is the most commonly performed revascularisation method among cardiac patients.7,8 Recent advances in medical treatment have resulted in reduced mortality in the acute stage of the illness, and this is usually accompanied by earlier discharge of the patient from hospital. 8 Thus, taking care of the patient in primary healthcare following discharge requires a different competence. There are few studies assessing these issues. 9 Discharge from hospital to home is a critical time for patients because they need to adjust their lifestyle, incorporate new medication and acquire new support and an expanded care team. 8 Patients are particularly susceptible to further cardiac events and effective secondary prevention is very important. 10
Qualitative meta-summaries of patients’ experiences conclude that some dimensions of continuity, such as coordination and communication among clinicians, are best assessed by patients.11,12 Furthermore, these studies showed that patients experienced negative relationships with healthcare providers, poor communication and difficulties in progressing through the system, and that they received insufficient information about further policy and follow-up appointments.9,11–15 It seems that the first weeks after discharge are difficult for patients, and it is important that care is coherent and consistent with their medical and psychosocial needs.5,16 Few studies have analysed patients’ experiences of continuity of care in a comprehensive manner, and they typically have focused on only one type of continuity or one care level.1,16 Therefore, the aim of this study was to explore how patients undergoing PCI experience continuity of care between secondary and primary care settings after early discharge.
Methods
Design
The study had an inductive exploratory design, 17 and semi-structured interviews were conducted between March and September 2015.
Patients
A purposive sample of 22 patients from one tertiary PCI centre in Western Norway participated
Demographics and clinical characteristics of patients after percutaneous coronary intervention (PCI) (N = 22).
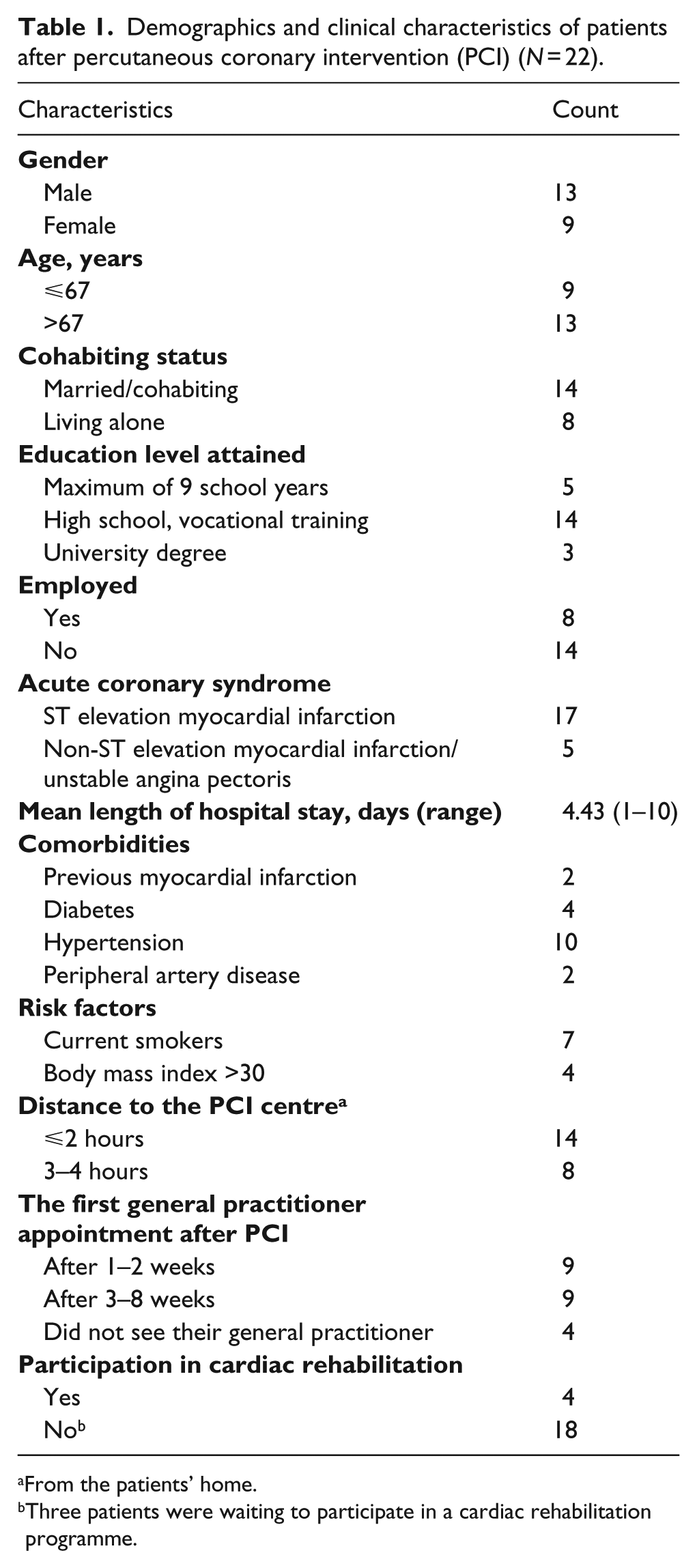
From the patients’ home.
Three patients were waiting to participate in a cardiac rehabilitation programme.
Inclusion criteria were patients undergoing first-time PCI intervention 6–8 weeks previously, ⩾18 years old and living at home. Patients who previously had undergone cardiac surgery were excluded from the study. The time interval was chosen to ensure time for follow-up care so patients could provide an adequate evaluation of early post-discharge continuity of care. Non-Norwegian-speaking patients and those lacking capacity to consent to research were not included. Patients fulfilling the inclusion criteria were identified through the Norwegian Registry for Invasive Cardiology (NORIC).
Data collection
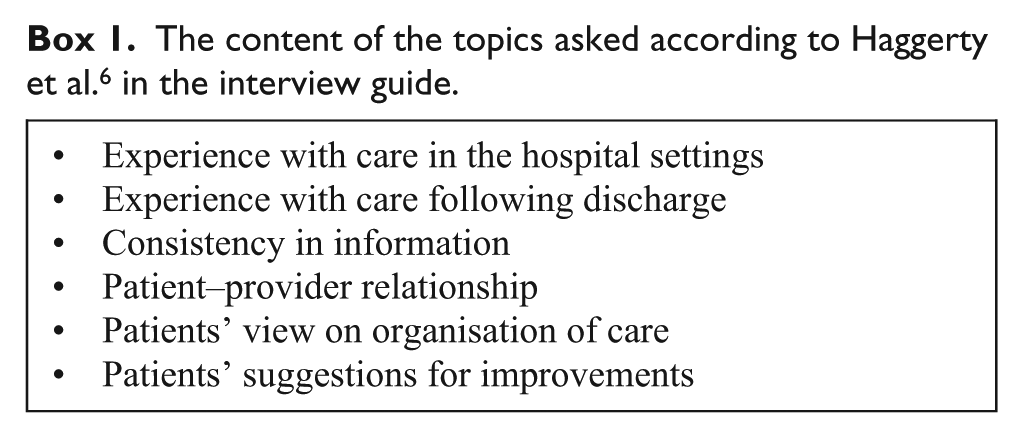
A semi-structured interview guide was developed from the authors’ clinical experience and from previous research on continuity and follow-up care of other patient populations.14,18 Development of the interview guide was guided by Haggerty et al.’s 6 definition of continuity of care (Box 1). The interview guide was slightly modified after performing two pilot interviews. Information letters about the study, including an invitation to participate, were sent by post to patients meeting the inclusion criteria. Reminders were sent after 2 weeks for non-responders, and after another 2 weeks, alternative patients of similar age and gender were invited to participate. This process was repeated until a sufficient sample size was reached that included sufficient richness, experiences and relatedness to the research questions. Interviews were conducted in the patients’ homes or meeting rooms, depending on the patients’ preferences. The first author carried out all of the interviews. The durations of the interviews were from 45 to 60 minutes, and they were audio-recorded and transcribed.
The content of the topics asked according to Haggerty et al. 6 in the interview guide.
Data analysis
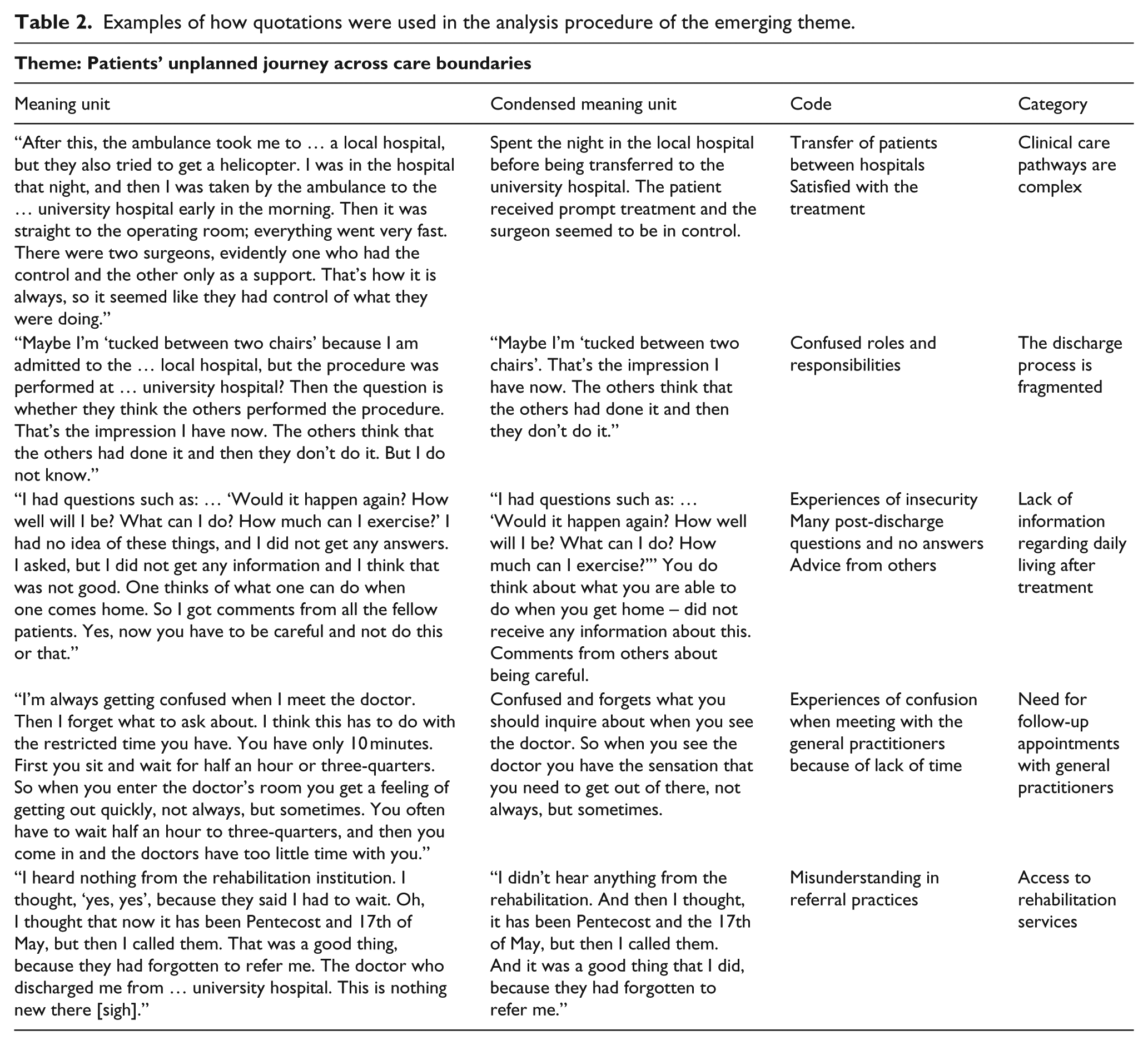
Qualitative content analysis according to Graneheim and Lundman was used. 17 An inductive approach was undertaken within a perspective of a hermeneutic interpretive paradigm. In our analysis, categories are seen as representing the manifest content (i.e. the content aspect) and themes represent the latent content, which can be seen as the relationship aspect. 17 The process of analysis involved a consideration of the whole transcript and parts of the transcript, moving repeatedly between these two levels in order to gain meaning. Each audiotaped interview was listened to twice and its transcript read through several times in order to obtain a sense of the whole. The text was divided into condensed meaning units that corresponded with the study aim. The condensed meaning units were abstracted and labelled with a code while preserving the whole context. Statements that appeared to be similar were grouped together and sorted into categories, and finally a theme emerged reflecting the bigger picture (Table 2). The first author also discussed the entire analysis process with the co-authors until consensus was reached.
Examples of how quotations were used in the analysis procedure of the emerging theme.
Ethical considerations
The ethical guidelines of the World Medical Association, Declaration of Helsinki and the laws in Norway guided the study (Declaration of Helsinki, 2008). Patients gave written informed consent regarding participation. Approval by the Norwegian Regional Committee for Ethics in Medical Research was granted (REK 2015/57).
Findings
Continuity of care within the healthcare system was experienced in different ways by the patients. The main theme was described as an unplanned patient journey across care boundaries. Patients undergoing PCI described the importance of receiving clear information on follow-up appointments and support in order to organise the care journey. These aspects were characterised by five categories (Table 2) and each of these categories will be presented individually using representative quotations in order to highlight important findings.
Clinical care pathways are complex
The clinical care pathways for patients were quite different depending on whether their PCI procedure was planned or acute. The elective patients had experienced the waiting time before the procedure as being frustrating and stressful. In particular, patients with chest pain were afraid to die if they waited too long. Patients who were brought directly to the PCI centre – usually by ambulance or helicopter – were more satisfied with the clinical pathway. They valued a smooth-running pathway, healthcare providers who always knew what to do and a clear division of tasks.
“An air ambulance took me to the university hospital and landed on the roof. Then, it was straight down to the operation, and then I was fixed. Everything went very fast. I was impressed in how fast it went.” (Woman, 77 years old)
Patients were satisfied with the technical treatment they received and felt safe and well cared for. The patients emphasised the importance of healthcare providers working as a team during the PCI procedure.
“Then, there was a team waiting for me. I was very impressed by this and of how they cooperated. One person of the healthcare providers did this and the other person that.” (Man, 71 years old)
After PCI, patients were transferred to the ward for further follow-up. Patients described stressful hospital environments where healthcare providers had little time to care for each patient. The pressure of the daily schedule sometimes made it difficult for healthcare providers to pay attention to the special needs of individual patients. Patients did not always understand who was in charge and what service to expect from whom and when. Patients who were hospitalized for an acute cardiac event were surprised by what had actually occurred. Patients were relieved by being free of symptoms and found it difficult to understand what they had been through. Furthermore, they were surprised that the PCI was so smoothly performed and that they did not need a longer hospital stay.
The discharge process is fragmented
Patients were often dissatisfied with the discharge process and wished that it had been better organised. Nurses were empathic and supportive, but patients had problems with describing their responsibility in the discharge process.
“It is a bit difficult to know who is a nurse and who is a physician. I try to see if they have a white coat, but they all wear the same uniform. However, they all say the same thing; that I do not have to worry about anything.” (Man, 49 years old)
The discharge encounter with the physician was short and often carried out in busy hospital corridors, to the dislike of patients.
“Doctors are also very busy, because you know they put a lot of pressure on themselves. You know they come running at full speed, and then you have to wait for several hours for them to visit you … Then, oh well, ‘thank you and goodbye.’” (Man, 49 years old)
There were patients who were transferred to their local hospital after treatment without receiving a final discharge letter. They argued that the various hospitals were not coordinated and this led to a lack of clarity in matters concerning responsibility.
Elderly patients felt especially vulnerable, powerless and confused.
“I have not seen a single paper, and it’s something that makes me disappointed. They haven’t given me any documentation or a written report … there is no communication, and that’s annoying me.” (Man, 80 years old)
Discharged patients who had to travel long distances thought that their transportation was inadequately planned.
Lack of information regarding daily living after treatment
Patients with fewer symptoms after discharge experienced their homecoming as being less problematic. Furthermore, patients going through planned PCI was more informed. However, patients felt unprepared during their early recovery and had a feeling of uncertainty about how to live after the PCI. Patients found the discharge instructions and precautions after treatment uninformative. They had received little information about their diagnosis, the PCI procedure, medication and technical matters, but even less information about the consequences of cardiac disease. The information received at hospital was superficial and sometimes difficult to implement in a practical way in everyday life.
“I did not know how much I could push myself. There was no discussion about these things, I was supposed to live normally. What is normal? Can I cut the lawn?” (Woman, 69 years old)
There were patients who were disappointed by the significant physical setbacks they experienced after their cardiac event.
“I felt awfully tired; I do not know how to describe it. I came home from work and was supposed to make dinner, but instead I was just hanging over the kitchen table. I was exhausted, but I did not feel any pain.” (Woman, 58 years old)
They wished the healthcare providers had informed them about symptoms or health problems to be aware of after discharge. Partners supported patients to facilitate continuity of care. However, patients described that they had to call friends and acquaintances that work in healthcare in order to get answers to their questions. Patients felt that they had to coordinate their own care.
“It’s sort of … we needed to take initiative ourselves constantly. If I had not discussed these things with other patients who had been at the hospital for the same reason and gone through the same PCI procedure as me, I would not have known anything about what would take place afterwards.” (Man, 68 years old)
They also called the hospital to clarify questions regarding treatment. Patients used information from newspapers or the internet in making decisions. There were patients who downloaded apps to help them make lifestyle changes. Patients who advocated for themselves were not always happy about such a role. They felt too ill to make their own choices and felt incapable of doing so.
Need for follow-up appointments with general practitioners
The first follow-up appointments with patients’ general practitioners (GPs) were not always arranged for them, and there were patients who had not visited their GPs, even by 8 weeks after their PCI.
“I haven’t spoken to anyone. I was discharged late April, and now we are almost tucked into the end of July. So I think it is strange that I have not received any call from the hospital for checking how I’m doing. But it is possible that this is not the routine.” (Woman, 80 years old)
There were patients who mentioned that their GPs were not fully up to date on their hospital treatment. Patients also felt that the information given by the GP was not always complete.
“The GP is not aware of my situation at all. No, she is not. The first thing she said was: ‘You use beta-blockers? Why do you not have beta-blockers?’ … Then, you know, I don’t know how to answer. But I was given a partial explanation from the cardiologist.” (Man, 49 years old)
Patients were insecure about the GP’s role and responsibility in following up after PCI. They were annoyed at the GPs because their cardiac disease was not discovered earlier and because they also expected them to prevent the disease more actively when the patient had a clear family history of cardiac disease. Furthermore, GPs had too little time for conversation and did not sufficiently help the patients with what changes to make and how to make lifestyle changes. There were patients who found it difficult to see the same GP.
“I think I’ve had 15 or 16 family doctors or something like that. I never know who my doctor is. They are often doctors in training who are trying to get more clinical experience.” (Man, 53 years old)
Patients commonly described problems in changing their GPs, particularly in rural areas where few were available. However, there were patients who were satisfied with their GPs and trusted their advice. Good communication abilities and interpersonal skills were important to patients.
Access to rehabilitation services
Patients who were offered rehabilitation expressed the greatest satisfaction with their follow-up after discharge. Rehabilitation sessions were valuable opportunities to discuss the patients’ concerns and to help them establish control over their lives and illness experiences. However, there were patients who did not receive information about cardiac rehabilitation, neither from the hospital nor from their GPs. They were disappointed about being denied appropriate care and believed that rehabilitation should be part of their treatment.
“I have not heard anything about rehabilitation – nothing! The only thing they said was that I had to call if I got symptoms like palpitations or pain. No, I have received no information or heard anything.” (Man, 53 years old)
The rehabilitation services across geographical locations varied, and location seemed to be an important factor in determining whether patients decided to attend or not. Patients also reported feeling frustrated about misunderstandings regarding referrals to cardiac rehabilitation and about long waiting times for rehabilitation.
“Why does it take so long before you can take part in the rehabilitation programme, then? It takes 3 months … I should have travelled straight to the rehabilitation institution after my hospital stay. I was motivated at that time.” (Woman, 46 years old)
There were patients who thought that the rehabilitation services were too extensive and preferred shorter treatment plans, e-health programmes and internet-based education in order to allow rehabilitation at home.
Discussion
The aim of the study was to explore how patients undergoing PCI experience continuity of care between secondary and primary care settings after early hospital discharge. This study provides empirical support for Haggerty et al.’s model of continuity of care drawn from patients’ experiences. 6 There is a growing recognition that healthcare providers can learn from patients, and patients’ experiences are increasingly being recognised and valued.11,13
Patients’ experiences of management continuity
Challenges in management continuity were brought about by a longer distance to the PCI centre. The clinical pathways were more complex as they involved multiple healthcare providers in a variety of settings. This sometimes led to discontinuity because of vague descriptions of who was responsible for what across different healthcare settings. Patients were unsatisfied with their discharge process, and discharge conversations were poorly planned. Nurses checked blood pressure, electrocardiogram and pulse many times during the patients’ stays in hospital, but these patients could not remember the nurses talking about discharge preparation. 19
Previous research in other patient groups shows that appropriate continuity of clinical management exists when healthcare roles are clearly defined and distributed across levels and when coordination and communication is good among healthcare providers.20,21 Preparation to return home and effective discharge planning after hospitalisation is part of continuity of care, 22 and this is increasingly viewed as being important, considering the trend towards shorter hospital stays. 23 Another study showed that hospital staff do not continue care after patients are discharged, mainly because they lack understanding and interest in post-discharge care activities. 16 In addition to this is time pressure in hospital.16,24 According to Haggerty et al., 6 patients are increasingly seen by an array of healthcare providers in a wide variety of organisations and places, thus raising concerns about fragmentation of care. It is important in shared care protocols to facilitate management continuity, which provides a sense of predictability and security for both patients and healthcare providers.
Our study revealed that not everyone is referred to rehabilitation, either by the hospital staff or by their GPs, and there were patients who experienced a system failure that delayed their rehabilitation. Furthermore, living long distances from centres and limited access to cardiac rehabilitation may be reasons why patients do not participate in rehabilitation programmes. 25 Multifactorial reasons contribute to patients failing to attend rehabilitation programmes, such as issues related to the healthcare system, to the healthcare providers and to the patients themselves.25,26 Hospital-based interventions that promote automatic referrals have a significant, positive impact on referral rates. 27 Furthermore, physicians’ endorsements and involvement enhance patient referral and enrolment in cardiac rehabilitation.8,28 Our study confirms that patients require more flexible systems that provide access to rehabilitation and other supportive services matching their needs.29,30 According to Haggerty et al., 6 flexibility in adapting care to the changing needs of patients is an important aspect of management continuity.
Patients’ experiences of information continuity
Patients going through planned PCI seemed more informed about the procedure than patients admitted for primary PCI. However, patients were unprepared after hospital discharge. Despite differences in patients’ wishes for how much information they desired, there were patients who stated that they were discharged without understanding their cardiac condition. Patients were advised to ‘live as they normally do’, but the patients felt uncertainty and expected additional guidance. The shortened hospital stay and emotional strain that patients experience have consequences on their ability to perceive information. 31 In addition it is difficult to achieve continuity through standardised processes. 13 Teaching methods should be tailored for each patient, and nurses are in a unique position to educate patients on the importance of modifying cardiovascular risk factors. 32 Haggerty et al. 6 claim that informational continuity refers to the use of information regarding past events and personal circumstances to make current care more appropriate to each patient.
By itself, information given to patients is insufficient to link components of care; this information must be discussed and reflected on in order to be effective. Our study shows that patients sometimes have to coordinate their own care. Consistent with other studies, there were patients in our study who reported that they obtained information from different sources, although it is understood that patient participation is a critical aspect of continuity of care in general.13,30 Consequently, healthcare providers need to ensure that patients are prepared to carry out their role in coordinating post-discharge care. 11
Patients’ experiences of relational continuity
The relationship between patients and healthcare providers is influenced by the organisational context. Patients were satisfied with the healthcare providers’ interactions during PCI treatment; however, they experienced different barriers to communication in hospital ward settings. Patients did not distinguish between communication with nurses and physicians in hospital. However, patients maintained that it was of utmost importance that healthcare providers showed them respect and took time to listen to them and explain matters to them. Nurses are in a key position to recognise patients’ needs and to pay attention to patients in order to build a therapeutic relationship. 33
Patients who visited healthcare centres in more rural areas experienced lower relational continuity. Standard follow-up usually consists of visits to GPs, but patients did not always meet with their GPs on a regular basis because of staff turnover and rotation. Furthermore, patients themselves had to take the initiative and organise an appointment, and sometimes it took several weeks for patients to meet with their GP. It is possible that patients should have been booked automatically to their GPs early after discharge from hospital. Consistent with current knowledge, relational continuity is hindered when patients find it difficult to consult with their assigned GPs. 34 These circumstances led to contradictory advice, and patients became confused about which advice to follow. 35 As a response to a general shortage of GPs, it is possible that cardiac nurses in primary care could pick up some of the slack in the health and care services. 36
There were patients who also lacked confidence in their physician and did not always believe that their physician had the ability to make the right care decisions. Patients perceive continuity as relational when there is trust and confidence in the relationship, maintaining and developing good continuity of care. 5 Furthermore, good adherence to treatment and patient satisfaction are enhanced as a result of relational continuity. 35 According to Haggerty et al., 6 even in contexts where there is little expectation of establishing ongoing relationships with multiple caregivers, the presence of a consistent core of healthcare providers gives patients a sense of predictability and coherence.
Methodological considerations
The trustworthiness of qualitative content analysis is often discussed in terms of credibility, transferability, dependability and confirmability. 17 To achieve credibility, we used qualitative content analysis to interpret variations through identifying differences and similarities in the content. The patients differed in age, gender and experiences, which contributed to variability in the phenomenon under study. Nevertheless, the patients only came from one hospital, which may be a limitation regarding transferability. On the other hand, this was a large tertiary university hospital, generating different care pathways. To strengthen the dependability of the results, the first author carried out all of the interviews and described the analytical process in great detail. All authors were familiar with the subject area and with the methodology employed. During the interview, the first author asked questions in order to verify her understanding of what the patient was saying. In addition, a brief summary of the interview was discussed with each patient. To achieve confirmability, all of the recommended steps in the analysis process of Graneheim and Lundman were followed. 17 Because the authors were aware of the possibility of being biased from their prior understanding of the topic, reflections on the content were all written down during the data analysis. Furthermore, dialogue with the co-authors reduced potential misinterpretation. In order to ensure objectivity, the authors participated in ongoing discussions throughout the analysis. In order to achieve transparency, every step was described in the analysis process with representative quotations from the transcribed text.
Conclusions
In recent years, cardiac care has undergone a significant change as high-technology treatment dramatically expands. A main finding has been that patients undergoing PCI find it challenging to move across the boundaries and each type of continuity – informational, management and relational – which has an important impact on a patient’s experience of how care is connected. Patients were satisfied with the technical treatment they received, but they experienced discontinuity of care when it came to discharge planning, follow-up appointments with GPs and access to cardiac rehabilitation. This study highlights the current deficiencies in continuity of care, and that nurses and other healthcare providers need to pay more attention to issues of service–system organisation in order to meet patients’ needs. The number of alternative services and the complexity of general practices should lead to a growing role of nurses and other healthcare providers in primary care. The framework of continuity of care can be useful when planning effective management of cardiac disease. Nurse-led initiatives to improve continuity of care involve a range of interventions at different levels of the healthcare system. However, it is important to focus on more personal care planning, interdisciplinary teamwork and self-management programmes.
Footnotes
Acknowledgements
The authors thank the patients who shared their experiences. We would also like to thank Sogn og Fjordane University College and NORIC for supporting this project, and the PROCARD research group and colleagues for being important discussion partners.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The study was financially supported by Sogn og Fjordane University College, Norway.
Understanding how patients experience their journey through the healthcare system is critical for improving continuity of care. Discharge planning and systematic follow-ups shortly after discharge are increasingly viewed as being important. Cardiac rehabilitation should be flexible in order to meet patients’ individual preferences and should be an integral part of acute care. Nurses should take a more active role in coordination of care between healthcare settings. Knowledge sharing and interdisciplinary collaboration across boundaries are important to continuity of care and should be part of a nurse’s role and competence.