
Abstract
This mixed-methods systematic review aims to synthesise current research to identify the risk and protective factors of wellbeing in the dementia social care workforce. Seven databases were searched in April 2024 for evidence published between January 2003 and April 2024, focusing on the risk and protective factors for wellbeing in the dementia social care workforce. Titles, abstracts and full text articles were screened by two reviewers. A deductive thematic analysis and narrative synthesis was performed on extracted data to reveal four themes. 5,237 qualitative and quantitative records regarding the dementia social care workforce in the UK were screened. 13 studies were included. Taking an ecological systems approach, risk and protective factors of wellbeing in the dementia social care were narratively synthesised into key themes including structural factors, interpersonal factors, personal attributes and factors generating a systemic sense of value. Our findings indicate that dementia social care workers experience many risk and protective factors to their wellbeing at multiple levels. Whilst these factors for wellbeing were categorised into themes, these often overlapped and should be considered together when addressing wellbeing in the dementia social care workforce. Therefore, a multisystem approach is required to fully address the wellbeing of the dementia social care workforce.
Introduction
Dementia is a growing public health priority in the UK, with prevalence projected to reach 1.4 million people by 2040 (Wittenberg et al., 2024). The progressive decline in cognition and motor skills associated with dementia often necessitates full-time support, much of which is provided by an estimated 700,000 unpaid carers and supplemented by paid social care staff in the UK (Carers UK, 2021; Clarkson et al., 2017; Donnellan et al., 2022). At least 60% of people receiving home-based social care, and 70% of older age residential care in England, are people with dementia (Skills for Care, 2024b). Adult social care workers therefore play a crucial role in supporting people with dementia and their families across all four UK nations.
Social care provision for people with dementia in the UK includes domiciliary care, respite services, day care centres, residential care, and peer support (Hussein & Manthorpe, 2012). Workforce structures differ by nation: Wales, Scotland, and Northern Ireland require registration and qualifications, while England lacks a statutory register and has lower qualification thresholds (Nuffield Trust, 2023). These structural differences, combined with variations in training, as well as chronic underfunding across all UK nations due to fiscal constraints and spending priorities (Needham & Hall., 2023; Oung, 2020), contributes to inconsistencies in quality and continuity of care (Alzheimer’s Society, 2024; Nuffield Trust, 2023). Consequently, local authorities have been forced to direct less funding to social care over time. These services are however vital in easing burden on unpaid carers and promoting wellbeing for people with dementia (Giebel et al., 2023; Samsi et al., 2022). This value has been extensively documented over the past decade across the UK and in recent years by multiple stakeholders, including healthcare professionals (Bergmann et al., 2022), third sector organisations (Alzheimer’s Society, 2025), as well as people with dementia and their unpaid carers (Giebel et al., 2023). The Covid-19 pandemic highlighted this value also, as service closures significantly harmed the mental health of both people with dementia and their carers (Giebel et al., 2020, 2021; Hanna et al., 2022). Similarly, the pandemic reportedly exacerbated existing pressures and brought about new challenges for adult social care workers, which includes care workers for people with dementia (McFadden, Ross et al., 2021, McFadden, Neill et al., 2021). Shortages of personal protective equipment, increased workloads, and greater emotional strain reduced wellbeing across the workforce (Donnellan et al., 2022; McFadden, Ross, et al., 2021). Since wellbeing is recognised by the World Health Organisation (2021) as a fundamental resource for daily life shaped by personal, social, and structural factors, addressing systemic challenges in dementia social care is vital to improve outcomes for people with dementia, carers, and the social care workforce itself.
Caring for people with dementia is associated with negative health consequences for both unpaid carers and professional care staff across the world (Fleming & Taylor, 2007; Islam et al., 2017; Lindeza et al., 2020; Reid & O'Brien, 2021). While the impact of providing unpaid care for someone living with dementia has been widely studied, less is known about paid dementia care workers, despite evidence that health and social care professionals are at heightened risk of stress-related conditions (McFadden, Ross, et al., 2021). Stressors for staff include emotional and physical demands; insecure contracts; low pay; long hours; complex client needs; poor work–life balance; and inadequate dementia training (Giebel, Prato, et al., 2024; Ravalier et al., 2021). Recruitment, retention, and skills shortages are persistent problems across all devolved nations and internationally (Eborall et al., 2010; Elliott et al., 2012; Hussein & Manthorpe, 2012; Skills for Care, 2024b). Compared with staff supporting people without dementia, dementia care workers often report higher stress, lower job satisfaction, more injuries, and greater risk of mental health problems (Ben-Arie & Lecovich, 2014; Costello et al., 2019). UK-based dementia care workers also report poorer wellbeing than their US counterparts (Islam et al., 2017). Taken together, this evidence indicates that the wellbeing of the dementia social care workforce may be under considerable strain
Much of the available evidence frames workforce challenges from the perspective of client or organisational outcomes, such as service quality, cost-effectiveness, or staff turnover (Backhaus et al., 2014; Hicks et al., 2004; Hussein & Manthorpe, 2012). Research also often adopts a deficit-focused lens, emphasising workforce weaknesses such as limited dementia-specific training, with the goal of improving client outcomes (Surr et al., 2017). Far fewer studies focus on the wellbeing of dementia social care workers, leaving their mental health underexplored. As Kitwood (1997) and Higgs and Gilleard (2016) argue, recognising the personhood of paid carers is as important as that of those they support. Shifting towards an asset-focused approach, one that builds on workforce strengths and resources, could help balance service demands with carer wellbeing, a direction increasingly recommended in UK policy (Local Government Association, 2010, 2020).
For the purposes of this review, the dementia social care workforce refers to non-clinical adult social care workers who provide person-centred, practical, emotional, and social support in residential, respite, domiciliary, and day-care settings. These workers play a central role in supporting independence and maintaining quality of life, hereafter referred to as “workers” or “the workforce” (Alzheimer’ Society, 2026; Hussein & Manthorpe, 2012) Key roles for this workforce include personal care and support, medication and health monitoring, emotional and social support, and practical assistance. Given the multifaceted nature of wellbeing and the workforce, this review applies an ecological systems perspective (See Figure 1), drawing on Bronfenbrenner’s Ecological Systems Theory (1979), McLeroy’s Ecological Model of Health Behaviour (1988), and the Dementia Inequalities Model (Giebel, 2024). These frameworks converge in recognising that individual outcomes, such as wellbeing, are not solely determined by personal characteristics, but are shaped through the dynamic interaction of interpersonal, community, and broader structural or societal influences. They highlight how health behaviours and inequalities in care emerge from these dynamic systems and provide a foundation for identifying the systemic changes necessary to safeguard the wellbeing of dementia social care workers. This figure illustrates the conceptual alignment between Bronfenbrenner’s Ecological Systems Theory (1979), McLeroy’s Ecological Model of Health Behaviour (1988), and Giebel’s Dementia Inequalities Model (2024). Although developed in different disciplinary contexts, each model situates individual outcomes within nested layers of influence. At the individual/intrapersonal level, personal characteristics and resources are central. The interpersonal/microsystem level captures relationships and social networks. The community/meso–exosystem level reflects the role of organisations, local structures, and cultural norms, while the structural/macrosystem level highlights broader societal, policy, and systemic determinants. By mapping these frameworks together, the diagram emphasises their shared recognition that outcomes emerge through the dynamic interplay of factors operating across multiple ecological levels. 
This review therefore aimed to systematically synthesise current evidence to provide clearer solutions to addressing the poor wellbeing of the workforce by addressing the following research question: “What are the risk and protective factors associated with wellbeing in UK-based dementia social care workers?”
Method
The protocol for this mixed-method systematic review was prospectively registered with PROSPERO [ID: CRD42024538042].
Search Strategy
Search Terms

Inclusion and Exclusion Criteria

Study Selection
During stage 1, two researchers (JB, AM, ratio of screening 80:20) screened the titles and abstracts of retrieved records, excluding articles that did not meet the inclusion criteria. At each screening stage, all included titles were merged from both reviewers, enabling random selection of the next quota of titles in the screening process. This was to ensure consistency in the screening process. The selected records in stage 1 were read in full during stage 2 by the same two researchers and articles that met the inclusion criteria (See Table 2) were included in the final review. Discrepancies (n = 4) during screening were resolved through team discussion.
Data Extraction
Data was extracted (JB) from 13 included studies into an Excel spreadsheet, including: Location within the UK; population; focus; design; measures; qualitative themes or quantitative outcomes; setting; and period of data collection (see Table 3). Categorisation of risk/protective factors was discussed with the research team and two PPI advisers with lived experience of providing domiciliary care for people living with dementia (CB (manager) and PG (CEO) from the same third-sector domiciliary care organisation supporting adults, including people living with dementia.) Disagreements (6%) were resolved collaboratively. Following extraction, an ecological systems approach was taken to synthesise extracted risk and protective factors before being narratively synthesised into themes and added to the data extraction table.
Quality Assessment
Study quality was independently assessed by JB and AM using the QualSyst tool (Kmet et al., 2004) (see Table 4). Quantitative studies were evaluated against 14 criteria and qualitative studies against 10, scored from 0 (not addressed) to 2 (fully addressed). The mixed-methods study (n = 1) was appraised separately for each component, generating two scores in line with recent reviews (Giebel et al., 2024). ‘Not applicable’ could be selected for quantitative criteria. Quality ratings informed interpretation but did not affect study inclusion. Scores of >80%, 70–79%, 50–69%, and <50% indicated strong, good, adequate, and poor quality respectively. Reviewer discrepancies (n = 4) were resolved through discussion.
Data Synthesis
A deductive thematic analysis and narrative synthesis were undertaken, guided by Ecological Systems Theory (Bronfenbrenner, 1979), the Ecological Model of Health Behaviour (McLeroy et al., 1988), and the Dementia Inequalities Model (Giebel, 2024). Risk and protective factors were mapped across four ecological categories (see Figure 1 and Table 5) to guide initial theme formation, before being narratively synthesised to form final themes through team discussion. As this is a mixed-method review, findings were interpreted complementarily, by synthesising quantitative and qualitative evidence separately and then jointly. This enabled confirmation of findings across multiple research methodologies.
Results
Overview of Included Studies
Data Extraction of Included Articles

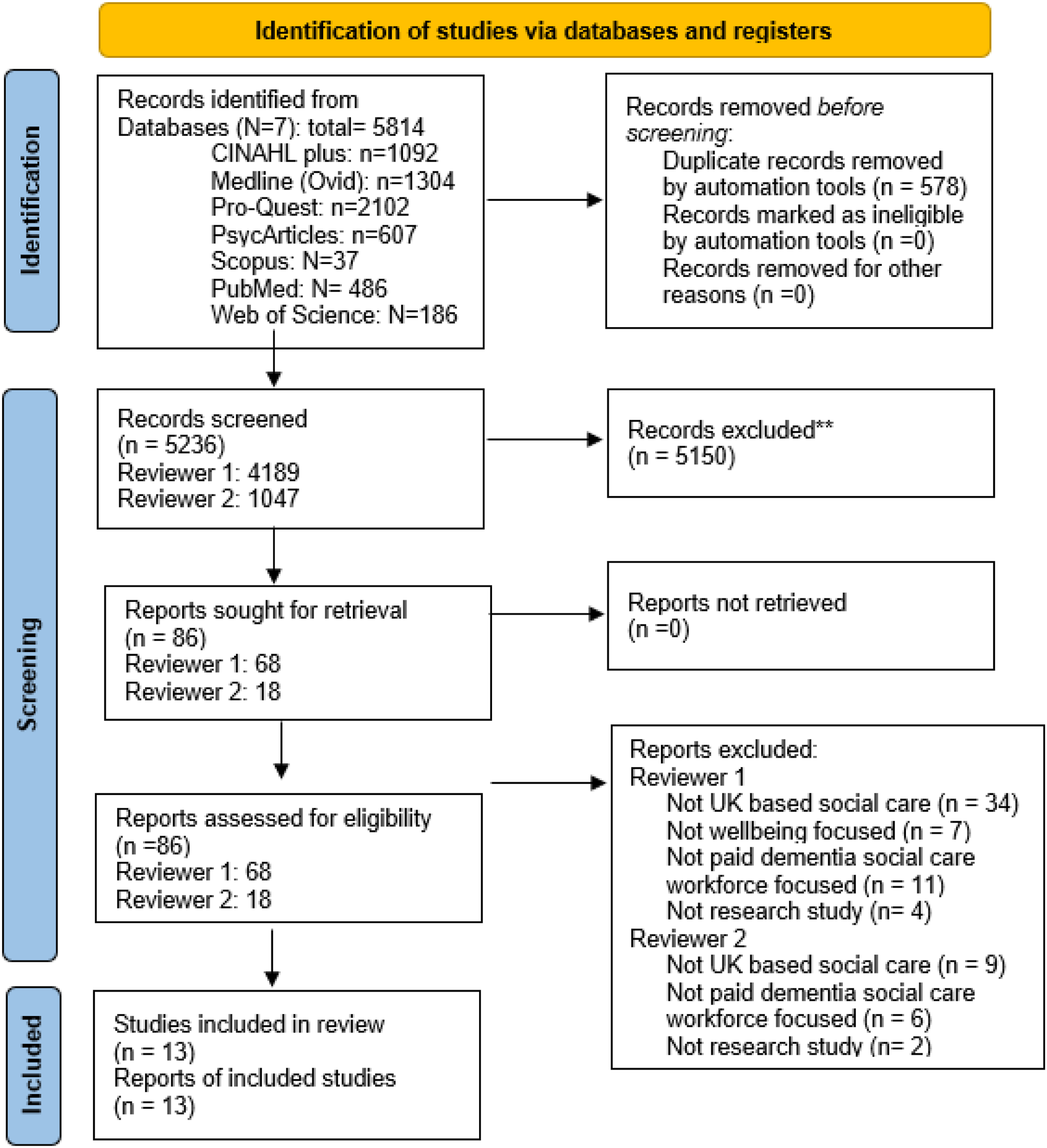
PRISMA flow chart showing included/excluded studies
Ten (76.9%) studies used qualitative methods, primarily semi-structured interviews with open-ended questions; one study also adopted an ethnographic approach, collating observations and semi-structured interview data
Quality Ratings
Final Agreed Quality Assessment Ratings for Qualitative and Quantitative Studies Included in Systematic Review

Narrative Synthesis
Summary of Extracted Risk and/or Protective Factors for Well-Being in Dementia Social Care Workers, Categorised in Terms of The Ecological Systems Framework and Resulting Themes

(N) reflects article number from Table 3
Structural Factors
All studies referred to structural factors that acted as risk and protective factors for wellbeing in dementia social care workers. Poor working conditions were commonly reported risk factors and were linked to workers leaving the sector. Reported organisational issues included poor shift scheduling and a lack of guaranteed hours, expectations to work longer hours (particularly during sickness cover), high workloads, unsociable lone-working hours, poor organisational communication channels, especially in emergency situations, and low pay (Briggs et al., 2021; Donnellan et al., 2022). Such conditions often led to negative health consequences over time, such as high levels of stress, anxiety and exhaustion (Leverton et al., 2021), forming risk factors for poor wellbeing in workers and reducing their quality-of-life over time (Healey et al., 2023).
Eight studies also reported a systemic lack of support as a risk factor for workers wellbeing, which emerged from organisations and wider governmental and societal systems. Organisational gaps included insufficient managerial and emotional support, limited respite between shifts, inadequate guidance when care challenges arose, insufficient dementia-specific training, and limited access to workplace mental and physical health support (Giebel, Prato, et al., 2024; Kadri et al., 2018; Leverton et al., 2021; Manthorpe et al., 2019). Wider system failures included funding cuts, which reduced access to healthcare professional support and increased workloads beyond role scope (Herron et al., 2020; Manthorpe et al., 2019), alongside inadequate guidance and PPE during the Covid-19 pandemic (Briggs et al., 2021). Such factors all posed substantial risks to workers’ wellbeing, often resulting in the experience of negative emotions, greater levels of stress and persistent anxiety, hence the finding that dementia social care workers were the least supported of all staff in care home settings (Islam et al., 2017).
Structural protective factors for wellbeing were also identified by nine studies. Organisational practices that facilitated a positive work culture included regular staff meetings and supervisory operations, 24/7 organisational communication, open-door management support policies, clear support pathways, dementia care training and flexible working arrangements were reported to protect workers from negative health consequences by creating a positive work culture. These practices reduced isolation by enabling workers to discuss role-related challenges experienced in their day-to-day carer roles (Donnellan et al., 2022; Giebel, Prato, et al., 2024; Hughes et al., 2023; Leverton et al., 2021; Manthorpe et al., 2019).
The final protective structural factor for wellbeing included teamwork. Teamwork that was encouraged across the organisation by managerial staff, and transcended the organisation, promoted a positive work culture for workers, facilitating wellbeing. This included teamwork across multiple professions such as managers and office staff as well as with external health professionals (Herron et al., 2020). Organisations that encouraged and facilitated teamwork across the workforce also enabled better dementia care to be delivered by creating a shared space for workers to learn from each other’s experiences. This increased self-efficacy within workers and satisfaction with their jobs (Herron et al., 2020; Manthorpe et al., 2019), facilitating wellbeing in-turn.
Interpersonal Factors
Nine studies identified interpersonal risk and protective factors for wellbeing. Interpersonal factors related to relationships within and across organisations, particularly staff relationships. Several studies reported limited cohesion and reciprocity due to lone working and minimal organisational contact (Donnellan et al., 2022; Duffy et al., 2009; Leverton et al., 2021). Combined with limited emotional support, this often resulted in emotional exhaustion, acting as risk factors for poor wellbeing (Duffy et al., 2009).
Discrimination and marginalisation were also identified as interpersonal risk factors. Two studies reported discrimination from clients, colleagues and society often attributed to class, race, and professional level (Hughes et al., 2023; Kadri et al., 2018). Experiences ranged from refusal of care from clients, prejudicial statements from other staff members, as well as bullying, harassment, and daily microaggressions from others in the community and within the workplace (Hughes et al., 2023). These experiences contributed to fear, negative identity issues, and physical and mental exhaustion, reducing their ability to maintain wellbeing. Poor organisational responses by management further exacerbated distress, and reinforced feelings of inadequate support. In the absence of managerial support, some workers adopted coping strategies such as emotional distancing, ignoring incidents or avoiding discriminatory situations, protecting their wellbeing consequently (Hughes et al., 2023). However, this sense of resignation to racism also caused difficulty to adjust in the workplace and led to further isolation and marginalisation, acting as a risk factor for wellbeing overall. Seven studies identified interpersonal protective factors, particularly informal support networks developed by workers. These networks often emerged where formal support was limited and included collaborative working with clients, peer support during joint shifts, informal guidelines for colleagues, supportive meetings, and communication via mobile technology (Hughes et al., 2023; Leverton et al., 2021; Manthorpe et al., 2019). Informal educational practices, such as learning from colleagues’ experiences, were also common (Manthorpe et al., 2019). This support from co-workers was integral to the continuity of care for clients and therefore autonomy of the workforce overall. Such support promoted a special sense of community, camaraderie and unison, protecting against poor wellbeing consequently (Donnellan et al., 2022).
In addition, workers also relied on external support networks such as family and friend networks. Such support provided workers with an informal outlet to discuss work related challenges and the burden that such challenges come with, consequently promoting wellbeing (Donnellan et al., 2022; Manthorpe et al., 2019).
Personal Attributes
Eight studies identified personal attributes that acted as risk and protective factors for wellbeing, including workers personal circumstances, education, and work-life boundaries.
Five studies highlighted work-life boundaries as both risk and protective factors for wellbeing. Adequate boundaries in client-carer relationships protected care workers from emotional over-involvement. Positive relationships could enhance job satisfaction and a sense of pride (Donnellan et al., 2022). However, overly close relationships could compromise wellbeing and expose workers to significant sources of emotional and physical burden (Leverton et al., 2021), particularly when workers took work home emotionally (Donnellan et al., 2022; Kadri et al., 2018), lacked respite from work life, or experienced client deterioration or death (Hughes et al., 2023). In some cases, blurred lines between clients and workers’ relationships led to deep emotional distress and experiences of heartbreak and grief in the event of client deterioration, presenting as a significant risk factor to wellbeing (Herron et al., 2020). This therefore highlights the delicate balance workers must employ to protect themselves from the negative consequences of the carer role, evidencing an area of support workers require from formal structures.
Workers also used personal coping strategies to support wellbeing, including humour, stoicism, self-care, hobbies and reflective practices (Donnellan et al., 2022; Hughes et al., 2023). The value of such methods in promoting wellbeing is evidenced by Travers et al. (2019), where workers report the benefits of diary writing in helping them to process difficult emotions and maintain their wellbeing. This is because diary methods enable workers to express their feelings whilst confronting issues that might otherwise remain unacknowledged. The diary method reportedly promotes clarity of thought, emotional regulation and increased self-awareness of care practices, enabling self-evaluation and promoting worker’s wellbeing consequently. Although such methods are helpful in providing temporary relief from the negative consequences of the carer role, they should not replace effective support from the organisation and wider systems.
Adequate dementia education and training were also identified across several studies as both risk and protective factors, forming a pertinent recommendation for future implication (Duffy et al., 2009; Giebel, Prato, et al., 2024; Hughes et al., 2023; Islam et al., 2017). Personal development in the form of training and education promoted and protected wellbeing in workers due to creating feelings of inner value, strength and resilience (Hughes et al., 2023). Importantly, Duffy et al. (2009) found that high self-efficacy seemingly acts a buffer against burnout in workers. Conversely, inadequate dementia education and training reduced confidence in workers ability to perform their role, creating inner personal conflicts and negatively impacting workers wellbeing (Duffy et al., 2009; Manthorpe et al., 2019). It is important to highlight that education as a personal factor also overlaps with structural factors, as care organisations should provide specific role training.
Factors Generating a Systemic Sense of Value
Five studies highlighted factors relating to workers feeling systemically valued. Feeling recognised as individuals with psychological and physical needs influenced wellbeing. Recognition could come from organisations, government bodies and other healthcare professionals, including NHS staff (Hughes et al., 2023; Kadri et al., 2018; Manthorpe et al., 2019). Workers sometimes reported feeling valued when completing tasks beyond the scope of their role. While this temporarily promoted wellbeing, this often led to high role expectations from the organisation and other healthcare professionals, creating an unmanageable weight of responsibility in workers, and causing conflict between different professional levels (Leverton et al., 2021). Staff were therefore often caught between delivering person-centred care and operating within a task-oriented system, which contributed to feelings of underappreciation, diminished personhood (Kadri et al., 2018), and adverse mental health consequences linked to marginalisation. In some cases, completion of tasks was prioritised over employee wellbeing because of a lack of national recognition of the carer profession (Giebel, Prato, et al., 2024), fuelling this feeling of a systemic lack of value.
Feeling valued was also linked to organisations responding effectively to workers’ needs, including addressing discrimination from multiple areas including the government, colleagues, and the public. Where care organisations failed to act, workers felt a diminished sense of identity, out-of-control and unimportant, leading to negative emotions and diminished wellbeing (Hughes et al., 2023). Workers consequently reported a sense of systemic injustice, creating a sense of mistrust in the organisations and deeper feelings of isolation and marginalisation within the workplace. This was particularly highlighted during the Covid-19 pandemic, as identified by Hughes et al. (2023), where professional discrimination was alleged at multiple levels and led to comparisons between roles. This created a sense that some roles were prioritised over others, highlighting disparities between dementia social care workers and the National Health Service (NHS), acting as a risk factor for poor wellbeing in some workers.
Discussion
This is the first mixed-methods systematic review to comprehensively synthesise evidence for risk and protective factors associated with wellbeing in UK dementia social care workers from an ecological systems perspective. Whilst this review highlights clear areas to be addressed within dementia care workers’ wellbeing, removing these interpersonal, structural and personal risk factors for wellbeing, and promoting a sense of feeling valued across workers, is not always possible. This is largely due to wider structural issues, such as a lack of financial support and guidance from the UK Government (Oung et al., 2024). These structural pressures are widely reported across adult social care; however, they may be particularly pronounced for dementia care workers due to the additional complexity of dementia-specific care needs.
It is also important to acknowledge limitations within the evidence base. Only two quantitative studies and one mixed-method study were identified, with some having small sample sizes. This likely reflects the strong emphasis on lived experiences within dementia care research, where qualitative approaches are often prioritised compared with broader adult social care research. Nevertheless, the current review identified a diverse range of qualitative methodologies, including semi-structured interviews, ethnographic observations, ethnographic interview methods, and diary methods. This methodological diversity provided in-depth insights into the experiences of dementia social care workers from multiple perspectives, enabling a more comprehensive understanding of risk and protective factors influencing wellbeing within this workforce specifically. However, the limited number of quantitative and large-scale studies contrasts with the broader adult social care literature, where larger workforce surveys are more common, highlighting a gap in dementia-specific workforce research. Future studies should therefore adopt more diverse methodological approaches, including larger-scale quantitative work, to strengthen the empirical foundation for policy and practice.
An ecological systems approach revealed several structural risk and protective factors for wellbeing, including poor working conditions, a systemic lack of support, positive organisational practices and teamwork. Although social care work generally involves significant emotional and practical demands, dementia social care workers may experience these pressures more intensely due to the complex and progressive nature of dementia-related needs (Backhouse & Ruston, 2022). However, the current review also highlights that preventable organisational factors further diminish wellbeing. Irregular and lone working hours, poor organisational communication channels, and low pay all contribute to poor working conditions for dementia social care workers (Briggs et al., 2021; Donnellan et al., 2022), challenges which are also widely reported across the wider adult social care workforce. Such risk factors, intensified during the Covid-19 pandemic, contributing to workforce attrition and increased organisational strain (Briggs et al., 2021), mirroring patterns seen across the adult social care sector more broadly.
Potential solutions identified by dementia workers in this review included introducing regulated staff schedules and improving out-of-hours contact with supervisors, particularly during emergencies. Such measures align with Skills for Care (2014), who recommend effective and consistent support and communication lines for workers, achievable through assistive technology such as mobile communication systems (Wilson & Small, 2020). Similarly, improving the poor working conditions identified such as low pay, may help to protect the wellbeing of the wider social care workforce, who remain among the lowest paid staff in England (Allen et al., 2019; Sissons et al., 2017). The introduction of a National Pay Framework (Hemmings et al., 2024) has therefore been proposed as a sector-wide solution to recruitment and retention challenges affecting both dementia care workers and the broader adult social care workforce.
Organisations can further support wellbeing by encouraging teamwork among workers and other health professionals, promoting a positive work culture across the organisation in-turn (Skills for Care, 2014; 2024a). An effective way to reduce workload pressures would be to increase the number of dementia specific social care workers, considering the high vacancy and turnover rates reported in social care recently (Mian & Mutebi, 2025; Office for National Statistics, 2025). However, workforce shortages may have particularly significant implications for dementia care services due to the specialist knowledge and continuity of care required. This review therefore supports current recommendations outlined in ‘The Workforce Strategy for Social Care' report published by Skills for Care (2024b). Addressing such structural factors may therefore contribute to increasing workers’ sense of feeling valued and help to reduce the deep feelings of neglect reported by dementia care workers from multiple stakeholders, which appear more pronounced than those reported across the wider adult social care workforce (Oung et al., 2024).
Improved organisational support, including stronger teamwork within and across multidisciplinary teams, may also reduce interpersonal issues such as workplace discrimination related to class, race, and professional level, helping to promote a sense of feeling valued in workers. While such interpersonal dynamics are present across the adult social care workforce, they may be intensified in dementia care settings where roles and responsibilities are often less clearly defined across professional boundaries. Organisations should therefore ensure roles are clearly defined to both workers and wider professionals (Skills for Care, 2014; 2024a) to protect workers from role creep and the workplace conflict this can cause. Although role ambiguity is recognised across adult social care generally, its impact may be greater in dementia care where workers often undertake emotionally intensive tasks without clear professional delineation
Promoting formal and informal dementia education (Giebel, Prato, et al., 2024; Islam et al., 2017) may improve working conditions and wellbeing by addressing the comparatively lower self-efficacy reported among dementia care workers relative to the wider adult social care workforce (Duffy et al., 2009; Rasmussen et al., 2023), potentially supporting workforce retention. While training needs exist across the adult social care sector, dementia-specific knowledge gaps appear particularly significant due to the specialised communication, behavioural management, and person-centred care approaches required when supporting people living with dementia. Dementia training is therefore consistently recommended (Surr et al., 2017) to boost confidence, self-efficacy, and care outcomes for people with dementia and unpaid caregivers. Despite this, a lack of formal education remains (Giebel, Prato, et al., 2024; Manthorpe et al., 2019), potentially contributing to the inadequate work-life boundaries, and the associated emotional distress dementia care workers reported in this review as a result of client deterioration, particularly during the Covid-19 pandemic
Taking an asset-focused approach however, this lack of formal education resulted in the formation of informal support networks across dementia care workers which provided peer learning and a positive space for discussing dementia specific client-related challenges, such as difficult client behaviour. This is known as behavioural and psychological symptoms of dementia (Rasmussen et al., 2023; Zidén et al., 2024) and includes the physical and verbal aggression reported in the current review (Backhouse & Ruston, 2022). These informal strategies therefore helped to protect staff wellbeing (Donnellan et al., 2022); highlighting a key strategy to supporting dementia social care workers specifically; a novel finding within this review.
Informal support networks were also particularly effective in managing workforce fear and protecting wellbeing during the Covid-19 pandemic. While the pandemic negatively affected the mental and physical health of the adult social care workforce broadly, dementia care workers faced additional pressures due to the vulnerability of people living with dementia to infection, the disruption of familiar routines, and the exacerbation of behavioural symptoms associated with isolation (Capstick et al., 2022). Staff shortages due to self-isolation policies, illness, funding restraints, and equipment shortages, such as adequate personal protective equipment, therefore negatively impacted dementia care workers mental and physical health (Briggs et al., 2021; Hughes et al., 2023). Similarly, personal attributes such as self-identified coping methods found in the current review also helped to protect worker wellbeing and should therefore be encouraged by organisations to help promote worker wellbeing. Nevertheless, although these are positive adaptations to significant sources of stress for workers, suggesting workforce resilience, this also exposes shortages in organisational support, warranting further investigation since not all informal practices may protect wellbeing in all workers.
The ongoing funding crisis in UK adult social care may prevent these gaps from being addressed, however. All regions of the UK have reported underfunding over the past decade due to fiscal constraints and spending priorities (Needham & Hall., 2023; Oung, 2020). For example, central government grants, the main source of income for English local authorities, decreased by 40% in real terms between 2009/10 and 2019/20; from £46.5bn to £28.0bn (2023/24 prices) (Atkins & Hoddinott, 2024), with similar trends across devolved governments of the UK. Even with emergency grants administered by Central Government to alleviate the additional pressures that the Covid-19 pandemic caused, local authority spending power still fell by 21% in real terms between 2009/10 and 2021/22 (Atkins & Hoddinott, 2024). Consequently, local authorities have been forced to direct less funding to social care over time, which may have prevented local authority care providers from improving poor working conditions for staff. While these financial pressures affect the overall adult social care workforce, their impact may be particularly acute in dementia care services, where higher staffing levels, specialist training, and additional time for person-centred support are often required. Limited funding may therefore restrict the ability of providers to employ additional dementia-trained staff to alleviate workload pressures.
As a result, high vacancy and turnover rates across adult social care have been reported, (Dodsworth & Oung, 2023; Office for National Statistics, 2025; Skills for Care, 2024a), widening the gap in available care workers for people with dementia. This has contributed to an overstretched workforce, that is often unable to provide consistent, personalised care that people with dementia need (Skills for Care, 2024b). Therefore, to address such economic issues in dementia care and protect workforce wellbeing, a multidimensional approach must be employed by multiple stakeholders, as previously campaigned for by Alzheimer’s Society (2019; 2025). A key step towards this, advocated for by Godard-Sebillotte et al. (2024), would be implementation of a dedicated, sufficiently funded and sustainable National Dementia Strategy, which government plans have lacked since 2009. Such a strategy would help to outline specific objectives to address the challenges within dementia care, aiming to improve the care, support, and resources available to meet the needs of the sector, including its care workers.
Strengths and Limitations
This review has highlighted intersectional risk and protective factors for wellbeing in the dementia social care workforce, enabling a positive, asset focused approach to be adopted in the future. The novel approach to data synthesis, utilizing an ecological systems approach, reveals previously unrecognised trends within the literature base. For example, whilst informal support networks are commonly evidenced for unpaid caregivers for people with dementia, it is a relatively novel finding within dementia social care workers. In addition, inclusion of two Patient and Public Involvement (PPI) (CB and PG) throughout all stages of the review increased the strength and quality of the findings in several ways including, increasing the relevance of the review, improving the research design and enhancing any interpretations to findings. This is because two PPI members within the research team provided helpful insights during the data extraction, synthesis, and interpretation stages, helping to synthesise and apply the extracted findings to the integrated ecological systems model, as well as contributing to member checking and the formation of themes, ensuring that the findings were understood and applied appropriately in real-world settings. This adds a unique dimension to the evidence, providing a more nuanced interpretation of the current state of wellbeing in the workforce, offering fresh insights for future research in this evolving field.
However, it is important to acknowledge that limitations of the review were identified, including wellbeing inconsistencies across included evidence. This is because some evidence provided constructs related to wellbeing in the workforce, as opposed to focusing on specific measurements of wellbeing. This is likely because there is no standardised definition and measure for wellbeing in dementia social care workers, highlighting an area for future development. In relation to these inconsistencies, it is important to note that we tried to be as inclusive as possible in terms of our inclusion criteria, including papers which discussed constructs related to wellbeing, as per the included definition, demonstrating a clear strength of the review. This is evidenced by including studies which do not explicitly report wellbeing in workers but rather constructs related to wellbeing such as mental and physical health. Despite this, it should be acknowledged that due to the difficulty of using the concept of wellbeing, potentially relevant papers of the inverse of wellbeing e.g., depression, anxiety, may have been missed. Finally, the included studies had sample populations of homecare workers and residential care workers only, despite our criteria enabling the inclusion of all types of workers, including day care centre and respite care workers. This is likely due to the lack of research within the wellbeing of the workforce, highlighting a gap in the evidence base to be addressed in future research. Some included studies may have involved participants caring for people without dementia; although only dementia-specific findings were extracted, this may reduce result specificity, as experiences cannot always be fully separated from broader caregiving roles.
Conclusions
Dementia social care workers are exposed to multiple systemic factors that can promote and present risks to their wellbeing. Whilst these factors for wellbeing were categorised into the themes: interpersonal, structural, personal attributes and factors generating a systemic sense of value, these factors often overlapped and therefore should not be considered separately. Improving dementia social care, and the wellbeing of its workers, requires systemic changes led by organisations, policymakers, researchers, and healthcare professionals. Organisational structures should seek to improve the risk factors presented to better support worker wellbeing, which may help to improve recruitment and retention rates within the workforce at present. This can be achieved through reducing workload pressures through workforce expansion, particularly at managerial level, and enhanced, dementia-specific training to better equip staff and address the low self-efficacy dementia social care workers are experiencing. In the absence of sufficient funding to reduce such pressures however, organisations should seek to adopt asset-focused approaches that build on workers’ existing resources, such as the informal support networks and training methods highlighted in the current review to be beneficial in protecting staff from the mental and physical health impacts of delivering dementia care. Adopting such methods may help to improve current working conditions and therefore staff retention by promoting staff cohesion, facilitating wellbeing consequently. For the attention of Government policy makers, employment of a National Dementia Strategy is imperative to address the challenges within dementia care and ultimately protect the wellbeing of the workforce. Without such systemic reforms, the wellbeing of the workforce will remain overlooked and the sector in crisis.
Footnotes
Ethical Considerations
Ethical approval was not required due to this being a systematic review of current literature.
Author Contributions
Conceptualization: JGJB, WJD, Resources: JGJB, WJD, Methodology: JGJB, WJD, CG, Software: JGJB, AM, Investigation: JGJB, AM, Data Curation: JGJB, Validation: JGJB, AM, PPI members, Project Administration: JGJB, Visualization: JGJB, WJD, Formal Analysis: JGJB, Supervision: WJD, CG, AJ, PG, Writing – Original Draft: JGJB, Writing – Review and Editing: JGJB, WJD, CG, AJ, PG.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Jessica Grace Jean Bird is a PhD student, funded by the University of Liverpool. Dr Clarissa Giebel is funded by the National Institute for Health and Care Research Applied Research Collaboration North West Coast (ARC NWC).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The views expressed in this publication are those of the authors and not necessarily those of the National Institute for Health and Care Research or the Department of Health and Social Care.