
Abstract
This research investigates the use of art-informed methods in social work research to explore collaboration between child protection social workers and other multidisciplinary professionals in New Zealand. The study focuses on these professionals’ perceptions and experiences of multidisciplinary collaboration within a hospital setting. “Drawing and Talking” is employed as an art-based research method, with data comprising 26 drawings created by individual participants including Police, statutory social workers, health professionals, crisis support and cultural support. These drawings reflect professionals’ views on collaborative practices. Interpretative phenomenological analysis was applied to both the drawings and the participants’ verbal explanation of their own drawings, identifying five key themes concerning multidisciplinary collaboration among child protection professionals. This study contributes to the existing body of knowledge on interdisciplinary collaboration in child welfare and offers practical insights. Moreover, it introduces a novel approach to studying multidisciplinary cooperation in this field.
Introduction
In child protection, multidisciplinary collaboration is widely recognized as essential for effective practice in cases of physical and sexual abuse (Herbert and Bromfield, 2019). While legal frameworks and operational practices of multidisciplinary child protection teams differ across countries (Zafar et al., 2021), they consistently involve professionals from social work, law enforcement, healthcare, and mental health. A key aim is to minimize potential for retraumatizing children through repeated testimony (Herbert and Bromfield, 2019).
A scoping review by Herbert and Bromfield (2019) of 63 studies indicated that multidisciplinary child protection collaborations produce increased rates of arrest, prosecutions, and convictions; support increased referrals for trauma support; and increase professional satisfaction (Herbert and Bromfield, 2019). However, child protection collaboration across organisational boundaries can be challenging, reflecting substantial disciplinary differences that exist within multidisciplinary teams (Herbert et al., 2020). As professional silos, poor communication, and uncoordinated responses arise, they can exacerbate the vulnerability of children at risk (Campbell et al., 2020).
Factors that support and block multidisciplinary collaboration in child protection have been noted at both systemic and practitioner levels (Price-Robertson et al., 2020). Systemic barriers include inadequate resources (Cooper et al., 2016), unequal power dynamics (Johansson, 2017), differing conceptual frameworks and goals (Mason et al., 2018), inconsistent confidentiality policies (Cooper et al., 2016), and lack of organizational support (Horwath and Morrison, 2011). On the practitioner level, barriers include lack of understanding of partner agencies’ scope (Herbert et al., 2020), unclear guidelines on when and how to collaborate (Alfandari &Taylor, 2022; Horwath and Morrison, 2011), and ineffective communication (Cooper et al., 2016), all of which hinder a coordinated response. Key facilitators include regular communication channels, fixed network structures that involved all stakeholders (Eilfgang et al., 2024), shared meetings (Søbjerg, 2017), co-location (Herbert and Bromfield, 2019), mutual understanding of roles (Cooper et al., 2016), and shared values (Winkworth and White, 2011).
Collaboration between different professionals involves specific challenges. Eilfgang et al. (2024) identified difficulties in collaboration between child protection and criminal justice workers, including burdensome criminal proceedings, interpersonal frictions and negative perceptions of other professionals. Social workers’ collaboration with healthcare professionals is hindered by misunderstanding of medical terminology, differing thresholds for risk perception, and concerns over confidentiality when sharing information (Campbell et al., 2020; Zafar et al., 2021). Similarly, collaboration with mental health professionals faces challenges due to varying perceptions of threats to child safety (Darlington et al., 2005).
Although elements of coordination and cooperation between services involved in child protection in New Zealand have developed since the 1970s, a concerted attempt was made in 2002 to enhance collaboration and streamline investigation and treatment processes across child protection services. Called Puawaitahi (Blossoming in Unity), this initiative involves, the police, medical teams, crisis support services and Oranga Tamariki (the national statutory social work agency, hereafter OT). All of these services, except OT 1 , are co-located at Puawaitahi in central Auckland.
The coordinated Puawaitahi service does not represent a complete collaborative system. It is important to understand that statutory responsibility for child protection in New Zealand lies specifically with OT social workers and Police. An evaluation of Puawaitahi (Stevenson, 2017), found that Puawaitahi effectively fulfils its mission, but needed to ensure consistency in referral quality and uniform implementation across regions. Other than this, research on professional collaboration in New Zealand’s child protection system is scarce, particularly from a social work practice perspective. The data presented in this paper is part of my doctoral research, which examines multidisciplinary collaboration within central Auckland’s child protection system, specifically focusing on the relationships between child protection social workers and other professionals. The research, including the drawing component of interviews was approved by the University of Auckland Human Ethics Committee.
While my data collection methods included interviews, non-participant observation, and text analysis, this article focusses on the use of visual materials: participant-created drawings. As Martikainen and Hakoköngäs (2023) noted, the drawing method helps to “make abstract social representations tangible” (p.985). My primary aim is to use these drawings and participants’ explanations of their drawings to better understand actual experiences of the otherwise abstract concept of collaboration.
The use of drawing in social work practice and research
In social science research, various visual materials have been utilized, including photography, comics, sketches, as well as film, video, digital visual media, and material artifacts (Grittner and Burns, 2021; Leigh, 2015; McNicol, 2019; Spencer, 2010). In her ethnographic study on child protection, Leigh (2015) used photographs to depict the physical settings of child protection agencies in the UK and Finland, helping readers to better understand the environments in which social work operates across different cultural and contextual landscapes. Studies indicate that drawing is widely adopted in health (Cheung et al., 2019; Guillemin, 2004) and psychology research (Ballús et al., 2023; James et al., 2018), whereas its use in social work remains limited (Clark and Morriss, 2015).
The drawing method is considered relatively unobtrusive and is often used as a research tool with children and adolescents (Ballús et al., 2023; Goodwin et al., 2023). There is a growing body of knowledge on the use of this method with adults in social services and healthcare, where it is regarded as conveying “a powerful message” by making the unspoken visible and encouraging empathy(Cheung et al., 2019; Schindel et al., 2022).In a study on urban planning for elderly care in Switzerland, Zweifel and Van Wezemaela (2012) found that in complex situations involving multiple stakeholders, intricate relationships, or chaotic processes, the linearity and causal logic required in verbal discourse often left both researchers and participants unsatisfied. To address this, they developed a research method combining drawing with interviews, where participants used various symbols and line representations to illustrate complex relational processes.
The “draw-and-talk” or “draw-and-write” method helps researchers explore participants’ intentions, thoughts, and experiences (Hartel et al., 2018; Lyon, 2020). Participants’ explanations of the motives and meanings behind their drawings can reveal deeper layers of meaning (Rose, 2016). Drawing also assists participants to summarise complex ideas, allowing them to organize their thoughts within a limited timeframe (Lyon, 2020). Art-based data collection and analysis does present several challenges, including participants feeling uncomfortable or resistant about drawing, or being uncertain about what to depict (Brailas, 2020). Adult participants are more likely to decline, emphasising that drawing skills are not the focus, which can strengthen confidence in the process (Martikainen and Hakoköngäs, 2023).
The use of drawing is well-suited for studying topics related to social work. Visualizing relationships is a fundamental skill in social work practice, with key techniques including the creation of genograms and ecomaps (Singer and Belluomini, 2018). These tools help social workers, and their clients, explore family backgrounds and surrounding resources more effectively. The process potentially engenders new insights and perspectives (Rempel et al., 2007). My study focuses on the complex relationships involved in multidisciplinary collaboration, particularly cooperation between social workers and other professionals. Accordingly drawing and talking was used to help participants envisage professional relationships within a complex system and express thoughts and feelings that might be hard to explain in words alone.
Methodology
This study’s theoretical framework is hermeneutic phenomenology, emphasizing the importance of understanding participants’ subjective experiences and the ways they construct meaning within their specific contexts (Bynum and Varpio, 2018). Drawing is particularly effective for capturing complex emotional and symbolic meanings, making it well-suited to exploring deeper layers of participants’ experiences (Boden et al., 2018). Therefore, an art-informed approach was adopted in this research. Drawings were used at the end of the in-depth interview as a post-interview approach. The purpose of the interviews was to give participants an opportunity to explore their views and feelings about the usefulness of the collaborative process, where the interview itself served to stimulate participants’ thinking and understanding prior to drawing (Brailas, 2020). For the drawing part, the “draw-and-talk” method (Lyon, 2020) was used to invite participants to explain what they had drawn.
Sampling
Using purposive sampling, internal recruitment emails and presentations delivered to various organizations, 24 participants who indicated interest and willingness to participate were recruited for individual interviews. Participants, drawn from central Auckland child protection practice settings, represented diverse professional backgrounds, including social workers, doctors, nurses, police officers, and counsellors; all were women. Participants took part in one-on-one in-depth interviews and were asked to complete a drawing.
Data collection
Interviews were conducted between April 2022 and February 2023, in consultation rooms or meeting spaces at participants’ workplaces. The researcher supplied blank A4 paper and a variety of drawing materials, including coloured pencils, crayons, markers, and ballpoint pens. At the end of an in-depth interview, following a standardized script, the researcher verbally asked participants, ‘Please draw a picture that illustrates how you collaborate with other professionals in child protection work.'
To prepare for the inevitable ‘messiness’ of creative arts-informed research and make the drawing process comfortable for participants, specific requirements were not imposed. Participants were invited to use colours, symbols, or lines in whichever way they wanted to, without worrying about drawing skills. All were open to the drawing activity. No time limit was imposed, and the process generally took around 10–15 minutes. Once participants completed their drawings, they were invited to describe the artwork to clarify its meaning.
Due to the limited number of specialist staff engaged in the central Auckland multidisciplinary child protection process, we did all we could to ensure participants’ privacy. Participants were anonymized and coded into two groups: a social work group (OT social workers and health social workers) and another professionals’ group (including police, doctors, nurses, counsellors, Evidential Video Interviewer, Crisis support, etc), coded as SW + number and OP + number. Drawings were labelled with the corresponding identification code and digitally scanned, while verbal explanations were recorded and transcribed verbatim.
Data analysis
The research team consisted of the primary researcher and two supervisors, all from the field of social work. The primary researcher is a PhD student from China studying in New Zealand, with extensive experience in child protection social work practice and research. Both supervisors also have long-term practice experience in statutory and NGO settings, contributing local knowledge and diverse perspectives to the project.
Data analysis followed the Bartoli’s (2020) interpretative phenomenological analysis framework, which modified Smith’s et al. (2021) six-stage process to incorporate visual materials, uncovering hidden meanings and experiences embedded in drawings and related interview data.
The first step involved immersion in the dataset, including participants’ drawings and their verbal descriptions. Then, notes were made to explore language used by participants, and semantic content. For the drawings, the researcher identified key visual elements such as figures, objects, environments, and symbolic representations. Analysis employed a hermeneutic circle, moving continuously between the whole and its parts to deepen understanding (Boden and Eatough, 2014). Visual representations and verbal descriptions were cross-referenced, forming the foundation for initial interpretations.
In the third and fourth steps, emergent themes were identified and organized into tables to distinguish connections across themes (Bartoli, 2020). For instance, visual representations of “arms encircling a group of people in the centre” was interpreted as representing collective collaboration and support. This imagery symbolized “connectedness” and security, fostering a stable emotional environment. Interview data reinforced the theme of collective collaboration, emphasizing shared values of equal and combined contribution. This process was iterative, with themes refined through comparisons between visual and textual data to ensure consistency. The focus was on “convergence and divergence” (Bartoli, 2020: 1012). Finally, themes were reviewed by the first author and supervisors to ensure reliability and transparency. By embedding themes within participants lived practice experiences, analysis captured meaning beyond surface-level descriptions.
Results
By analysing the content of the 26 drawings (two participants provided two drawings) along with their corresponding verbal explanations, 17 drawings were selected and presented from the original 26 based on their thematic relevance to multidisciplinary collaboration, diversity of professional perspectives, and to avoid redundancy in visual content. Four key themes were identified: core values of collaboration, challenges in collaboration, complexities within collaboration and health professional specificity. The following sections present images and comments illustrating each theme.
Theme 1: The Value of Child and Family-Centred Collaboration: The ideal
Seven participants’ drawings emphasized the ideal vision for child- and family-centred multidisciplinary collaboration. Interestingly, this theme’s drawing was exclusively produced by social workers (OT and health social worker), highlighted core values such as equal support and cooperation. From these seven drawings, four were selected to illustrate in this article, as others contained overlapping symbolic elements. Figures 1–4 illustrate this theme by featuring linked arms, open hands, wreaths symbolizing different collaborators, and round tables of cooperation; all conveying the ideas of interconnectedness, mutual support, teamwork, and trust across professions and agencies. Verbal explanations of the drawings reflected participants’ diverse cultural backgrounds. Drawing examples of multidisciplinary collaboration centred around children and families (SW1). Drawing examples of multidisciplinary collaboration centred around children and families (SW2). Drawing examples of multidisciplinary collaboration centred around children and families (SW3). Drawing examples of multidisciplinary collaboration centred around children and families (SW4).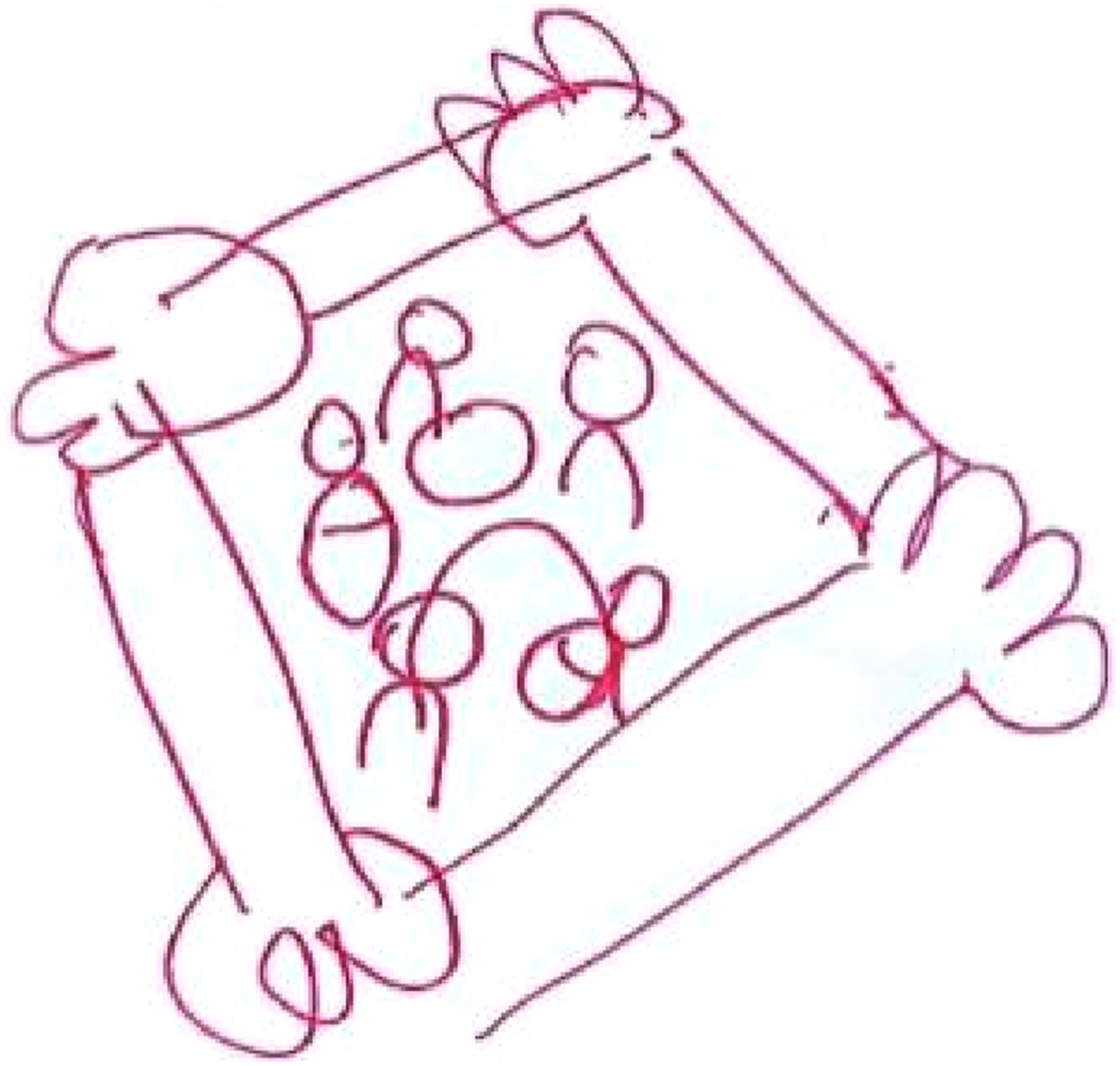
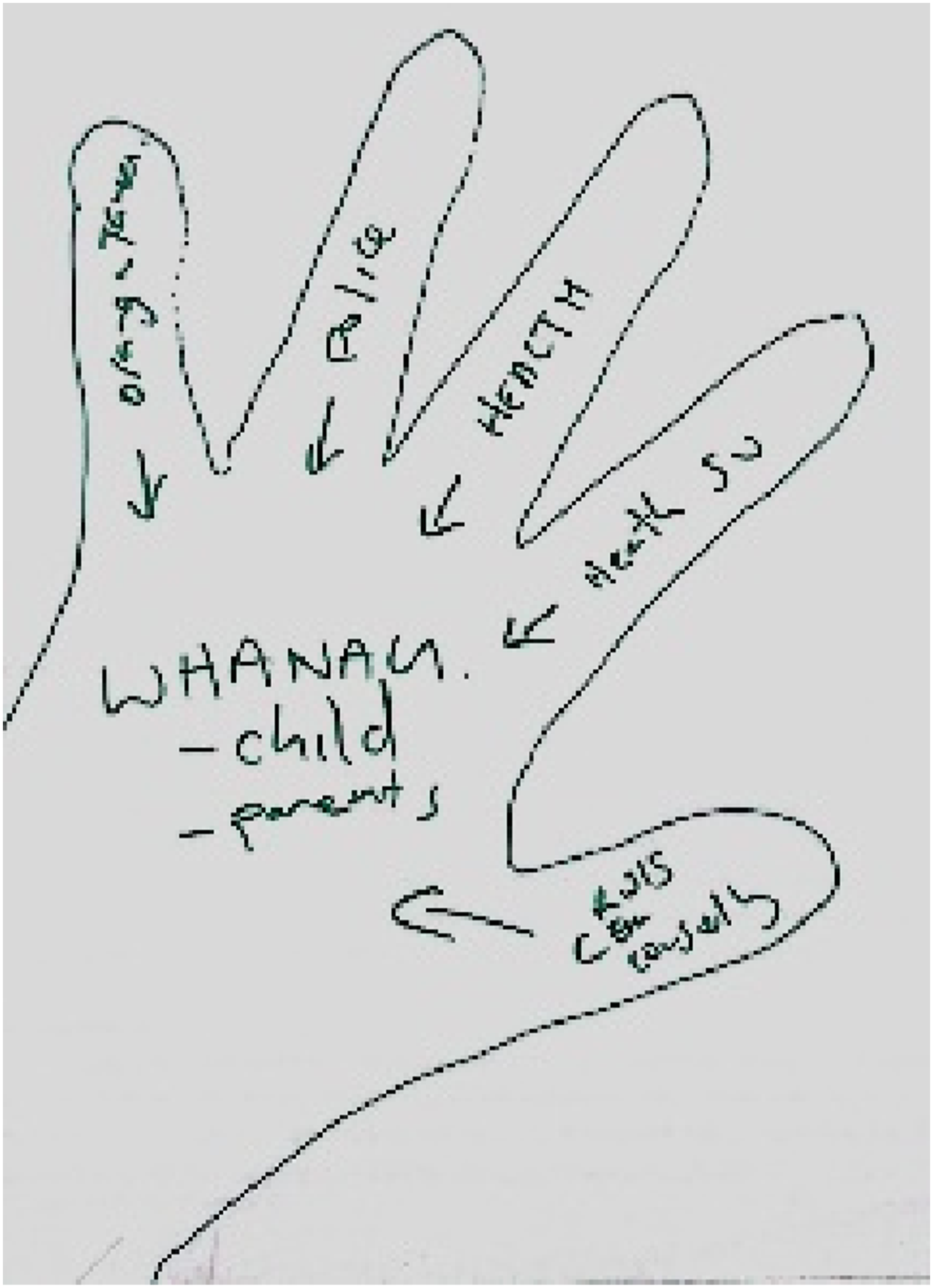
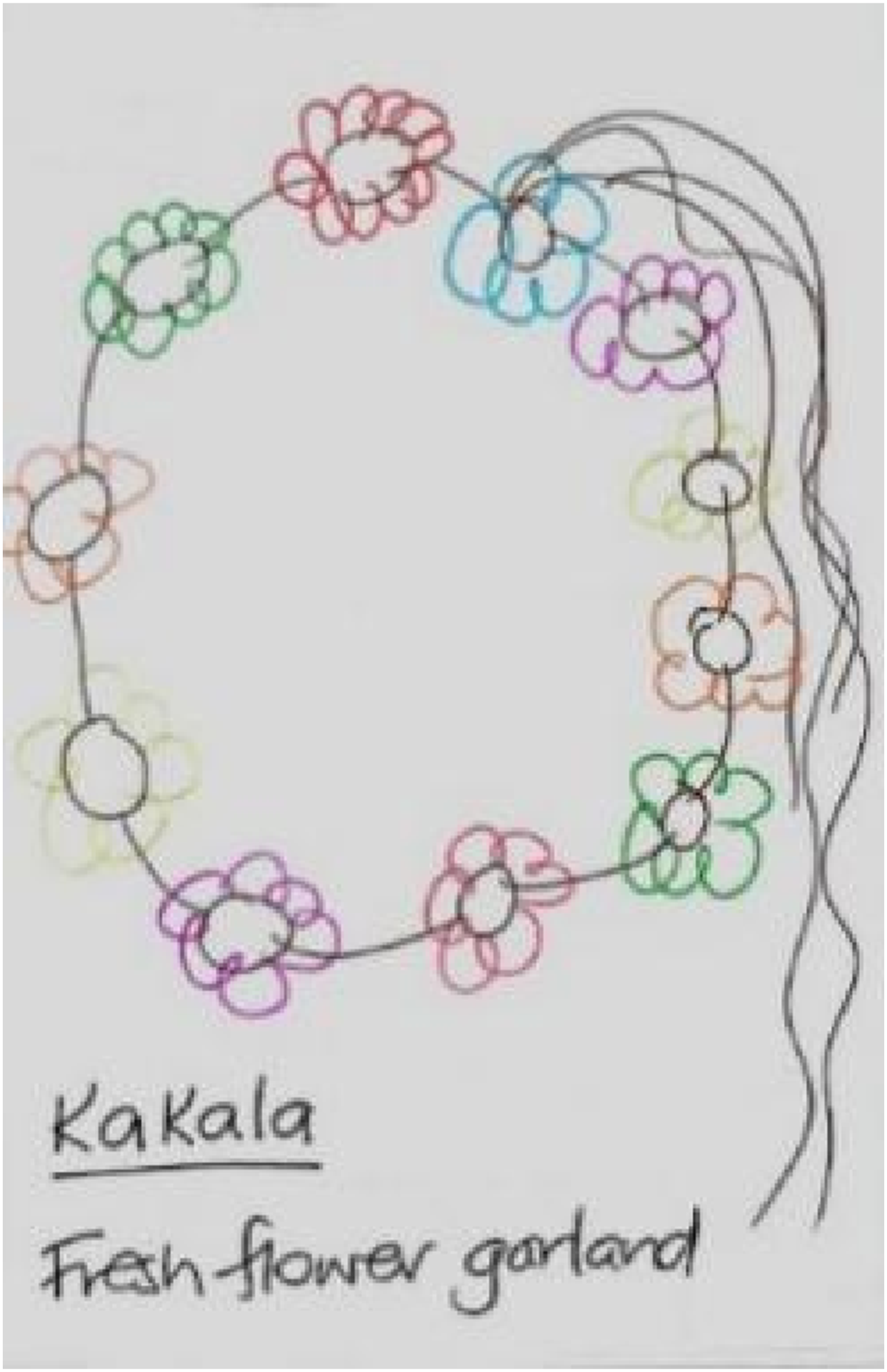

Figure 1 depicts collaboration as a group of multidisciplinary professionals holding hands around a child and family in need of assistance. SW1 emphasised that the core of service should encompass children, their families, extended family and significant others: “Like we’re all sort of equally contributing in providing to assist families, and they’ve always sort of focusing that the kids and the family are always at the centre of the decisions that we make.”
Figure 2 depicts an open palm, with fingers representing five professional groups: police, health, health social work, crisis support and counselling. Arrows pointing towards the centre of the palm, labelled ‘child and parents,’ illustrate that supporting families is the core of multidisciplinary collaboration. Additionally, the open hand holds special significance in Māori culture. As explained, “this symbolizes many things, especially the concept of welcoming in Māori culture - showing your hands is a gesture of openness and non-threatening intent.”
In Figure 3, collaboration is painted as a Pasifika-style garland with each flower representing a different professional. The garland is described as a gift to the family and child, a “safety plan.” This highlights the practical aspect of multidisciplinary collaboration, where the garland represents not just symbolic unity but tangible services and resources. As SW3 emphasized, It's like placing the garland around their neck and saying, “There you go, you've got your support. You've got people here, housing, an audited key person, Family Start counselling, a GP, all these different services to support you as you work through this.”
SW4 drew three professionals—representing OT, the police, and the health authority —sitting around a circular table (Figure 4). In the centre, she painted family encircling the child. She emphasized that effective collaboration requires departments to “join hands, share information, and create opportunities,” and expressed disappointment that this level of collaboration is not yet fully realized. SW4 highlighted the importance of respecting families, stating, “We work from the assumption that the family knows what is best and safe for the child. Our role is to strengthen that, not create it. We’re here to create opportunities for families to improve.”
In summary, participants’ drawings revealed their perception of unity as a core element of multidisciplinary collaboration. Images of hands, garlands, and round tables, symbolized connection, sharing, and a sense of trust and togetherness. The consensus was that children and families are at the heart of multidisciplinary work in child protection. The question of whether this reflects actual practice, or a shared belief is considered in the discussion section.
Although the images above illustrate an ideal collaboration vision from social workers, there were slight differences. While all agreed on the goal of serving children and families, SW4 expanded the scope to include Iwi (tribe) 2 , noting that “they should be given significant decision-making power.” Similarly, SW1 emphasized that “significant others” should be considered part of the family unit. In contrast, the other two participants focused more narrowly on children and parents as the core service group.
Differences in roles influenced which agencies were seen as key collaborators. For example, from their position as a health social worker, SW2 identified five primary professional groups. By contrast, SW4, an OT social worker, focused solely on OT, the police, and health, presenting a more tightly knit collaboration framework. (SW5).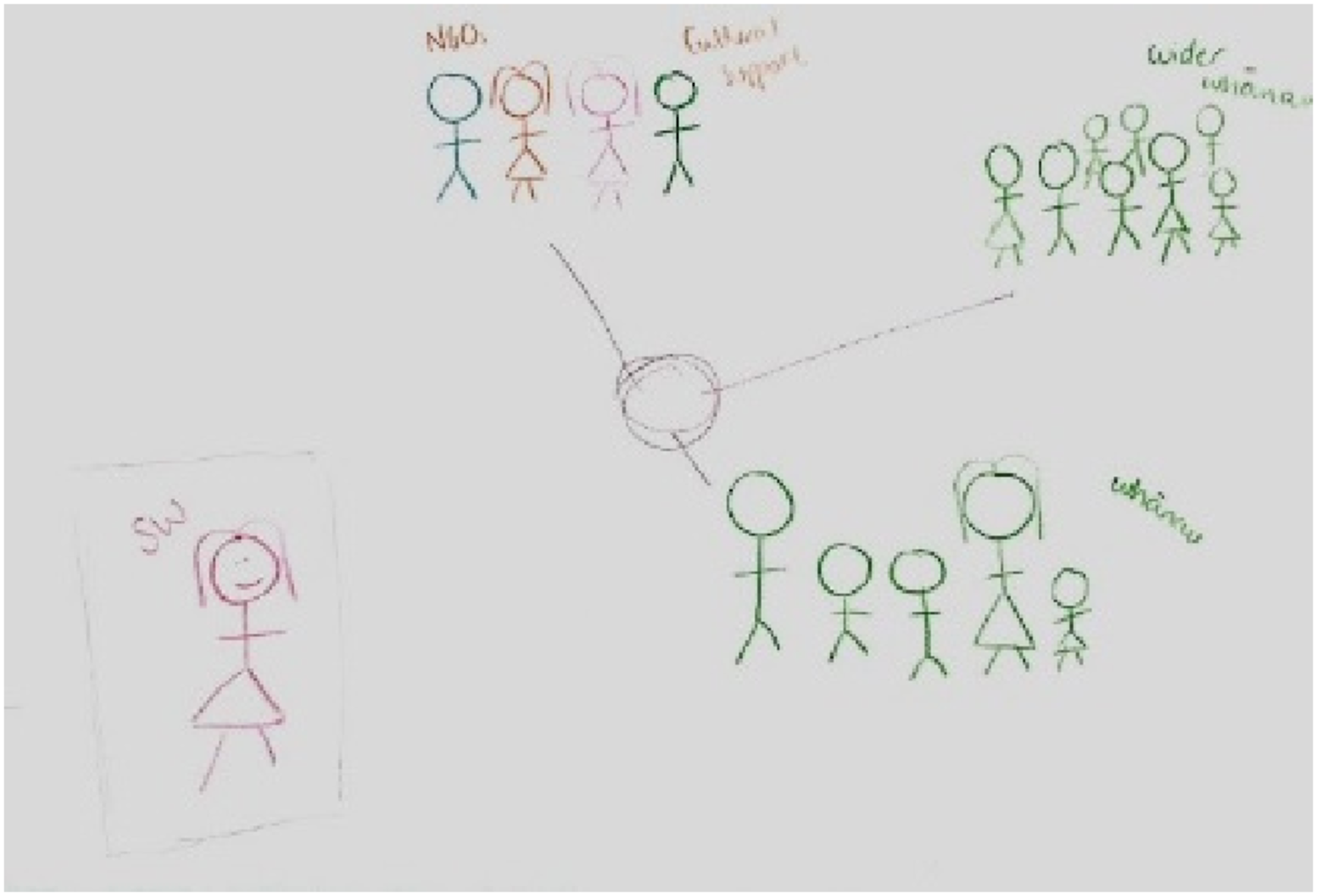
SW5 presents a different understanding of social work involvement in multidisciplinary collaboration, seeing her role as temporary and supportive, rather than one of long-term involvement. In her drawing (Figure 5), the social worker is intentionally placed at the periphery as: “My job is to get all of these people to come together and work together… So I want to stay over here and not be involved with these people.” This perspective frames OT social worker as “co-ordinator” or “facilitator,” rather than “core member” or “active participant” in the collaborative process.
Theme 2: Challenges in collaboration
Another important theme is barriers and challenges faced in collaborative work. These challenges were visually represented through metaphors, such as images of individuals falling into water, chaotic lines, and jagged shapes. Participants explained that these representations symbolized obstacles like lack of shared goals, difficulties in aligning perspectives, insufficient accountability, and differing interpretations of legal policies. Interestingly, all the drawings in this section were created by professionals employed by OT (Figure 6). SW 6.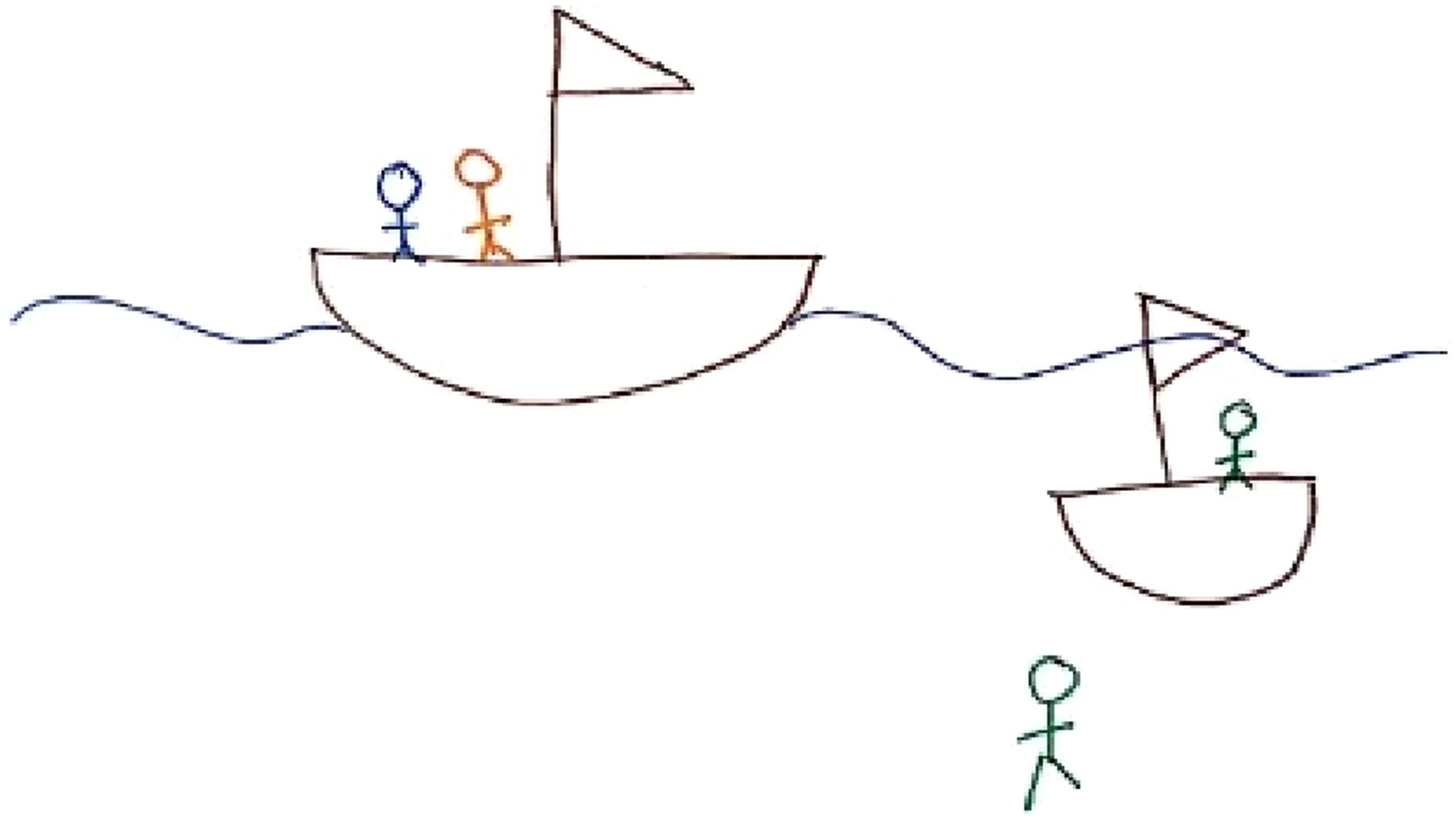
SW6 drew a small boat as a metaphor for the collaborative relationship. She points out that multidisciplinary collaboration is like collaborators rowing the same boat: “You’re trying to row to the same destination. But it’s trying to get everyone on the same boat really.”
One key challenge is determining leadership and operational dynamics. SW6 noted that not all practitioners move in the same direction, sometimes disagreeing on case management. While she expressed satisfaction with police cooperation— “I definitely think the police are on the same boat”—she highlighted challenges elsewhere, particularly the mismatch in pace with mental health services. “Sometimes people can fall off the waka (boat)…kind of almost be in their own little waka at times. They can have their own way… agencies like mental health can sometimes be drowning in their own work …And yeah, that paddling in a different situation.”
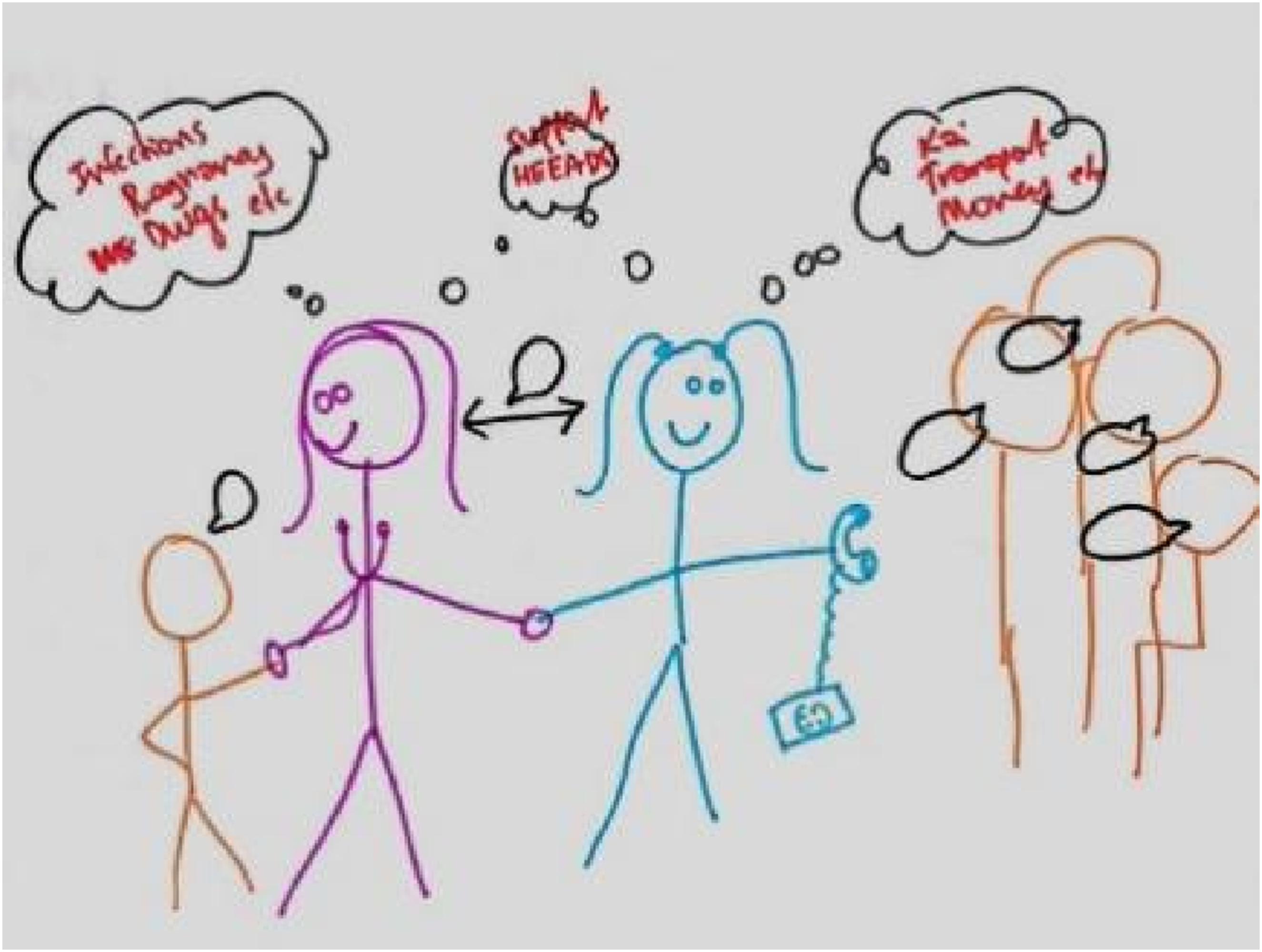
Figures 7 and 8 express frustration with the current state of collaboration, specifically emphasizing fragmented communication and collaborations between professionals. (SW7). (Other professional “OP” 1).
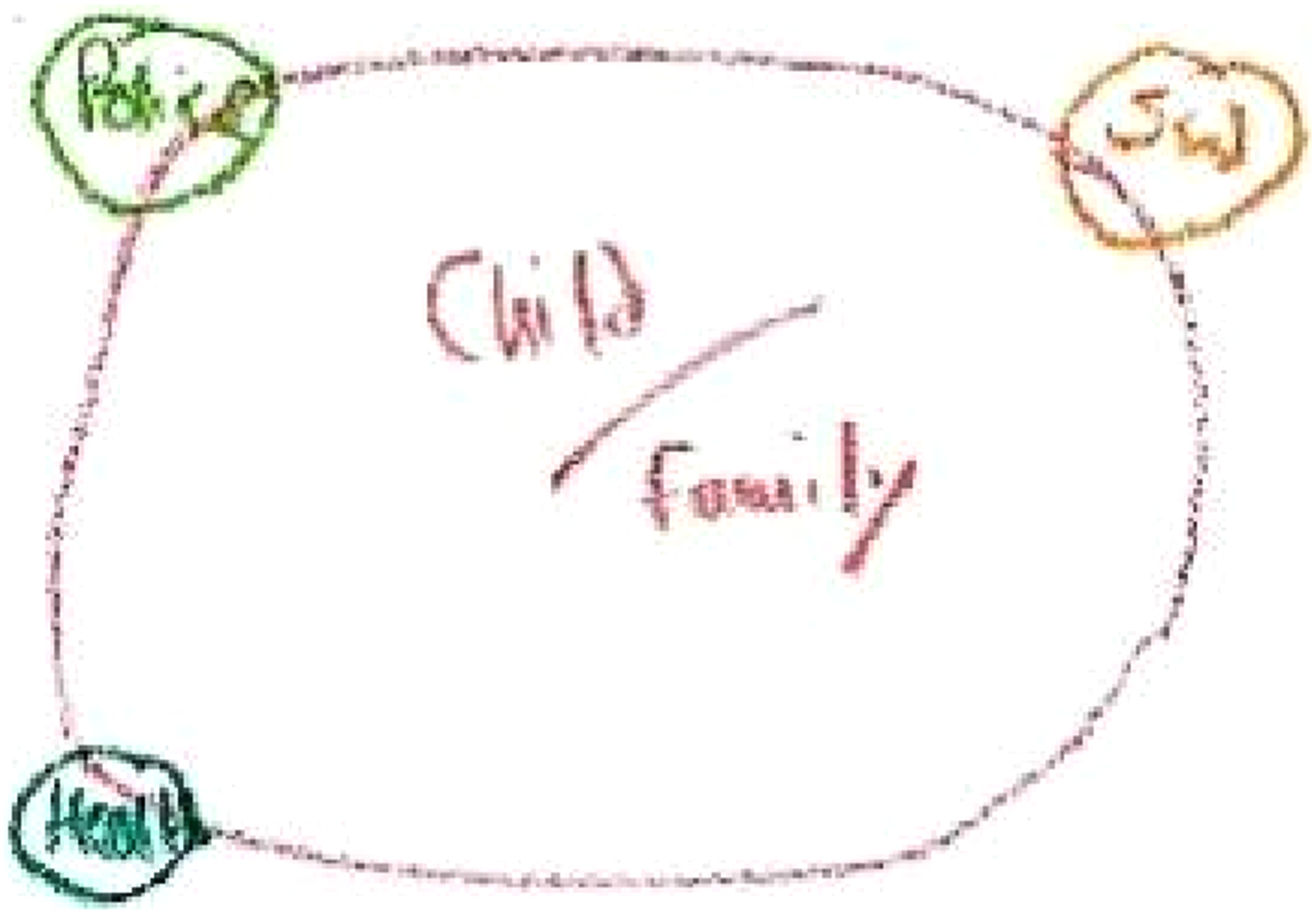
Figure 7 shows a large circle representing the negotiation table for collaboration, with different community partners “sitting around the table.” In the upper left corner, a chaotic tangle of red lines symbolizes communication breakdowns. This criticism is evident in SW7’s description of her sense of burden regarding the current state of collaboration, experienced as “chaotic,” “frantic,” and “a tad overloaded.”
At the centre of the image, a black circle symbolizes SW7’s hope that each professional can link together like a chain, learning from one another. However, in practice she found collaboration ‘performative’ - going through the motions and enacting rhetoric superficially. She points out: “Although we are at the table, I just feel like we’re not really at the table.” OP1 saw the current state of multidisciplinary collaboration as a circle (Figure 8). “Different departments are positioned at various corners providing support, rather than being in a true collaborative state.” Both participants reveal significant gaps between the ideal and the reality of collaboration. Despite the presence of formal structures, they indicate that the current process lacks effective communication and integration and highlight the need for genuine engagement and interconnectedness to improve outcomes in multidisciplinary work.
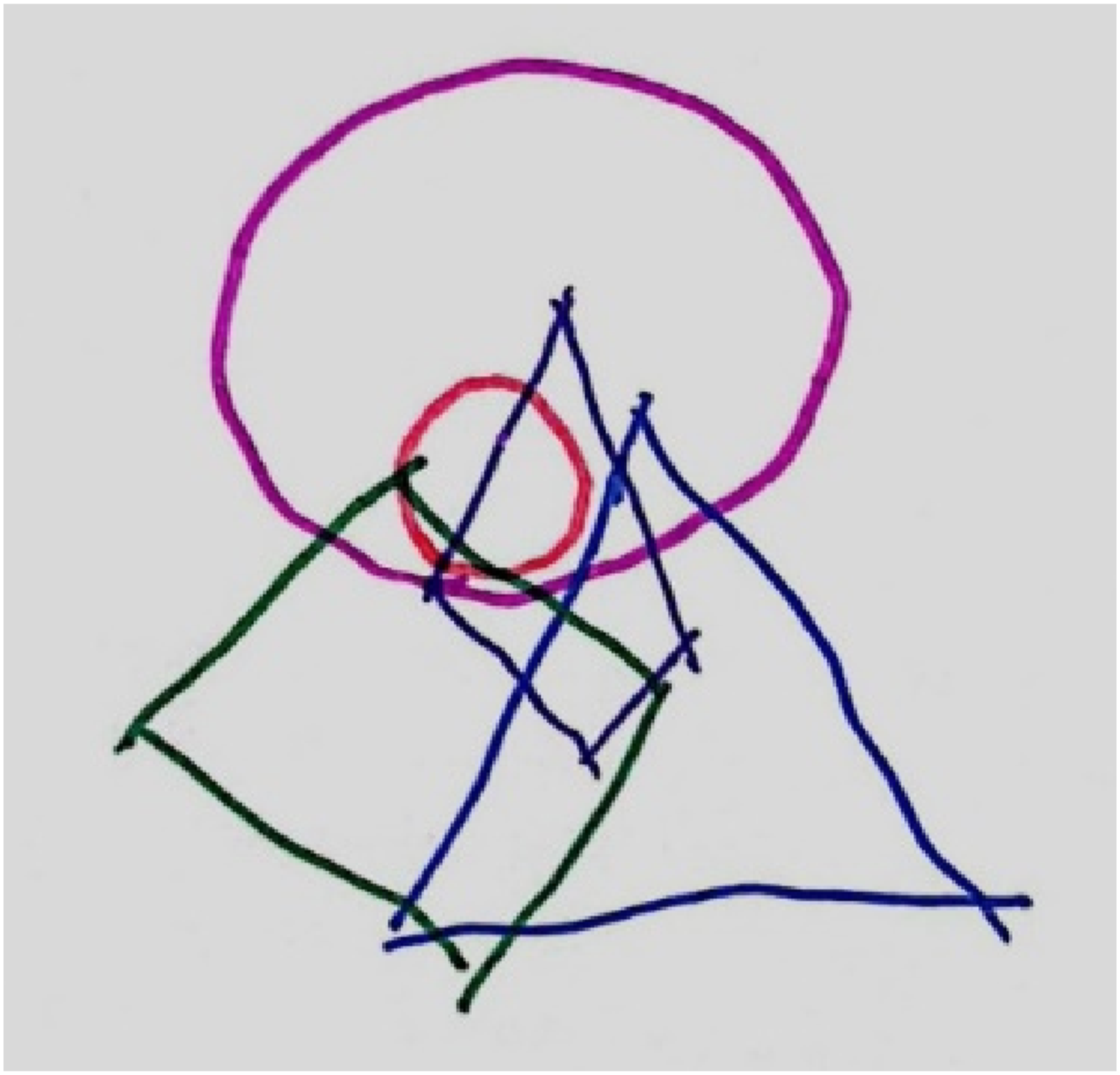
Figure 9 uses a layered structure, with the outer circle representing key departments and the inner circle labelled “Police legislation, rights, and obligations”. Lines connecting each service to the inner circle symbolize varying interpretations of these legal and policy concepts, identified as a major cause of collaborative difficulty. (SW 8).
Using the social worker role as an example, SW8 highlights how these differences manifest in practice. …Social work in New Zealand is obviously guided by different legislation. We have rights and obligations as social workers, and policy influences our work. I think we don't all have a shared understanding of what that means within different roles, leading to disconnect and misunderstanding.
In Figure 10, OP2 emphasizes that while collaborating professionals’ aim for the same result, systems are not in tune: I see crisis support sort of part of Health… that dotted line means it's a little bit of fractured relationship. Ultimately, we're following two separate paths to achieve the same outcome…safety, well-being, and prosecution…But not quite (sure) how it accountable… So two different paths, same sort of objective, but quite fractured. (OP2).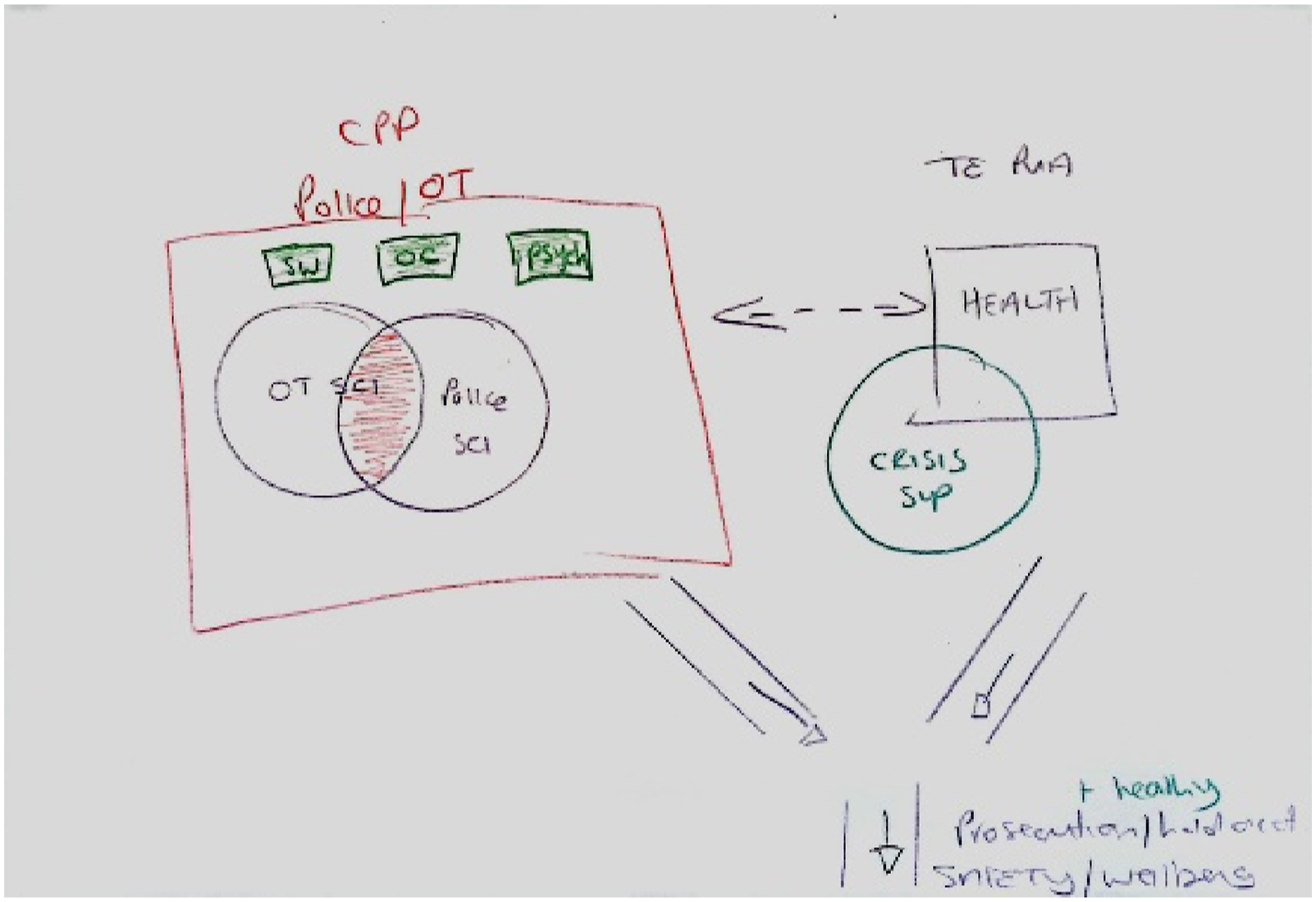
Therefore, even when goals are shared, the lack of a coherent accountability structure in multidisciplinary collaboration can lead to weakened partnerships.
Theme 3: Complexities within collaboration
The third theme highlights the complexity of collaboration in child protection. This stems not only from the inherent intricacies of child abuse cases but also from interactions between various departmental staff, communication dynamics, and management of case timelines. Together, these factors complicate the process and make it challenging to visually represent the collaboration involved.
Figure 11 uses traffic signs as a metaphor to show how the smoothness of collaboration depends on the partners involved. SW9 stresses the difficulty case complexity poses for collaboration difficulties. She emphasizes that effective collaboration occurs “when everyone is on the same page and communication is clear, allowing things to progress smoothly”. (SW9).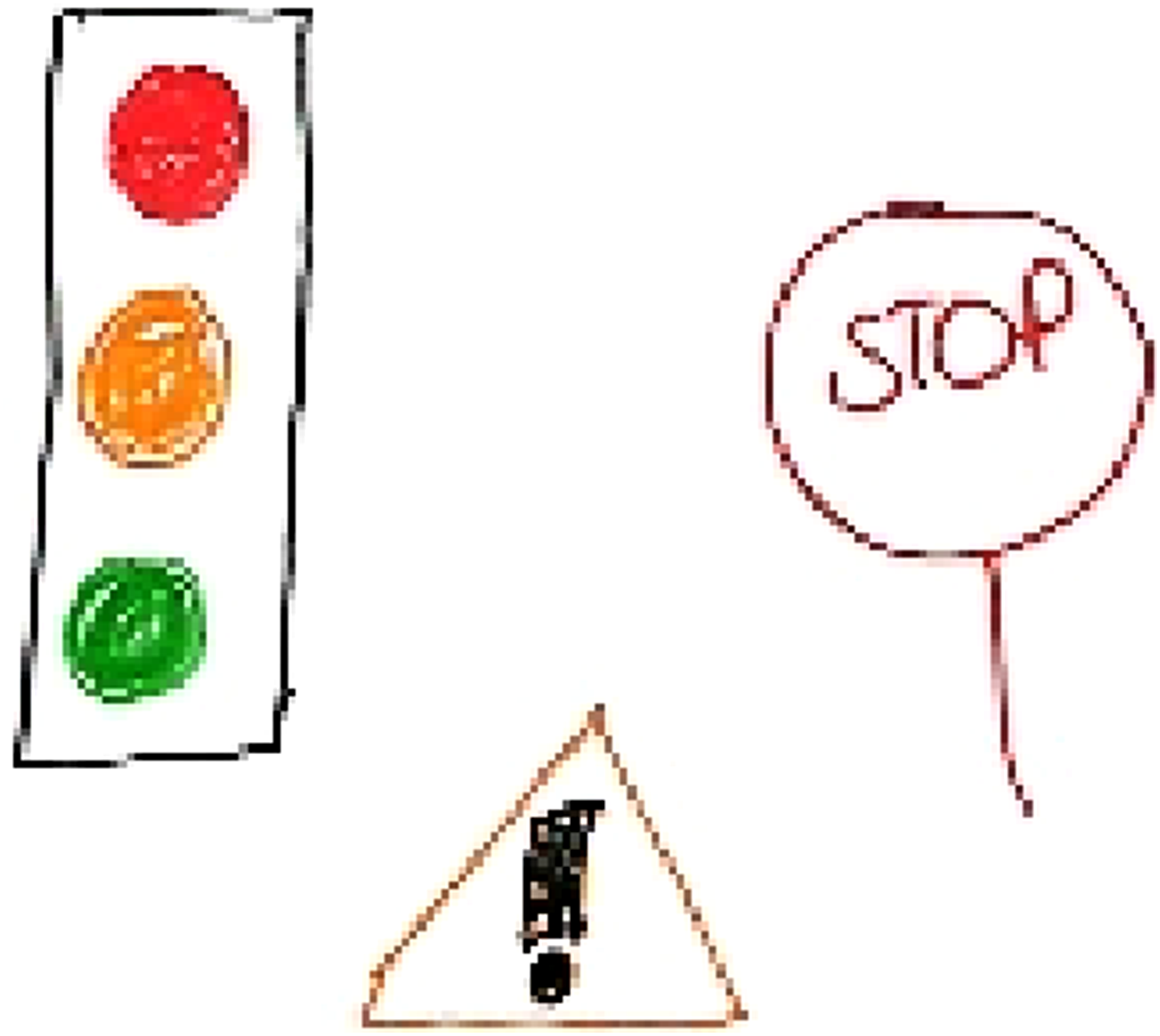
Figure 12 illustrates complex dynamics affecting the crisis intervention team’s work with different sectors. Wave-like lines symbolize a harmonious relationship with the health system, reflecting well-coordinated cooperation: “This is us as a full line… it’s a lot more in harmony.” In contrast, sharp lines represent a turbulent relationship with the police: “My relationship with police is very up and down.” Grey, blurred lines highlight the ambiguity in the relationship with OT: “I don't know what's happening. To me, it's just a fog. It's not bad. It's not good.” (OP4) (OP4).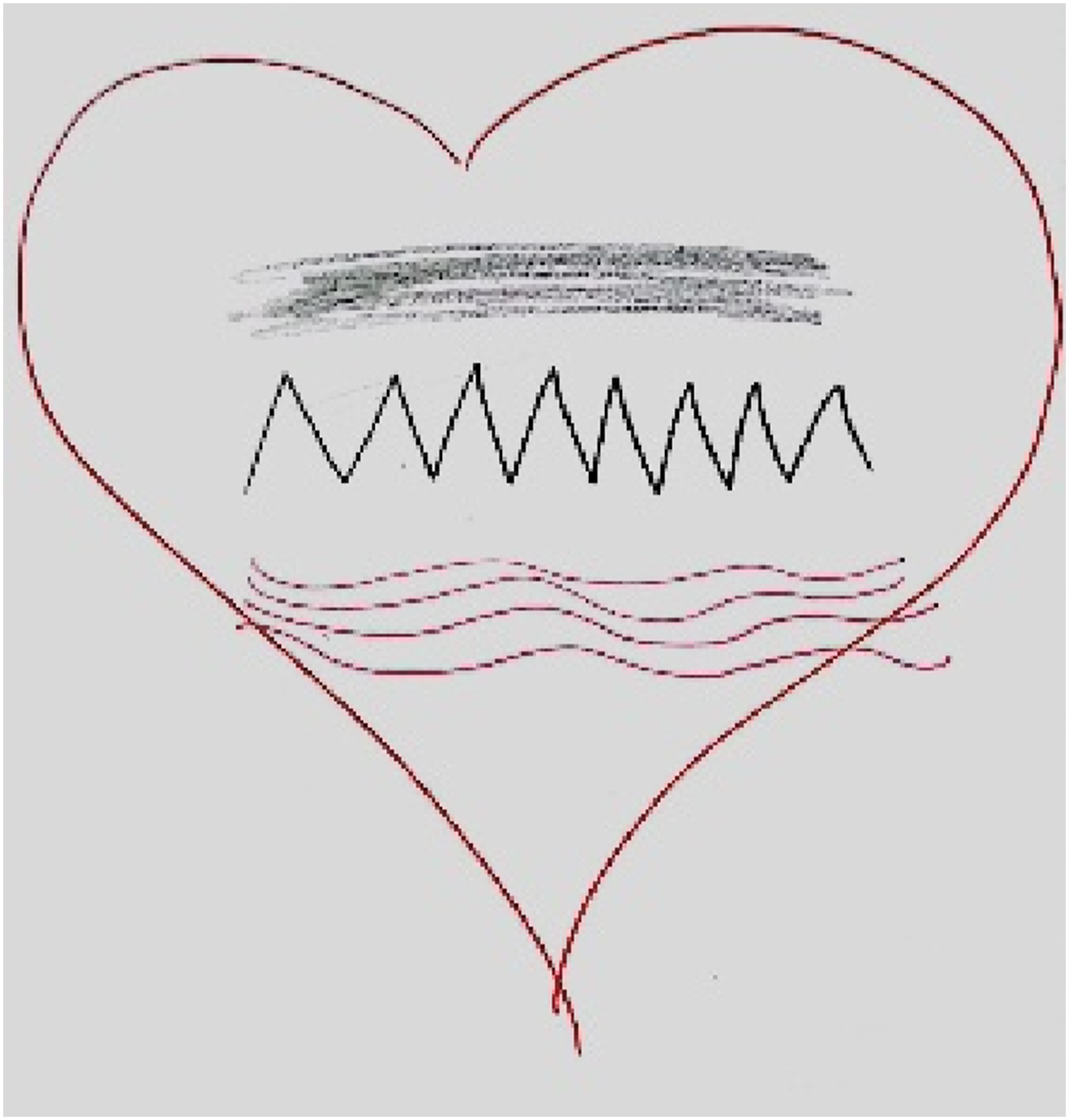
Although multidisciplinary collaboration is driven by shared positive intentions—symbolized by a large heart in the figure—interactions between partners are complex.
Figure 13 emphasizes the temporal and situational complexity of multidisciplinary collaboration in child protection. By illustrating a web of intricate connections, it highlights how professionals are interconnected yet interact at different times and for various reasons. “We all connect with each other at different periods, and for different things, different reasons… So, this person connects with this person, which then may connect with me …We might not connect with each other at exactly the same time place for the exact reason.” (SW10) (SW10).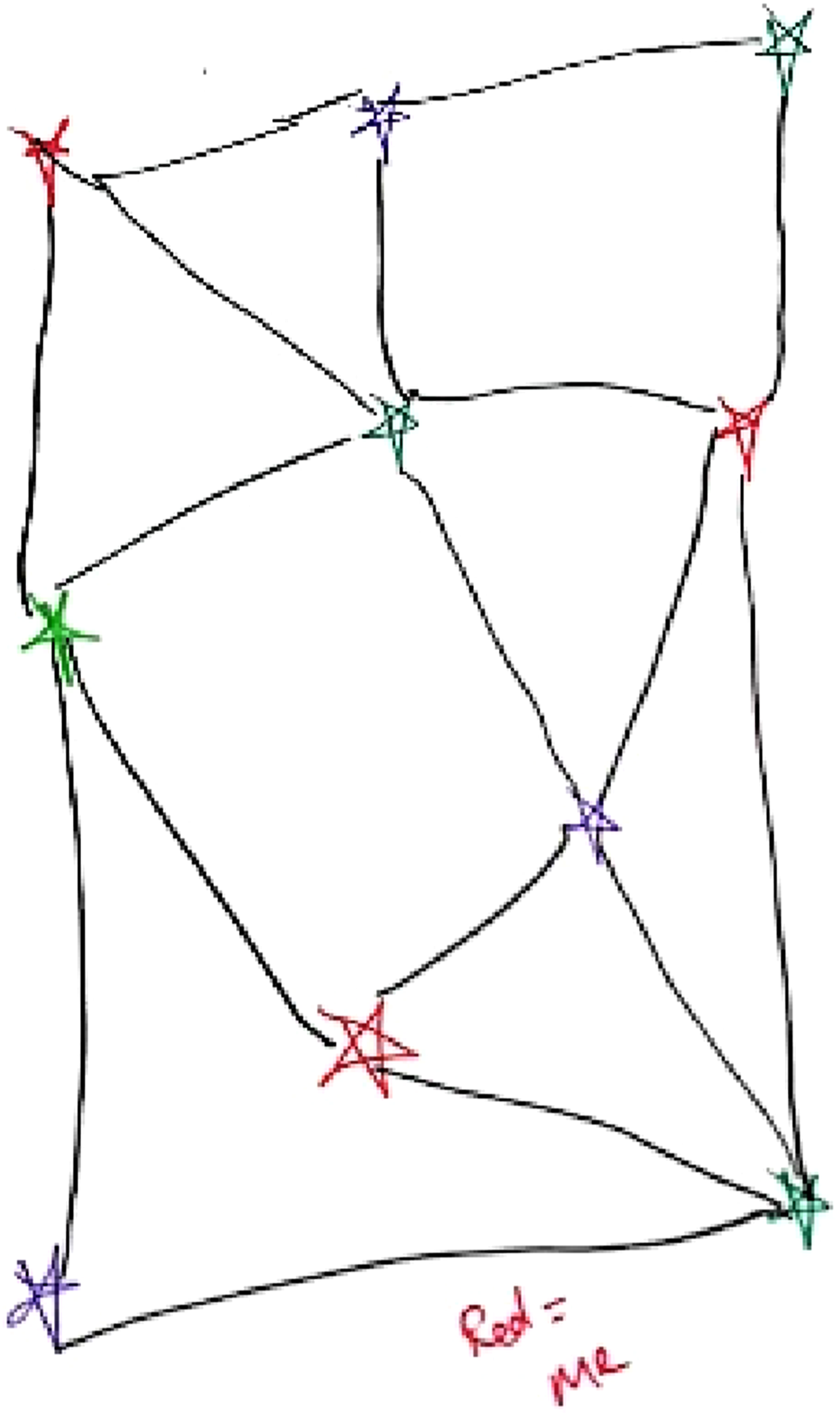
In child sexual abuse cases, where interventions sometimes span long timelines, collaboration occurs in a fluid, non-linear manner. Multiple stakeholders may be involved, but they do not always work simultaneously, have direct interaction or involve the same individuals, adding a layer of unpredictability to the collaboration process.
OP5 found herself unable to complete her drawing due to the multifaceted nature of child sexual abuse cases and the collaboration process. She provided a detailed explanation of complexities in case collaboration (Figure 14). “The difficulty with this is that there are so many possibilities because you come together for the consult, and basically, there are four different outcomes that can happen: no action, OT only, police only, or both police and OT…”
OP5 highlighted the short-term and fragmented nature of collaborative practice, noting that the limited involvement of different professionals, such as OT and the police, restricts the depth and continuity of their collaboration. “Of 100 cases I handle, less than 5% continue beyond the initial stage. Once the child or young person is safe, and initial safety planning has been completed, there’s no need for further involvement. The only cases that continue are those involving children under custody orders and that number is very small. So, ongoing collaboration isn’t a significant factor.” “My ongoing collaboration happens because of new cases coming in, not because of long, drawn-out investigations. There’s no collaboration because…OT is gone within the first month. After that, it’s just the police.” (OP5). Drawings of the health team on multidisciplinary collaboration (OP6). Drawings of the health team on multidisciplinary collaboration (OP7). Drawings of the health team on multidisciplinary collaboration (OP8).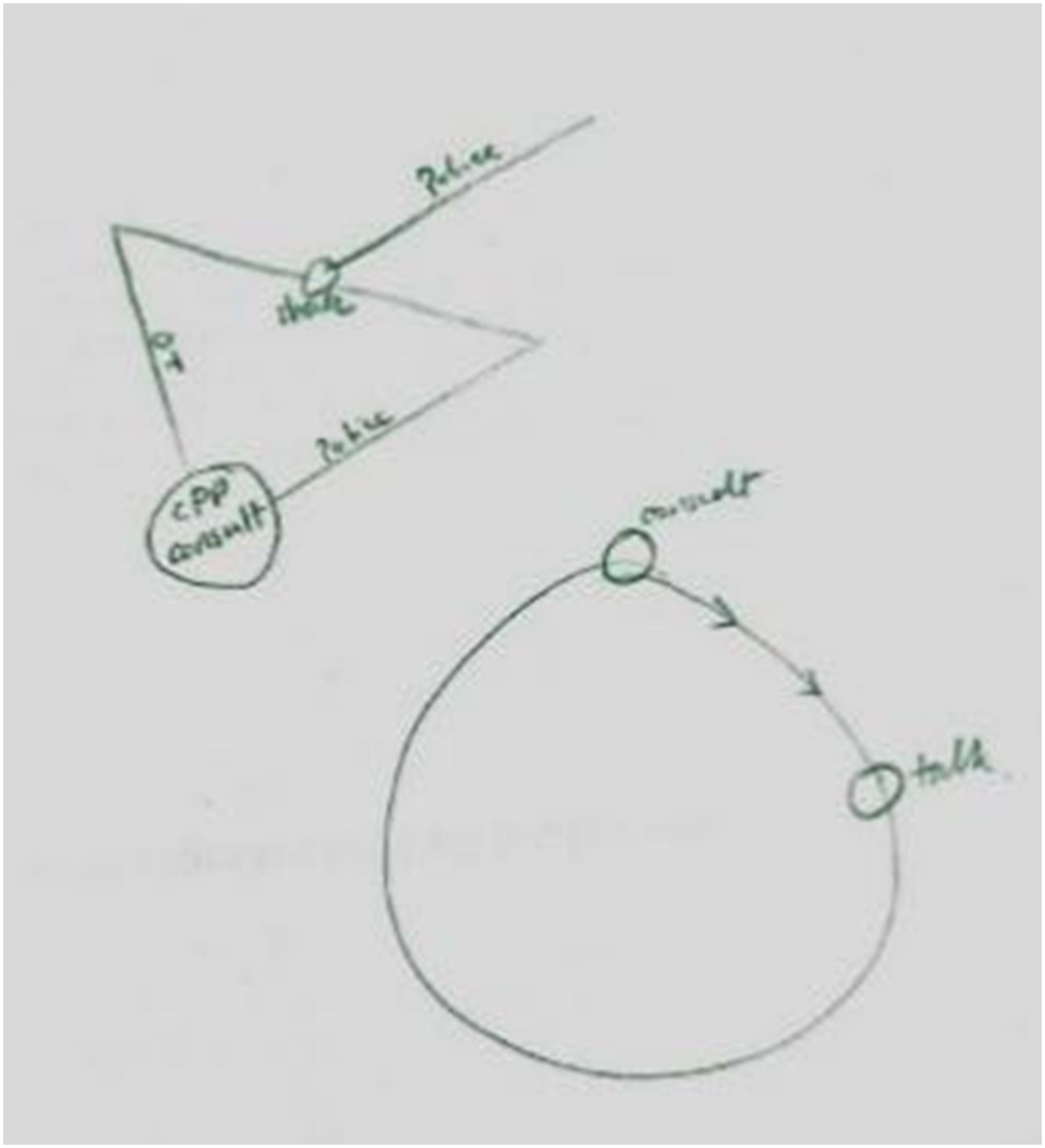
Theme 4: Health professional specificity in collaboration
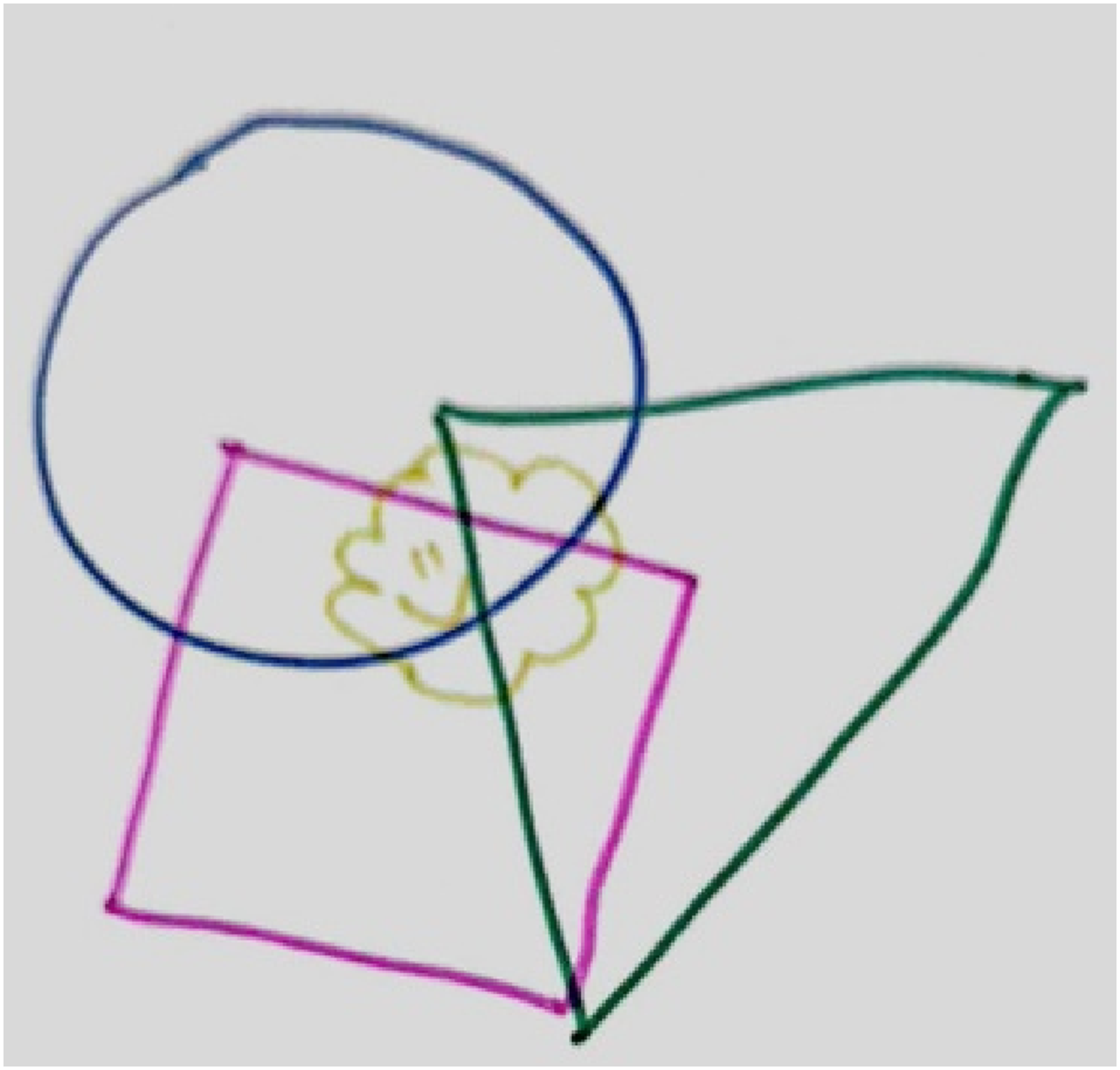
The drawings from health professionals present distinct characteristics: clear role divisions, crisis intervention features, collaboration in overlapping support, and challenges in working with OT (Figure 15, 16 and 17).
These drawings above convey that each role within the health team has its own specific responsibilities, or as OP6 said, “things that are separate that we do”, with professionals independently managing their own tasks and addressing child and family needs from their own professional perspective. “We're working together, but in my experience, I would tend to do more of the frontline work with the child... whereas a social worker is doing more of the frontline work with the support person or whānau...” (OP8)
While collaborating professionals have specific duties, there are overlaps in their work, as illustrated by intersections between different shapes in the drawings. Collaboration involves professionals relying on one another to complement and expand their perspectives. “We're thinking about what the other person isn't thinking about... trying to not double up or not miss anything at the same time - that's working together, isn't it?” (OP8)
Awareness of the limited nature of intervention was evident, due to interactions with families and children usually being short-term, and crisis driven. “I don't think anyone ever has a full view…the child and family's life is so much bigger than us...interaction with the child and family...is often just at a crisis point... We just are a drop in the bucket.” (OP7)
The health team highlights challenges in collaborating with the OT, particularly with communication and overlapping roles. “I think there's a lot of frustration... it can take hours to get on the phone to [OT].” (OP6) “Not sure if I've got OT right here, but they're often working with other parts of the child and the family - the purple diamond shape sort overlapping with our social workers role” (OP7)
Discussion
This study used an art-based method, incorporating drawing and interview techniques, to explore the experiences and perspectives of professionals from different roles on multidisciplinary collaboration in child protection. Data analysis produced four key themes: The Value of Child and Family-Centred Collaboration, Challenges in Collaboration, Complexities within Collaboration and Health Professional Specificity in Collaboration.
While this research revealed diverse understandings among a range of professionals regarding multidisciplinary collaboration, participants who were social workers displayed remarkable consistency in emphasizing collaboration, highlighting their strong focus on teamwork and egalitarian, trusting relationships. Collaboration is deeply rooted in social work values. For instance, the New Zealand Social Workers Registration Board’s Principle 8 (2024) underscores the importance of collaboration and open communication among colleagues. Similarly, the ANZASW (2019) Code of Ethics highlights kotahitanga (unity, solidarity, collective effort) as a core value.
Zweifel and Van Wezemaela (2012) categorized collaboration models into three types: a round table, a network, and a hierarchy. In this study, social workers’ drawings align with the “round table” model, symbolizing unity and equality. This idealized view indicates values and aspirations that social workers bring to child protection collaborations. However, multiple drawings suggest that real-world multidisciplinary practice is fraught with complexity and professional frustration.
Health professionals’ drawings emphasized the unique roles and complementary functions of various professions, represented by overlapping shapes. This focus on practical realities and defined role boundaries may stem from the inherently close teamwork of health teams, which fosters a clearer understanding of each member’s function. A transparent understanding of roles and acceptance of each other’s contributions can effectively foster trust, a known facilitator of collaboration (Herbert et al., 2020). However, this pragmatic perspective differs from social workers’ idealized view of collaboration, potentially leading to differing expectations about collaborative modes and processes.
Regarding barriers to multidisciplinary collaboration, this study echoes findings from previous research (e.g., Cooper et al., 2016; Price-Robertson et al., 2020). Statutory child protection social workers highlighted issues such as mismatched goals, ineffective communication, and differing understandings of policies and roles, leading to trust deficits and potentially chaotic practice. This study also highlighted the challenge of unclear accountability in collaborations between Crisis Support, OT, and the police, stemming from unstable partnerships, ambiguous collaboration processes, and differing priorities. This reflects Bovens’ (2007) research about “problem of many hands,” where fragmented responsibilities and inconsistent frameworks obscure accountability, making it unclear which agency should take the lead or hold responsibility for outcomes.
Overall findings also emphasise the significant impact of the complexity inherent in child protection cases and systems on professional collaboration. The complex contexts of differing cases, professional differences, and misaligned schedules across departments often hinder collaborative efforts (Darlington et al., 2005; Eilfgang et al., 2024).
These challenges can also be viewed as manifestations of subtle, silent struggles for discursive authority, interpretive power, and decision-making rights (Villumsen and Kristensen, 2015). For example, in New Zealand, tension can characterise the relationship between OT and other organizations. In the Puawaitahi context, this is potentially influenced by the fact that OT social workers are not co-located with other services connected to the Puawaitahi model. This resistance may be a strategy to protect the boundaries of professional jurisdiction, indicating unresolved power struggles (Johansson, 2017).
Reflections on drawing as a research methodology
This research used the draw-and-talk technique to explore participants’ perceptions of the complex topic of multidisciplinary collaboration. As Zweifel and Van Wezemaela (2012), p.10) noted, drawing can serve as a method for “making visible of integrated worldviews and internal models that people all have.” In this study, the combination of drawing and in-depth interviews not only enabled participants to express their emotions and experiences of collaboration but also revealed implicit understandings and expectations about multidisciplinary teamwork. Drawing made the intrinsic values and subconscious models of professionals visible, capturing latent characteristics that are difficult to articulate through language (Hartel et al., 2018; Rose, 2016). Furthermore, the post-interview approach (Brailas, 2020) in which drawing is incorporated as the final step of the interview process rather than as an entry point, helped participants quickly focus on key memories and impressions of complex situations. Drawing served not only as a tool for expression but also as a medium for reflection, enabling participants to identify and highlight significant aspects of their collaborative experiences.
Concerns surrounding the use of drawing in adult research can be mitigated. While some participants initially expressed concerns such as “I can’t draw” or “I might not do it well”, and one was unable to complete their drawing due to the complexity of the system, none refused to draw. This counteracts suggestions in the literature that adults often need to overcome preconceived notions about “good” or “bad” drawings, stereotypes about “artistic” abilities, and concerns about their drawings being perceived as “childish” (Lyon, 2020). Trepidation was relieved through gentle guidance and clarification by the interviewer, using the following simple strategies: (1) Clarifying that the goal of the drawing exercise was to capture thought processes. (2) Providing multiple options for expression, including lines, shapes, colours, or simple symbols. (3) Emphasizing that participation in the drawing activity was optional, with participants free to respond verbally instead. Furthermore, drawing is just one option; future research could consider incorporating other expressive mediums, such as coloured markers, sand trays, or LEGO blocks, to provide additional flexibility.
Limitations
There are several limitations to this study. The participants were generally spent 10–15 minutes to complete and explain their drawings as the post-interview approach, this may not have allowed for the same depth of exploration as when drawing is used as a primary research method at the beginning of an interview. Future research could explore the use of drawing as both a primary tool and a reflective method, potentially incorporating extended interviews that provide participants with additional time to refine their images and engage with follow-up questions. Such approaches may deepen engagement and enrich insights from participants, making art-informed methods an invaluable approach for exploring abstract and multidisciplinary topics. Another limitation relates to the gender composition of the participant group, as all were women. This may limit understanding of whether gendered professional experiences influence how participants engage with art-informed methods. Future research could include a more diverse participants to explore potential gendered dimensions of visual expression and reflective practice.
Conclusion
Art-informed research methods, particularly the integration of drawing and interviews, provide a unique tool for exploring the complexities of multidisciplinary collaboration. This study highlights differences in the understanding of collaboration between social workers and health professionals, offering critical insights into collaborative practices in child protection. It identifies key challenges in the Auckland, New Zealand context, including communication gaps, inconsistent goals, lack of accountability mechanisms, and different understanding of polices and roles. Tensions between Oranga Tamariki (OT) and other collaborators were also highlighted, pointing to deeper structural issues within the system. This highlights the need to address power imbalances and conflicts that complicate teamwork. Two key recommendations are proposed to address these challenges. First, targeted multidisciplinary training and regular cross-agency communication platforms are needed to promote shared understanding of core concepts such as collaboration, risk, and safety, and to support mutual awareness of professional roles and responsibilities. Second, the structural power dynamics between key agencies require critical exploration, particularly the policy and practice-level imbalances that contribute to inter-agency disconnection—such as the lack of physical co-location of OT social workers. These broader systemic tensions are further explored in my doctoral research. While the research is limited in scale, its practical implications for improving understandings of multidisciplinary cooperation are significant.
It also demonstrates the value of drawing as a method in social work research, revealing non-verbal and often unconscious differences in professional perspectives Beyond its academic contribution, this method holds practical potential for professional training. For example, practitioners could be invited to visually represent complex concepts in child protection—such as collaboration or thresholds of risk—and then engage in group discussions. Such exercises can help make underlying differences in understanding more visible, fostering deeper mutual recognition and more effective multidisciplinary cooperation.
Footnotes
Acknowledgments
I extend my sincerely gratitude to all the participants in this study for their tremendous support throughout the process. Thank you for generously sharing your professional knowledge and experiences. Sincere appreciation to Dr Brian Rodgers and Dr Laura Ann Chubbs for their constructive feedback.
Ethical approval
This study was approved by the University of Auckland Human Research Ethics Committee (approval no. UAHPEC25252) on Feb. 8th, 2023. All participants provided informed consent and agreed to have their drawings published as part of this research paper.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the author(s) received financial support from Chinese Scholarship Council and University of Auckland joint scholarship for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.