
Abstract
This paper reconstructs a fragment of psychiatric-psychoanalytical geography, interfacing it with the ‘new walking studies’, centring on a walk conducted in 1935 by a man experiencing mental health problems in Glasgow, Scotland. This man, a patient of the psychiatrist Thomas Ferguson Rodger, had mobility problems that rendered walking difficult – prone to stumbling, staggering, wavering – but with the likelihood of these problems being psychosomatic in origin. Through analytic sessions enacting a kind of ‘make-do’ psychoanalysis, the patient reflected on his mobility problems, as when relating his own walking ‘experiment’. Explanations advanced for his difficulties mixed psychoanalytic tropes with a gathering self-awareness of how fraught childhood experiences, had created the frame for an adult existence continually shying away from wider encounters and challenges beyond the domestic sphere. Central here was forward momentum being lost, whether walking or advancing through a life-course, with material and metaphoric senses of being stalled or stuck – spatially, environmentally – constantly entraining one another. This case study is deployed to illustrate claims about the ‘worlding’ of psychoanalysis, and to offer provocations for how such a psychiatric-psychoanalytic geography fragment might be illuminated by work on the cultural geographies of walking.
The history of walking is an unwritten, secret history whose fragments can be found in a thousand unemphatic passages . . .
1
Introduction
On 21st January 1935, a man went for a walk in the West End of Glasgow. An unremarkable walk, if completed awkwardly, it acquired significance for the man as a ‘patient’ striving to understand his difficulties through analytical sessions with the Glasgow psychiatrist Thomas Ferguson Rodger (1907–1978). 2 This excursion was minutely recorded in a three-page account entitled ‘A Walk 21/1/35’, an accompaniment to an update on the patient’s condition dated 23rd January 1935, both of which were authored by the patient and survive in the Rodger papers at the University of Glasgow Archives (Figure 1). 3 Other attempts at locomotion by the man were detailed, together with his reflections – occasionally glossed by Rodger – tracing plausible origins of his movement impairments in the psychodynamics of earlier life. While not following the letter of Freudianism, and clearly inflected by a psychiatric training and ‘day job’ in Glasgow’s mental hospitals, Rodger’s aim was still to enlist the patient in their own self-analysis. Moreover, Rodger was deeply concerned with psychiatry in its socio-environmental contexts, 4 a concern intensified by his war-time experiences and manifested in a post-war advocacy of community-based psychiatry beyond ‘the asylum’. This concern also shaped a readiness to set his interwar patients – and to encourage his patients to do the same – in the everyday spaces of their routine social lives. ‘A Walk 21/01/35’ entailed just such a tiny brush with worldly geography.
Some ‘Dream Books’.
In 2019 cultural geographer and trained psychotherapist Liz Bondi wrote about going for a walk taken at least once a week over several years, leaving her university office and journeying to the site of the counselling agency where she runs sessions. 5 She reflects on the changing seasons, the changing mixtures and textures of peoples, surfaces, plants, colours and light, and on the ‘interface between an external environment and internal experience’, asking about ‘how my walking contributes to my practice as a counseller/psychotherapist (I use the terms interchangeably)’. 6 Wondering critically about the connections between psychotherapy and ‘psychogeography’, she deduces that ‘[t]he sense of inner spaciousness I experience on my journey . . . speaks to my capacity to symbolise feelings or emotions sensed in and through my body’. 7 Peppering her account with references to different schools of thoughts within psychoanalysis/therapy, namechecking Freud, Winnicott and Bion, her essay suggests an eclectic engagement with wider constellations of ‘psy’ theorising and practice, an eclecticism perhaps akin to what Rodger brought to his consulting room as attended by the 1935 perambulator. Her approach ‘is simultaneously internal and external, always apprehended through my psyche-soma’, a concept borrowed from Winnicott to scramble the Cartesian mind-body dualism and preceded by Freud’s model of the ‘body-ego’, regarding ‘the unconscious as necessarily bodily’. 8 Bondi foregrounds her feelings as inflected by her familiar yet never identical ‘micro-journey’, interpreting what it means for and enables in her counselling role, but she also indicates how her approach opens to similar embodiments of psychodynamic processes displayed by her clients: ‘Just as I deployed my senses on my journey here, so I use my senses again now I am with my client. . . . I observe, noticing details such as how my client comes into and occupies this space’. 9 Running the man’s walk in 1935 alongside Bondi’s walk encapsulates key themes of our paper to follow: the entanglements of walk, world and psyche; the pertinence for matters of therapeutic encounter and intervention; the eclecticism of the ‘psy’-disciplines in how they may sometimes be practised; and diverse possibilities for bringing into touching-distance human geography’s ‘psychoanalytic turn’ with work on the cultural geographies of walking.
Our paper only focuses on a small aspect of the wider intellectual landscapes indexed here, and at the outset we acknowledge a wish to stay close to the rich empirical materials associated with ‘A Walk, 21/5/35’, to build from within them rather than piercing them throughout with word and concept from secondary literatures. Some further orientating remarks are nonetheless needed, beginning with our first departure-point in academic geography’s so-called ‘psychoanalytic turn’ since the mid-1990s. 10 This turn has entailed adopting a variety of psychoanalytic concepts (Freudian, Winnicottian, Lacanian) to explore phenomena such as geopolitics, urbanisation, ruination and more, 11 as well as considering the emotional relationalities outworked in micro-spaces of psychotherapeutic encounter. 12 Actual mental ill-health has figured marginally in this turn, with fewer links than might be anticipated to the subfield of mental health geographies, 13 but a key manoeuvre in this respect is what Cheryl McGeachan calls the ‘worlding’ of psychoanalysis. 14 She draws inspiration from how the Scottish psychiatrist R.D. Laing retained a psychoanalytic orientation, but siphoned its insights from the recesses of the unconscious to illuminate – and to show how in return the unconscious is shaped by – everyday socio-spatial worlds full of the fuss and bother of humans (and objects) interacting well or badly. Such a perspective chimes with Bondi’s essay, which references Laing’s notion of ‘ontological insecurity’ arising when an ‘outer reality’ challenges inner constructs of how things are and should be. 15 Tellingly, Laing remained a psychiatrist, even as he critiqued the conformity-inducing dimensions of psychiatry within a capitalist social order, 16 and he was always concerned to interact with the disturbed, often schizophrenic, patients presenting before him. McGeachan explores numerous of Laing’s cases, 17 and it is in the spirit of her inquiries that we address below our empirical ‘fragment’ of psychoanalysis-meeting-psychiatry-meeting-geography, while also – also echoing McGeachan – contributing to literature on the historical geographies of the ‘psy’-disciplines. 18
A second departure-point is work on the cultural geographies of walking, particularly in the guise of what Lorimer has called the ‘new walking studies’, a ‘term point[ing] towards a marvellously eclectic array of walking-thinking-practices’. 19 This journal, cultural geographies, has carried numerous papers in this vein: some on how articulations of literature, reading and walking resonate with place and landscape 20 ; some on the political-aesthetic ‘arts of exploration’ experimenting with how walking, individually, in installations or on ‘walking tours’, can illuminate or subvert established socio-spatial orders 21 ; and some on walking routes, pilgrimages or marches that deepen spiritual or ethical entanglements with both the ‘good’ of holy places and the ‘bad’ of threatening, violent, even genocidal ones. 22 A pioneering paper by Wylie, based on experiences when walking the British South West Coast Path, examines how ‘self-landscape relations’ arise as the walking body – sometimes anxious, sometimes exhilarated – presses on through the undulations ahead: ‘the path . . . resonated not in muscle or bones, but in nerves’. 23 The reference to ‘nerves’ foreshadows what we discuss shortly. Relatedly, Scriven, theorising his autoethnographic Irish walking pilgrimage, writes that ‘[t]he body is our means of perceiving the world, but the world is our means of perceiving our body’, 24 the latter claim capturing something of how the 1935 man actively used the world to assess his own nervously embodied state. Other studies have alighted more squarely on ‘the equipmentality of walking’, including clothes, shoes, maps and GPSs, 25 or on the competencies of walking, ‘the gait, rhythm and musculature of walking bodies’, 26 sometimes acknowledging that differently abled bodies and psyches afford different capacities for walking (or, indeed, not walking). 27 In the wider horizon of a ‘new mobilities paradigm’ 28 attention has turned to the different modes of environmental encounter afforded by walking in contrast to cycling, running, motoring or other travel modes, 29 and to differential mobilities associated with different human groupings ranged along diverse axes of social difference. 30 Crucially, this literature has also considered immobilities, asking questions about ‘stillness’ and ‘stasis’, how such states may relate to or are ‘awaiting’ mobilities-to-come, and about how individuals who are slow or ‘stuttering’ in their movements are understood both by themselves and by others. 31 All these dimensions hold relevance for the empirical fragment on which we now report.
The walk
The document central to our paper entailed a first-person narrative of the patient’s chief physical difficulty, his encumbered walking in external spaces that he normally avoided, recounting what caused him to falter and what propelled him on. It recorded the patient’s perambulations in and around the Botanic Gardens in Glasgow’s West End (Figure 2), offering finely-observed phenomenological detail – of when he stumbled, rested, recovered and strolled on – seasoned by the psychoanalytic seed of self-inquiry. The opening paragraph rattled with the patient’s trepidation as he attempted ‘a walk in quiet streets’, disclosing how he ‘felt apprehensive before leaving’. 32 He struggled to maintain a sanguine attitude as his physical symptoms intruded, writing: ‘For the first hundred yards I felt uplifted by the fact that I was doing better than I expected, and then my legs got tired, and the gait strained and unnatural’. Invoking a psychosomatic reading briefly held this tiredness at bay: ‘I reasoned with myself that the symptoms were merely manifestations of my mind, and I carried on with renewed energy til exhaustion caused me to stop’. This capacity to explain away his physical symptoms was reassuring, strengthening his intent, and he ‘determined not to be beaten’. He traversed ‘Queen Margaret Drive, [. . .] a long road’, before crumpling in disarray at a bench at the Gardens’ entryway (Figure 3).
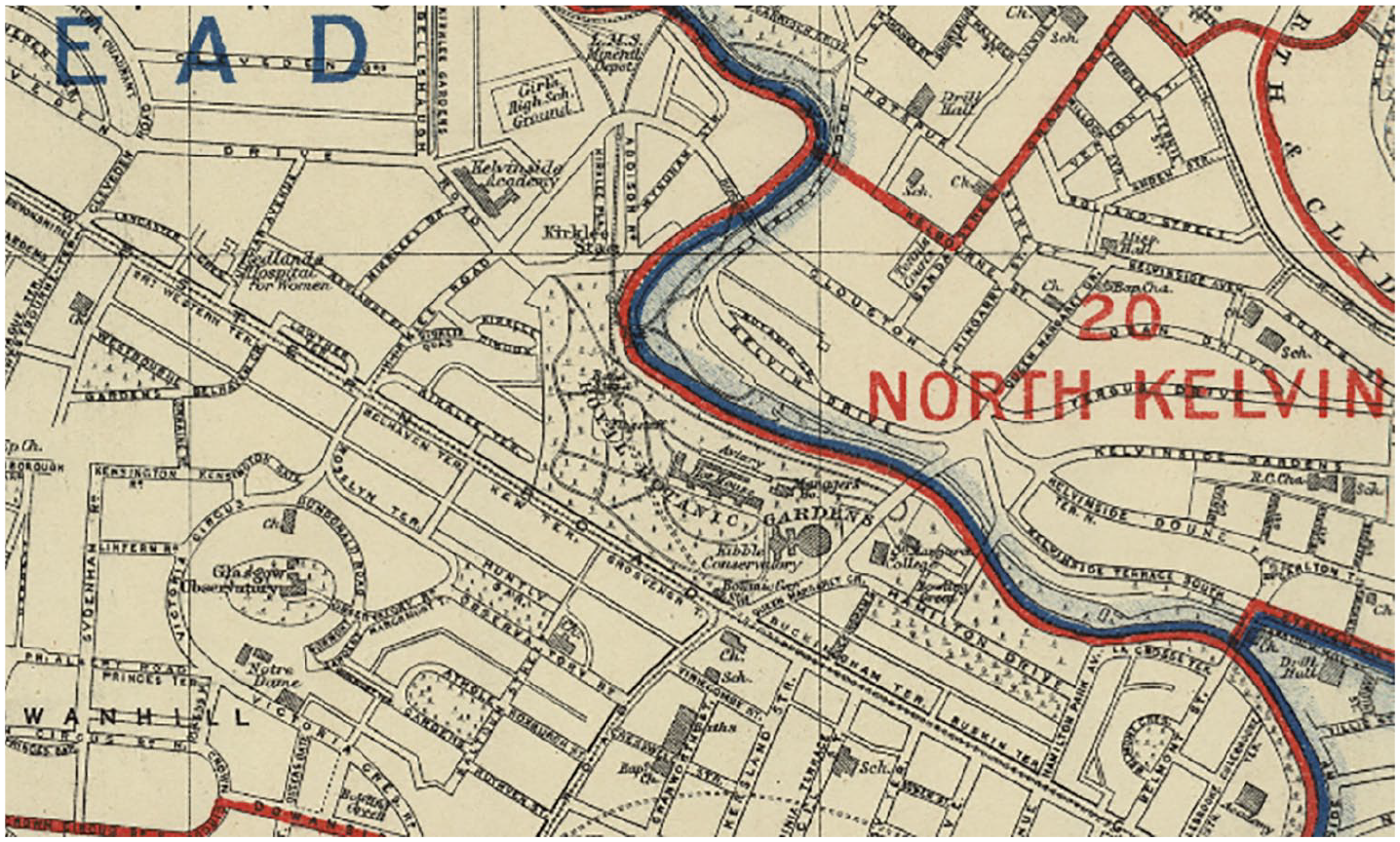
Map of the Botanic Gardens and its surroundings.
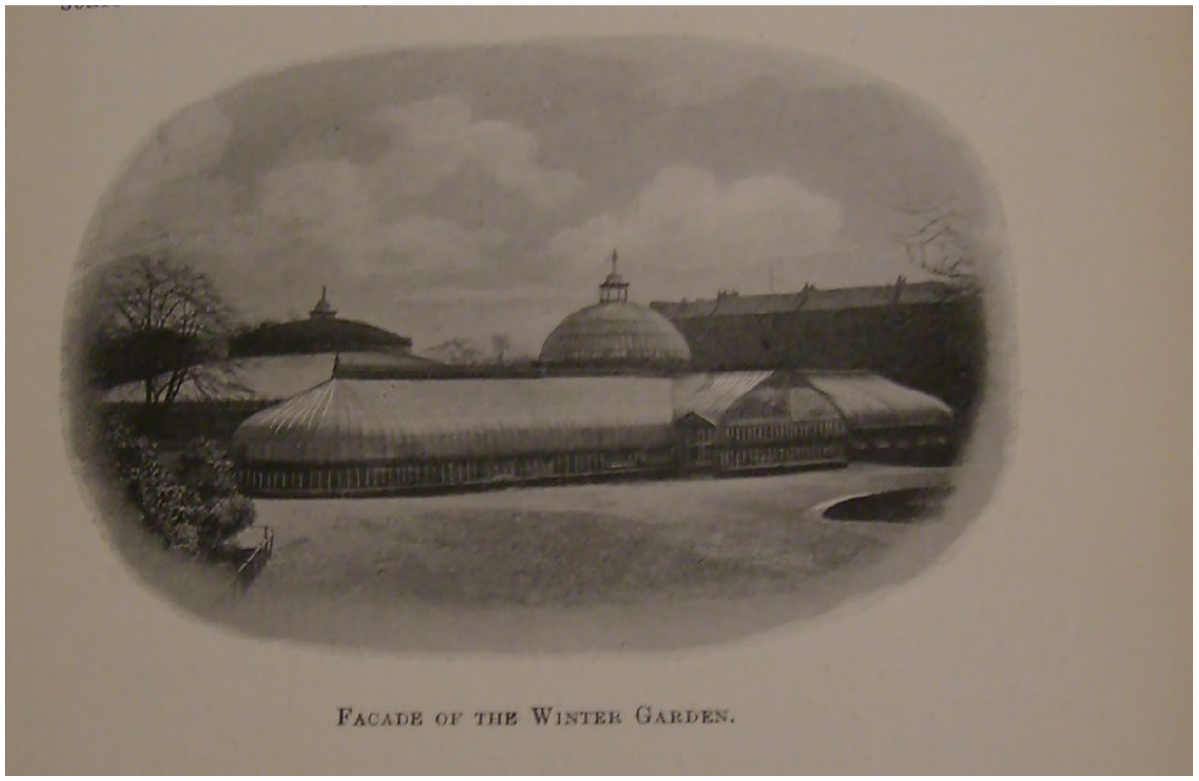
Illustration of the Botanic Gardens.
When the patient advanced again, ‘with renewed confidence’, his locomotion was stymied by a social stimulus ‘at the flagpole’: ‘I had to pass some people and my confidence disappeared’. A psychosocial sensitivity alerted him to how his symptoms flared in response to other walkers but faded after their passing, but this social encounter filled him with disquiet and lethargy: I became apprehensive, my legs and feet became tensed, and I walked slowly past the people, pushing each foot forward as though against a heavy wind resistance. The physical effort was accompanied by a feeling of terrific pressure at the back of my head.
With greater distance from other walkers, these symptoms expired or mutated: ‘the head pressure disappeared, the physical tension relaxed and these were replaced by a headache, and pains in the legs’. At this juncture, the patient disclosed his investigative ambition: this experimental walk was enacted precisely to procure insight into what triggered his condition. He appraised what had happened: ‘aware that the most potent factor had been the passing of the people, I decided I would test it again by walking past the people sitting in front of the hothouses’. An impending ‘feeling of collapse’ halted this trial, however, pressing him to return to the refuge of home by a less stimulating route: ‘I made my way by easy stages along the quiet paths’.
The patient’s implicit plan to master his unwieldy physicality became increasingly evident as the walk progressed. Both at the beginning and climax of the narrative, he reconfigured stages of his walk into psychologically manageable steps. For example, after first reaching the gates of the Botanic Gardens, he pragmatically split his journey into shorter stretches punctuated by restorative pauses at benches: ‘While resting I reasoned that, having got so far, I could reach Kirklee by walking along the river, taking a rest at each seat’. 33 Arriving there, the patient then ‘sat on a seat, exhausted but elated’. The close of the account brought the psychological dimension of his coping methods into sharpest outline. Indeed, the ‘exhausted’ patient grew ‘apprehensive’ at the prospect of traversing a traffic-laden Queen Margaret Drive, but revealed a strategy reliant on a mind-body connection, the possibility of mentally controlling his gait: ‘I determined I would keep calm; if I relaxed my mind my legs would relax’.
The patient had invested in this ‘frame of mind’, an internalisation of psychodynamic ideas, presumably imparted by Rodger, to carry him home. This attitude still proved hard to sustain, as nearing the roadway the patient began ‘walking slower and slower, apprehension and physical tension growing simultaneously’. He described a moment of crisis: as he ‘stopped at the edge of the pavement in a panic, my legs wouldn’t move and I felt like collapsing’. The patient’s rationalisation of his difficulties faltered, and instead the threat of falling in the street pushed him onwards: ‘I reasoned with myself but suddenly I felt I must move at once to avert a collapse’. He forced himself to recommence walking: ‘I [. . .] glued my eyes to the other side, forcing a foot on the road. I pushed each leg forward as though against a heavy wind resistance’. The intensity of this psychological concentration detached him from his surroundings: ‘I felt as if I were in the air with no grip on the road’. Nearing his destination, the patient, again sensitive to psychosomatic shifts, observed how his physical distress changed: ‘As I got over the crown of the road and approached the other side, the head pressure eased, my legs relaxed, and I stepped on to the pavement feeling exhausted and aching, and headachy’. He felt accomplishment in overcoming his anguished mobility, noting how he ‘walked home more easily uplifted by the fact of my achievement’. Such was the effort expended, though, that this walk continued to take a toll: ‘The nerves throughout my whole body, even to face and teeth ached and vibrated for the rest of the day’.
Other walks
This walk narrative was presaged and echoed by briefer statements on the patient’s other outdoor ventures.
34
For example, a report for the week ending 10th April 1935 was structured into brief diary-like entries for each day, comprising terse flash narratives recounting his daily perambulations around Glasgow, pairing an itinerary of streets negotiated with details of symptoms and preoccupations. Beginning on Thursday, the jotting read: Thursday Gardening at Hillfoot. Brighter. Less fatigue. Went alone to library for Brill’s Psychoanalysis [italics added]. Nervous in library. Nearly collapsed outside. Great difficulty getting home.
35
Though sparing, this glimpse disclosed the unpredictable vacillation of the patient’s condition from improved to verging on ‘collapse’, and how his curiosity for psychoanalysis, in this instance a psychoanalytic textbook, pulled him out of domesticity. The entry for Monday contrasted his comfortable movement at home with his inhibited walking outdoors: ‘Staggered badly when attempting to walk a few yards alone to a shop but could go upstairs two at a time’. Monday’s notes also showed that he took pleasure in some social outings: while at the cinema with a companion, the patient endured ‘palpitations for over an hour’, but concluded that he still ‘[e]njoyed the show’.
A similar format featured in an account dated 26th December 1934 with a digest of the patient’s condition for Thursday and Friday, augmented by an expanded two-paragraph account for Saturday clarifying his project of self-inquiry, but here turned towards ‘the past’. 36 He observed on Thursday that he ‘[f]elt very disturbed, mind going over past, sex predominating’, 37 while in Saturday’s entry he stated that he ‘[c]ouldn’t get my mind off past, sex predominating’, before elaborating on a disastrous excursion with his wife. A free association upon a dream dated 30th/31st October 1934, recalled in an analysis dated 1st November 1934, revived memories of stressful walks from the patient’s youth. 38 A perilous experience from his military years emerged: as he walked on a ‘narrow wall’ carrying a rifle, ‘[t]he man behind me jumped + struck the butt of my rifle which dashed into my glasses + injured my left eye’. Just starting working life aged fourteen, moving ‘a small motor-car engine’ affected his mobility in the same manner as his current symptoms: afraid he might lose his grip on the ‘far too heavy’ engine, he ‘staggered all over North Street’. Most significantly, the patient recalled ‘being taken into that shop in Maryhill Road’ after his ‘1st attack in the street’, as was recorded in the margin. In a report covering 7th to 11th April 1939, the outlying last session in the series (see below), he detailed the somatic disarray that had ‘almost overcome’ him: ‘When alone, my stomach keeps working, ears + throat feel distended, and my legs are nervous’. 39 Indeed, ‘[w]alking or standing, alone or accompanied, raise the symptoms til I could scream’, adding that he would ‘feel stricken with fear as though every activity in my body had ceased’. Perseverance caused his symptoms to proliferate: ‘When I persist, my eyes won’t focus, [. . .] my whole body feels distorted and extremely painful till I have to give in’.
Locomotion under analysis
Rodger and the patient co-explored the latter’s troubled bodily geographies through a quasi-psychoanalytical gaze. Through weekly logs and free-associations upon oneiric shards, the theme of immobility, broadly understood, became transposed from the physiological to the mental sphere, positioned as a form of stasis locked psychologically and traced socially across the patient’s case history. Notwithstanding his sometime scepticism towards psychoanalytic theorisations, the value of a self-investigative, self-analytic spirit prevailed, encouraging ‘experiments’ such as his West End perambulation.
Father, family and psychological stasis
In an analytic session dated 6th February 1935, the patient described how, pressured by familial obligation, his steps had become leaden: his legs ‘drag[ged] in the street’ because his parents, as well as his ‘wife’s people’, were ‘a drag on me’. 40 He explained that ‘[t]he drag that has always been in me because of my father + mother has prevented me doing what I wanted’. Familial demands struck the patient as a conjoined physical and emotional force, causing his legs to buckle. He confessed that it was this ‘drag’ that ‘kept me back’ before, recalling a walk when his ‘legs’ turned ‘dead’. His progress through life, whether maturing into adult roles or simply walking the street, was thus ever constricted. Never ‘free’, he had always been ‘drag[ged]’ down by his ‘responsibilities’, as in the childhood task of physically supporting his inebriated father voiced in an analytic session from 13th February 1935, revisiting a violent dream of retribution. Unable to cope with bearing his father, a ‘heavy man’, upright, he admitted: ‘I had some terrible jobs with him – even when I was older I couldn’t manage it’. 41 The patient ventured whether his unsteady gait was connected with his father’s drunken lurching: ‘[t]he thought comes into my mind – the number of times I have been with my father & he was staggering. Has that anything to do with me staggering?’.
A dream from the night of the 5th/6th August 1935 commenced with the patient’s homespace being invaded by uninvited visitors, including his inebriated father. Steering his father away from the others, the patient ‘cut him short and laid off at great length of how I had been off work for 15 months, and that my chance of recovery was only one in eight’.
42
His wife corroborated this story, while his father affirmed ‘he knew’ that his son had been admitted to ‘the asylum in Edinburgh’. When the patient claimed that recovery might be unreachable, he added that he ‘might never even walk again’ and ‘might end in Barlinnie’.
43
In the analytic session of 13th February 1935,
44
Rodger transcribed the patient’s aforementioned dream of retribution from the night of 7th/8th February: [D]reamt that he was sitting with a lady at a table. A very big man [. . .] I found myself with a gun in my hand. As he raised his right hand to strike me I shot him in the wrist. . . . I explained that I was going to make him suffer as I suffered and that I was going to shoot him in both legs and the stomach. I deliberately shot him in the legs. I did not shoot him in the stomach nor in the head.
The patient identified his dream self as ‘most vindictive – it was just like the satisfying of an unfulfilled wish’, a longing to inflict on his father physical debilities akin to his own, including mobility impairments. 45
Streets, workplaces and social stasis
The instability of the patient’s early life rippled into the present, sabotaging his will to move onwards through the world, whether on a daily or a longer-term basis. With respect to the latter, the patient’s regular logs recorded how his condition confined him to the domestic sphere. In a weekly report ending 14th August 1935, he provided a digest of how it interfered with his free time, in that, although ‘strain[ed]’ at work, he was equally encumbered during periods of recreation: ‘Ear pressure worst at nights, and at weekends [. . .] Evenings and weekends spent mostly indoors. Still can’t walk in the streets’. 46 When the patient was ‘[l]ess irritable, and keen to take an interest in things generally’, the implication is that we would have followed his curiosity outdoors. A report ending 21st August 1935 emphasised a thwarted impulse to escape domesticity: ‘Evenings and weekends spent quietly at home; would be keen to go out but too exhausted’. 47 While the patient preserved himself through avoiding anything challenging, which he particularly identified with being and walking outside, he also deprived himself of a desired engagement with the external world.
The sources also elucidated how repeated moments of physical immobilisation on the streets entangled with, maybe sometimes straightforwardly causing, pronounced stasis in the patient’s conjoined psychological and social worlds. Unsurprisingly, to avoid social embarrassment, he wished to conceal his problems when in public spaces. In the analysis dated 1st November 1934, the patient divulged why he eschewed company when walking: ‘First thing that comes into my mind is my desire to leave anyone I am with on the street’.
48
Accompanying ‘a young lady’ to her car one evening some years previously, he reminisced, the exertion required to avoid falling caused the patient to disengage from his companion: ‘My thoughts were on keeping straight the whole way down. I merely replied in monosyllables’. A self-consciousness attached to his staggering in front of anyone but his ‘wife and boy’, and he admitted that in the ‘five years’ since developing his affliction he had sought ‘to hide that mostly in connection with meeting people’.
49
His apparent ignominy was heeded by Rodger, who made it a point of conversation with the rare interjection: ‘[You appear to have been ashamed of it!]’. Affirming, ‘Yes I have been ashamed of having the trouble’, the patient linked his decision to take sedative medication with a desire to convince others that he was cured, indicating that treatment, as well as ill-health, had a social dimension. The patient was temporarily liberated by medication, explaining how ‘a little bromide made me feel a new man [. . .] I walked calmly down the street’. Unfortunately, the effects wore off and the patient then ‘doubled + trebled the dose to appear better for the sake of others’. His inability to resolve his illness, coupled to his self-consciousness, meant that in the longer term he continually adjusted how he moved in the world. He rued how his condition had ‘
Entangled with work choices, the patient’s self-determination was rendered shaky by his condition. Disclosures about his mindset suggested a kind of psychological staggering, a hesitancy about what steps to take forward, akin to his physical impairment. In a report for the fortnight ending 15th May 1935, he vacillated indecisively on the factors that either eased or worsened his condition. 50 He remained unsure of the parameters of his illness and thus of his whole existence, observing that ‘[t]he symptoms are not consistent in their reaction to what I do’. Finding both ‘rest and activity’ could aggravate his condition, he remarked that ‘sometimes I feel better when working and at other times, the opposite’.
Pondering his suitability for different spheres of employment, he worried that manual work caused him ‘physical suffering’, yet he also endured hardship ‘on light work or not working’; while uncertain of his capacity to engage with the wider world, the patient held himself back as a means of self-preservation, confining himself within a narrow version of life, characterised solely by those tasks achievable ‘with minimum discomfort’.
51
Even ‘gardening’ could provoke erratic responses: while sometimes unscathed by long periods of labour, equally he could turn anxious ‘when standing doing nothing’. On many occasions, his psychological strategising stalled, notwithstanding his newly acquired knowledge of psychoanalysis: Sometimes it all seems so simple. My nerves are upset by a subconscious conflict [. . .]. I feel that when the conflict is removed, the nerves will settle and the incapacitating symptoms will go. Then depression comes in and it all seems so difficult. I get impatient at the time I have suffered.
The motion of stalling hence well described the patient’s own subjectivity, forever teetering between ‘simpl[icity]’ and ‘difficult[y]’, ‘hope and despair’.
A ‘make-do’ psychoanalysis
The materials presented above signal that the patient settled into a quasi-psychoanalytic relationship with Rodger, that is, a ‘make-do’ psychoanalysis skewed towards the social, the environmental and the worldly. ‘Make-do’ forms of psychoanalysis were certainly not unique to Rodger at this time. As Hayward writes, the conclusion in the late-1920s of the British Medical Association’s inquiry into psychoanalysis reinforced the thriving ‘eclecticism’ of British psychotherapeutic culture rather than elevating an orthodox Freudian practice. 52 Moreover, discussing the relationship between Freud and the civil servant and ‘field scientist’, C.C. Fagg (1883–1965), Forrester and Cameron evidence that, to a degree, even Freud occasionally encouraged an improvised psychoanalytic practice. 53 Fagg’s deep immersion in psychoanalysis included writing on the subject, analysing and sporadic communication with Freud over a period of ten years from 1923 to 1933. Letters between the two reveal that Freud endorsed Fagg’s unusual psychoanalytic method, proposing that Fagg’s diversion of an ‘obsessional’ patient’s ‘skoptophilia’ from ‘full-breasted women’ to ‘watching birds’ could be viewed as a rehabilitation. 54 According to Forrester and Cameron, the case of Fagg evinces ‘Freud’s broad-minded approach[es] to unorthodox practitioners’.
Rodger himself was self-taught in psychoanalysis (Figure 4). 55 He adapted his version of psychoanalysis during the 1930s in response to work demands at different psychiatric sites: Glasgow Royal Mental Hospital (informally known as Gartnavel) where Rodger was Deputy Superintendent, the ‘Out-Patient Psychiatric Unit of the Western Infirmary’ and the ‘Lansdowne Clinic for Functional Nervous Disorders, an Out-Patient Clinic for the Treatment of Psychoneuroses’. 56 He undertook analytic sessions with a few mentally unwell patients, perhaps ex-asylum in-patients such as the patient at the heart of our paper, likely meeting them at his own Glasgow home (Figure 5). However he habitually relied upon a ‘common-sense’ psychotherapy, a form of pragmatic and humanistic treatment informed by how psychoanalysis critically illuminated the neuroses, but one that moved (in briefer, fewer sessions) towards acknowledging the significance of the patient’s worldly context in both causation and cure. 57 Rodger employed psychoanalytic insights in such a make-do fashion in different contexts from his earlier career into the post-war period. During the latter, while Professor of Psychological Medicine (1948–1973) with his department at Glasgow’s Southern General Hospital, 58 he advocated an explicitly ‘eclectic approach’ according significance to the ‘psychological and interpersonal aspects of the disease and its treatment’ alongside the prescription of somatic therapeutics. 59 Ultimately, his interpersonal focus was not unique: a number of writers have explored the broader tradition in Scottish psychoanalysis, associated with W.R.D. Fairbairn and Ian D. Suttie, in which this focus was foundational. 60
Rodger, on holiday, posing outside Freud’s house, Berggasse 19, Vienna, c.1930s.

Rodger’s living room at 30 Falkland Mansions where he likely analysed his patients.
Without overly dwelling on Rodger’s practice, it is important to note that, while his voice is largely absent in the patient’s dream book, he still set the tone and parameters for the underlying sessions. 61 Returning to the fragment of psychiatric-psychoanalytical geography that is the patient-led account, we encounter this ‘make-do’ approach through following how the patient self-analysed using, but at times also resisting, a limited palette of baggily Freudian notions. These sessions never quite delivered the expected Freudian life narrative, and rather the patient’s employment of psychoanalysis was more gestural, his discussions incorporating basic concepts but also digressing into a more commonplace language and meaning. While vexed with ambiguity and a lack of a discernible narrative arc culminating in definitive insight or recovery, his case history still coheres into an expansive psychosocial narrative underpinned by everyday understandings of ill-health and unhappiness.
Occasionally the patient ran through possible explanations for his condition that were typically psychoanalytic. Notably, in a supplementary account attached to the weekly report dated 20th February 1935, the patient considered the viability of four possible aetiologies of his illness summarised under the following headings: ‘“Fear of my wife”, “Incestuous desire”, “[P]oetic justice” and “Sins of the fathers”’. 62 Interrogating these rough-hewn psychoanalytic narratives, he struggled to find any of them convincing, and in practice the patient’s damaged childhood, emerged as the most plausible cause of his present inability to cope. While in previous patient-authored reports psychoanalytic ideas had been manoeuvred by him in a more psychosocial direction, this document reveals, to a far greater extent, the disjuncture between the ostensibly analytic stories suggested to him by Rodger and his own story as charged by personal experience. Through the patient’s deliberation on the viability of each theme, the quasi-psychoanalytic clothing slipped or was rejected in favour of a less high-brow, but more whole-hearted, articulation of his pain.
A report dated 19th December 1934 summoned, if not faithfully replicated, a nascent ‘object-relational’ perspective on the patient’s immobility, likely emulating Rodger’s style of theorising. 63 When inactive, the patient was plagued by a disquiet that lingered until it could affix itself to something: ‘If I decide, or require to go anywhere, do anything, the apprehension or anxiety immediately attached itself to the object and symptoms become very acute’. 64 This anxiety manifested as he pursued his goals, hindering his progress forward, or made itself felt as a ‘bad reaction’ after the fulfilment of the task, discouraging future persistence. As he reflected, this anxiety manifested ‘whether the object be pleasure, work, or the most trivial incidents’. It thus lived restlessly within the patient: ‘when I’m doing nothing, I feel as though the anxiety wants to attach itself to something tangible’. This theorisation continued in the final report, covering several entries for March/April 1939. 65 The analysis seemingly stopped for a period before being later recommenced; in the relevant patient book, the second-from last session preceding that in 1939 was dated 28th August 1935 and the patient confessed that he had ‘missed the constructive working of the analysis’ in an entry from April 1939. 66 His interpretation in 1939 chimed with an object-relational stance as he described the externalisation of his agitation: ‘Anxiety has attached to everything and the symptoms have almost overcome me’. For the period 7th to 11th April 1939, his account of ‘one of the most painful spells’ was again imbued with a psychosomatic and psychosocial perspective, the kernel of the patient’s theorising hinging upon a sense that his immobility arose to curtail any engagement with ‘reality’ which, although ‘desirable’, past experiences had proven to be ‘painful’.
In a session from March 1935, meanwhile, the sole psychoanalytic description utilised was the concept of ‘subconscious desire’. 67 The patient wrote: ‘The predominating thought has been that the physical symptoms and difficulty in walking are the expression of the subconscious desire to withdraw from the responsibilities and pleasures of life’. 68 Notwithstanding that the ‘subconscious’ bestowed the patient with a tool to psychologise his superficially physiological affliction, the astuteness of the insight owed much to his self-perceptive prowess. It was through reflecting back on his past, not necessarily psychoanalysing it, that he discerned what can be cast as the worldly entanglements of his illness: ‘my symptoms vary according to the extent I meet, or am subjected to[,] life’. It is arguably in this phrase that the patient most cogently encompasses the core of his difficulties: inspired by a form of psychoanalysis on-the-hoof, he arrived at an awareness of his mental ill-health, with its markedly stumbling embodiment, as a subconscious aversion to ‘life’, to being ‘subjected to life’, surfacing in a retreat from – and immense unease if forced to engage with – the spaces of life in the everyday world beyond his home.
Conclusion
This paper has reconstructed what we reference as a small fragment of psychiatric-psychoanalytical geography, one in which it is possible to detect the co-mingling of psychiatric objectives (of treating and hopefully curing patients presenting with identifiable mental illnesses) and psychoanalytical concepts/practices (theorising the workings of the psyche, taking seriously the unconscious, passions and drives, and adopting certain strands of ‘on the couch’ 69 analytical procedure). It is a fragment in which matters of space, place and environment are repeatedly centralised, most obviously with respect to the patient’s embodied (im)mobilities. His difficulties in moving, particularly walking, are crucial, connected to problems with accessing the public realm of external environments, as transparently foregrounded in the patient’s ‘walk’ in January 1935. This wavering is then related, metaphorically, to his movement through life – the trickiness of maintaining a ‘forward’ momentum – as tied into more concretely spatialised hesitations about putting himself forward, in terms of employment, recreation and relationships.
This case history is partly the patient’s self-analysis at Rodger’s behest. Across multiple sessions full of dreams, free associations and reflection, the patient adopts, adapts and sometimes rejects more typical psychoanalytic explanations. A loosely psychoanalytic hue nonetheless remains, but always leavened with a healthy dose of what we might frame as a ‘geographical imagination’. 70 Ultimately what the patient finds most convincing is an account of how, leading from the traumas of an unhappy childhood with an abusive father, he has progressively sought to distance himself – physically, psychically, socially – from the spaces and environments of ‘reality’. He has sought to prevent himself from being ‘subjected to life’. In part this retreat is to prevent embarrassment from stumbles, but arguably it is more to stop the lively world ‘out there’ seeping ‘in here’, causing his precarious psychological – and physiological – balance to over-topple. Keeping close to the grain of the patient’s words within a knotty nexus of psychiatry and psychoanalysis, we have shown how this nexus was itself shot through with – was thoroughly contoured by – a walking geography of steps literally taken and not taken.
There are numerous resonances throughout with work on the cultural geographies of walking, perhaps most obviously in what is recounted, paralleling Wylie’s 2005 paper, about the imbrication of walking with ‘the nerves’ – with restlessness, anxiety, elation, and other states that clearly entrain body and mind, emotion and cognition – and how aspects of the self are both shaped and disclosed as the walking body makes its way into and through the world. The ‘make-do’ psychoanalytic sessions between Rodger and his patient repeatedly dwell on ‘the always emotional-affective nature of walking’, 71 taking extremely seriously ‘what could be considered the less remarkable, unspectacular and [usually [unreported everyday experiences associated with walking’ 72 (the ‘unemphatic passages’ of our opening epigram). The smallest details of walking – of uneven surfaces (curbs, ‘crowns’ of roads); of objects (benches, flagpoles, rivers); of people (differing in their affects whether close or distant) – become prominent, as too details of gait, muscles, leaden legs, tensed feet, pressured head and more. These tiny phenomenologies of the walking body-world assemblage are shown to matter deeply, here set within a form of ‘psy’ knowledge-making scaling up and out into the patient’s problematic life-history and stunted worldly engagements. Moreover, the stilling, slowing and stalling of the patient’s walking – stumbling, staggering, wavering; or immobilities punctuated by hesitant mobilities – are central to his story, offering the key, at once materially rooted and metaphorically projected, to understanding his tendency to withdraw from ‘life’ beyond the home.
Finally, reference can be made to a geographical study, if not one yet identified with the ‘new walking studies’, in which walking is nonetheless pivotal. In their study of missing people, many with mental health difficulties, Parr and co-workers discuss the erratic movements of these people as they move across the city, usually on foot, often circling their old haunts and neighbourhoods as places of memory and meaning (even if temporarily forsaken). 73 Building from in-depth interviews with ‘returned’ missing persons, these authors note that ‘journeys were described as nonlinear and characterised by circles, loops and squares’, as well as being ‘narrated as a deliberate, if shaky, set of decisions about where to walk and the geographies of walk’. 74 As they continue, ‘the ‘interior’ and ‘thinking life’ of [these] people in crisis was intimately linked to their missing mobilities’, meaning their movements while missing, and ‘characterised by stuttering duration, fast and uncertain rhythms and even clumsy occupations of space’. 75 Most of the vocabulary here, excepting ‘fast’, could be applied to the patient in our psychoanalytic-psychiatric fragment. The precise meld of mental health problems and bodily resonances is different, with no suggestion that missing people became mobility impaired in the same way as the patient with his fraught ‘nerves’, but the manner in which the latter’s difficulties were ‘worlded’ – as walk entered world, as world played back on walk – holds clear affinities with the stutterings and clumsiness evoked by Parr and colleagues. The conceptualisation here also dovetails with what we have derived from Bondi and McGeachan, and with what Rodger and his patient themselves conjectured, allowing us to discern fresh perspectives on how academic geography’s psychoanalytic and walking ‘turns’ might in future step together.
Footnotes
Acknowledgements
The authors gratefully acknowledge the assistance of: the University of Glasgow Archive Services staff and Moira Rankin, Head of Archive Services; Alistair Tough and staff at NHS Greater Glasgow and Clyde Archives at the Mitchell Library, Glasgow; and the Sibbald Library staff at the Royal College of Physicians of Edinburgh. For providing images and permitting their reproduction in this article, we thank University of Glasgow Archives and Special Collections; the National Library of Scotland; and Dr Christine Rodger. We are also very grateful to Gavin Miller for his insightful discussion of this research. We must particularly thank two referees who commented on the initial submission: their thoughts have immeasurably improved the final version here, not least in prompting us to do more with cultural geographies of walking.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article is developed from the first author’s PhD research which was funded by a Lord Kelvin Adam Smith PhD Scholarship (2013–2017) from the University of Glasgow.