
Abstract
Few studies have explored the moral and ethical dimensions of how, in practice, social workers talk about and handle cases as part of their daily work. At the same time, identifying and examining the ethical dimensions of actual social work practice can be challenging because ethics is often hidden within the complex particularities of daily work. This article applies and develops Sarah Banks’ conceptualisation of “ethics work” to examine how care managers in Sweden are “doing ethics”, while seeking and providing collegial support and guidance on how to deal with the wishes of adult (potential) service users who are reluctant to accept support – or whose wishes in the matter are difficult to determine. The study is based on an analysis of 14 audio-recorded case conferences. With the help of Banks’ conceptualisation, the analysis makes visible how the case discussions in question encompass a complex “doing of ethics”, by means of which the welfare of individuals is balanced against care managers’ legal duty to adhere, without exception, to the principle of self-determination. The findings suggest that further research that applies and develops Banks’ conceptualisation of ethics work by examining “actual” social work practice in situ, while recognising the particularities of the social and societal context in which this work is taking place, could provide new knowledge and understanding about both the specific and common challenges that social workers face in different parts of the world. It could also make the ethical dimensions of social work practice more widely recognised and valued.
Introduction
“Care manager” is the title for social workers in Sweden whose formal role is to assess individual needs for social services such as home care or residential care (in Sweden: special housing). Since the 1980s, Swedish law advises care managers to apply the principle of self-determination, without exception, in cases concerning adults who need social services to manage their daily living. 1 To grant or provide social services, informed consent from the individual is needed, and no direct or indirect pressure is allowed to obtain this consent (Giertz et al., 2021). Consequently, to act in accordance with the law, care managers are obliged to always respect the wishes of adults, including in cases where informed consent is difficult to obtain due to issues such as communicative or cognitive difficulties on the part of the (potential) service user. This includes cases where the individual’s explicit point of view clearly differs from the social worker’s assessment of their needs – and with the opinions of relatives and health professionals. In contrast to the situation in many other countries, there is no legal support for the use of autonomy instruments to assess the decision-making capacity of adults, and relatives have no formal role in deciding on behalf of someone such as an older mother or father (Mattsson and Giertz, 2020; Nedlund and Taghizadeh Larsson, 2016). The Swedish National Board of Health and Welfare (NHBW, 2017a; 2017b) provides guidance to social care professionals on how to support “older people” and “adults with disabilities” “with reduced decision-making capacity to express their wishes”, for example by employing different types of communication aids, but do not question the importance of fully adhering to the expressed wishes of all adults. Issues such as potential differences between expressions of “irrational wishes” and reasoned preferences are not raised or discussed.
One way to understand why this route has been chosen as part of the Swedish welfare system when it comes to self-determination, is to consider Sweden’s history of abusive acts, such as compulsory sterilization, which was carried out against adults with intellectual impairments, among others. Thus, the current approach was intended to reduce the risk that some adult citizens do not receive the respect due to them or that they become the objects of similar abusive acts (cf. Giertz et al., 2021). However, a perhaps unintended consequence acknowledged by some researchers is that Swedish law is more directed towards protecting the self-determination of its citizens than to ensuring that relevant support and protection are provided to those adults who have a reduced capacity to decide for themselves (Nedlund and Taghizadeh Larsson, 2016; Nielsen, 2012).
Purpose and research questions
By applying, and developing, Banks’ conceptualisation of “ethics work”, this paper examines how care managers (immediate managers included) in Sweden are “doing ethics” while – in practice – seeking and providing collegial support and guidance on how to deal with the preferences of adult (potential) service users who are reluctant to accept support – or whose wishes in this matter are difficult to determine.
The following questions are central: • How do care managers deal with their legal duty to adhere to the principle of self-determination? • What dimensions of “ethics work” can be identified among the care managers dealing with this legal duty?
Although there are several studies about the ethical aspects of social work (e.g. Banks et al., 2020; Segal and Gur, 2023), only a few studies (i.e. Saario et al., 2018) in this field have used naturally occurring data (Silverman, 2015) to examine how social workers or other welfare workers do ethics in situ. The present paper addresses this gap in knowledge as it is based on an analysis of 14 audio-recorded internal case conferences between care managers, encompassing discussions on 16 cases. The purpose of the paper is to contribute to understanding and knowledge about the ethical dimensions of contemporary social work practice, including the challenges that social workers may face in specific welfare contexts, and how these are addressed in practice.
Ethics work
In using the term “ethics work”, Banks (2016: 3) is referring to the processes and “efforts of noticing, attending, thinking, interacting and performing” that social work professionals “put into seeing ethically salient aspects of situations, developing themselves as good practitioners, working out the right course of action and justifying who they are and what they have done”. Banks concretises and conceptualises what this ethics work might entail by presenting a number of ethical dimensions or features (outlined in the methods section) of the sense-making work that social workers do in practice, which she has identified through interviews with social workers and first-person written cases collected over many years.
Banks (2016) situates her work as part of a growing trend in the field of social work ethics and professional ethics. Common to the literature in this field is that it seeks to broaden the domain of professional ethics, which is dominated by principle-based approaches, to acknowledge ethics as embedded (and embodied) in everyday practice. This broadening ambition entails positioning dilemmas and decisions within a social, political, and cultural context and acknowledging responsibility in a relational sense, as stretching beyond the isolated individual decision-maker. In the present study, this is acknowledged by examining the ethics work accomplished by care managers as part of case conferences taking place in a specific (Swedish) welfare context.
Banks herself acknowledges that her conceptualisation of various dimensions of “the doing of ethics” in social work is drawn from accounts that have been given by social workers in response to explicit requests for ethics cases. As a way of further using and developing the conceptualisation, she discusses its potential for analysing social work practice in situ, based on material such as recorded team discussions.
State of the art
The literature on moral considerations, ethical dilemmas and conflicting pressures in social work and social welfare practice is extensive and includes social workers’ perceptions, experiences and (re)tellings of dilemmas that they have encountered (e.g. Banks, 2016, 2018; Corvol et al., 2012; Segal and Gur, 2023; Ylvisaker and Rugkåsa, 2022; Östlund et al., 2023) and – to a considerably lesser extent – how dilemmas are handled in practice, e.g. in recorded interactions between professionals during meetings (Juhila and Raitakari, 2010). In recent years, in collaboration with researchers from Finland, Banks has applied her conceptualisation of ethics work to “naturally occurring” audio-recorded data as part of a study of meetings in community mental health settings in the UK and Finland, where welfare workers, service users and other stakeholders take part and deal with everyday practical issues relating to the lives of service users, drawing primarily on ethics work as “performance work” that includes and requires “reason work” and “role work” (Saario et al., 2018). The present study adds to this analysis of how ethics work is actually done, in practice, by acknowledging all seven of the features encompassed by Banks’ conceptualisation. We have done so in order to analyse “naturally occurring”, internal, case discussions among social work colleagues in the welfare context of Sweden. We also suggest two additional features to be added to Banks’ (2016) original conceptualisation.
Concerning the challenges and dilemmas related to the principle of self-determination and reluctant clients, studies carried out in Sweden (Nilsson and Olaison, 2022; Nordström and Dunér, 2001; Österholm et al., 2015) and other countries (e.g. Messmer and Hitzler, 2011; Suoninen and Jokinen, 2005), have shown how subtle persuasion, coaxing and asking closed question, are employed ‒ including by social workers in Sweden ‒ to achieve various activities despite greater or lesser degrees of reluctance on the part of clients. According to Corvol et al. (2012:88) these strategies are blurring the boundaries “between the measures actually accepted by an individual and those imposed in one way or another by the case manager”. Also adding to this area of research, the present study provides insights into considerations and discussions among social work colleagues preceding that such strategies are applied in practice.
Material and methods
Data was collected in four Swedish municipalities. Contact was established with the immediate managers of care managers – i.e. care managers holding managerial positions – at local social work agencies. All of these immediate managers gave consent, so we were also able to inform the care managers in a subordinate position at these agencies about the study and ask if they were willing to participate. Written informed consent was given by all the care managers individually before data collection began. Each immediate manager, who was also responsible for leading and organising the case conferences, was then provided with an audio recorder. This person also decided which conferences to include, and when to begin and end the audio recordings. No researchers were present during the meetings, but the audio recorders were collected at the end of the data collection in the office. In total, 39 case conferences were recorded. All audio recordings were transcribed verbatim by a professional transcription company, using a modified version of the Jefferson (2004) transcription system.
An ethical review of this study was carried out by the Swedish Ethical Review Authority (Dnr. 2019-05965).
Analysis
For the analysis presented in this paper, Banks’ work on ethics and values in social work and her conceptualisations of different features of ethics work were applied as analytical tools to a total of 16 case discussions, pertaining to 14 recorded case conferences from the dataset. The following description of the features of ethics work is taken from Banks (2016:4): 1. Framing work – identifying and focusing on the ethically salient features of a situation; placing oneself and the situations encountered in political and social contexts; negotiating/co-constructing frames with others (including service users and colleagues). 2. Role work – playing a role in relation to others (advocate, carer, critic); taking a position (partial/impartial; close/distant); negotiating roles; responding to role expectations. 3. Emotion work – being caring, compassionate and empathic; managing emotions; building trust; responding to the emotions of others. 4. Identity work – working on one’s ethical self; creating an identity as an ethically good professional; negotiating professional identity; maintaining professional integrity. 5. Reason work – making and justifying moral judgements and decisions; deliberation with others on ethical evaluations and tactics; working out strategies for ethical action. 6. Relationship work – engaging in dialogue with others; working on relationships through emotion, identity and reason work (dialogue work). 7. Performance work – making visible aspects of this work to others; demonstrating oneself at work (accountability work).
However, the initial steps of the analysis were data-driven in the sense that we started in the data corpus when deciding upon our focus for further analysis. As a start, the transcripts from all the audio-recordings were read to gain an overall picture of the (39) case conferences; that is, the issues that care managers raised and discussed at the meetings. During this phase, we decided to pursue an analysis of the sequences relating to (potential) service users who were reluctant to accept the services offered to them, or when the individual’s preferences were difficult to determine. These sequences relate to the subset of 14 case conferences analysed in the present study. The initial motive for choosing these conferences for further analysis was that they were considered intriguing due to the lack of obvious fit with how, in previous studies, care managers have largely been described as the (municipal) organisations’ extended arm, devoted to fulfilling political and administrative requirements (Lymbery and Postle, 2015; Olaison and Donnelly, 2022). In the sequences during the 14 conferences in question, the care managers seemed preoccupied with, and unsure about, (the moral and ethical question of) how to work out “the right course of action”, to both meet recognised needs and protect the self-determination of individuals, rather than issues such as whether (potential) service users’ needs meet municipal and administrative criteria for receiving certain services. Thus, a focus on the ethical dimensions was deemed a relevant choice for analysis, as was, subsequently, Banks’ (2016) writing on ethics work.
The data corpus was scrutinised by the first author to identify all sequences involving the issue of (potential) service users who were reluctant to accept the services offered to them, or where the individual’s preferences were difficult to determine. Longer sequences from the transcripts (i.e., from the utterance that introduced the case until the discussion on the particular case was finished) were then extracted to make sure that utterances were analysed in relation to the context (Braun and Clarke, 2006). As a result, 16 case discussions were extracted, pertaining to 14 of the 39 recorded conferences and representing all four municipalities.
In practice, the application of Banks’ (2016) conceptualisation as an analytical tool meant that the extracted data set was scrutinised by the first author to identify, code and collate data sequences via an iterative process that involved checking if, and if so how, the sequences related to the features of ethics work as described by Banks. We also suggest two additional features to be added.
Results
In this section, we first provide some contextual information regarding the recorded case conferences, and then present our analysis of care managers’ ethics work on the preferences of adult (potential) service users. All the names of people and places in the paper are fictitious to ensure confidentiality.
The case conferences
The case conferences differ in terms of what is being talked about, in that they are focused on individual cases or more general issues and questions concerning the care managers’ work. However, the majority of the talk during the case conferences is devoted to discussions on separate, individual cases, with one case (one individual) being dealt with at a time. At an overall level, these case discussions comprise three distinguishable phases: (1) Case presentation: a care manager introduces a case that she (or he) is responsible for assessing. (2) Input and discussion among the participants. (3) Rounding: agreement on points such as whether an application for a certain type of support should be approved or rejected – or how the care manager responsible for assessing the case should proceed.
This structure resembles how planned intra-professional meetings in other areas of social work, in other countries, have been described (Taghizadeh Larsson et al., 2023).
Ethics work on the wishes of adult individuals
During the (16) case discussions, an adult individual’s wishes – in terms of reluctance to receive social services, or unclear preferences – is introduced, either by the care manager responsible for assessing the case during the first presentation phase of a case discussion (six case discussions), or later, by another participant – in most cases the immediate manager, during the second phase of input and discussion among the participants (10 case discussions). Introducing the wishes of the individual during any of these phases also means making this dimension visible as a salient dimension of the case, which is identifiable as “framing work” (Banks, 2016: 4). The ethical dimension lies in the fact that the (ethical and legal) principle of self-determination then becomes highlighted as a relevant aspect of a judgement that in itself encompasses moral dimensions by virtue of having to do with how to act in relation to other humans and “deciding the right course of action” (Banks, 2016: 10) in a specific case. Consequently, throughout the rest of this results section, the term framing is used, to highlight that we identify what the care managers choose to say in similar accounts as (ethical) framing work.
Below, we first examine the ethics work done by care managers who raise the wishes of (potential) service users for whom they are responsible at their case presentations. After that, we focus on the doing of ethics accomplished by another participant at the meeting during the second phase of input in case discussions where the individuals’ wishes have not been raised by the care manager responsible for assessing the case during the case presentation. Lastly, we examine the ethics work done by the participants during the (16) case discussions when raising and discussing ways to proceed with the cases, after and beyond the meeting.
In reporting and asking for input on a problematic case
At an overall level, the case discussions in which the wishes/reluctance of a (potential) service user are introduced as part of the case presentation by the care manager responsible for assessing the case encompass a report of a problematic case and end with the care manager explicitly asking for input from the other meeting participants on how to proceed. Below is an excerpt from the latter part of one of these case presentations:
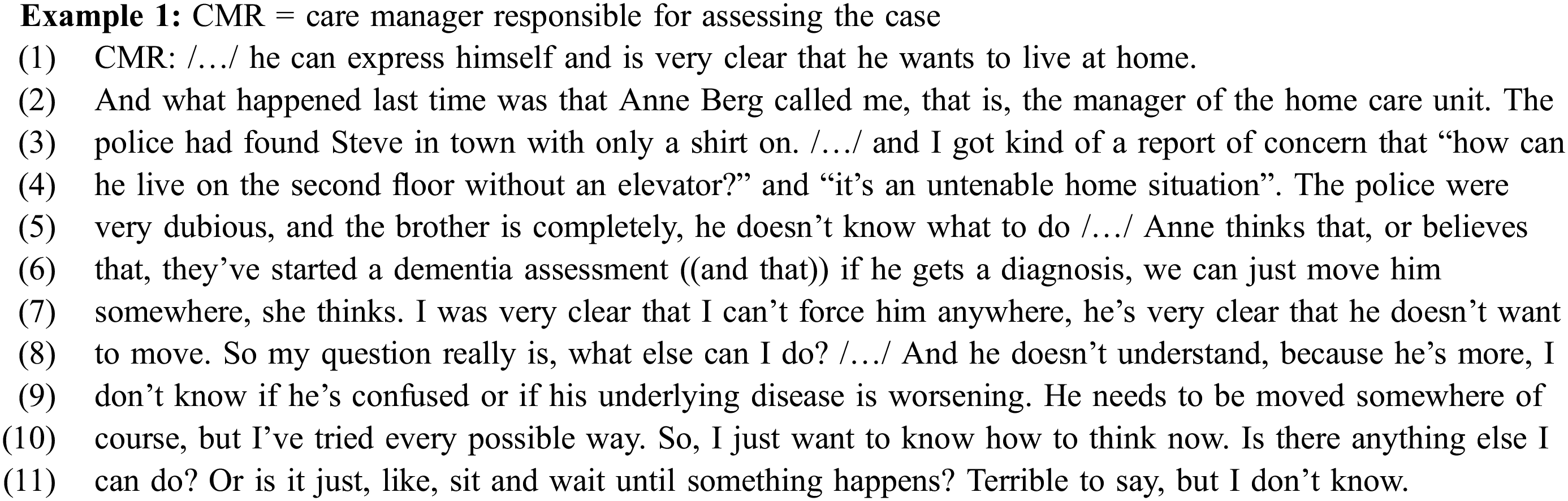
Several dimensions are framed as complicating this case, in an intermingled way, as in all the case presentations in question. In the excerpt above, this is illustrated by the care manager responsible for assessing the case talking in the first line about the wishes of the man in question in terms of his explicit reluctance to move to special housing, while at the end of her presentation (line 8-9) she also indicates that he has reduced cognitive abilities and reduced decision-making capacity. Furthermore, other parties – a brother, home-care staff and the police – are highlighted as engaged in the case and as putting pressure on the care manager to act because they believe that the man’s health and welfare is endangered (“found in town with only a shirt on”; “untenable home situation”).
A common thread across this type of case presentations is that they also include accounts where the care manager responsible for assessing the case refers to a situation in which she (or he) has told other parties engaged in the case (family members or other professionals) that she cannot grant or provide social services support without consent from the individual in question. In the excerpt above, this is visible in how the care manager (re-)tells how she has told the manager of the home care unit, “Anne”, that she cannot place the man in special housing without his consent (“I was very clear that I can’t force him anywhere”). Here we identify ethics work in the form of “identity work” and “performance work” (“accountability work”). That is, in accounts like these the care managers responsible for assessing the cases discursively perform and present themselves to their colleagues as adhering to the principle of self-determination, by explicitly protecting and supporting the right of individuals to make decisions about their own lives in situations where other parties or professionals consider this to be unnecessary or wrong. In other words, in these accounts, the care managers present themselves as aware of “the importance of professional integrity – acting in accordance with the values of the profession” (Banks, 2016: 10) – which encompass acting in a way that is accountable in relation to the legislation regulating the work of care managers in Sweden. This is also identifiable in how, throughout the case presentations, the care managers responsible for assessing the case frame the option of not acknowledging the wishes of the older adult as non-existent, by not – explicitly – raising this as an existing option. Additionally, they do not – explicitly – talk about themselves as faced with a dilemma where they must choose between adhering to the individual’s wishes or acting; for example, to make sure that the adult’s health or welfare is not endangered.
However, simultaneously, they are, implicitly, demonstrating an openness to negotiate and co-construct the legal framing of the principle of self-determination as inviolable with colleagues (cf. Banks, 2016: 4). This is accomplished by the care managers in question raising the cases for which they are responsible as problematic at a case conference in the first place, and then including an alternative course of action, which conflicts with the principle of self-determination, as logical and as the “right course of action”, while presenting the case. In the excerpt, this is identifiable when the care manager says: “he needs to be moved somewhere, of course” (line 9). In this way, the care manager in the example is implicitly framing the problem for which she is seeking input as a matter of finding a way to achieve what she already “knows” is the right thing to do, despite the fact that this might involve her not fully complying with her professional duty to apply the strict legal version of the principle of self-determination. At the same time, she is asking for justification from the others (“Or is it just, like, sit and wait until something happens?”). The way in which the excerpt above ends, with utterances hinting at emotions, might be understood as part of this parallel framing of the case. It may also be interpreted as “ethical emotion work” (Banks, 2016: 8) and as an expression of “moral distress” (Banks and Von Köppen, 2021: 330), which relates to the care manager being in a situation in which she is unable to do what she feels is morally right due to (legal) constraints associated with her role as a professional in a particular setting.
Included in the care manager’s concluding request for input from the other participants at the meeting in Example 1 is also an embedded request for their input on whether (full) adherence to the principle of self-determination is the only legitimate option when proceeding with the case (“or is it just, like, sit and wait until something happens?”). Other case presentations end in similar ways, with the care manager responsible for assessing the case more or less explicitly asking the other participants at the case conference for their input on whether there might be alternative ways to proceed with the case, ways that prevent the individual from continuing to put herself or himself at risk. In this way, encouraging guidance from social work colleagues on how to determine the right course of action, or engaging in joint reasoning – or “reason work” (Banks, 2016: 4) – on strategies for (ethical) action, could tentatively be named (ethical) invitation work. This is a label that could also be applied to the illustrated types of case presentation as a whole by exposing the case as complex and the problem that the social worker is facing as lacking a given or easy solution.
Raised (by the immediate manager) as an issue of relevance
At the remaining (majority of) case discussions, the care manager responsible for assessing the case does not mention the individual’s wishes when presenting the case. Instead, this dimension of the case is raised by another participant at the case conference as an issue of relevance during the second phase of input and discussion among the participants. With just two exceptions, it is the immediate manager who raises this issue, indicating the existence of different roles and power relations within the group.
Below is an example of how this is done (Example 2). In presenting the case, the care manager responsible for assessing the case has described problems related to an application concerning a permanent place in special housing for a man, Richard, with “escalating frontal lobe dementia”, focusing on the difficult situation of Richard’s wife (e.g. “/…/ when I talked to the wife she was at the point of collapse, completely distraught and exhausted /…/”). She (CMR) has not mentioned Richard’s standpoint on the matter during her case presentation, but this issue is raised by the immediate manager (IM) during the subsequent phase of the case discussion:
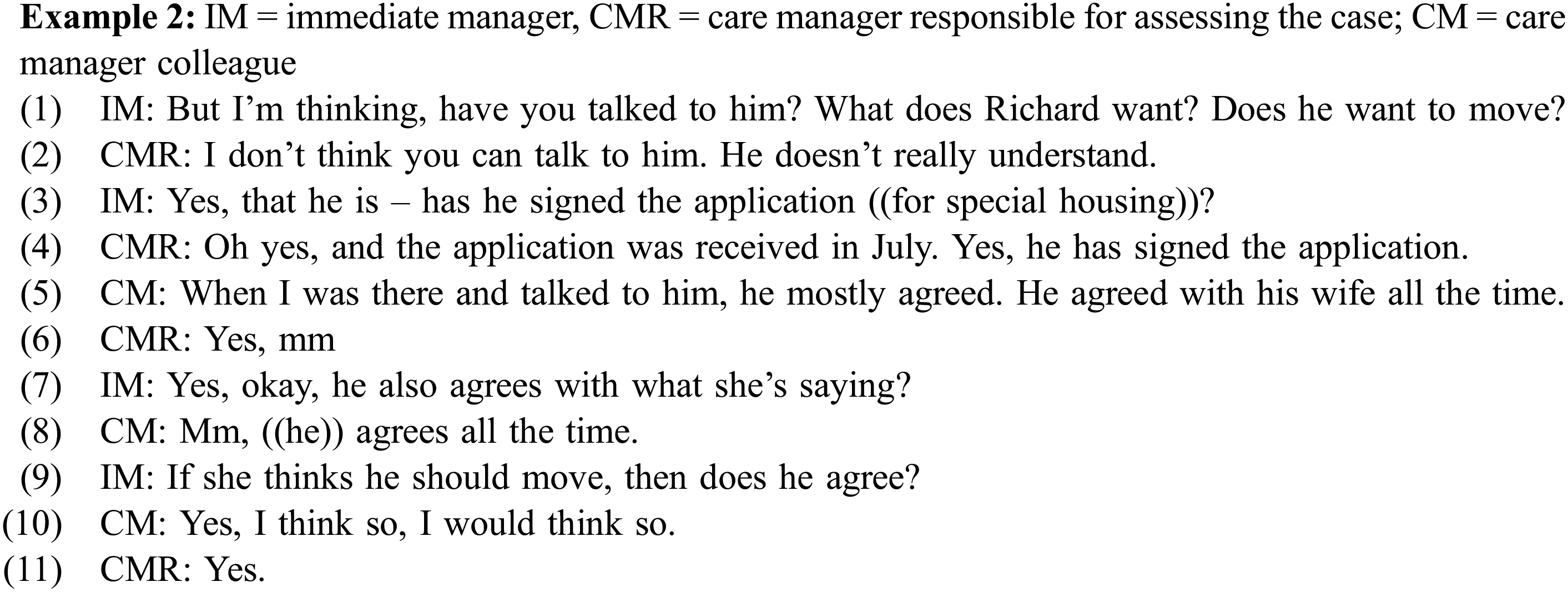
As in other case discussions where the wishes of the individual are not raised as part of the case presentation, the immediate manager raises this issue as a salient feature of the case, by explicitly asking for it (line 1). She then continues posing questions on the matter until seemingly content with the answers provided by the care manager responsible for assessing the case and, sometimes, as in this case, from other participants at the meeting, who engage in the discussion (lines 3, 7 and 9). By their questions, the immediate managers – implicitly –ignore any motives raised by the presenting care managers for not considering the wishes of the individual. In this case, this means ignoring Richard’s reduced decision-making capacity as a motive for not considering his standpoint (line 2).
In terms of ethics work, the immediate manager’s input is identifiable as both (ethical) “role work” and “performance – and accountability – work”. That is, as a social worker in a managerial position, she is responding to, and performing in relation to, role expectations that she will take responsibility for the work accomplished by the social services unit. This is accomplished by raising the individual’s wishes – and thus also the care manager’s legal duty to adhere to the principle of self-determination – as a salient feature of a case when this has not been done by the care manager responsible for assessing the case. However, in none of these case discussions do the immediate managers explicitly question the relevance of also incorporating other aspects and interests into the decision. In the example above, the immediate manager does not explicitly question the care manager’s (CMR) framing of the situation of Richard’s wife as an (additional) important dimension of the case.
As briefly exemplified above, the responsible care manager’s (CMR) way of framing the case, and the difficult situation of the wife as a salient feature of the problem for which she is requesting input in her case presentation, does not include ethics work on the principle of self-determination/the wish of the potential receiver for a place in special housing. However, her way of approaching the case may be understood as a form of (ethical) “role work” that encompasses acting as an advocate for Richard’s wife and as framing listening to – and caring for – the wife as the right course of action – and as more relevant than applying the principle of self-determination in this particular case. It could also be described as an example of a situated approach to ethics, “in which what is right is decided in relation to the particularities of each situation” (Banks and Von Köppen, 2021: 331).
In suggesting and discussing strategies
After the wishes of the (potential) service user have been raised at a case discussion, those present at the meeting discuss strategies on how to proceed with the cases, after and beyond the case conference.
The following excerpt (Example 3) illustrates how one of the strategies that figure in the (16) case discussions is raised and discussed as part of an overarching strategy to work step by step towards consent to take up a permanent place in special housing. The case concerns a man who was presented by the care manager responsible for assessing the case as a person whose wishes are difficult to determine. The strategy itself can be summarised as encompassing: to supply, accept and process an application form for special housing signed by the (potential) service user, while not being sure about the individual’s standpoint on the matter – or whether family members will in fact be the actors behind a received signed application.
The excerpt provides a starting point for a subsequent discussion of the ethics work identified in the care managers’ discussions of strategies:
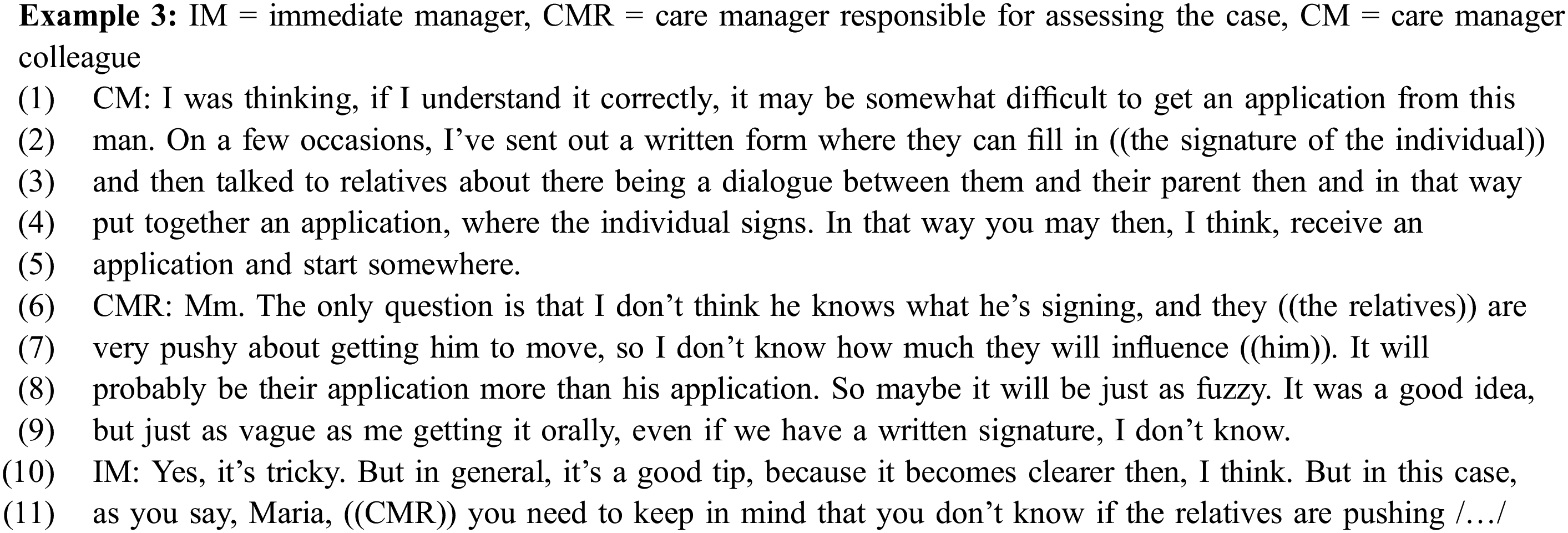
In this example, the strategy in question is suggested to the care manager responsible for assessing the case (CMR) by a colleague (CM) in the first section of the excerpt (line 2-5). The CMR in turn acknowledges inherent problems related to the individual’s (legal) right to self-determination. That is, problems related to whether the man will understand the implications of signing an application form or whether the signing will be done under the influence of family members (“it will probably be their application more than his application”). The immediate manager confirms her doubts about applying the suggested strategy in this particular case, while also acknowledging that the strategy may prove useful in other cases, because of the relative clarity that a written application implies.
Common to all the strategies raised is the fact that they may be considered ways of receiving some sort of consent to (some sort of) service by blurring the boundaries “between the measures actually accepted by an individual and those imposed in one way or another by the case manager” (Corvol et al., 2012: 88). They may also be considered ways of balancing adherence to the principle of self-determination with values such as attentiveness (noticing the need for care) and responsibility (taking care of others) Tronto, 1993; Banks, 2016). Thus, from a Swedish legal perspective, applying these strategies could be considered a case of bending the law, with its stipulation of a strict application of the principle of self-determination and the related rule of informed consent (Giertz et al., 2021). However, suggesting and discussing these strategies could also be seen as (ethical) “reason work”. As Banks writes, the “deliberation with others on ethical evaluations and tactics; working out strategies for ethical action” (Banks 2016: 4) that reason work encompasses is “less about abstract rational processes following principles of logic, and more about practical reasoning based on particular situations and cases and dialogue with others – what Toulmin calls ‘reasonableness’ as opposed to rationality” (Banks, 2016: 10). According to Banks and Von Köppen (2021), making ethical evaluations by acknowledging the particularities of a situation is much more demanding than adhering rigorously to rules that (like the strict, legal version of the principle of self-determination in Sweden) are designed to maximise public good. Confirming the efforts that the care managers put into finding the right course of action in each individual case, several strategies were raised and discussed in one case discussion. The maximum number (five different strategies) was raised in the case discussion quoted above (Example 3). As in this excerpt, a strategy suggested by one of the care managers was sometimes rejected by one or more colleagues as not being relevant to use or try in a particular case. Conversely, a strategy that was rejected in one case discussion (including the strategy presented in the extract) was accepted as relevant to use or try in practice by all the participants at the end of another discussion, further illustrating that these judgements are made on the basis of shared reasoning about the applicability of a strategy in a particular case. In several cases, strategies were suggested and discussed as part of an overarching strategy to work towards consent step by step.
Overall, it is not made explicit during the (16) case discussions that the participants in these discussions are not perfectly adhering to their professional duty to apply the law, but balancing self-determination in relation to other values in suggesting strategies. Rather, it seems to be accepted as part of a tacit agreement between colleagues, including the immediate managers. However, in one of the case discussions, the immediate manager explicitly justifies a strategy as being based on a moral judgement – that is, on what is considered to be in the best interests of the individual. This occurs after she has responded positively to a suggestion from another participant to try to receive consent for short-term care for a woman with dementia by talking about the service in positive terms, but without using the word “special housing”, to make it easier to achieve the next step, which is to get the woman’s consent to remain permanently in the special housing:

In describing the strategy as “tiptoeing around in a grey area”, the immediate manager is performing her awareness that it means bending the law. Simultaneously, she is doing (ethical) “reason work” in a way that justifies exactly that. In her role as an immediate manager, she is thus also justifying the fact that the care managers at the office incorporate other values and interests than the wishes of the adult individual in question when talking about and dealing with a case, even though this might result in a situation in which they do not perfectly adhere to their legal duty to apply the principle of self-determination in cases concerning adults assessed as being in need of social services. Another way of understanding this statement, which is unique in the empirical material, is that the immediate manager is suddenly reminded that the meeting is being recorded and will be listened to by “outsiders” whose approach to the matter is unknown. She therefore feels the need to explain – and defend – the discussion that took place during the meeting (to us as researchers).
The (16) case discussions are rounded off in a variety of ways. A notable dimension of how several of the discussions end is that spoken agreements on how to proceed imply trying one – or more – of the suggested strategies. That is, whether a certain strategy will work in a particular case is discussed as something that has to be tested, by applying the strategy in practice, in a direct meeting with the individual.
Tentatively, we suggest that this shows that ethics work on the principle of self-determination and the (ethical) reasoning work concerning possible strategies when handling cases where the (potential) service user is reluctant to receive support, or whose preferences in the matter are difficult to determine, may be considered as being followed by yet another dimension of (ethics) work. In contrast to the care managers’ discursive doing of ethics in the case conferences, this other form of ethics work – this (ethical) “trying work” – encompasses trying out which strategy, or way of meeting needs, provides the right course of action by testing them, in practice, in each individual case.
Discussion
As our analysis illustrates, the law regulating Swedish care managers’ work and their application of the principle of self-determination does not have a consistent impact on how, in practice, care managers approach a situation in which the (potential) service user is reluctant to accept support, or where the individual’s wishes in the matter are difficult to determine. While some may acknowledge their legal duty to adhere to the legal principle when dealing with cases like these, others may prioritise other values or be more preoccupied with other aspects of the cases that they are handling, and with the other parties involved.
The analysis also suggests that, for some care managers in Sweden, the obligation to comply with the legal principle may pose particular challenges. Despite the fact that, clearly, adhering to the law and leaving the individual without support would be a less time-consuming – and more rule-following – way to deal with “reluctant clients” in practice in the Swedish context, a social worker may approach this type of case as a moral challenge. She (or he) may choose to ask her (or his) colleagues for advice on how to handle the case during the regular case conference in the office. In front of colleagues and manager, she may engage in a complex balancing act, involving various forms of “ethics work”, to present the case in a way that allows for relevant guidance on how to deal with the perceived challenge in a manner that corresponds to, and justifies, what she feels and “knows” is “the right course of action”, while simultaneously presenting herself as fully aware that, according to the law, there is already a given solution for how to handle the case as a professional social worker in Sweden, which constrains her from following her moral compass. The fact that the ethics work carried out by these Swedish social workers may also be seen as “law work” explains the complexity of these case presentations. So does the embedded uncertainty about what one’s colleagues – and one’s immediate manager – consider legitimate when dealing with reluctant clients. At the same time, whether it is legitimate to bend the law may be too sensitive a matter to be openly addressed. Consequently, the findings also suggest that asking for advice from colleagues regarding how to meet the perceived needs of reluctant clients may require courage on the part of the social worker. This, in turn, suggests that the wider societal context in which case discussions take place – and the formal rules and regulations associated with it – may contribute to less (or more) open and frequent collegial discussion about particular challenges (Österholm et al., 2024). Consequently, it may also contribute to more (or less) well-considered decisions about how to deal with the individuals in question, and also to more (or less) internal stress for practitioners (cf. Banks and Von Köppen, 2021; Odo et al., 2023).
While the welfare context of this research is specific, the dilemma/s confronting the Swedish care managers in question concern challenges that are experienced and handled by social workers internationally. They are related to the individual’s right to make their own choices and decisions concerning welfare services, and social workers’ responsibility to promote the welfare of (potential) service users (Banks, 2012), to social workers’ duty to obey professional boundaries and regulations while meeting the specific needs of the (potential) service user (Odo et al., 2023), and the balancing act between professional accountability and personal engagement in the case (Banks, 2013). The importance of social workers managing, and balancing, these perspectives, expectations and dilemmas, in practice, has been raised by several scholars and is stressed as part of the ethical standards of the International Federation of Social Work (IFSW) (Van der Tier et al., 2021).
In summary, our analysis supports the findings of a recent qualitative survey study (Banks et al., 2020), by suggesting that factors related to the wider context in which social work is carried out help to shape the context in which ethical challenges arise and the options available to social workers to address them, but that the ethical concerns perceived by social workers are similar across different countries and welfare systems (cf. Skotte, 2023).
Examining – and developing – the features of ethics work in practice
To our knowledge, the present study is rather unusual in using Banks’ (2016) conceptualisations of various dimensions of “the doing of ethics” in social work for analysing social work practice in situ, in this case based on recorded, internal case conferences and discussions – and considerations – among colleagues about how to deal with cases. We found this to be a useful approach, which made otherwise hidden (moral) aspects of the social work practice in question visible and understandable. As in our data, social workers do not necessarily explicitly mention ethics when discussing cases with colleagues (Juhila and Raitakari, 2010), or in “doing ethics” in practice. Thus, while in a sense “ethics is everywhere” in discussions like these, in another sense “ethics is nowhere in particular” (Banks, 2016: 13). While this motivates research directed towards uncovering the ethical dimensions of actual social work practice, it also represents a challenge when conducting the analysis (Banks, 2018). The case conferences and case discussions chosen as data for the present study probably facilitated the identification of the ethics work accomplished by care managers in practice. By encompassing a context in which they put into words the challenges that they encounter as part of their daily work, the case conferences could be considered as contributing to a “dilemmatic space” (Banks, 2018: 7), where the challenges and contradictions that are always embedded in social work practice come to the surface as identifiable conflicts and ethical dilemmas.
The main challenge that we encountered in conducting the analysis was that the same account could be considered as simultaneously encompassing a number of the features identified and named by Banks. This was not wholly unexpected because, according to Banks (2016: 3), the elements of ethics work “are inter-connected in the complex world of practice”. Our solution was to choose and apply the feature – or features – that we considered to provide the most insights, in relation to the objective and purpose of the study.
Furthermore, based on the presented analysis, we propose the incorporation of two additional features into Banks’ (2016) conceptualisation. We refer to these as “invitation work” and “trying work”.
In professional life, ethical invitation work would imply talking about a challenge encountered as part of one’s daily work in a way that encourages input and guidance from others – such as colleagues or an immediate manager – about how to determine “the right course of action”, or that prompts the engagement of others in joint “reason work” on strategies for (ethical) action. That is, telling others and asking for input in a way that accommodates and exposes the case, and the problem that the social worker is facing, as complex, with no easy or obvious solution.
While we suggest “invitation work” as a separate dimension of ethics work, alongside reason work, framing work etc., invitation work can include these other forms. For example, as our analysis has shown, a social worker may engage in “performance work” (“accountability work”) as part of the narrative of the problem or dilemma for which colleagues are invited to provide their input, which in turn points to the challenges that invitation work may pose for the individual social worker. As she (or he) may be unsure about whether those invited consider it either legitimate or responsible to even consider the matter as a challenge or dilemma (but may see a request for guidance and support as a lack of important knowledge about existing rules on the part of the inviting social worker), “invitation work” can be a delicate matter. As suggested by previous research on collegial discussions in social work (e.g. Johnson-Lafleur et al., 2019), initiatives taken by individual social workers to raise and share some of the challenges that they encounter may be encouraged by stability and continuity in terms of meeting participants and a person in a supervisory position who is flexible and empathetic towards both clients and practitioners.
(Ethical) trying work provides an alternative way to conceptualise a phenomenon that has been described in previous research as a set of strategies that blur the boundaries “between the measures actually accepted by an individual and those imposed in one way or another by the case manager” (Corvol et al., 2012:88), and as “subtle persuasion” (Suoninen and Jokinen, 2005). Unsurprisingly, and unlike invitation work, (ethical) trying work as such is not visible in our data. This is because trying work does not take place during collegial discussions, but is undertaken in direct contact with (potential) service users in an embodied, performed practice, while balancing individuals’ right to make their own choices and decisions concerning welfare services against values such as attentiveness (noticing the need for care) and responsibility (care for others) (Tronto, 1993; Banks, 2016). Our basis for considering these strategies as part of ethics work is the insights that our data and analysis provide into the ethical reason work that may precede that they are employed in practice.
Like invitation work, trying work is suggested as a separate form of ethics work, but one that is difficult to imagine without the involvement of both emotion work (building trust; responding to others’ emotions) and relationship work (engaging in dialogue with others). It resembles Habermas’ “discourse ethics”, which implies that morally sound decisions are made during a discussion in which all the concerned parties participate (Sandman and Kjellström, 2018). However, while trying work encompasses a recognition of the actions or reactions of the individual concerned, it does not necessitate discursive input, but could mean that nonverbal expressions of consent to, or being content with (or the opposite), a suggested or materialised social service is acknowledged, or read off, by the social worker.
A potential strength of (re)conceptualising strategies that blur the boundaries “between the measures actually accepted by an individual and those imposed in one way or another” (Corvol et al., 2012: 88) as ethical trying work is that it acknowledges that these actions may encompass a moral dimension, and be preceded by thorough ethics work, which could make them more understandable as part of professional social work practice. However, we are open to the argument that whether the application of such strategies involves ethical dimensions or whether it is more relevant to understand them as expressions of pragmatism, i.e. trying “what works”, could be seen as an empirical question.
Conclusions
With the help of Banks’ (2016) analytical description of the ethical dimensions of some of the work that social workers do in practice, the analysis presented in this paper has provided insights into how the conflicting pressures and challenges that social workers have to handle across the world are dealt with, in practice, by care managers in collegial case-conference discussions located in a particular (Swedish) welfare context.
Based on the analysis presented in this paper, we argue that further research applying and developing Banks’ conceptualisation of ethics work in examining “actual” social work practice, while acknowledging characteristics of the social and societal context in which this work is conducted, could provide new knowledge and understandings about both particular and shared challenges that social workers have to deal with in different parts of the world. As the current dominant managerialist discourse risks rendering invisible the often rather hidden moral dimensions of what social workers (still) do, and say, as part of their daily work (Banks, 2018; Hill and Laredo, 2020; Van der Tier et al., 2021), it is important that this work is recognised and examined.
We also suggest that the team meeting among social workers provides a fertile context for further research into the ethical dimensions embedded in social work practice. We base this on the analysis presented in this paper, as well as on previous research showing that discussions with colleagues can help to stimulate social workers to reflect upon ethical dilemmas and to deliberate on the ways in which they legitimise their ways of dealing with cases – and individuals (van der Tier et al., 2021). Consultation with colleagues may even be the most common way for social workers to deal with ethical dilemmas (Linzer et al., 2003).
Additionally, while team meetings have a long history in social work practice, these collective aspects of social work have so far received very little scholarly attention (Olaison et al., 2023; Taghizadeh Larsson et al., 2023). Consequently, much of what is going on at meetings where social workers discuss cases behind the scenes – that is, without the presence of clients, next of kin or other professions – remains largely obscured. This includes what issues are considered meaningful to raise with other social workers in contemporary, diverse, social work contexts – and how colleagues find ways of dealing with these issues collectively.
Footnotes
Author notes
The manuscript has been proofread by CBG Konsult & Information AB (
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by FORTE Swedish Research Council for Health, Working Life and Welfare [Grant number 2019-00610]. Useful comments were provided by members of the Gerontological Social Work (GEROSOC) research group, Linkoping University, Sweden and by two anonymous reviewers of this journal.