
Abstract
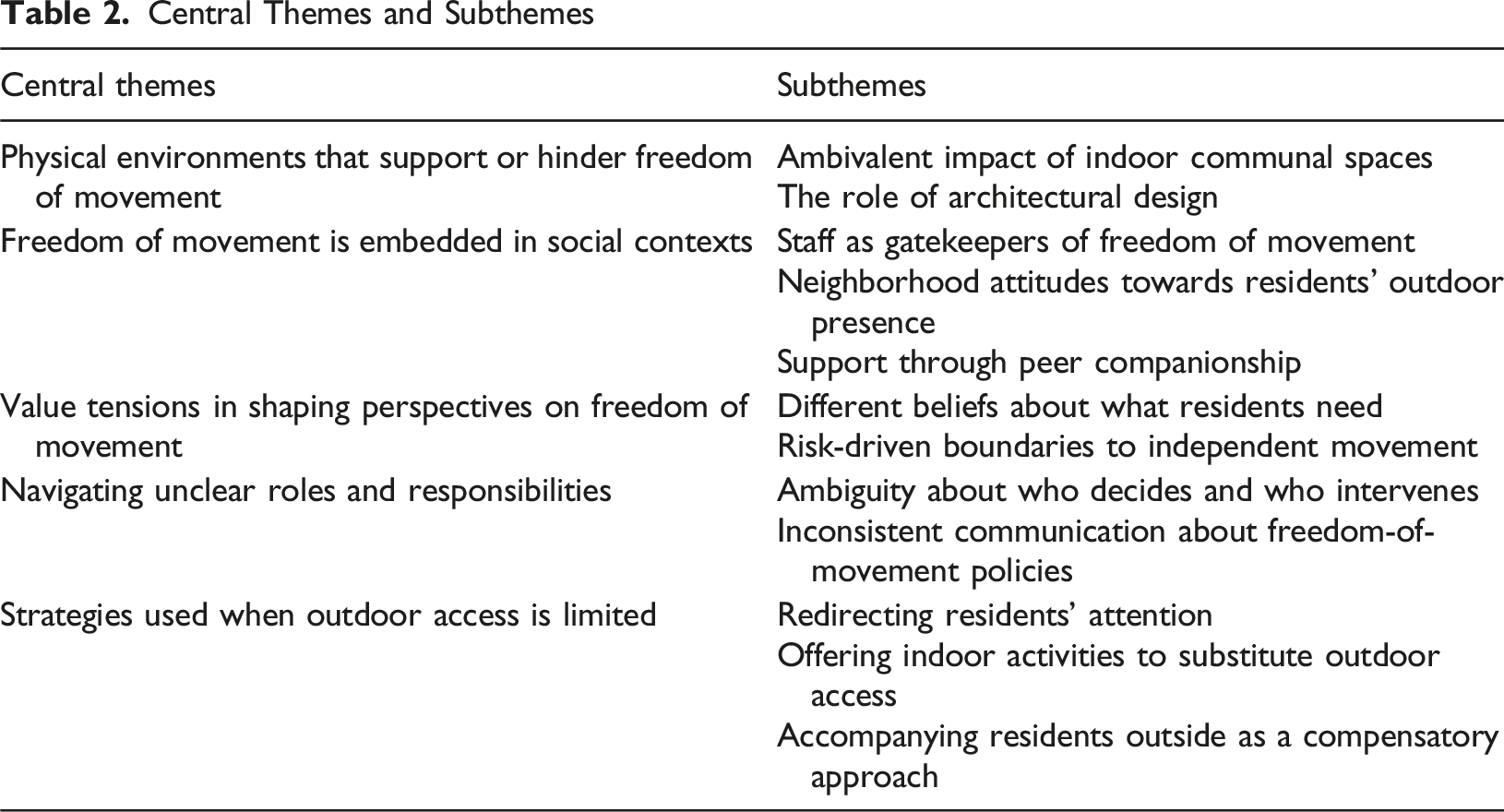
Freedom of movement for people with dementia has received increasing attention in recent years, particularly in nursing homes. Nursing home residents’ families play an important role in supporting their freedom of movement. Therefore, this qualitative study examines how families interpret and experience the freedom of movement of nursing home residents with dementia. Exploratory in-depth interviews were held with 13 family members of nursing home residents living with dementia. Data were analyzed thematically, starting with open coding and iterative refinement of codes. These codes led to the formulation of subthemes, which were clustered into five central themes: physical environments that support or hinder freedom, freedom is embedded in social contexts, value tensions in shaping perspectives on freedom, navigating unclear roles and responsibilities, and strategies for limited outdoor access. These central themes showed how family members interpret and experience freedom of movement in nursing homes for people with dementia. The findings underscore the complex and multifaceted nature of freedom of movement as families see it. Importantly, they suggest that nursing homes should actively involve families in shared decision-making and daily practices that balance freedom and safety to better support the quality of life of residents with dementia.
Introduction
In recent years, freedom of movement for people with dementia has received increasing attention, particularly in nursing homes. This refers to nursing home residents’ ability to move freely within and outside the facility, without being restricted by locked entrance doors (van Liempd et al., 2023). Freedom of movement contributes to nursing home residents’ autonomy because it allows them to choose when, where, and how to move inside and outside the nursing home environment. Autonomy refers to a person’s ability to make choices and influence one’s environment to live a meaningful life, even when facing social, physical, or cognitive limitations (decisional autonomy). Autonomy can be exercised even when individuals rely on support to carry out their decisions (functional autonomy) (Boumans et al., 2022; van Loon et al., 2021).
Research suggests that increased freedom of movement is associated with positive health outcomes, including reduced agitation, enhanced well-being, and improved quality of life (Detweiler et al., 2008; van Liempd et al., 2024; Wigg, 2010). At the same time, it raises safety concerns such as falls, disorientation, and exposure to external hazards like traffic (Niemeijer et al., 2015; Steele et al., 2020). Balancing nursing home residents’ freedom of movement with their safety is therefore complex (Landeweer et al., 2021; Portegijs et al., 2022). Given the potential benefits and risks, decisions regarding freedom of movement require careful consideration and individual tailoring.
Decisions on freedom of movement are often made on behalf of nursing home residents with dementia by both family members and care professionals (van Andel & Holkenborg, 2024). Family members often provide emotional support and practical assistance and participate in care decisions (Puurveen et al., 2018). Moreover, persistent staff shortages in nursing homes have created a need for family members to contribute actively to daily care and support residents’ autonomy, including their freedom of movement (van der Weide et al., 2025). Collaboration between families and care professionals, guided by shared decision-making, mutual trust, and clear communication, is therefore important to support residents’ freedom of movement. However, this can be challenged by the involvement of different perspectives, unclear expectations, and limited time or resources (Paananen & Lindholm, 2023). A collaborative approach ideally facilitates dialogue and decision-making regarding freedom of movement and ensuring that care is coordinated and clearly communicated to all involved.
Some studies have explored how care professionals address the balance between safety and freedom of movement in nursing homes (Evans et al., 2018; Landeweer et al., 2021; Portegijs et al., 2022). However, little is known about how families interpret and experience this aspect. Understanding family members’ perspectives can help align expectations, strengthen shared decision-making, and ensure that residents’ freedom of movement and safety are addressed in a way that best meets their needs. Therefore, this study aimed to describe how family members interpret and experience freedom of movement for residents with dementia living in nursing homes.
Methods
Study Design
This study used a qualitative descriptive design (Sandelowski, 2000) to describe family members’ perspectives on freedom of movement of nursing home residents with dementia. The study was conducted within an interpretivist paradigm (Sithole, 2024), which assumes that reality is socially constructed and context-bound. The report follows the COREQ checklist, ensuring transparency and completeness in the methodological description (Tong et al., 2007).
This study was approved by the Ethics Review Board of Tilburg University (reference RP1447) and by the Research and Science Committee of the participating care organization.
Participants and Setting
This study was conducted in a Dutch nursing home housing 65 residents with dementia. The participating nursing home is a nonprofit, publicly funded long-term care organization located in a southern province of the Netherlands. Open-door policies are often implemented in nursing homes to support freedom of movement for people with dementia (Driessen et al., 2017). The participating nursing home has such a policy, and all residents have freedom of movement within the building and in enclosed outdoor spaces. Wristband-integrated technology enables them to access their apartments independently. They are free to leave the nursing home premises unless an individual assessment determines otherwise, in which case the technology can be configured to keep the exit doors locked. Around the nursing home, a “dementia-friendly walking path” has been created, consisting of tiles adorned with the alpine forget-me-not (Myosotis alpestris). This path serves as both a symbolic and functional element in the outdoor environment. The path is designed to support individuals with dementia in recognizing their surroundings and feeling safe while navigating independently in and outside the nursing home. The first floor of the facility features a large central plaza with a kiosk, various seating areas, and an open space that includes a library and four communal living rooms. The second and third floors consist of apartments for residents, each comprising a separate living area, bedroom, and private bathroom. Residents can use the elevator, which is equipped with grab bars and connects the different floors, allowing them to access their apartments or the shared spaces on the first floor. Apart from the elevator, physical assistive features in the shared spaces were limited. Mobility aids such as grab bars, support poles, or other devices along the walls were not provided.
In this study, family members of nursing home residents with dementia were recruited using mixed purposive sampling (Palinkas et al., 2015) and snowball sampling (Parker et al., 2019). The first author prepared an information letter and consent form outlining the purpose and procedures of the research. These documents were sent via the assistant of the nursing home manager to the residents designated first contact persons, usually partners or adult children who serve as the nursing home’s main point of contact regarding the resident. The first contact person could forward the invitation to other family members if appropriate. Those who expressed interest were then asked to complete and return the consent form. No additional selection criteria were applied, ensuring that all family members who wished to share their perspectives on freedom of movement could participate.
Data Collection
Between October and December 2024, all interviews were conducted by the first author (SvL). SvL received academic training in interview techniques and had prior experience conducting qualitative interviews in similar settings. As a policy advisor for a nursing home organization, SvL is familiar with the long-term care context but independent of the study site and not involved in the care of residents. To enhance rigor and reduce potential bias, the first interview was conducted together with another, independent, researcher with experience in qualitative interviewing (i.e. peer debriefing (Dahal, 2025)). After the first interview, the approach and potential biases were reflected upon. Subsequent interviews were conducted solely by the first author. The assistant of the nursing home manager contacted participating family members by telephone to schedule an interview appointment. The interviews were conducted in a private room located in a building adjacent to the nursing home, ensuring confidentiality and minimal disturbance.
A short introduction was provided to the family members, including a brief explanation of the concept of freedom of movement to ensure a shared understanding. The interview then began with the open question: “What is your perspective on freedom of movement for nursing home residents with dementia?” Probing questions were asked to encourage further elaboration on issues raised by the family members. Toward the end of the interview, a brief set of three sensitizing topics was consulted to check whether they had been covered; If a topic had not emerged naturally during the conversation, we asked the family members to share their perspective on it. Specifically, the three key topics were: (1) freedom of movement and safety, (2) communication between staff and family members, and (3) freedom of movement and overall health. These topics were based on a recent literature review (van Liempd et al., 2023) and additional relevant studies (Høyland, 2024; Landeweer et al., 2021; Portegijs et al., 2022; Puurveen et al., 2018; van Andel & Holkenborg, 2024; van Liempd et al., 2024). Further, the topics were discussed and refined within the author team to ensure their relevance to family members’ perspectives on freedom of movement in nursing homes.
Each interview was scheduled to last approximately 45 minutes. All interviews were audio-recorded, and the audio files were transferred to a secure repository after each interview. Recorded interviews were transcribed verbatim, and audio files were deleted afterwards.
The intended sample size was approximately 12–15 family members, based on evidence that thematic saturation in relatively homogenous interview studies is often reach within the first 12 interviews (Guest et al., 2006). Saturation was monitored throughout data collection and analysis by assessing whether the researchers needed to generate new codes to capture the transcripts’ content. Saturation was assumed when no new codes were needed to label the data.
Analysis
The qualitative data were analyzed using reflexive thematic analysis following Braun and Clarke’s six-phase approach (Braun & Clarke, 2006, 2019). First, the first and second author familiarized themselves with the data by reading interview transcripts. Next, the first and second author independently coded the first two interview transcripts to generate initial codes, after which they compared their coding, discussed discrepancies, and refined the codebook through an iterative dialogue. Both authors used the adapted codebook to independently code two more interviews. Again, they discussed their coding and whether the codebook sufficiently covered the relevant data from the transcripts. After further complementing and fine-tuning the codebook, the first author coded the remaining transcripts. All coding was conducted using ATLAS. ti version 23 to facilitate the organization and analysis of the qualitative data. Codes were subsequently collated into subthemes, which were initially reviewed and refined through discussion between the two authors to ensure they accurately reflected participants’ perspectives. Finally, the subthemes were finalized and central themes were defined collaboratively with all co-authors, who were independent of the study site, providing external perspectives and helping to minimize potential bias (Nowell et al., 2017).
Results
Participants
Family Member’s Characteristics (n = 13)
Central Themes and Subthemes
Physical Environments That Support or Hinder Freedom of Movement
Family members described a variety of ways in which freedom of movement within the nursing home’s physical environment either supported or hindered residents’ use of that freedom. Indoor communal areas played an important role in facilitating spontaneous interactions, yet their impact on both social interactions and freedom of movement was often experienced as ambivalent. Some family members actively used these spaces to create informal meeting points that attracted both residents and other visitors. For instance, they motivated residents to join them in these communal spaces for activities or beverages. These shared moments were seen as valuable opportunities for engagement that emerged naturally during daily routines. We brought cookies or pastries daily, and when someone passed by, they were invited to join for a cup of coffee and a treat. These informal moments often led to spontaneous gatherings, with four or five residents attending the conversation. (Son)
At the same time, some family members observed that indoor communal areas could be overstimulating or confusing for residents, occasionally leading to agitation or withdrawal to their apartments. They reported that difficulties in understanding one another, due to differences in cognitive functioning or communication styles, sometimes led to tensions, friction, or residents withdrawing to their apartments, which could contribute to feelings of loneliness and demotivate them to move around. It’s very overstimulating. What you see is people who don’t understand each other, or they say something, and it’s taken the wrong way. It clashes. (Partner) I think it is unfortunate that there is no common living room on the ward where he lives. In other nursing homes, such spaces do exist, but not here. Because of this, he does not see anyone during the day, as he remains in his apartment. And if he does not want to see people, that is up to him. I also tell him that. But then he says, “Yes, but I feel so lonely.” (Partner)
Large communal spaces, corridors and other interior walking routes were generally viewed as valuable features for residents who needed physical activity or had a strong urge to move. Some family members appreciated how these spaces enabled repetitive walking within a safe, contained environment, illustrating the role of architectural design in shaping movement opportunities. He can walk through all the corridors, not just one ward. He just goes back and forth, left to right, and that’s what he does. (Daughter)
Free access to the enclosed garden and terraces was also considered important. These areas were especially valued when they were directly connected to living rooms or other communal spaces. Family members noted how such designs offered residents a greater sense of space and the opportunity to move around more freely. However, certain architectural features, such as a small garden and the lack of natural elements and circular walking paths, were perceived to restrict resident’s ability to move freely. Every living room leads outside, or you can go through another one. I think that’s fantastic, people have freedom, and it’s outside. I often see residents walking around out there. (Partner) At a minimum, I would prefer the outdoor area to be larger. Ideally, there should be a wider strip, or even a pathway encircling the entire premises, so that residents can truly walk around. Alternatively, a somewhat larger area with some trees or planting would also give the impression of walking more freely. I believe this would make going outside much easier than having residents walk on the street. To what extent they would actually do so is uncertain, but I think the urge to go out onto the street would be less strong if such an outdoor space were available. (Partner)
According to some family members, the dementia-friendly walking path extended the nursing home into the outdoor environment, potentially offering residents a safe and accessible way to move beyond the building and the enclosed garden. While the visual cues along the path were considered a positive feature, some participants observed that not all residents understood or remembered their intended function. As a result, the cues did not always support independent wayfinding as intended, which may have limited residents’ autonomous use of the environment. It’s lovely, every time we walk there, we say, “Follow the flowers and you’ll find the door.” And every time my father says, “Beautiful, those flowers,” but he doesn’t understand the concept. (Daughter)
Freedom of Movement Is Embedded in Social Contexts
Family members described how freedom of movement was shaped not only by the physical environment, but also by the social and relational context of the nursing home. In particular, staff attitudes and actions, interactions with the surrounding neighborhood, and the presence of peer relationships were considered to influence whether and how residents moved beyond the immediate living areas. Several family members emphasized the role of staff as key facilitators or, at times, as gatekeepers of residents’ freedom of movement. Their encouragement or lack thereof could make a difference in whether residents felt supported to move within or outside the nursing home. Some family members suggested that motivating residents to go out requires a personalized approach, for instance, by linking outdoor activities to familiar places or routines. Encouragement from staff is important. I think if others could take him along, some people go cycling, if you told my father to go cycling, he’d say “pff.” But if you mentioned familiar places, I think he’d go. (Daughter)
Family members also noted that neighborhood attitudes towards residents could hinder residents’ freedom of movement, as their presence in public was not always understood or accepted. Concerns among community members sometimes led to tensions, especially when residents’ outdoor presence was perceived as unusual or unsafe. Family members became aware of such perceptions either when picking up a resident who needed assistance to return or when being called by neighbors who had seen a resident walking outside the nursing home grounds. Such attitudes were experienced by families as discouraging and added a layer of social friction to the issue of outdoor mobility. People in the neighborhood thought it was ridiculous that someone was still allowed to walk outside if they had to be picked up. It became more and more unpleasant. (Daughter)
Support through peer companionship was mentioned as another way in which the social context shaped residents’ freedom of movement. For instance, family members described a “buddy system,” in which residents could support fellow residents who were hesitant to go outside alone. Walking or spending time outdoors together was seen as a practical way to reduce anxiety, boost confidence, and provide mutual support. I think it would help if a fellow resident could be found to go on the adventure together. Like a buddy system. That would be great for her. Then I could imagine her going beyond the forget-me-not path. (Daughter)
Value Tensions in Shaping Perspectives on Freedom
Family members held different perspectives about residents’ opportunities to go outside independently. While participants widely recognized the value of freedom of movement, their perspectives reflected different beliefs about what residents need. Some participants had chosen this specific nursing home because it offered freedom to go outside, which they believed was what the resident desired. They emphasized the importance of outdoor access for maintaining residents’ emotional well-being and continuity of old habits. For these family members, the opportunity to go outside was seen as contributing to the residents’ health and quality of life. I think he’s happier when he can go out or do something, rather than sitting inside all day. That’s what my father was used to. Sitting inside all day makes him unhappy. So, we were really glad that he could go outside. (Daughter)
Others emphasized, however, that going outdoors was not an option, either due to safety concerns or residents’ lack of interest. Their relatives had little or no desire to go outside independently, suggesting that for some residents, the need for freedom of movement in this domain had diminished or was no longer a priority. I don’t see my husband doing that; he has no desire. I don’t think he’d ever go outside on his own. (Partner)
Participants also talked about boundaries to independent movement, that were often based on their estimation of risks. Some family members described making a conscious decision to prioritize freedom of movement within boundaries that felt safe. For example, they mentioned a Global Positioning System (GPS) tracking device to allow residents to go for walks independently in the neighborhood while their whereabouts could be monitored. They acknowledged the importance of preserving a sense of agency and familiarity, especially for a resident with dementia living in a nursing home. It was important to us that if he had to move, he would still have freedom of movement, as long as it was safe for him. (Daughter)
At the same time, safety concerns were a recurring issue. Several family members expressed discomfort or anxiety about residents being outside unsupervised, especially given the cognitive challenges associated with dementia. The unpredictability of the outside world was perceived as a potential source of hazards. Consequently, family members sometimes described restrictions on freedom of movement as necessary, often based on assumed risks of disorientation or imagined accidents. Even when residents were physically capable of going outside, the possibility of becoming lost or distressed was seen as justifying restrictions on their freedom of movement. There are so many risks. These people just don’t know anymore. You’re not here for nothing; otherwise, you could’ve stayed at home. (Son) For his safety, it’s no longer good. He could walk the distance and return, but once he’s there and it doesn’t match what’s in his head, he gets confused, starts wandering, and gets lost. (Daughter)
Navigating Unclear Roles and Responsibilities
Family members described challenges in communicating with staff regarding residents’ freedom of movement, particularly related to ambiguity about who decides and who intervenes and inconsistent communication about freedom of movement policies. Several participants indicated that decisions about outdoor access were not explicitly discussed with them. While notes might have been recorded in formal care plans or digital client records, this information was not always shared in conversations between staff and family. We never had a conversation about it. It’s in the report in the client record, but we never discussed it separately. (Daughter)
This lack of dialogue sometimes created uncertainty about the family’s role in supporting outdoor mobility. In some cases, family members were unaware that residents could go outside, for example, with track-and-trace technology. When asked about their possible role in facilitating such outings, such as assisting with bringing residents back, differing perspectives came forth. Primarily, children of residents expressed reservations, emphasizing that this would be difficult to combine with other responsibilities. Partners were more likely to perceive a role for themselves in assisting with returning residents. That’s difficult, we are both working. You can’t just leave work during the day to pick up a parent. (Daughter) I believe it is unreasonable to expect this as a standard responsibility of healthcare providers. They are already doing a great deal at the local level, and it would be unrealistic to assume that such efforts can be extended further afield. (Partner)
Ambiguity about which residents were allowed to go outside and under what circumstances also created uncertainty about how to respond appropriately. Some participants described situations in which they intervened out of concern, such as when they saw a fellow resident standing by the door. These situations could sometimes lead to tension or conflict among those involved. I once got punched in the stomach by a resident when I said, “Sir, maybe you should go that way.” He didn’t like that. (Partner)
Unclear organizational policies further contributed to some families’ uncertainty about the extent to which residents were free to move independently. Families described inconsistencies between what they were told, for example, that the nursing home had an open-door policy, and what they observed in daily practice. What’s unclear to me is that they say it’s an open-door policy, but the doors aren’t open. Are there residents who can go outside? Because it seems the opposite, the door is always closed. (Partner)
Strategies Used When Outdoor Access Is Limited
When residents were not permitted to go outside on their own, some family members expressed that alternatives were needed to help manage their relative’s restlessness, need for movement, or desire for stimulation. The strategies and resources available within the nursing home to meet these needs were seen as important in supporting residents’ well-being. One common approach family members mentioned was to distract residents and redirect their attention when they expressed a desire to go outside. For instance, they redirected their attention to a meal, activity, or comforting topic, which was sometimes effective, though it did not always work. Some family members noted that this approach could lead to frustration when the underlying need remained unaddressed. I’d say, “First have a nice meal, and then we’ll see.” That’s a distraction. But it doesn’t always work. Sometimes he gets angry; he wants to go to a nearby town. You can’t say, “That’s not possible.” That doesn’t work. You have to sugarcoat it. (Partner)
When outdoor access was impossible, the availability of meaningful indoor activities as a substitution became particularly important. While some family members were satisfied with the activities offered, others expressed concerns about a lack of organized engagement or stimulating interaction within the nursing home. They saw that residents often spent extended periods sitting without active involvement or stimulation. I really miss the activity coordinators. Those people [the residents] just sit there. That’s not movement. (Partner)
To help meet the need for movement and stimulation, some family members took an active role by accompanying residents and facilitating outdoor experiences during their visits. Going for walks together was seen as beneficial not only for physical health, but also to provide a sense of satisfaction that could reduce restlessness later in the day. Still, these efforts were not always sufficient to meet residents’ ongoing needs. When I’m there with my sister, we always take a long walk. We try to make sure our father feels he’s been outside enough, so he’s not tempted to go again. But it doesn’t always work. (Daughter)
Discussion
This study described how family members interpret and experience the freedom of movement of nursing home residents with dementia. Findings point to diverse interacting aspects that shape family members’ perspectives, including environmental features, social and relational dynamics, value considerations and practical strategies. Initially, all participants expressed broad support for the principle of freedom of movement. This aligns with previous research, which suggested that, from family members’ perspective, the ability to move freely meets residents’ physical activity needs and contributes to their autonomy, as residents can choose where to go without feeling restricted (Hoek et al., 2019). However, participants in the current study quickly shifted to considering the specific situation of their own relative, often resulting in more cautious or nuanced views. This shows the existence of multiple, sometimes inconsistent, perspectives on the value and implications of residents’ freedom of movement. Previous research has emphasized that the physical environment of nursing homes, including factors such as spatial layout, plays an important role in fostering residents’ freedom of movement while also shaping the extent and nature of informal care by influencing family members’ opportunities, roles, and interactions (Chaudhury et al., 2017; Holmgren, 2017). Consistent with Holmgren (2017), our results suggest that residents’ freedom of movement within indoor communal areas enables family members to create informal meeting points, fostering social interaction and supporting informal caregiving interactions. Further, family members perceived the nursing home’s physical environment as both enabling and constraining residents’ freedom of movement. Large communal spaces, walking routes, and enclosed outdoor areas can promote residents’ freedom of movement and facilitate social connections. At the same time, the same features could limit the practical ability to move freely or to make choices about movement. Overstimulating environments sometimes led residents to retreat to their rooms. Moreover, the absence of a continuous walking circuit meant that they frequently encountered closed doors, reducing their sense of freedom in movement. This reflects broader design challenges described in the literature, namely achieving a balance between overstimulation and sensory deprivation, while providing varied environments that foster choice and freedom of movement (Siegelaar et al., 2025). Family members valued free access to enclosed gardens and terraces, especially when directly connected to living or communal spaces, as these enhanced residents’ sense of space and freedom. Some noted, however, that small size, limited natural elements, or a lack of circular paths could restrict movement and the feeling of freedom. These findings align with previous research on dementia-friendly outdoor environments, which has shown that well-designed gardens can support autonomy, engagement, and well-being (Høyland, 2024; Motealleh et al., 2022; van den Berg et al., 2019). In addition, some family members emphasized the importance of outdoor spaces beyond the nursing home grounds, including dementia-friendly walking paths. They perceived that such accessible routes could further support residents’ mobility, outdoor activity, and independence. This view aligns with recent research indicating that certain environmental features, such as connected and well-maintained walking paths, safe crossings, and nearby green spaces, can encourage more frequent and prolonged outdoor walking among individuals with dementia (Nouri & Chaudhury, 2025).
Reflections on the physical environment, both within and beyond the nursing home grounds, also revealed differences in how family members weighed safety against freedom of movement. Some family members prioritized safety, preferring their relatives to remain behind locked doors to avoid potential dangers outside, while freedom of movement was considered less important. Others emphasized the value of freedom of movement over safety, especially when this had been important to their relatives in the past. This suggests that while freedom of movement is generally valued, its practical application for individual residents is closely tied to tailored assessments of safety, autonomy, freedom, and personal context. Recent research has emphasized that freedom of movement and safety are not mutually exclusive but require a careful balance in day-to-day decision-making (van der Weide et al., 2025).
Our findings suggest that dialogue between family members and care staff is not always present, which leaves some family members unaware of residents’ options and potential trade-offs. Consequently, their views on freedom of movement may be based on individual assumptions or limited knowledge. Boumans et al. (2022) argued that freedom of movement and safety should be negotiated through dialogue and collaboration among family members, care staff, and, ideally, residents themselves, to support residents’ autonomy without compromising safety. Shared decision-making is essential not only for aligning perspectives on freedom of movement and safety but also for establishing practical agreements. For example, shared decision-making helps determine who is responsible for escorting a resident with dementia back inside when they are outdoors. This aligns with the findings of Hovenga et al. (2024), who suggested that family members and nursing home staff should initiate dialogue more actively to clarify and evaluate the division of roles and responsibilities, including regarding freedom of movement. At the same time, care staff operate within organizational contexts characterized by time constraints, staff shortages, and responsibility for residents’ safety (Miller et al., 2026). These conditions may limit opportunities for sustained dialogue and contribute to implicit assumptions on both sides about freedom of movement, risk, and responsibility. Similar tensions between families and staff have been described in previous research, particularly in long-term care settings where safety and freedom of movement must be continuously negotiated (Hovenga et al., 2024; van der Weide et al., 2025). Although current findings mostly align with previous research, this study adds nuance by examining family members’ perspectives in a nursing home where an open-door policy has been implemented in everyday practice. This provides insights that have not been captured in previous studies. The results describe how family members interpret freedom of movement within a context shaped by organizational arrangements, practical constraints such as staffing and supervision possibilities, and communication with care staff. They suggest that family members’ views are influenced not only by values related to safety and freedom, but also by their understanding of what is practically feasible and how roles and responsibilities are experienced in daily care. The COVID-19 pandemic further emphasized the importance of family involvement in nursing home care. Periods of restricted access limited family members’ presence and participation in everyday care and decision-making, exacerbating challenges in collaboration between families and staff. Previous studies have shown that reduced family involvement during the pandemic negatively affected residents’ quality of life and contributed to emotional distress among family members (Cousins et al., 2022; van Corven et al., 2022; Verbeek et al., 2020). These findings reinforce the view that family members should be positioned as partners in supporting residents’ freedom of movement, rather than as external or supplementary actors.
When residents’ outdoor access was limited, family members sought alternative ways to address restlessness and the need for movement and stimulation. While strategies such as distraction or indoor activities were sometimes used, they were not always effective. To overcome these challenges, many participants facilitated outdoor experiences, such as neighborhood walks. This aligns with findings by Ciofi et al. (2022), who observed that such facilitated walks are particularly valuable for residents who are not permitted to go outside independently. Facilitated walks not only provide sensory and physical stimulation but may also reduce residents’ tendency to go outside on their own. While some residents were not allowed to go outside independently, others were allowed to do so but appeared uncertain or hesitant to venture out alone. Based on family members’ perspectives in this study, pairing residents for outdoor walks may help residents feel more confident when going outside together. The dementia-friendly path could also support confidence by providing an environment with recognizable landmarks. The value of using landmarks for spatial navigation was also emphasized by participants with dementia in the study of Chaudhury et al. (2025). In addition to strategies mentioned by family members in this study, previous research indicates that trained volunteers can facilitate participation in outdoor activities and social engagement, enhancing residents’ freedom of movement while helping to reduce staff workload (Van der Ploeg et al., 2014; Weissbach et al., 2023).
Limitations
This study was conducted in a nursing home with an implemented open-door policy, allowing residents to freely go outdoors, except when an individual assessment indicated a risk of serious harm. This study’s setting was a larger-scale residential care facility for residents with dementia, which may limit the transferability of the findings to more typical, smaller-scale units. To support interpretation of the findings, we describe the care setting, our recruitment and sampling approach, and provide the basic demographic and relational information of participating family members. This information may also enable readers to consider how the findings may relate to other contexts. Another limitation is that direct information on residents’ levels of autonomy, independence, physical abilities, and cognitive status was not collected and therefore could not be included in the analysis. This study focused on describing family members’ perspectives, rather than examining how these perspectives may differ in relation to resident characteristics. Nonetheless, such characteristics may shape how family members perceive and interpret residents’ freedom of movement, potentially influencing their experiences and concerns regarding outdoor access and safety. Furthermore, family members’ gender and type of relationship were collected and reported descriptively to contextualize the sample; however, their potential contribution to perceptions of freedom of movement was not analyzed. Although gender and family roles may influence perceptions, involvement, and family relationships, exploring their potential influence was beyond the focus of the current study. Given these limitations, future research could systematically examine how differences in residents’ characteristics affect family members’ perspectives, and how gender and family roles may shape experiences and views on freedom of movement in nursing homes.
Implications for Practice
Based on this study’s findings, structured dialogue and shared decision-making involving family members may help clarify residents’ needs and possibilities, as well as the respective responsibilities of staff and families in supporting residents’ freedom of movement. Dialogue between staff and family may help to ensure that freedom of movement is supported in everyday practice. Such dialogue may help align expectations, address concerns about safety and responsibility, and support collaborative decision-making that reflects residents’ values and the variety in how they experience freedom and safety (van Andel & Holkenborg, 2024). Accessible and engaging environments, such as living areas with direct connections to enclosed outdoor spaces and a dementia-friendly neighborhood, may enhance the freedom of movement of residents with dementia. When outdoor access is limited, family members noted that meaningful alternatives, such as personalized indoor activities or accompanied structured walks, can help meet residents’ movement and stimulation needs.
Conclusion
Freedom of movement in nursing homes is multifaceted and subject to varying interpretations among and within family members. Advancing freedom of movement in nursing home requires open dialogue and collaboration between staff, residents, and their families, as well as consideration of environmental and practical elements within and surrounding nursing homes.
Footnotes
Acknowledgements
This research was conducted at the Academic Collaborative Center (ACC) Older Adults of Tranzo, Tilburg University. This is a structural and equivalent partnership between Tilburg University and 11 organizations in the field of long-term care for older adults: Avoord, Azora, Brabantzorg, CZ Zorgkantoor, De Wever, Groenhuysen, Mijzo, Surplus, SVRZ, TanteLouise, and Thebe. Scientific research within the ACC is conducted through cocreation with older adults, family caregivers, and/or care professionals and in accordance with the guiding principles of scientific integrity. We thank all older adults, family caregivers, and care professionals for their valuable contributions to this study.
Ethical Considerations
This study was approved by the Ethics Review Board of Tilburg University (reference RP1447) on 15/08/2024.
Consent to Participate
All participants provided written informed consent prior to enrolment in the study.
Consent to Publication
All data are anonymized and non-identifiable; general informed consent for participation, including use of anonymized data for publication, was obtained from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset is not publicly available due to the sensitive nature of the data. All data are securely stored in a controlled digital environment, accessible only to the first and second authors, in accordance with established data handling and reporting guidelines.