
Abstract
Approved Mental Health Professionals (AMHPs) undertake Mental Health Act (MHA) interviews and they make the ultimate decision, based on doctors’ medical recommendations, to detain an individual in hospital without their consent. AMHPs are required to embed the statutory guiding principle of Empowerment and Involvement as well as to maximise service users’ self-determination and this is part of a broader policy orientation toward principles of participation, involvement, shared decision-making and supported decision-making. Yet there is very little research in this area and AMHP practice takes place in the absence of guidelines or clear evidence base. Consequently, more needs to be understood about effective techniques for communication and involvement. This study was conducted with AMHPs from an AMHP service in England. A qualitative methodology was employed to gather indepth information about AMHPs’ communicative practices. MHA assessments were observed and audio-recorded to enable Conversation Analysis to be used to analyse the content and style of communication within interactions. Findings suggest that at a micro, conversational level, AMHPs worked to address obstacles to communication as well as to maintain, or restore, affiliation and alignment in their relationships with service users. Evidence suggests that communicative techniques form part of AMHPs’ broader coordinating and empowering role. The study concludes that there is a need for a more deliberate and deliberative approach to re-engineer how AMHPs and service users work together, providing original evidence for AMHP practice and supporting future training.
Background
At an international level, mental health legislation sanctions the compulsory detention of individuals identified as having a mental disorder (Fistein et al., 2009) and the legal frameworks enabling this detention involve key statutory professional roles. One of these roles is the Approved Mental Health Professional (AMHP), a role specific to England and Wales in the United Kingdom. This role can now be undertaken by social workers, mental health nurses, occupational therapists and psychologists, having been changed from that of the Approved Social Worker (ASW) via the 2007 amendments to the Mental Health Act 1983 (MHA). The professional perspectives, value-base and requirement to apply a social perspective (DoH, 2015 p.122) to decision-making remain largely unchanged and in England, the vast majority (95%) of AMHPs are social workers (Skills for Care, 2024).
Statutory contexts
The AMHP role rests on several clear professional imperatives. The Code of Practice to the Mental Health Act 1983 (DoH, 2015), to which AMHPs must ‘have regard’ (p.12) in order to avoid legal challenge, clearly states that the AMHP is independent and autonomous, having the ultimate responsibility, based on doctors’ medical recommendations, for making the decision to detain (DoH, 2015 para.14.52; s.13 (5) MHA 1983). It is the AMHP who has overall responsibility for coordinating the process of assessment (DoH, 2015 para. 14.40) and this is usually understood in practical terms, for example ensuring the attendance of doctors to examine the person as well as other colleagues, including police or ambulance personnel.
AMHPs also have a duty to interview a person in a ‘suitable manner’ (s.13 1C (2) MHA; DoH, 2015 para. 14.49). This phrase originally related to the need for Deaf service users to have access to an interpreter with fluency in British Sign Language, as well as conveying a need for sensitivity to the difficulties faced by those who might not speak or understand English (Young et al., 2024). It also considered the needs of children who might have difficulties in communicating effectively (Jones, 2023 p.120). In practice, the phrase has been extended to address other barriers to understanding, for example not interviewing when the person appears to be ‘subject to the short-term effects of alcohol or drugs … which makes interviewing them more difficult’ (DoH, 2015 para.14.56) or attempting an interview through physical barriers such as a closed door or window (DoH, 2015 para. 14.55). Arguably, however, there has, to date, been little focus on communicative barriers.
Statutory guiding principles should always be considered when making decisions in relation to legal interventions and all UK jurisdictions have principles relating to service users’
1
involvement in decision-making. In England, AMHPs are required to embed the Empowerment and Involvement principle, whereby ‘patients should be fully involved in decisions about care, support and treatment’ and further: [they] should be enabled to participate in decision-making as far as they are capable of doing so [and] support should be provided to ensure maximum involvement (DoH, 2015 para.1.10).
The guidance does not explain in detail what this ‘assistance or support’ might entail, but it does say that people should be given sufficient information about their care and treatment in a format that is easily understandable to them (DoH, 2015 para.1.10).
The requirement to involve service users in decision-making is consistent with AMHPs’ professional qualifying criteria and practice imperatives. Qualifying and then ongoing re-approval to practice requires the satisfactory completion of the competencies set out in the Mental Health (Approved Mental Health Professionals) (Approval) (England) Regulations 2008 (HMSO, 2008) whereby AMHPs are required to: promote the rights, dignity and self-determination of persons consistent with their own needs and wishes, to enable them to contribute to the decisions made affecting their quality of life and liberty (1c)
as well as to: communicate appropriately with and establish effective relationships with patients … in undertaking the AMHP role (4a)
and to: discharge the AMHP role in such a way as to empower the patient as much as practicable (4h).
Empowering and involving service users in decision-making are vital components of practice and the professional value-base. Yet there is no clear written representation or evidence-based understanding as to what good practice in this communicative sphere looks like. Certainly, however, the AMHP role goes further than a processual or legalistic one: it is relational, interpersonal, and its professional and policy imperatives require sound communication skills (Hemmington and Vicary, 2023).
The Independent Review of the MHA in England (DHSC, 2018) addressed aspects of involvement and the sharing of information with service users, referring to this in general terms as ‘shared decision-making’ (SDM). It pointed to evidence that SDM is not practiced routinely for those subject to the Act (DHSC, 2018 p.71) and it acknowledged that culture change is required to ensure that practice which enables empowerment and involvement becomes routine. Significantly, it recommended the mandatory recording of evidence of SDM (DHSC, 2021a) which implies that professionals need to understand how they are applying principles of ‘sharing’ in a MHA assessment encounter.
A further limb to this developing agenda is found within the Convention on the Rights of Persons with Disabilities (hereafter CRPD) which came into force in 2008 (United Nations General Assembly, 2006). In general, this seeks to protect the rights of persons with disabilities (which includes those with mental health problems) that exist in other international treaties (Newton-Howes et al., 2021; McCusker et al., 2023). These include dignity, equality, non-discrimination, individual autonomy, fair access to resources and support, and full social participation and inclusion (Dawson, 2015). Significantly, it recognises that disability exists at the point at which ‘various barriers may hinder the full and effective participation of persons with impairments in society’ (Szmukler, 2019). Identifying potential communication barriers is therefore key.
The premise of Article 12 of the CRPD (UN Committee on the Rights of Persons with Disabilities, 2014), equal recognition before the law, is that despite a perceived or actual impairment in decision-making ability (‘mental capacity’), people with mental health problems maintain the right to legal capacity (Duffy and Kelly, 2017; Richardson, 2012) and this means taking ‘appropriate measures to provide access by persons with disabilities to the support they may require in exercising their legal capacity (Article 12 (3)). The Committee on the Rights of Persons with Disabilities General (the body that monitors the implementation of the CRPD by the State Parties) made clear that this right to legal capacity should be interpreted as a ban on substituted decision-making (where people make a decision on behalf of another person); coercion within commonly held ‘best interests’ frameworks would be an example of this (UN Committee on the Rights of Persons with Disabilities, 2014). It spoke of the need for a shift towards supported decision-making that involves the determination and delivery of support in accordance with the will and preferences of individuals. This would seem to be consistent with AMHPs’ statutory and professional imperatives, outlined above, yet whilst the CRPD has been found to influence some research activities, there are significant gaps around supported decision-making specifically and implementation strategies more broadly (McCusker et al., 2023).
Policy contexts
The idea that people should be offered more choice within healthcare settings has been increasingly developed such that the ‘choice agenda’ has been seen as a dominant reform within European healthcare systems (Costa-Font and Zigante, 2016). SDM is enshrined as a principle in England’s National Health Service Constitution (DHSC, 2021b) and the General Medical Council’s guidance on decision-making and consent says that SDM is ‘fundamental to good medical practice’ (GMC, 2020 p.4) although, again, these read as general principles around involvement and choice and not specific methods.
The benefits of these ‘sharing’ approaches and the rhetoric of choice have been argued from different perspectives. Ethicists argue that it is a self-evident right that people should determine what happens to their bodies (Nelson and AAPA, 2001). Clinicians believe that including people in decision-making leads to an enhanced therapeutic relationship and improved health outcomes, including with treatment ‘adherence’ and treatment satisfaction (Drake et al., 2010; Morant et al., 2016). Economic perspectives see increased consumer control as a means of embedding the healthcare industry further within forms of market discipline (Polsky et al., 2003). Politically, there has been a growth in agendas such as personalisation, choice and competition in service delivery and, as such, there is a broader policy orientation towards the neo-liberalisation of health and social care (Glasby, 2012). Further, Kourova and Webb (2022) draw attention to a ‘paradox of empowerment’ where policies of empowerment have been co-opted by neoliberalism and ostensibly emancipatory discourses of empowerment have, in fact, had the potential to effect the opposite by legitimating the offloading of responsibilities to vulnerable and dependent people.
In mental health settings, policy trends and organisational rhetoric have a broad approach mirroring aspirations towards SDM, supported decision-making, self-determination and so on in the ways in which they speak of the need for collaboration, coproduction and partnership with people who use (or are subject to) mental health services (DHSC, 2019; NICE, 2021). The first National Workforce Plan for AMHPs (DHSC, 2019) began to consolidate the different aspects of AMHP work and their relative challenges. It recognised that AMHP work is values-based and oriented to a human rights approach, and it acknowledged the affective and relational issues attached to the work. It spoke of the need to promote service users’ dignity, human and civil rights (p.34). More broadly, AMHP services should seek to embed the principles of coproduction, to ‘ensure the patient experience and perspective is captured and harnessed’ and to identify ways in which service users are ‘able to engage and influence the development of … AMHP practice’ (p.34). Finally, AMHP reporting should make clear reference to the principles of the MHA and how AMHPs have considered these throughout their work with individuals and those connected to them (p.34). Again, however, there is very little evidence in terms of specific communicative techniques underpinning empowerment and involvement.
People with lived experience of MHA assessments and detention
The voice of people with lived experience of MHA assessments, and thereby AMHP interventions, has been limited if not ‘almost completely lacking’ (Akther et al., 2019 p.8) and there is only a very small body of research exploring service users’ experiences of these (Barnes et al., 2000; Hemmington et al., 2021; Blakley et al., 2022). More needs to be understood about the process of the MHA assessment (McGuinness et al., 2018; Wyder et al., 2015) as, generally, the literature conflates hospital detention and the assessment itself. This lack of research could be said to be indicative of the comparative value assigned to different types of evidence and research priorities (Barnes et al., 2000).
There are suggestions that some service users have expressed a fatalistic view that coercive treatment is inevitable, compounding feelings of failure and powerlessness (Hemmington et al., 2021; Olofsson and Norberg, 2001). Decisions take place in the communicative space between mental health professionals and service users and, yet, people with lived experience of assessment report being ‘seen but not heard’ (Johansson and Lundman, 2002). Further, service users themselves have described their being unaware of the nature of the assessment, describing the experience as ‘deliberately secretive … and Kafkaesque’ (Blakley et al., 2022). These all speak of a lack of involvement.
Ultimately, MHA assessments have been seen to have an essentially private nature and are undertaken by professionals away from public gaze and without public scrutiny, despite the serious implications for people’s liberty (Bean, 1980; Sheppard, 1993). Little is known about how AMHPs communicate with and relate (or indeed fail to relate) to service users. Research in this area has relied on retrospective interview and self-report data, rendering the data merely summaries or even idealisations of what occurred and, as such, the complex details of talk-in-interaction are lost (Schegloff, 1998; Toerien and Kitzinger, 2007). The focus has been on the overt, structural or ‘macro’ methods of power, control and coercion rather than the more subtle forms of manipulation at the individual level of negotiated decisions (Quirk et al., 2012). A qualitative study, outlined below, introduced a focus on the micro, conversational level, exploring AMHPs’ conversational manoeuvres behind their empowerment strategies.
Materials and methods
To explore communication in MHA assessments in detail, a qualitative study was undertaken in an AMHP service in England. The research was granted ethical approval via the National Health Service Health Research Authority in England (REC reference 15/IEC08/0019), via a Research Ethics Committee flagged to consider research which has the potential to fall under the remit of the Mental Capacity Act (2005). Informed, signed consent was obtained from all participants involved in the study, and this was revisited as part of a full debrief following the assessment scenario. With all participants’ consent, four MHA assessments were observed and audio-recorded to enable Conversation Analysis to be used as a method of data analysis aimed at exploring aspects of the content and style of communication within interactions.
Conversation Analysis
Conversation Analysis (CA) is a fine-grained analysis of conversational patterns and manoeuvres, and it can illustrate the ways in which involvement, affiliation and (dis)empowerment can be enacted. Conversations are considered to be based on precise and predictable rules, structures and relational alignments between participants (Heritage and Sefi, 1992) and patterns and sequences of speech are analysed with reference to, for example, turn-taking, length of pauses, points of overlap and interruptions. Crucially, practitioners can ‘see’ their own practices, what happens, what works, and what constitutes effective communication by ‘freezing the analytic frame’ on practice (Stivers, 2002). Epistemic injustice increasingly features in discussions about mental health settings (see Fricker, 2007) and in this study, CA was used to look at the way that this is enacted through the ways in which participants in MHA assessments assert, contest and defend their claims to knowledge (and arguably power) within their interactions.
Epistemics in language
Conversation Analysis attends to social epistemics in terms of the ways that participants handle knowledge distributions amongst themselves (Heritage, 2012; Kasper and Wagner, 2014). They manage their epistemic status, knowledge access, rights and obligations in their conversations and, within this, they then shape their identities and establish their social relations (Heritage and Raymond, 2005). Participants in conversations naturally adjust their actions and understandings in keeping with what they know about the world and, usually, they will treat one another as having privileged access to their own experiences and as having specific rights to narrate them (Sacks, 1984). However, in mental health settings, this is different. Service users and professionals have different (and unequal) epistemic communities and as such they own their associated identities, beliefs, knowledge, experience and, sometimes, idiosyncratic language including jargon (Heritage, 2008).
Epistemic status and deontic status
Conversation Analysis also addresses aspects of epistemic status. This concerns the possession of information as well as the distribution of rights and responsibilities - what participants can accountably know, how they know it and, crucially, whether they have the right to possess and articulate it (Heritage, 2008). In general, people’s thoughts, feelings, experiences, hopes and expectations are usually treated as theirs to know and describe (Labov and Fanshel, 1977; Sacks, 1984) but mental health professionals hold authority contained within their professional perspective, or ‘epistemics of expertise’, and as such they lack access to knowledge about a service user’s life, situation, ‘epistemics of experience’ (Heritage, 2008) or lived experience. The epistemic status differential between professionals and service users is reflected in asymmetric access to institutional speak (Kasper and Wagner, 2014) including jargon or ‘coding’ through knowledge of medicine, the law or resources. Embedded within this is deontic status, relating to participants’ rights to determine their own future courses of action (self-determination) or ‘how the world ought to be’ (Stevanovic and Peräkylä, 2012).
Findings
As outlined above, Mental Health Act assessments were audio recorded and transcribed verbatim to enable data analysis using Conversation Analysis. All encounters involved one service user (depicted here as ‘SU’), one examining doctor (‘Dr’) and the interviewing AMHP (‘AMHP’). The extracts of conversations presented below are taken from the transcripts from three different recordings. For reasons of space and fine focus, fragments of conversation have been selected from complete transcripts to evidence the particular themes, including AMHPs’ vigilance to epistemic asymmetries. In keeping with CA conventions, the Jeffersonian (2004) transcription system was used for analysis to enable the inspection of, for example, hesitations, hitches, silences, overlaps, breaths, laughter, prosodic cues, and other accompaniments to speech production. Throughout, there was evidence of AMHPs being alert to signs of conversation troubles and departures from congruent conversation. The first of these was where AMHPs worked to address an apparent block or diversion in the flow of conversation, using a technique known in CA as ‘repair’.
Repair
When conversational ‘troubles’ occur, there is recourse to a ‘repair mechanism’, explained in CA terms as an organised set of practices through which participants edit, rework, address and potentially resolve problems by seeking clarity (Sidnell, 2010). Speakers actively monitor their recipients for signals of understanding and will change course mid-turn if, for example, patterns of eye contact, facial expressions or nods suggest something is amiss (Bavelas et al., 2000). Repairs reflect attempts to achieve shared understanding as they are evidence of the effort a speaker is investing to take the listener’s needs into account by preventing misunderstanding and displaying sensitivity (McCabe et al., 2002). Extract 1 begins shortly after the doctor had shared their belief that the service user was a ‘problem drinker’ and the AMHP took up the conversational reins.
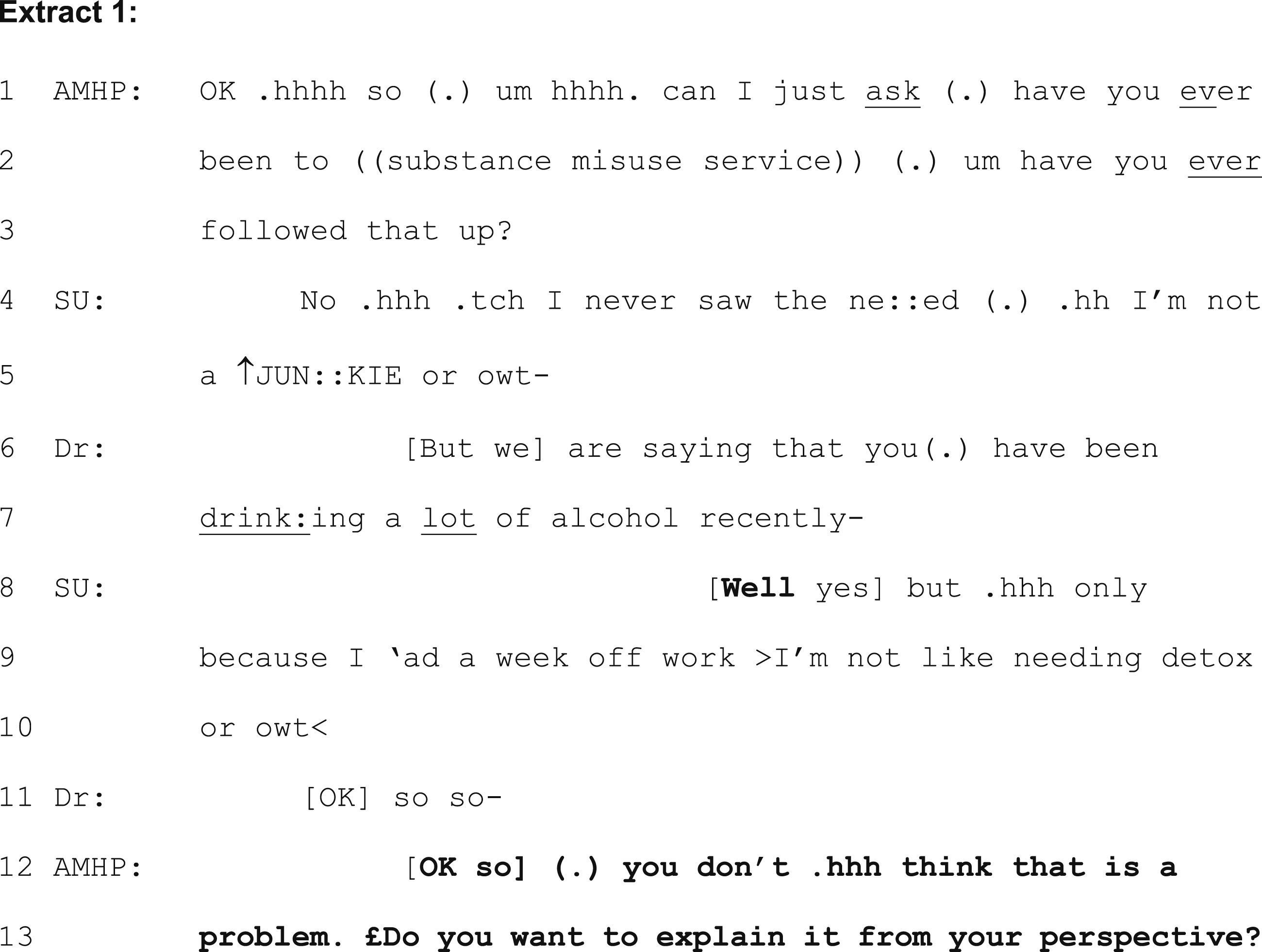
The AMHP asks about the substance misuse service (line (2) but receives a rejection and picks up on disengagement and an objection to the doctor’s belief about the ‘problem’. In line 5, the capital letters indicate ‘amplitude’ (or an increase in volume) and the upward arrow (↑) denotes a marked change in pitch. This dissatisfaction and, potentially, disengagement, is also flagged by the word ‘well’ at line 8 which, in CA, is understood to be indicative of a forthcoming complex response or indication of opposition or disagreement (Ruusuvuori, 2005). The AMHP picks up on these cues and no longer pursues the alcohol-as-problematic agenda, prioritising affiliation and re-engagement instead (and a ‘smile voice’, denoted in CA by pound sign (£), is observed at line 13). The AMHP observes the service user’s disagreement at lines 4-5, reinforced at lines 8-10, and works to repair the conversation, choosing affiliation and alignment over the apparent escalating conflict.
Affiliation, non-affiliation and alignment
Evidence has routinely suggested that what is important to service users is being listened to and heard (Akther et al., 2019). Research using CA in healthcare settings suggests that what matters to a person is the opportunity to tell their story, including its emotional aspects, but that professionals have a need to extract the significant facts from the story and work out the next step whilst still being sensitive to the emotional content and demonstrating that it has been properly heard (Benwell et al., 2024). If not done effectively, this can lead to conflict between institutional goals and the heightened emotional valence of a person (Weiste, 2016) particularly in situations where they may reasonably be classed as a ‘service refuser’. To avoid this, professionals can listen for cues that people are seeking legitimisation for their concerns and then seek to provide affiliative responses. Affiliation or ‘taking a stance that matches the teller’s stance toward the event(s) being described’ (Stivers, 2008 p.35) must be evidenced to avoid escalation rather than problem-solving or including or empowering a person in their decision-making.
In CA, the terms affiliation, non-affiliation and alignment have been used interchangeably as ways of demonstrating partnership-building (Steensig and Drew, 2008). As above, evidence suggests that professionals often prioritise the collection of facts over affiliating and addressing joint or shared problem-solving approaches (Ruusuvuori, 2005, 2007). The service user in Extract 2, below, had concerns and extensive beliefs that their neighbours were watching them and interfering with their lives to the extent that they had recently confronted them. Extract 2 illustrates the ways in which language and beliefs are ‘psychiatrised’ but, in the end, the AMHP reinstates the service user’s perspective and position to address the lack of affiliation and alignment.
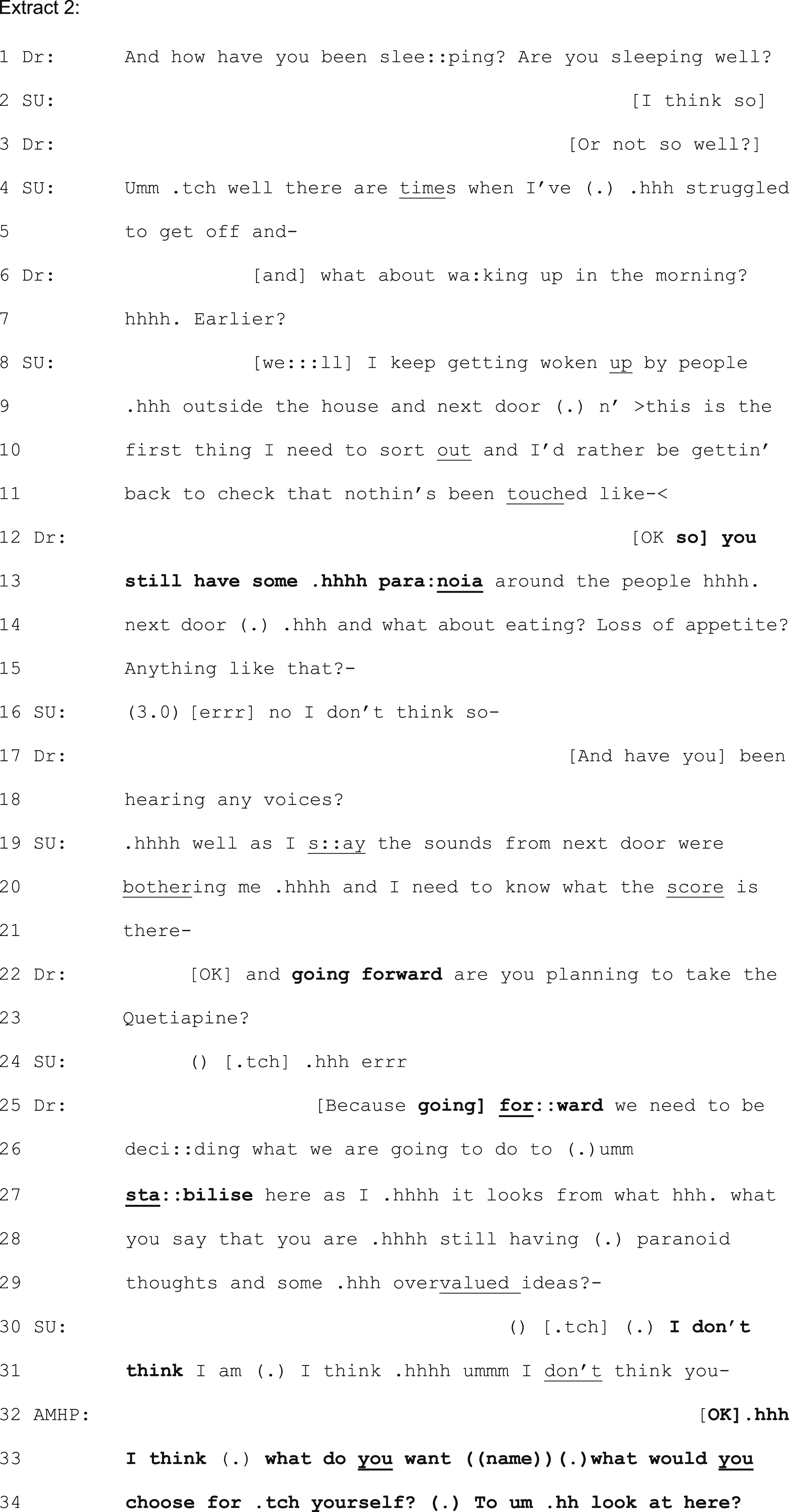
At lines 22 and 25, the doctor’s use of ‘going forward’ is, in CA terms, a ‘pre-closing’ device (Beach, 1995) – it is actively closing down conversation and is used to end or avoid the service user’s elaboration. It deletes the service user’s previous content and their own primary concerns about their neighbours. At lines 12-14 the doctor picked up on these concerns but edited and replaced them with their interpretation and psychiatric frame of relevance (Beach and Dixson, 2001; Deppermann and Spranz-Fogasy, 2011).
The doctor’s drawing on jargon through medical terminology and authority (using words such as ‘paranoia’ at line 13 and ‘stabilise’ at line 27) are examples of the ways in which communication and its frame of relevance are shaped by professional identities and settings (Drew et al., 2001). The doctor responds to the service user with ‘so you still have some paranoia’ (lines 12-13) distilling, and thereby deleting, the concerns provided by the service user (Heritage and Watson, 1979). The doctor is summarising the service user’s description in terms of a diagnostic framework and labelling (Johnson and Cotterill, 2002). In so doing, the significance of the service user’s narrative and epistemic status is diminished and affiliation is at risk of being lost.
At lines 30-31, the service user expresses disagreement (‘I don’t think …’) and, at line 32, the AMHP is alert to this disagreement and they attempt to repair this in order to realign and reinstate affiliation. ‘OK’, at the start of their talk, acts as a receipt token which can also be used as an upcoming change of activity (Gardner, 2001). At this point, the AMHP was also observed to hold up a hand, palm facing outwards, as a ‘stop’ gesture towards the doctor 2 . Here, the AMHP is attempting to topicalise and prioritise the service user’s concerns and again attempts alignment by asking ‘what would you choose for yourself … to look at here?’ (lines 33-34). Here, the AMHP attempts to shift the conversation back to the service user’s domain, thereby involving them in the conversation. Further, there is a heavy emphasis on the ‘you’ (denoted by the underlining in the text). This keeps the service user involved by attempting to place them centre-stage and it invites them to make a proposal for a course of action that would address their difficulties. In addition to affiliation, using this information-soliciting question, the AMHP once again claims lesser epistemic and deontic rights than the service user and provides an opportunity for the service user to draw upon their own knowledge of the situation in order to generate an idea.
Professional and service user interactions are characterised by several asymmetries that are created through the differences in roles, knowledge bases and expectations. The doctor is the expert who possesses formal biomedical knowledge and authority, whilst the service user has a social and personal lay perspective (Lindström and Karlsson, 2016). These are not always in unity as participants orientate to their own respective epistemic domains. To make an objective conclusion and diagnosis, the doctor requires specific and often measurable information about symptoms. However, the person may have difficulty in providing (or be unwilling to provide) this type of information. When service users disagree, then, they marshal an epistemic resource that is theirs alone - their own experience - to express reservations and to seek reconsideration (Ong et al., 2021).
In medical interactions, epistemic asymmetries lead to conversational failure when doctors pose questions that conflict with service users’ primary knowledge, and service users assert their epistemic rights by taking an independent stand (Lindström and Karlsson, 2016). This is illustrated in Extract 3 below, where there is a challenge to an assumption within the doctor’s question. Here, the doctor requests information in line 1 by using a statement (‘You’ve got a lot of suspicion there’) suggesting that they are relatively certain of their proposition.
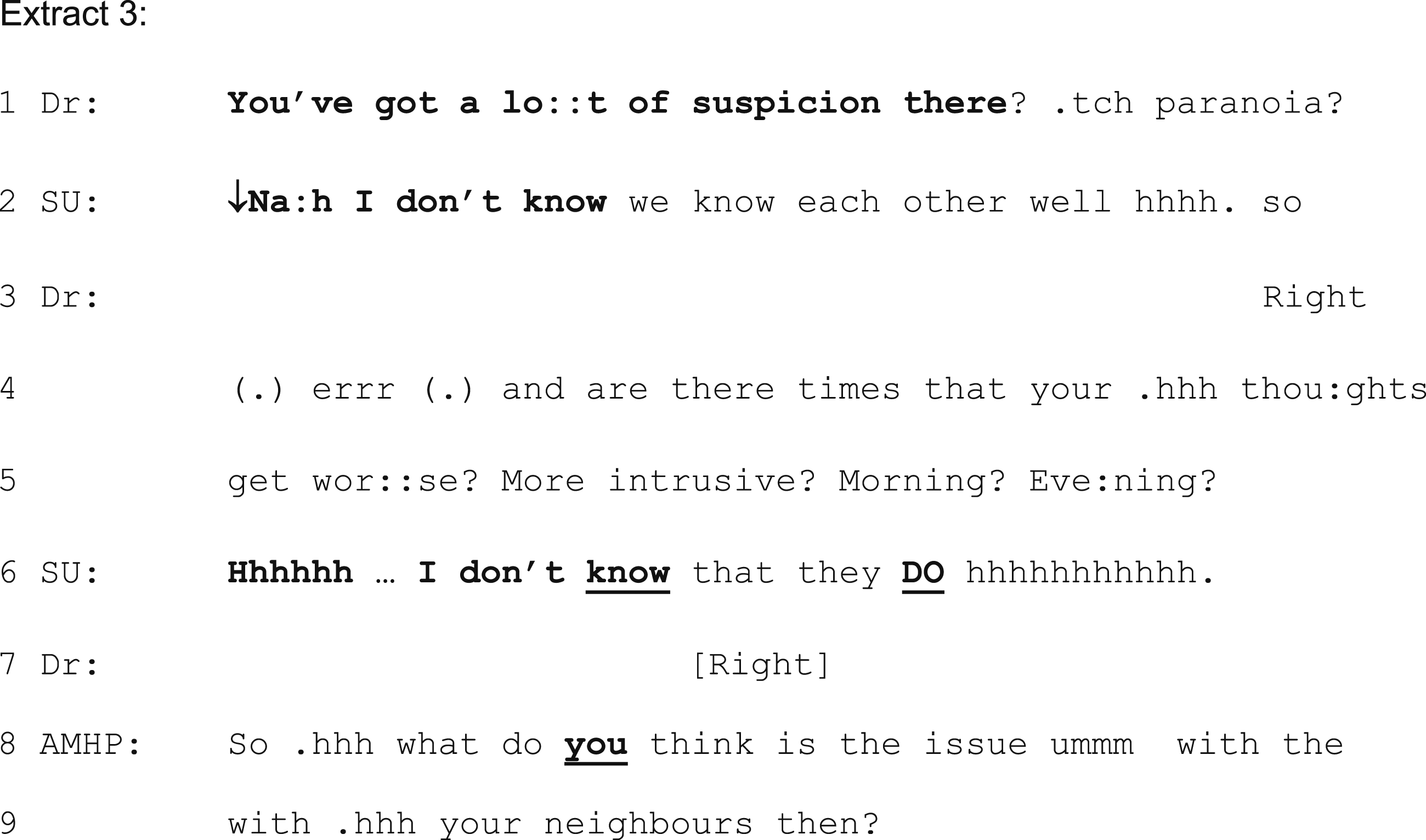
The service user says ‘I don’t know’ in lines 2 and 6. Lindström and Karlsson (2016) refer to ‘I don’t know’ (IDK) prefaces as ‘epistemic disclaimers’. Rather than displaying an actual, recognised lack of knowledge it is signalling interaction problems (and epistemic tensions and asymmetries) between participants, suggesting there is something about the proposition that cannot be accepted. As nonconforming responses, IDK responses are resisting something about the question and challenging the rights to knowledge. Their non-cooperative feature may also be used strategically to avoid talking about specific topics (Hutchby, 2005) and to head toward a more independent epistemic position (Heritage, 2002). This is observed and picked up by the AMHP who intervenes at line 8 and returns the conversational lead and ownership to the service user.
This type of technique was observed frequently, although there were times where alignment and affiliation were not always to be perceived by all parties. In Extract 4, below, the service user is presenting an interpretation of whose ‘side’ the AMHP is on. In this scenario, the doctor has stated that ‘we’ think the person needs to be in hospital. This immediately compromises the AMHP’s professional and statutory independence (they are as yet undecided about the outcome). The service user, rather than using the typical or expected neutral referent (‘the doctor’ or ‘he/she’) is doing more than just referring in this response.
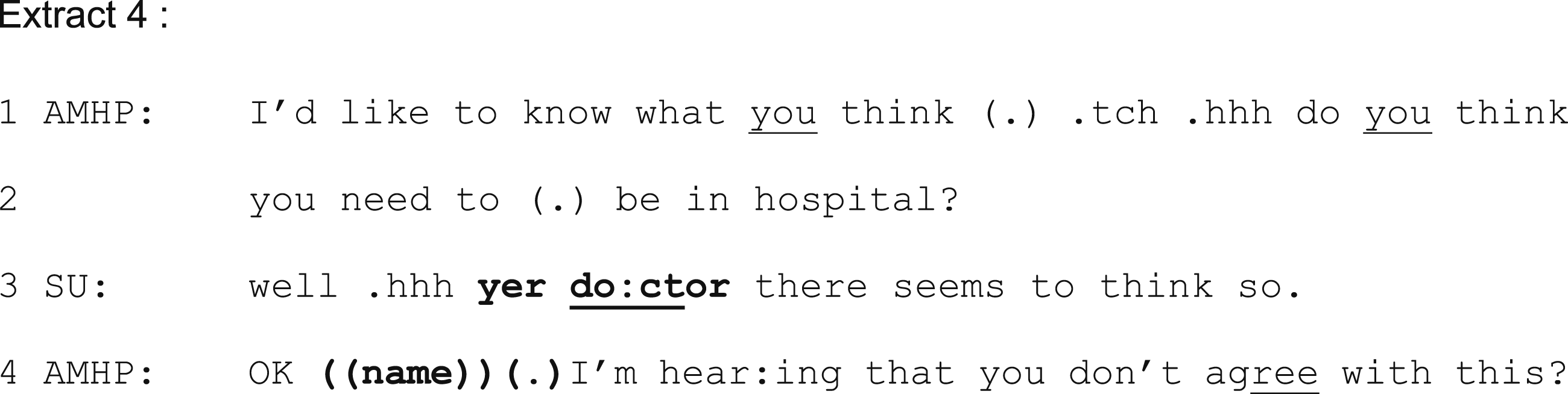
In using the alternative recognitional (Stivers, 2007) ‘yer doctor’ (line 3) the service user is demonstrably associating the AMHP with the doctor rather than with themselves. As a ‘marked’ form of reference, this can be an act of provocation and is similar to the classic ‘look at what your son has done now’, used to explicitly associate the referent (the parent) with the aberrant son. The AMHP hears and responds to this. At line 4, they use the service user’s name to personalise and register the concern and they attempt to realign. The AMHP simultaneously tries to downgrade both their own deontic and epistemic authority through the phrase ‘I’m hearing that’ (Muntigl et al., 2020) and, as such, they are deferring and conveying respect to the epistemic authority of the service user as well as attempting engagement and alignment.
Observations of this kind are subtle but powerful ways in which service users have spoken of being seen but not heard. Conversational exchanges convey clear messages about relative value and credibility of participants’ knowledge. When speakers request information, for example, they presuppose that the hearer has epistemic access to this information, whereas when they make announcements they are presupposing that the hearer does not (Stivers and Rossano, 2010). In Extract 5, the doctor’s announcement of a decision at line 1 (‘you are going to need to’) indicates their higher deontic status than the service user.

In Extract 6, however, the AMHP proposing an outcome in the form of a question claims more equal distribution of deontic status. The use of ‘we’ at line 1 also serves the purpose of an attempt at engagement and the sharing of knowledge and status.

This fine-grained study of AMHPs’ communicative actions highlighted the ways in which AMHPs, at times, would seek to repair and return epistemic privilege to service users. Specific types of questions served to advance or block conversations and these appeared to be important in hearing and inviting service users’ ideas and preferences. At times AMHPs aligned themselves with service users and shared perspectives. They adapted their alignments and affiliations as part of nuanced conversation. Communication moved beyond a static, linear exchange of information the more the service user was empowered to be involved within it.
Discussion
This study provided insight into AMHPs’ interventions within their statutory encounters. AMHPs are required to interview service users in a ‘suitable manner’ (s.13 C (2) MHA 1983) and findings here indicate that this can involve the addressing of conversational barriers as well as physical ones. The AMHP value base rests on a rights-based, justice focused approach (DHSC, 2019) and, arguably, the critical elements of such an approach include communication and dialogue, presence (‘being with’ the person) and the creation and promotion of facilitating conditions (Statsny et al., 2020).
AMHPs have professional and statutory imperatives involving the Empowerment and Involvement principle (DoH, 2015), specific professional responsibilities to ‘promote the rights, dignity and self-determination’ of service users (HMSO, 2008) and all this takes place against a wider backcloth of aspirations variously referred to as co-production, shared decision-making and supported decision-making depending on the context. Yet practice techniques, skills and training around how to do this are, as yet, undeveloped or absent and, to date, AMHP practice continues to lack a clear evidence base or organising theory. In this research, AMHPs did appear to intervene and co-ordinate their interventions but arguably did so at an intuitive level. There is, then, a need for a more deliberate, deliberative and measurable approach that simultaneously reengineers how AMHPs and service users work together. Crucially, it has been suggested from research with ASWs that those who feel inadequately trained and supported in the more subtle skills of their own profession may be more likely to defer to practitioners of more highly codified disciplines, such as psychiatry and the law, contrary to the statutory formulations of their own roles (Sheppard, 1995). There is, then, an urgent need for AMHPs to focus on their core professionalism and to begin to build an evidence base for their distinctive and unique role and the skills and professionalism within this.
It has been suggested that service users who have been involved in mental health services for some time have acquired a ‘learned expectation’ that they should assume a passive role in decisions (Rosén et al., 2001). Similarly, mental health service users have long described a ‘them and us’ experience (Akther et al., 2019; Barnes et al., 2000). In this research, there was evidence that AMHPs worked to downgrade their professional authority through their communicative actions, and they evidenced empowerment in the way that they restored epistemic primacy to service users who they viewed as being entitled to their subjective experience and, also, as having a right to communicate it.
Service users have described ambush, a sense of fait accompli and little discussion around options and alternatives to hospital admission, leaving them to believe that the only outcome could be admission (Barnes et al., 2000; Hemmington et al., 2021; Blakley et al., 2022). To rebalance this, approaches that are deliberately based on empowering, involving and supporting will enable AMHPs to consider the ways in which they can further consider the need for allyship, advocacy and a consideration as to who they are actually there for (Hemmington, 2024). Although coercive interventions are typically experienced negatively, their impact may be mitigated by kind and caring staff (Katsakou and Priebe, 2007; Wyder et al., 2015). People who have not felt coerced (even where they have been detained) believed they were actively involved in their admission and treatment process, were given information about the rationales, offered alternatives and given time to consider their options and to make decisions accordingly (Akther et al., 2019; Katsakou et al., 2011). In MHA assessments specifically, where things have been seen to have been manageable, or even to have gone well, the AMHP has listened or even acted as advocate/ally and ‘stood up’ for the person (Blakley et al., 2022; Hemmington et al., 2021).
AMHPs will always need to balance some form of a ‘paradox of empowerment’, not least in that they are both advocate and applicant for detention. However, AMHP work is fundamentally a socio-relational process involving a focus on the person in their environment (Abbott, 2021) and a greater focus could be toward ideals of democratised practice, allyship, having features of coproduction at the centre of the assessment (Hemmington et al., 2021) or, as the late Matt Simpson phrased it, ‘opening avenues to change gears and buy time’ (Simpson, 2024 p.1) to promote greater collaboration with service users. Within a context of time restrictions and high workloads, participatory approaches to assessment encounters, and with it a focus on fine-grained conversational encounters, may not seem to be a priority or even possible. Yet, the service user-professional relationship is the foundation for empowering and inclusive interventions. The relationship is not simply a prerequisite, it is essential in framing the context within which supporting, empowering and maximising service users’ self-determination occurs.
Overall, the ‘hows’ of enacting principles of information-sharing and decision-sharing has been described as being poorly understood or absent in mental health settings and these are compounded by a lack of training (Drake et al., 2010; Matthias et al., 2013; Morant et al., 2016). Training could begin to focus on an increasing attitude shift focusing on AMHP work as relational work, perhaps even addressing whether it could or should also support service users ahead of future MHA assessments (Blakley et al., 2022) as well as broadening the research to include medical colleagues. AMHPs’ coordinating role could certainly focus on the apparent inequality of the relative weight given to participants’ interactional contributions, and their vigilance can enable them to better steer the development of decision-making interactions at a micro-level.
Conversation Analysis, as a unique mode of enquiry, lends itself well to small sets of naturally occurring data (Potter, 2002; O’Reilly and Parker, 2013) including even single case analysis (Whalen et al., 1988) or very specific and idiosyncratic situations (Toerien and Kitzinger, 2007). For Robinson (2007) the integrity of the approach is grounded in the assumption of a known, recognisable order-at-all-points. Similarly, for Sheppard, 1993, the resources of past CA findings can be ‘brought to bear on a single fragment of talk’ (p.101) to support findings in new or different scenarios. Certainly, applying an understanding of conversational manoeuvres and evidence illuminating the ways in which conversations are forwarded or blocked served to shed light here on the very specific conversations that take place between AMHPs and people they interview.
Finally, while the pause button has been pressed on the Independent Review of the MHA in England (DHSC, 2018), the point that service users’ knowledge and perspectives are discounted or undermined within decisions about care and treatment still stands. It seems likely that there will be an ongoing acknowledgement that across all the statutory and professional landscapes culture change will be required to address service users’ participation, involvement and co-production methods.
Conclusion
This research introduced, for the first time, ways in which evidence-based models for AMHPs’ communication can begin to be developed through greater vigilance over the role of epistemics and conversational manoeuvres. There is a much-needed introduction and discussion about what AMHPs are, in actual fact, doing. Previously, ways in which AMHPs enact, find evidence for and report on their application of the statutory Empowerment and Involvement principle, as well as their professional imperative to maximise service users’ self-determination, has been absent. Additionally, AMHPs’ co-ordinating role has long been perceived as merely setting up an ‘assessment’ scenario in practical terms. This research however illustrated ways in which they extended their co-ordinating role to one which carried into and throughout the conversations themselves. At times, their work gave the appearance of a skilful directing of traffic, choreography or conducting of the conversational movement, including deliberate work to subtly advocate for people and to restore and oversee harmony.
Despite perceptions of invisibility or being misunderstood, this research shows how AMHPs bring clear and measurable skills to complex situations. There are now opportunities to start to build on this emerging evidence and, with it, to acknowledge AMHPs’ distinct professional role, skills and purpose. An ongoing focus on relational dynamics and being explicit about what happens behind the scenes brings this area of practice to greater scrutiny. Qualitative research of this nature needs to be developed in order to move a step further in developing an original and much-needed evidence base for AMHP practice. This study introduces a template for future training and a critical evaluation of practice, encouraging a deliberative approach to AMHP practice which can re-engineer how AMHPs and service users work together.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.