
Abstract
Seeking and receiving social support following violent and abusive relationships is a complex process, involving a range of barriers for anyone. LGBTQ survivors of intimate partner violence face additional barriers to both seeking and receiving appropriate help, yet few studies have explored the way these barriers are navigated from the experiential viewpoint. Knowledge of the subjective journey to access social support may help improve social work practice with LGBTQ people leaving abusive relationships. This study explored the lived experiences of support-seeking through in-depth interviews with LGBTQ survivors of IPV in Sweden (n = 7, age range 18–56). Interpretative Phenomenological Analysis was used for interview design, conduct, and analysis to offer a detailed, first-person, and contextual account of the support-seeking process. Drawing on a phenomenological analysis of lifeworlds, five main themes were produced which illuminate some of the shared experiential features of participants’ journeys to access support. Within each main theme, the analysis also highlights divergences relating to participants’ differing lifeworlds. The analysis thus provides an in-depth, phenomenological understanding of the support-seeking process, including the barriers to, but also the individual and social enablers of, seeking support. Support-seeking processes for LGBTQ survivors of IPV may, at the experiential level, be more diffuse than current theoretical models suggest, with relational ‘strategies of navigation’ being of primary concern to individuals. For policy and practice, the importance of the wide range of generic professionals, who may be the first point of contact, should be emphasised, as well as the role of family and friends as a support and catalyst in the support-seeking process.
Keywords
Introduction
Seeking and receiving social care and support is an integral but complex part of leaving violent and abusive relationships. Many survivors of intimate partner violence (IPV) seek informal support from family and friends and/or formal support, such as from health professionals, the police, and social workers (Calton et al., 2016; Liang et al., 2005). Part of what makes help-seeking complex relates to a range of barriers that adult survivors of IPV in general may face, such as a lack of awareness of IPV and available services, lack of accessible services, fears of consequences of disclosure, lack of material resources, personal barriers, and systemic failures (Robinson et al., 2020). LGBTQ survivors of IPV face additional barriers to both seeking and receiving appropriate support (Calton et al., 2016; Edwards et al., 2015), such as limited understanding of the problem, stigma, and systemic inequities. A key challenge for social work practice with LGBTQ survivors of IPV concerns how to understand and work with internal or psychological barriers to support-seeking, as well as promoting informal social systems that may support the survivor.
There is scant research, however, that has followed both formal and informal support-seeking from the experiential viewpoint of LGBTQ survivors of IPV on their ‘journey’ from problem identification to receiving help. Such qualitative knowledge may help to better tailor support and outreach services for LGBTQ survivors of IPV. The present study aims to contribute to this gap in the literature via an Interpretative Phenomenological Analysis (see Smith et al., 2009) of in-depth interviews with a Swedish sample of LGBTQ survivors of IPV who sought help, either formally or informally.
Support-seeking among LGBTQ IPV survivors
Liang et al.’s (2005) model of seeking social support following IPV highlights that there are three stages in the help-seeking process: recognising there is a problem, deciding whether to do something about it, and selecting a source of help. In each stage there are individual, interpersonal, and sociocultural barriers to seeking help. The original model was based on heterosexual/cisgendered IPV survivors, but in a later application, Donovan and Barnes (2019) argued that for LGBTQ survivors there are additional barriers at each stage of the help-seeking process.
Similar to heterosexual/cisgendered survivors of IPV, LGBTQ survivors are more likely to seek informal support, such as from friends or the LGBTQ community, rather than formal support (Edwards et al., 2015). However, even if informal support is the preferred source of help, not all survivors have access to a network that would support them. If the person is unsure of or ashamed or closeted about their sexuality, turning to friends may be too big an obstacle as this requires both disclosing their sexuality and the violence (Hardesty et al., 2011). One study of transgender survivors of IPV concluded that most participants did not have supportive family structures (Guadalupe-Diaz and Jasinski, 2017), which places a greater onus on friends or the LGBTQ community.
The LGBTQ community can sometimes, however, be a barrier to seeking and receiving support. Lesbian women who share their experiences of abuse in the queer community may encounter other queer women disbelieving them or not wishing to engage in the conversation (Harden et al., 2020). This has been interpreted in relation to ‘the myth of lesbian utopia’ – the idea that lesbian communities are safer than heterosexual communities because the absence of men, and that a relationship between women is naturally egalitarian (Barnes, 2011; Harden et al., 2020; Walters, 2011). 1 In cases where the queer community is the only source of social support, it can be a huge risk to disclose being abused by another queer woman. The partner may be well-known in the community and the desire or need to keep ties to the community is thus a barrier to seeking help within the community (Harden et al., 2020). This can be put in the wider context of societal homophobia; because same-sex relationships are already marginalised, there may be a reluctance to seek help outside of the LGBTQ community so as not to reflect badly on the community (Guadalupe-Diaz and Jasinski, 2017).
Both informal and formal support systems are, however, nested in societal structures, which have effects at the individual level. The main societal narrative of IPV can be viewed as having roots in the discourse of ‘cisgendered heteronormativity’ (see Donovan and Barnes, 2019). Briefly, this hegemonic discourse renders other patterns of sexuality, gender identities, and sexual practices not just invisible, but in contrast to the acceptability and even desirability of the cisgendered-heteronormative identity and life. Thus, the normative story of IPV is of a physically stronger cisman that is physically violent to a weaker ciswoman, both of whom have been living as a heterosexual, monogamous couple. This makes it harder to tell or hear other stories of IPV, which in turn has consequences for LGBTQ survivors seeking support (see Ovesen, 2021). For example, the partner who is physically larger may be assumed to be the perpetrator, whether that is true or not (Harden et al., 2020). Transgender survivors’ experiences of IPV can be doubted as they are ‘too butch’ or ‘once a man’, or they can struggle to access formal resources that are dichotomised along traditional gender binaries, that is, male/female (Guadalupe-Diaz and Jasinski, 2017). One study found that among transgender survivors of IPV, genderqueer/non-binary respondents who were assigned female at birth and trans men were most likely to seek help (Messinger et al., 2021). This may be because they have easier access to woman-centred service agencies, if cisnormative service agencies erroneously code them as women.
In Sweden, there have been some efforts at the national level to broaden the narrative of IPV. The national strategy to combat ‘men’s violence against women’ addresses IPV in the LGBTQ community (SOU, 2015), although the general framework given in the strategy’s title may alienate some LGBTQ survivors of IPV. Actual support services for IPV are devolved to local councils. While some councils may have their own specific policies or action plans for LGBTQ survivors of IPV, only 12% have previously reported that they are adequately prepared for LGBTQ IPV survivors, and the lack of services particularly concerned transgender people (SOU, 2017). For example, while women’s shelters in Sweden nowadays usually welcome trans women, there are still few shelters for trans men.
Among IPV survivors who seek formal help, services are not always tailored for their needs and are often perceived as unhelpful or even harmful (Edwards et al., 2015). Survivors considered services helpful if the providers were knowledgeable, resourceful, and were non-judgemental about LGB populations (Edwards et al., 2015). Questions remain, however, about the experiential process of seeking social support, both informally and formally. For example, how are fears about homo- or transphobic services (or society in general) experienced in the decision to seek help? How do issues of identity and community affect support-seeking, and how are psychological and societal barriers understood and experienced by LGBTQ survivors of IPV?
The present study
The present study aims to explore the lived experiences of seeking social support among LGBTQ survivors of IPV. Liang et al. (2005) proposed that research is needed that captures the diverse experiences of decisions to seek help and which help is chosen. Our study aims to capture both internal, subjective processes, as well as external, physical, and social processes. For this, a phenomenological perspective provides a fruitful approach to researching individual, lived experience (see Dahlberg et al., 2001). Methodologically, we apply Interpretative Phenomenological Analysis (IPA) (see Smith et al., 2009) with the aim of providing in-depth, contextual, first-person accounts of survivors’ own narratives; in short to understand survivors’ experiences from their own perspective. To our knowledge, IPA has not previously been used in studies of support-seeking following IPV. Chan and Farmer (2017) argued that IPA could be an important methodological tool for understanding the experiences of people in LGBTQ communities. IPA has also been used in similar studies of experiences of seeking help and support (e.g. Dawood and Done, 2020).
The study includes both those that found help/support, but also those that did not, in order to explore the process through which LGBTQ survivors of IPV make sense of their situations. Both informal and formal help-seeking are included. Firstly, previous research has highlighted that LGBTQ survivors may be more likely to turn to informal support. At the same time, there may be obstacles to relying on informal support in cases where coming out has led to troubled relationships with friends or family or if the community is not perceived as a possible source of support. Secondly, it may be the case that informal support is an important stepping stone to accessing formal support. By having a phenomenological, experiential starting point, we aim to follow the stories or ‘journeys’ of each of our participants.
We draw on a sample of survivors of IPV in Sweden. Sweden provides an interesting case study as it tends to be viewed as a progressive country in terms of equality and tolerance generally, and regarding LGBTQ rights specifically. In 2021, Sweden was ranked the second most LGBTQ-friendly country in the world for LGBTQ travellers. 2 Most (95%) of the Swedish population think that LBG people should have the same rights as heterosexual people (Forte, 2018). Additionally, Sweden is characterised as a high-income country with a well-developed welfare state (Lindbom, 2001) thus providing good conditions for formal social support services.
Materials and methods
Design
The current study used single in-depth interviews and the methodological approach drew on IPA (see Smith et al., 2009). IPA builds on phenomenological and hermeneutic philosophical traditions to explore the way that people experience their lives and how they make sense of their experiences. It has been described as a distinctly psychological qualitative approach but to experiential, rather than discursive, research (Eatough and Smith, 2006a). While IPA recognises that experience is shaped by social processes – and shares common ground with, for example, Foucauldian approaches – it also argues that experience cannot be reduced to language (Eatough and Smith, 2006b). The sum of the phenomenological field – the lifeworld – includes physical, material, emotional, and relational experiences, as well as discursive or meaning-making aspects of these experiences. IPA acknowledges that accessing another’s lifeworld is only possible indirectly via understanding how the other makes sense of their lifeworld. Thus, phenomenological interviews are largely a joint exploration of participants’ lifeworlds, where participants’ own understandings of their experiences are brought to the fore through an open, empathetic style of interview. Thus, the interview guide contained only a few themes such as the process of deciding to seek support, what kind of support was wanted, and experiences of support. The guide was used in a flexible manner to follow the participant’s stories, through a listening and supporting style of interviewing with a phenomenological focus on drawing forth accounts of experiential and sense-making features.
Sampling and procedure
IPA uses purposive sampling, where a small number of participants with a common experience is sought. The study had four inclusion criteria. The participant needed to: (1) self-identify as LGBTQ, (2) have been subjected to intimate partner violence, (3) have wanted to have and/or had sought support within the last five years, (4) be 16 years or older.
Participants were recruited via adverts in social media. LGBTQ-organizations and activists helped spread the advert online. The recruitment advert was viewed over 12,000 times and clicked on over 400 times. Nine people made contact and received an information letter about the study and eight participated (including giving their informed consent). One participant was excluded from this article since they were subjected to violence from a parent, giving seven participants in total. Due to Covid-19 restrictions, interviews were conducted either via Zoom or telephone at the choice of the participants. Four interviews were conducted by the first author. Three interviews were conducted by the second author. An LGBTQ-certified counsellor was available to speak to the participant following the interview, if the participant so wished. The study was approved by the Swedish Ethical Review Authority (Dnr, 2020-05698) and conformed to the principles of the Declaration of Helsinki.
Analytical approach
The interviews were on average one hour long (range 37–78 min) and were recorded and fully transcribed. The transcriptions were analysed following methodological guidance in Smith et al. (2009). In brief, the analysis aims to explore participants’ life worlds and sense of their lived experiences – their thoughts, emotions, and physical experiences – and the meaning made of these experiences. IPA recognises, however, that the analyst must also make sense of participants’ own sense-making – the ‘double hermeneutic’ – which makes IPA avowedly interpretative (Smith et al., 2009). Drawing on case-study method and idiography, the analysis proceeds with several detailed readings, line-by-line notations, and a preliminary analysis of each case in turn. This results in emergent themes for each participant. These are then compared in an iterative, cross-case analysis, where commonalities and divergences are explored and organised into higher and lower order themes for the sample as a whole. This process involves continually returning to the transcript to check interpretations against the preliminary notations and the interview extracts in the context of the interview as a whole. Both authors engaged in several rounds of iterative discussion to arrive at the resulting thematic structure.
Participants
Pronouns, gender/sexual orientation, and pseudonyms of participants.
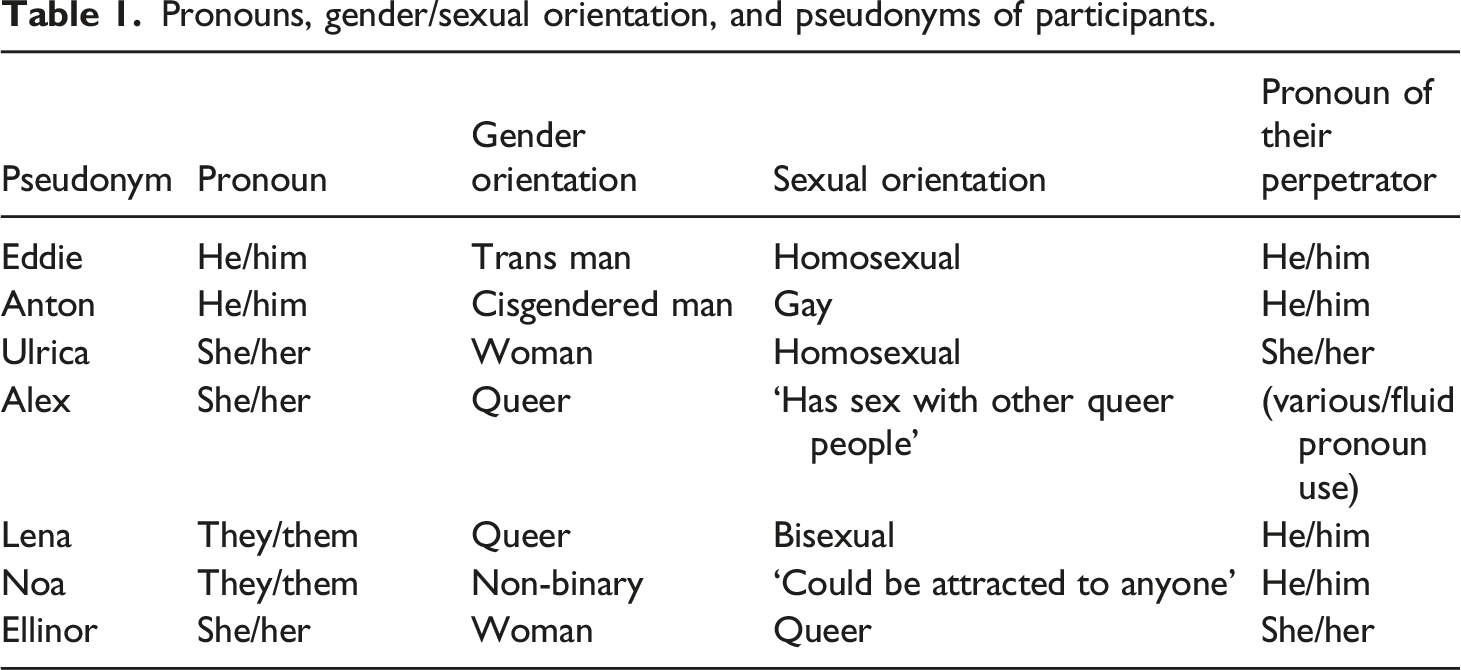
The participants were not asked about ethnicity, but all interviews were conducted in Swedish, and all participants spoke fluent Swedish. All quotes are the authors’ translations.
The participants were subjected to violence from a partner with whom they had a longer relationship and lived together under the same roof. With one exception, the participants were subjected to violence within 2–5 years of the interview.
Results
The analysis of the interviews resulted in five main phenomenological themes. These illustrate, at a broad level, commonalities between the participants’ lived experiences of support-seeking as survivors of intimate partner violence. Each of the themes will be explicated in turn, using quotes and interpretive analysis to demonstrate some of the idiographic variations within each theme. As a sign-posting device for the reader, the higher-order theme headings are listed here: (1) Doubts and worries about seeking support, (2) Signalling and hoping to be understood, (3) Navigating between solidarity, identity, and help-seeking, (4) Being seen and understood, (5) Need of support today.
All participants had sought support from someone during or after the violence, even the participants who had stated before the interview that they had not sought any kind of support. Most participants had sought support informally from family and friends. Six of the seven participants had sought professional support, whereof two had sought support from social services. Other examples of formal support sought were school counsellor, teacher, police, hospital, health centre, psychologist, psychiatry, women’s shelter, and suicide hotline. It can be noted that none of the participants described seeking support at organizations for LGBTQ people, such as the Swedish organization RFSL. 3
Doubts and worries about seeking support
All participants described doubts and worries relating to seeking support. These doubts had different expressions: lack of direction in where to turn for support, fear of not being believed or taken seriously, and doubt about whether their experiences were real violence, or if the violence was severe enough to have the right to support. Ulrica, a gay woman, felt that she had no clear vision of from whom to seek support, or how. In the quote below, she exemplifies a sense of parallel worlds, where women’s shelters exist, but not for her since the perpetrator was a woman:
Ulrica initially relates her lack of knowledge about where to get help to being in her first real relationship, but on almost instant reflection she sees that a women’s shelter could have been an option. An interpretation here is that in Ulrica’s lifeworld being homosexual automatically excluded such support services for women, as ‘women’ was interpreted as ‘women in relationships with men’, creating not lack of knowledge, but a general doubt about where to turn as a gay woman. Most participants mentioned women’s shelters as a potential source of support, but not all felt that they could seek support there, either because they were not ciswomen or because their partner was a woman.
For some participants, doubts and worries about seeking formal help were more directly connected to fears about how they would be treated or what the consequences would be of making contact. Ellinor, a queer woman, describes a situation where although she described fearing for her life, she didn’t dare call the police. She relates her reluctance to seek help to being disbelieved in some way as an LGBTQ person:
Ellinor refers to a ‘something’ that she fears the police might start; we interpret this diffuse fear as being about the prospect of negative questions which focus on her sexuality, and the wider idea that marginalised sexual identities would be treated suspiciously. For some other participants, the fear of not being believed or being believable was also in relation to their partner. Many participants had moved in with their partner and lacked their own accommodation. Some participants had dropped out of school, were on sick leave from their work, or lacked employment. Many also described mental illness and self-harm, often because of the violence. In summary, they feared that their partner would be perceived as the trustworthy person since the partner, at least from the outside, appeared to be the ‘responsible citizen’.
Eddie, a transman, presented a slightly different angle of being afraid to contact formal support services. He feared that the trauma of his abuse would be used against him in his gender reassignment treatment:
In other parts of the interview, Eddie described a picture that all formal support services probably share information, and that there is no possibility of confidentiality or anonymity. Thus, he fears that if he talked about his experiences, for example at a local, municipal service, that this information would be shared and used against him.
Only two of the participants had experiences of the local social services office, which in Sweden is generally tasked with providing support following IPV, regardless of sexual/gender identity. In general, none of the participants had a clear idea of what kind of support they could get there, such as financial and housing support. Some participants had experienced doubts about whether the violence that they had received was IPV and within the remit of ordinary formal support. Noa, a non-binary person who described their experiences as ‘subtle psychological manipulation and torture’, felt that they could not relate to the societal story of physical IPV. They attributed this to the fact that it was their first relationship, and that their partner used his experience of earlier relationships to explain what was right and wrong. For Noa, there were other IPV survivors more deserving of help: those in acute situations of physical violence. This then positions Noa’s experiences as not acute or less worthy, creating a dilemma about seeking help. Similarly, Anton, a gay cisman, also described how his picture of IPV was shaped in relation to how society talks about IPV, and concludes that this made it difficult for him to understand his experiences:
Anton is referring to a few years earlier when, as a teenager, he had never heard of men being subjected to violence in relationships with other men. Set against such a backdrop, his experiences were initially hard for him to make sense of. Thus, in Anton’s lifeworld, doubt and worries about seeking support had been at a proto-stage of making sense of what had happened to him. We interpret his reference to ‘they never said’ (our emphasis) as the effects of the wider societal discourse that IPV is men’s violence against women.
Signalling and hoping to be understood
All participants had in some way communicated to people in their surroundings that something was wrong in their relationship. In many cases, it was difficult for other people to see and understand this, but also hard for the participants to explicitly ask for support. As often is the case in IPV generally, most participants gradually became isolated from friends and family, which made it more difficult to see what was happening from the outside. Most participants described feeling shame and withheld information so that others would not see how bad the situation was. At the same time, there was a hope that someone would see and understand. Alex, who identified as queer, felt that it was friends who first expressed that something was wrong, which led to a sense of both shame and relief.
For Alex, the sense of shame grows or becomes more tangible in the moment of the problem being witnessed by others. This suggests that Alex had carried the weight of the stigma silently herself for some time, and hence the relief that comes with (finally) being ‘seen’ or understood. Noa also described a sense of living with the silent weight of stigma, yet hoping that someone would notice. Noa was living with their partner after dropping out of school and as the relationship progressed, Noa gradually lost contact with most of their friends, which made Noa think that no-one would ever discover that they were being abused. Noa reflects on when someone did eventually notice:
That this was the first time that ‘anyone had reacted’ suggests that there were, for Noa, many other times when people could have noticed and reacted. Noa’s sense that there were ‘definitely others who’d have noticed’ also gives a picture of living with the shame or stigma of imagining that people do see and know that something is wrong. Noa’s acknowledgement of the difficulty for others to act suggests both the actual difficulty (for Noa) in understanding their own situation but also perhaps an excusatory view of those who didn’t react sooner.
Anton, Ellinor and Ulrica all described that it was hard to tell anyone about the violence because their partner showed a positive picture of their relationship on the outside and in social situations. Their partner thus controlled the story of their relationship in front of others. For example, in Ulrica’s case, the partner was seen to minimise the violence by making it appear as funny in front of others:
For Ulrica, signalling that something was wrong became a more complex, drawn-out process where she had to counter the narrative being controlled by her partner. Eventually, when Ulrica had stopped contacting her family at all, another sibling got in touch and asked directly if something was wrong. Ulrica described a slow, careful ‘trickling out’ of information, which we interpret as testing her own narrative – and more importantly, testing if others would understand and ‘see’ her story – in the face of the dominant story told by her partner.
The lack of understanding by others was in some cases more clearly connected by participants to the heteronormative interpretations of other people. For Anton, his outward physical build was viewed as making his experiences of abuse less comprehensible for other people. In the next extract, he recounts a situation where he described the abuse to a nurse whom he met after he tried to commit suicide as a result of a series of severe beatings from his partner:
Anton describes the clash between the normative story of who is subjected to IPV and his own appearance. He understands that his appearance can make his story harder to grasp for others. Thus, despite the nurse being the first person that Anton felt listened to him, this was accompanied by facing the nurse’s sense of shock and initial difficulty in comprehending him as a survivor of IPV, creating an extra layer to the interaction for Anton to handle regarding being understood.
Navigating between solidarity, identity, and support-seeking
Some of the participants described situations in everyday life where they were met negatively as LGBTQ people, in the form of offensive comments, always being attributed the wrong pronoun, or in other ways questioned by people in their surroundings. This meant that the validation and sense of belonging with other LGBTQ people, either to the partner or to a wider community, became vital. Some participants described how this sense of belonging, and the loyalty that follows, made it hard to share their experiences of violence with the very community that would otherwise be a source of support.
Ulrica described that her abusive partner was comfortable in her own identity and was the first person to affirm Ulrica’s sexual identity. When the violence escalated, it was hard to let go of the feeling of acceptance.
Ulrica explained how she glossed over the violence and did everything for the relationship to function, to keep the sense of affirmation in her sexuality. This in turn delayed her in arriving at the decision to seek support. Similarly, Alex portrayed a need to defend other queer people in general, including the partner who abused her:
For Alex, there is a solidarity with the queer community at all costs. The defence against a heteronormative society has a negative: you cannot say that another queer person is violent towards you, which meant, for Alex, that she felt that she could not ask for help from the people who she would ordinarily turn to. Ellinor described a similar dilemma: she felt shame in relation to both the queer community and mutual friends, and wanted to protect both herself and her partner by not speaking about the violence. A consequence of not being able to speak to her closest friends was that she lost the chance to get their perspective on questions such as: is this right, is this normal, would you tolerate this if it happened to you?
When deciding to seek support, there was a common view among the participants that the support for survivors of IPV is mainly for women subjected to violence from men. Queer or lesbian women – and non-binary people who feel they are able to pass as cisgendered women – may therefore decide to pass as heterosexual women to get access to support. This can be done by relying on the heteronormative support system to assume that you are a cisgendered heterosexual woman, or to present the partner as a man in order to get general guidance about IPV without risking a negative reaction. Lena, who identified as queer, participated in a group treatment for women subjected to intimate partner violence, and concluded that:
Lena’s ‘ability’ to pass as a ciswoman shows another angle to how some participants navigated between identity and help-seeking. In this case, Lena appears not to mind being misgendered as the group treatment was valuable.
Being seen and being understood
Most of the participants had at least one person who they felt understood and ‘saw’ their situation and gave them the support they needed. Sometimes this came from a friend, a family member, an NGO, a municipal or regional support provider. The positive sense of support was presented in terms of a personal, non-judgemental, and understanding approach, as well as some level of knowledge of the issues of both IPV and LGBTQ.
Noa described that a close friend had provided support throughout the process, both providing perspective but also patience to let Noa arrive at their own decision. For Anton, it was a nurse with whom he had slowly built up a trusting relationship over a series of hospital visits, who both provided an attentive, empathic attitude, but also who gave directive or motivational advice. He described something that seems as simple as someone who cared and listened. Both Ellinor and Lena had received support from a municipal support centre for victims of sexual abuse and prostitution after they left the abusive relationship. Lena described that the support centre had broad knowledge of violence and sexual abuse, which made it possible for them to feel normal and for their reactions to be seen as normal reactions to trauma.
Being seen and being understood for Lena is both a sense of a caring, empathic response, but also being normalised. The interpretation we make here can be taken further in that being understood is in part the act of the other – in this case Lena’s therapist – who ‘explains things’, that is, puts Lena’s experiences into words that make her feel normal and human. Ellinor also recounted a similar experience of meeting someone who she felt understood her experiences. She felt that she did not have to explain her experiences in the same way she would need to do somewhere else, suggesting an accepting and non-judgemental approach by the person she met.
It’s not over because it’s over – need of support today
Although it was not a question included in the interview guide – nor an intended focus of the study – all participants described having a remaining need of support, whether they had sought support or not. These needs were described as psychological, social or relational consequences in form of low self-confidence, poor self-image, insecurity, jealousy, or avoiding sexual/romantic relations entirely. For some participants, there was an enduring sense of needing professional help. Noa described thinking about looking for a psychologist, but needing someone who understood both IPV and LGBTQ issues. They also concluded that ‘it would be nice’ to meet someone who do not misgender them.
For Anton, he felt that he had turned to self-injury to deal with his experiences. He described feeling ugly and disgusting, recounting feelings of worthlessness and, although he described feeling much better today, expressed a need to speak to ‘a professional’. Alex also relayed a similar need and had made several attempts to get psychological support, but had been put off by long waiting times within the public healthcare system. At point of interview, she was avoiding forming new relationships.
Ulrica also described negative consequences for forming new relationships, but for her there was also a sense of broken trust towards societal systems with an over-hanging sense of injustice.
Discussion
The theme of ‘Doubt and worries about seeking help’ found in our study was described in a similar fashion in Liang et al.’s (2005) framework concerning help-seeking among women subjected to violence from men. Whilst the participants in our study had similar doubts about what had happened to them, and whether they should act or accept the situation as normal, there were additional layers of doubt and worry. These concerned fear of receiving a negative response to their sexual/gender identity, difficulties defining the violence, and how the violence will be perceived by both informal and formal networks. This is alongside uncertainty in a more practical sense about what support is available for LGBTQ people. These issues can be understood partly as a product of a largely heteronormative, if not at times homophobic, society (Donavan and Barnes, 2019). The fear of a negative response is likely to be based on one’s own or other people’s actual experiences. Calton et al. (2016) highlight that the societal image of IPV as heterosexual men’s violence towards heterosexual women is so strong that even professionals can misjudge signs of IPV among LGBTQ people.
Navigating survivorhood?
A first step for social work outreach concerning IPV is identifying (and helping survivors identify) the abuse. Some of the participants in the present study had difficulties themselves in coming to an understanding of their experiences as violence or abuse, for example when being overly controlled, monitored, or neglected. While this is not uncommon for IPV in general, our analyses also confirm that being in one’s first LGBTQ relationship, regardless of age, can create an extra layer of doubt about ‘normality’, on which abusers can capitalise to control their partner further. Donovan et al. (2014) termed this as experiential power, in the sense that a partner who has more experience – in terms of more sexual partners or relationships as a LGBTQ person, who is out and has connections to LGBTQ peer groups – can have the power to set the ‘rules’ of the relationship. However, our analyses also draw attention to the complexity of factors involved in ‘navigating survivorhood’ as a relational phenomenon, such as growing isolation from friends and family, how signals from the survivor that something is wrong are sent, but also read or misread by friends and family, alongside newness and/or security in the LGBTQ identity. Hardesty et al. (2011) made the point that if survivors were living in a more closeted manner, they instead tried to solve the problem alone, rather than turning to their informal network. However, we suggest that being ‘closeted’ or not is one important aspect, alongside the role of which others are available in the informal support network, their responses, as well as loyalty to the LGBTQ community.
Our findings also have implications for the theoretical understanding of social work models of support-seeking processes following IPV. Liang et al.(2005) model of help-seeking builds on how the problem is understood more instrumentally, for example, as a crime or a health issue. Our analysis of help-seeking from an experiential viewpoint suggests a more diffuse, but relational process of understanding the problem via other people; the importance of via whom one trusts in and seeks support. Moreover, navigating survivorhood may depend on how informal resources respond, but also how formal resources, such as social work outreach, present the support they offer. The process of deciding where to seek support was a meandering, at times drawn-out, experience for most of the participants; none of them started with a clear view of the problem nor which resources were for them or who to turn to. Ovesen (2021) terms this process the ‘vicissitudes of help-seeking’ to capture in LGBTQ IPV survivors’ iterative, subtle attempts to get help. When deciding whether to seek informal support, participants in the present study had to judge carefully which people would believe them, test the waters by slowly releasing part of the story, and then turn to those who were most trusted to listen to their experiences. Those who described themselves as part of a larger LGBTQ community struggled with their perceived need for belonging or loyalty to the group, which meant that they felt that they could not speak negatively of another LGBTQ person in the community. When deciding whether to seek formal support, participants had to navigate other questions, such as trying to find out what support there is generally, which support if any is for LGBTQ people, deciding whether it is beneficial to try to pass as a straight cisgendered woman if possible, and overcoming both expected and experienced negative responses. Our suggestion is that these ‘navigatory’ concerns are more central to the social support-seeking process for LGBTQ survivors of IPV.
These strategies of navigation in support-seeking used by our sample of seven participants varied from intensive trial-and-error-approaches (one of the participants named at least 15 different attempts) to speaking to only one friend who noticed that something was wrong. The understanding of the problem – and what to do about it – appears, however, to develop partly in relation to responses, both formal and informal. The second main theme of the analysis – ‘Signalling and hoping to be understood’ – highlights a cautious testing of reactions from informal networks. As part of the navigation strategy, it may be that this kind of testing of one’s own understanding in relation to how people respond is an important part of problem formulation and understanding that support is needed. However, it is important to note that even when participants were met with incomprehension or, worse, tacit refusals of help, some hope remained that they would be understood as survivors of IPV. In cases where such understanding was not received, a sense of general injustice remained.
On the other hand, the theme of ‘Being seen and understood’ points to some central if not, simple features of what ‘good’ understanding means. Basic qualities such as empathy, listening, non-judgementality, as well as consistency (i.e. being there over time) were highlighted. Such features are common to many broad therapeutic approaches, for example, Rogerian principles of person-centred counselling (see Mearns and Thorne, 1999). Some participants also highlighted that skill, knowledge, or competence in LGBTQ issues also played a role, suggesting that ‘good’ understanding requires more than just generic counselling skills.
Understanding what support is available
The analysis also has implications for social work policy and practice concerning services for survivors of IPV. It is apparent that the help structures that the participant met, or expected to meet, had a cisgendered-heteronormative way of understanding the dynamics of IPV. This highlights the need for IPV support services to be alert to whether and how their public documentation and external communications includes a range of potential IPV situations. Rather than descriptions of services having a passive role in defining what support can be given, our analyses draw attention to the potential active role of communication about services to help survivors of IPV describe and define what they might need help with. This may particularly be the case where survivors are struggling both with defining the abuse, but also have (justified) preconceptions about the set-up of services.
In terms of actual service delivery, the current study highlights the wide range of general professionals, beyond social workers, with whom IPV survivors come into contact in their support-seeking process: teachers, school counsellors, workplace managers, nurses, doctors, the police, debt counsellors, and so on. While specialist social workers may competently deal with IPV survivors in LBGTQ populations, there is a huge range of general services that have a key role to play as the first point of contact towards accessing formal support. As recounted by some of the participants in the current study, if this first contact is negative, it becomes the only contact. Some participants, for example, struggled with getting professionals to understand that they were subjected to violence because their gender expression did not match the stereotype of an IPV victim or because their perpetrator was not a man. Donovan and Hester (2015) have previously maintained that IPV is often implicitly understood as a problem for heterosexual people, and as a problem of mainly physical violence and with gender norms influencing the understanding of what a victim and perpetrator looks like. Such norms may be the target of developmental work for general professionals who are the likely first point of contact.
Most participants were unsure of what resources were available for them as survivors of IPV, excluding mentions of a women’s shelter. Adult survivors of IPV are in general unaware of resources available for IPV, especially resources that are specific to identity communities (Robinson et al., 2020). The societal view of IPV may in part shape the way available resources are perceived, for example that women’s shelters may be seen as only for (cisgendered) women who are subjected to violence from men. However, some participants had understood the notion of social support as being for acute needs and, in particular, from physical violence. This stands in contrast to the range of long-standing support needs mentioned by participants, such as psychological and emotional trauma, relational and sexual issues, alongside debts and other legal and financial issues. In Sweden, similarly, no doubt, to many other countries, there are a number of municipal services that could provide support in these areas (if you know they exist). Thus, there may be a need to better advertise that these services are available as well as directing survivors of IPV to them.
A final implication for practice concerns the role of family and friends. The analyses in the current study highlight that the process of turning to friends and family for support is not always a simple, one-step, process. Rather, it is potentially a cautious, meandering process where the survivor may ‘trickle out’ information to test how people react, particular in the face of a more dominant narrative being controlled by the abuser. Even when friends and family realise what is happening, they may not know how best to react. Providing support to friends and family in how they in turn can help someone who may be being abused may also be a useful part of support services.
Limitations and future directions
The purpose of the phenomenological analysis in the current study was to provide a context-specific, experiential analysis, giving depth and nuance as a contribution to the existing literature. The hermeneutic concept of parts illuminating the whole lends weight to the idea that we can learn about more broad principles based on specific cases. Our sample is, however, specific to its context. It is interesting that despite Gothenburg having a reputation as LGBTQ-friendly city, this did not seem to translate into noticeable results in terms of positive IPV help-seeking experiences, at least in this sample. There may be other context- or culturally specific aspects to the sample which could mean that the results do not readily translate to other contexts. Thus, similar research in terms of method is warranted with samples in other contexts.
The sample is also specific to the method of recruitment, which was advertisements in social media. While the advertisement received over 10,000 views, we have no way of knowing what proportion of a presumed ‘total’ LGBTQ population saw it. The sample was slightly skewed in terms of age towards the 18–30 age group, which may also be an effect of the recruitment strategy. It is noteworthy that there were no participants over the age of 56, which means that the experiences of middle aged and older LGBTQ people are not represented. This is important as support-seeking strategies among older LGBTQ people may differ. For example, elderly care staff may be an important first point of contact. Future research should consider efforts to include older populations or have this population as a sole focus.
Conclusion
The current study adds to the literature by providing a nuanced, phenomenological, first-person, and in-depth account of the barriers to, but also the enablers of, the support-seeking processes in LGBTQ survivors of IPV. Such an account of the subjective journey to access social care and support could help improve social work practice for LGBTQ survivors of IPV and beyond. While we used a sample comprising a mixture of sexual and gender identities, our results point to many commonalities in the support-seeking process, both among LGBTQ people, but also with survivors of IPV in general, such as growing isolation from ordinary social networks. The results also suggest that help-seeking processes for LGBTQ people may be more diffuse than current models of support-seeking following IPV allow. Rather, relational ‘strategies of navigation’ appear to be of primary concern, in terms of both the ‘journey’ of understanding oneself as a survivor of IPV, alongside the ‘journey’ of getting both informal and formal support networks to act and react positively.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.