
Abstract
People with dementia can live alone successfully even when they do not have support from family or friends. This requires professionals to be able to provide timely and effective support. This study aims to identify professional perspectives on the challenges and strategies in supporting people with dementia who live alone and have no informal support. Semi-structured qualitative interviews were conducted with twenty-two professionals working in dementia-related roles across various sectors in England. Interviews were analysed using Reflexive Thematic Analysis. Themes were finalised through support of the study advisory team, including people with lived experience of dementia. Six themes were identified, reflecting stages of the ‘dementia care pathway’, from identification of patients to discharge. Professionals reported experiencing barriers around identifying clients, communicating with them, gathering information, engaging with them, managing risks, and setting up continuity of care. They shared strategies for each of these challenges. This study identified some key strategies that a variety of professionals can deploy to promote access and use of services for an especially vulnerable population to be able to live independently for as long as possible. These strategies would need to be embedded and consistently implemented across different sectors. This would ensure that people are identified and supported in a timely fashion and could, in turn, prevent more costly long-term care and contribute to cost-containment.
Introduction
Most people who live with dementia have someone to provide unpaid help or informal caregiving (DoH, 2016). Informal and unpaid care provided by family members and friends/neighbours is the most common type of dementia care worldwide (Rosenwohl-Mack et al., 2021). Other than undertaking a wide range of caring duties in the home and promoting social wellbeing (Duane et al., 2013; Newhouse et al., 2001), informal caregivers are critical to navigating and arranging support from health and social care services, particularly as dementia progresses.
Reflecting this, in the United Kingdom, much of the evidence about good commissioning and practice in dementia support is based on the assumption that people with dementia have an informal caregiver (NICE, 2018). However, not every person with dementia has a regular informal caregiver (Newhouse et al., 2001), and even if they do, the person with dementia might be hesitant or reluctant to seek support (Heaton et al., 2021) or their networks may be unwilling or unable to help with care decisions (Samsi & Manthorpe, 2013). While it is difficult to establish the exact prevalence, approximately 40% of people with dementia who live in the community in the United Kingdom live alone (Clare et al., 2025) and as many as 1 in 10 of these have little or no informal support (Clare et al., 2025). With increasing numbers of people living alone and ageing without children, the number of people with no informal caregiver will continue to grow (Michalowsky et al., 2018).
Living independently is a priority for many people with dementia (Quince, 2011), and current policy promotes supporting people to live independently in the community for as long as possible (HM Government, 2014). Support can be provided by a range of services including social care, social prescribing, occupational therapy, and third sector organisations. It spans a wide range of activities including personal care, home care or domiciliary care, support in day centres, reablement services to help people regain independence, social opportunities, the provision of aids and adaptations for people’s homes, and information and advice (The King’s Fund, 2025).
A recent research project, ‘Improving support for those living alone with dementia without informal caregivers’ (LAWD) (Aspinal et al., 2023), found that people with dementia who live alone and do not have informal caregivers want to maintain independence and decisional autonomy for as long as possible. However, the symptoms associated with dementia, such as increased anxiety, memory difficulties and fluctuating/reducing problem-solving abilities, can mean that finding out about, accessing, using and changing support services as their condition dictates can be particularly difficult, as evidenced in a systematic review on service use by people living alone with cognitive impairment (Rosenwhol-Mack et al., 2021). Falling through service gaps potentially exposes them to precarious care situations (Illiger et al., 2021) and worse health outcomes (Aldridge et al., 2020). Instead, through support to make initial contact and continued use of support services, these people could stay independent and remain at home for longer.
So far, research has provided key evidence of the needs of people living with dementia from their own experience and documented health and service use gaps in this population. However, substantial evidence is lacking about how this type of support happens in practice from the perspective of support providers, i.e., the professionals. This information is key to generate evidence that is grounded in real-life professional scenarios on the practicalities, challenges and strategies in supporting clients with dementia who live alone.
This study aims to bridge this evidence gap by offering professional perspectives around the unique challenges and effective strategies in supporting this population. The evidence will be useful for a range of professionals to provide better support to their clients.
Methods
Design
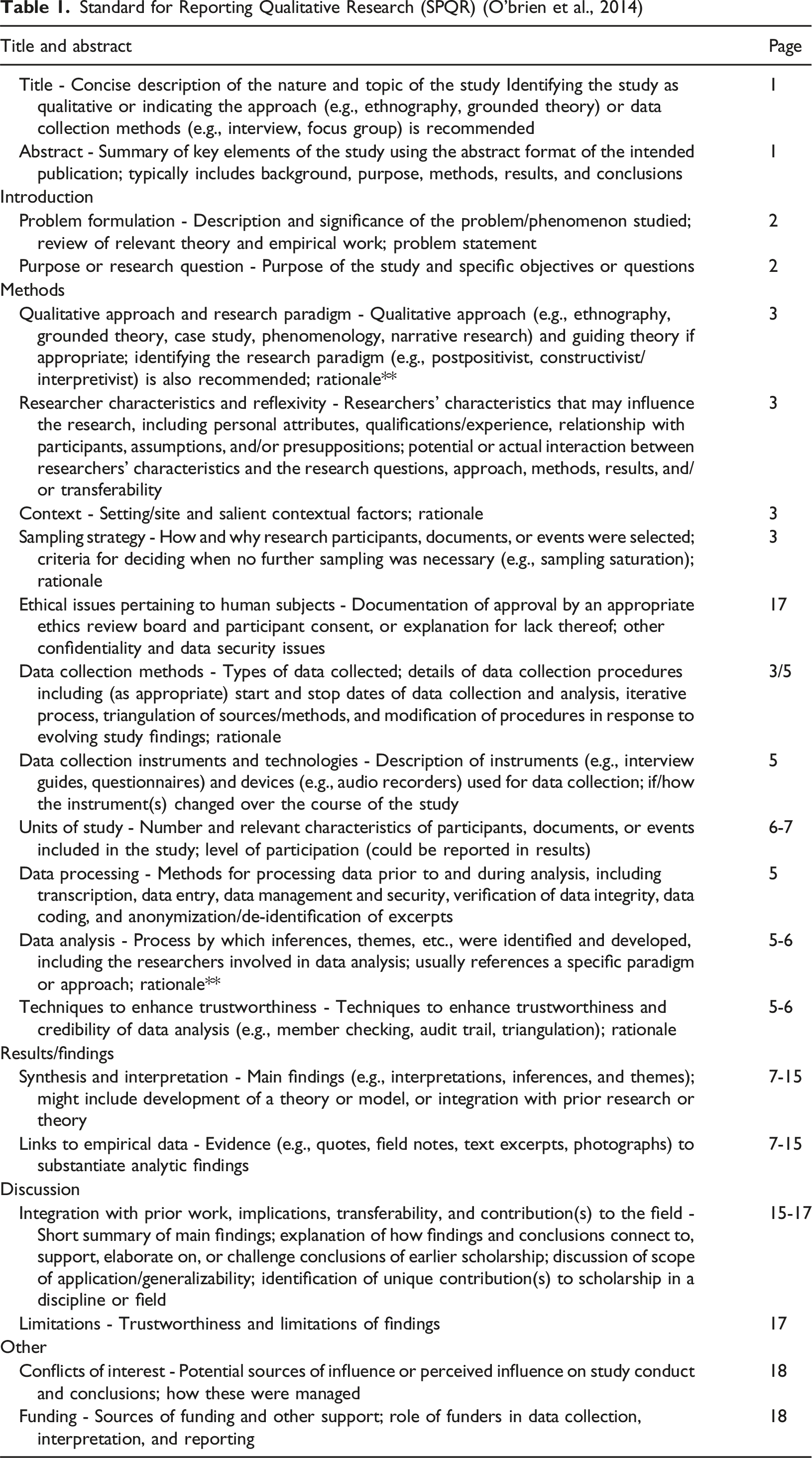
Standard for Reporting Qualitative Research (SPQR) (O’brien et al., 2014)
Sample
The sample included professionals: • working in any sector (e.g., voluntary, statutory, private sectors) in England • working in any professional role (e.g., social prescribers, social care workers, admiral nurses, staff in voluntary sector organisations) • supporting people with dementia who live alone and do not have informal support to access and use social care services • aged 18 or over, based in England, able to give consent and take part in an interview in English.
Recruitment
Potential participants were identified through the study team’s network across England including social care services, social prescribing services, primary care networks, local authorities and the private and voluntary sectors.
Because the study team’s networks were used, participants were recruited through snowball sampling. In line with principles of Research Inclusion by the National Institute for Health and social care Research (NIHR), we aimed to include in the study representation of different genders, ethnicities and localities. This was important to ensure that views and experiences reflected the diversity in the community of professionals supporting people living with dementia. Therefore, to make the study sample diverse, participants’ socio-demographic characteristics were monitored as recruitment progressed, and new participants were involved in the study purposefully if their characteristics had been underrepresented thus far. It was anticipated that up to 25 professionals would provide sufficiently diverse, rich, complex and multi-faceted data. However, an in-situ decision was made about the final sample size, based on consistent monitoring of data sufficiency (richness, complexity) (Braun & Clarke, 2019).
Data Collection
Consent was obtained from participants before the interview commenced. It was gathered in paper or electronic forms depending on participants’ preference. A demographic questionnaire was also sent to participants and collected before the interview. A time/date for the interview was agreed.
Interviews were conducted remotely via Microsoft Teams to maximise geographical reach and to accommodate participants’ work and personal commitments. The interviews were all conducted by the first author (CDL), a qualitative researcher with expertise in dementia research. They were recorded on Microsoft Teams.
Materials
The interviews were guided by a topic guide (Appendix) informed by the scoping review and developed with support from a study advisory group. The group comprised two Patient and Public Involvement (PPI) collaborators with dementia living alone and with no informal support from underserved communities: Black British, and Lesbian, Gay, Bisexual, Transgender, Question/Queer and other sexually minoritised groups (LGBTQ+). It also included two researchers who conducted previous work in this area, one social worker working and a commissioner of Adult Social Care services working respectively in two Local Authorities in England. The topic guides were used flexibly to accommodate exploration of unanticipated relevant topics.
Data Analysis
Analysis of interviews started after the first interview was complete and was an ongoing process, informing subsequent interviews (e.g., identifying emerging relevant topics). Interview transcripts generated by Microsoft Teams were proofread/corrected, fully anonymised by the first author (CDL), and assigned participants unidentifiable codes, i.e., P01, P02.
Interviews were analysed using Reflexive Thematic Analysis (Braun et al., 2023). As such, emerging common patterns were generated from the transcripts and coded into preliminary themes. During weekly meetings with the study team, the preliminary themes were discussed. This was an iterative process that continued throughout the coding of transcripts. New themes were created as they were identified during analysis, and existing themes were edited, merged, collapsed or discarded. The research team convened with the advisory team to reach consensus on final themes (e.g., relevance, exhaustiveness).
Results
Participants’ Characteristics
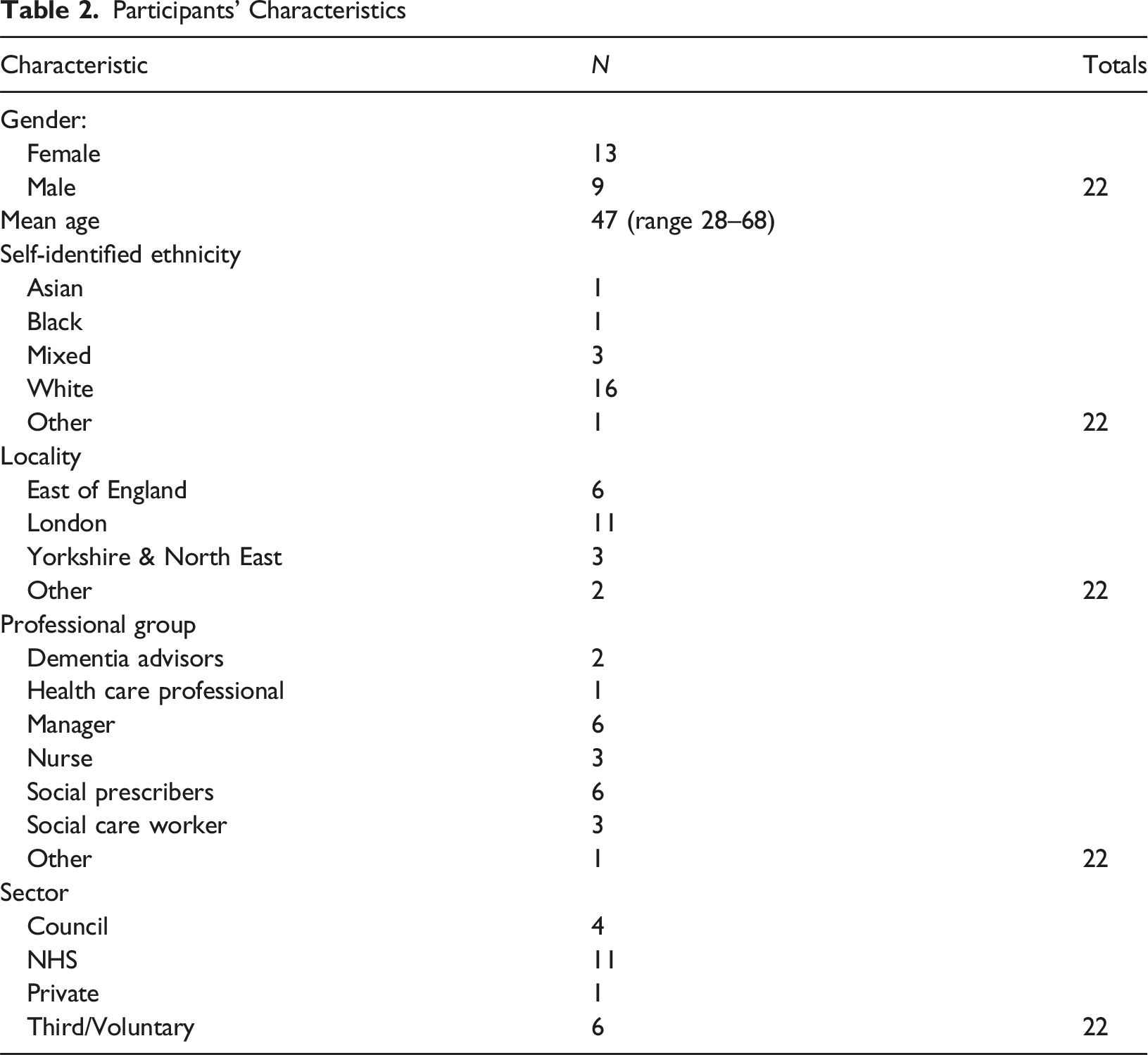
Participants had a diverse range of professional roles, including Social Prescribers (n = 6), Dementia Advisers (n = 2), Nurses (Specialists (Dementia and Delirium, Admiral Nurse and Dementia Care Lead) (n = 3), Managerial or Leadership Roles (e.g. Head of Operations, Programme Lead, Service Manager, Project Manager) (n = 6), Social Care Workers (n = 3), and Other Specialist Roles (e.g., Occupational Therapist, Clinical Research Practitioner, Health and Wellbeing Manager) (n = 2). Professionals were employed in the National Health Service (NHS) (n = 11), the Third Sector (n = 6), Councils (n = 4), and the Private Sector (n = 1).
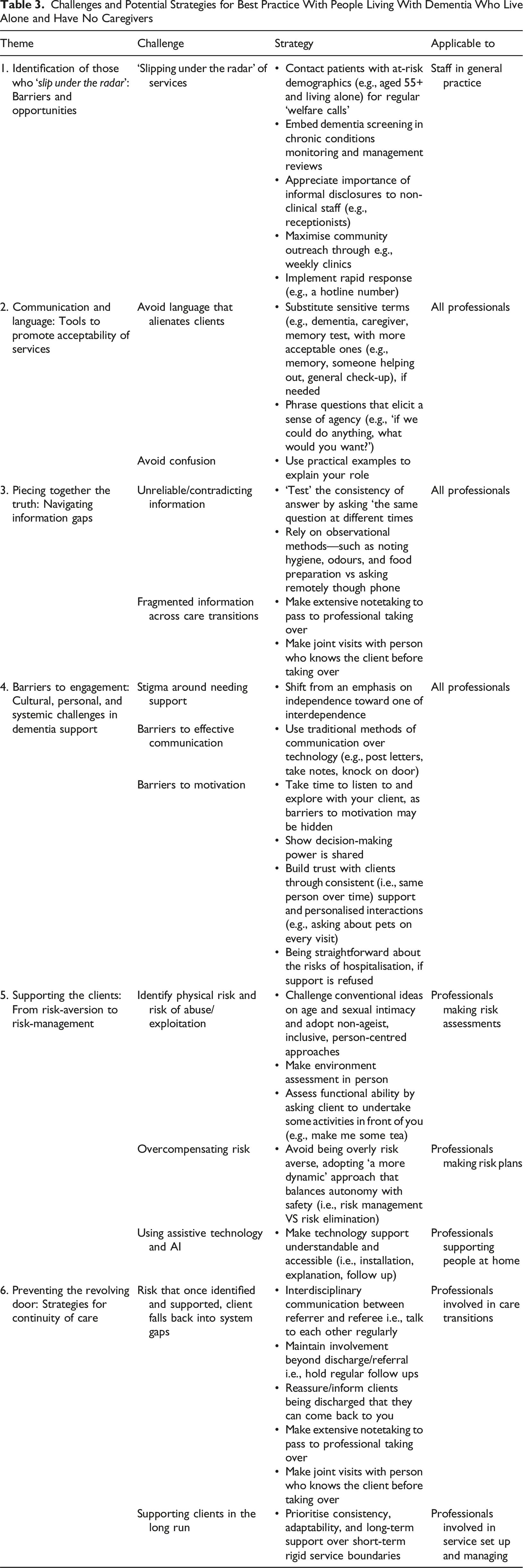
Interviews lasted an average of 45 minutes. All participants completed the interview in one session. Six themes were identified, which are reported below in chronological order, reflecting stages of the ‘dementia care pathway’, from identification of patients to post-discharge continuation of care (Figure 1). The challenges and strategies are summarised in Table 3. Themes identified, mapped out on the ‘dementia care pathway’ Challenges and Potential Strategies for Best Practice With People Living With Dementia Who Live Alone and Have No Caregivers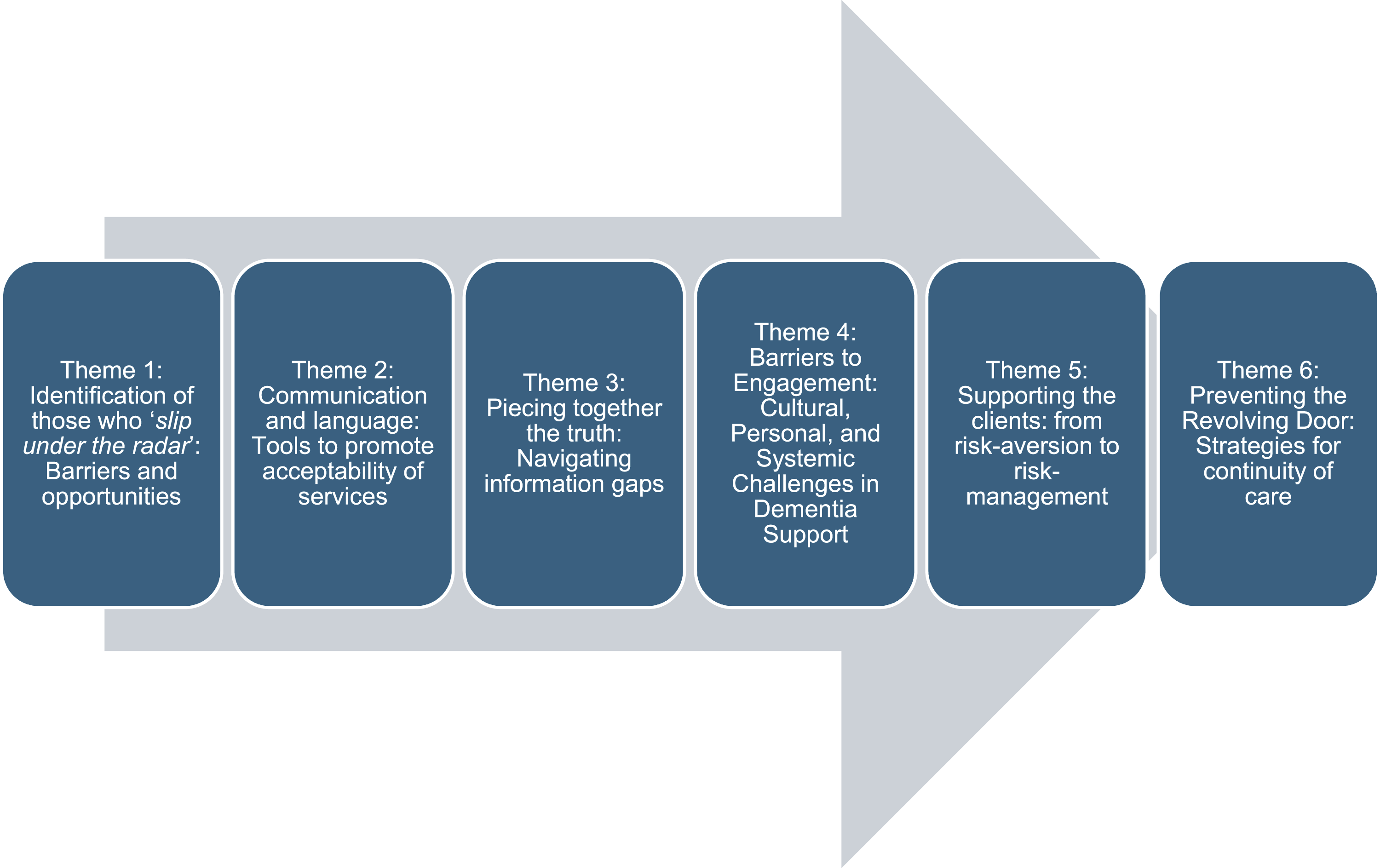
Identification of Those Who ‘Slip Under the Radar’: Barriers and Opportunities
The phenomenon of people with dementia who live alone and have no informal support who ‘slip under the radar’ of services involves a complex interplay of stigma, systemic gaps in service integration, and limitations in consent-based social care frameworks. Participants discussed current issues and potential strategies.
Limited face-to-face patient interactions do not place professionals in a position to identify the early signs of dementia that a patient exhibits. A professional suggested that ‘on the telephone they could talk, but you wouldn't know how they are’ (P03; Dementia Adviser).
As a result, many people with dementia who live alone and have no informal support are only identified following serious incidents. In some cases, police involvement triggers referral: ‘Patients who are found wandering are picked up by police and then brought to hospital… that could be enough to trigger a concern’ (P08; Dementia and Delirium Clinical Nurse Specialist). One professional reported that only when ‘There’s a crisis and they come to hospital…then we would look at…completing a social care assessment’ (P07; Social Care Worker).
In the absence of informal caregivers, often facilitating timely diagnosis of dementia, some strategies were proposed to identify those who might need support in a timely fashion.. While these strategies are applicable across the board of all living with dementia, they were found to be especially important in this group. A proactive approach whereby services contact patients aged 55+ and living alone and initiate ‘welfare calls’ with targeted questions that may ‘bring out the possibility that there’s some dementia going on’ (P15; Social Prescriber). Regular follow-ups with these patients should be made to ‘check in every six months or once a year just to see how they’re doing’ (P17; Social Prescriber).
Chronic conditions monitoring and management also present opportunities for the identification of dementia in people living alone. ‘We know that there are risk factors about long term conditions for dementia, like diabetes. So, when people access annual health reviews for diabetes, for example, we could identify people who start to look like they might need some services for dementia as well’ (P06; Dementia Programme Lead).
All staff working in services or organisations, such as receptionists and volunteers, also play a key role in helping timely identification and referral of people with dementia who live alone. Participants reported how through informal disclosures to staff—e.g., ‘I’ve got dementia’— people have been able to bypass traditional systems of identification (e.g., clinical appointments) and get timely support’ (P20; Social Prescriber).
Maximising outreach of services into community settings is also key in a population who is so hesitant and unable to seek support. One participant stated a need to deploy outreach community-based care navigators or ‘at least a system where people’s vulnerabilities are flagged up’ (P08; Dementia and Delirium Clinical Nurse Specialist).
In conclusion, the insights provided by participants underscore both the limitations and the untapped potential of services in promoting identification of those with dementia who live alone without informal support. At present, this particularly vulnerable group often remains invisible until crisis.
Communication and Language: Tools to Promote Acceptability of Services
Communication and language are essential tools in dementia care, serving not only as conduits for information but also as mechanisms for emotional safety, trust-building, and behavioural engagement. This is particularly helpful with people with dementia who have no informal caregivers who would typically act as facilitators in communication between professionals and the person with dementia.
Professionals recognise that ‘most of the time, [patients] kind of know they have dementia, but they deny that because it's just too much for them to cope’ (P01; Dementia Adviser). Consequently, they tend to adapt their language. Terms like ‘dementia’ are sometimes avoided in favour of less sensitive alternatives (e.g., memory issues), with professionals trying to ‘use their language to meet people where they are’ (P01; Dementia Adviser).
The same applies in clinical settings, where professionals often rephrase more sensitive terms like ‘dementia review’ or ‘memory assessment’ into the more generic ‘general check-up’, or as a professional suggested ‘a bit of an MOT [Used metaphorically - UK vehicle test]’ (P08; Dementia and Delirium Clinical Nurse Specialist), to increase engagement. Rephrasing can be an effective strategy to overcome resistance in clients. One professional reported how the question: ‘would you be happy for somebody to come and help you with your medication in the morning?’ (P14; Clinical Research Practitioner) proved more acceptable than the same question using the term ‘caregiver’.
Similarly, terms like ‘care’, ‘need’, and ‘support’ may trigger resistance, whereas describing assistance as ‘someone to help around the house with the cleaning’ (P17; Social Prescriber) can be more palatable. This was confirmed by another professional offering support for personal care, who found that: ‘asking - do you need help with bathing? - may elicit rejection in the client, whereas - what if there was somebody here that you could call if you can’t get out? - reframes support as acceptable’ (P21; Social Prescriber).
Practical explanations using simple language and concepts are key to fostering trust: ‘I don’t over complicate it. I just basically explain why I’m there and what I can do for them’ (P09; Social Care Worker). Language is also instrumental in promoting autonomy; for example, asking ‘if we could do anything, what would you want?’ (P12; Social Care Worker) elicits personal aspirations and promotes a sense of control on decision-making.
But language is not just about words. Professionals emphasised the need to communicate with—not about—individuals with dementia. It is not acceptable to assume the person lacks capacity and ‘act like the person’s not in the room, perpetuating exclusion and undermining agency’ (P14; Clinical Research Practitioner), especially when no advocate is present. Engagement must be intentional and respectful, as people ‘pick up on’ non-verbal cues of dismissal or disinterest’ (P14; Clinical Research Practitioner).
Overall, language use in dementia care can be used as a tool to promote acceptability of services in this population by being adaptive, person-centred, and grounded in empathy.
Piecing Together the Truth: Navigating Information Gaps
Accurate information gathering in dementia care is essential for effective assessment, planning, and intervention. Yet, this is particularly challenging with people with dementia who live alone and have no informal caregivers to relay accurate background information. There is often ‘no one when they are unwell… to tell us about them’ (P02; Dementia and Delirium Clinical Nurse Specialist). One professional working in acute settings noted, ‘If you don't know, what you see is what it is. You can't quite say if that is a worsening of their condition’ (P02; Dementia and Delirium Clinical Nurse Specialist). Lack of information about the client undermines the foundation for rehabilitation and personalised care.
Professionals also report that some individuals may provide misleading or incomplete information, either intentionally or due to cognitive decline. Fear of institutionalisation, for example, can lead individuals to underreport their needs: ‘There is a huge fear that a healthcare professional is going to swoop in and tell them they can’t stay’ (P14; Clinical Research Practitioner).
One strategy that has been successfully used is to ‘gauge’ the consistency of answers by asking ‘the same question at different times of the day, because they may respond differently to women or men or someone of the same background’ (P02; Dementia and Delirium Clinical Nurse Specialist). Phrasing the same question in varied ways across different days may help to identify accurate information.
Remote assessments were found to be especially vulnerable to misinformation: ‘What the patient tells you over the phone isn’t necessarily a true reflection’ (P09; Social Care Worker), reinforcing the importance of face-to-face visits. On the other hand, ‘observational methods—such as noting hygiene, odours, and food preparation—are critical’ (P13, Service Manager). For example, ‘[a professional] asking for a drink (e.g., tea) can reveal the real functioning of the person and the status of the home’ (P14, Clinical Research Practitioner).
Collaborative visits between professionals enhance accuracy, especially when one professional ‘knows the person better’ (P18; Social Prescriber). Finally, meticulous documentation is vital: ‘I need to be very detailed in my notes if someone else is following up’ (P20; Social Prescriber), ensuring continuity and accountability across care transitions.
Barriers to Engagement: Cultural, Personal, and Systemic Challenges in Dementia Support
Even when identification and referrals are made, individuals may (initially) decline support. This lack of engagement is a common and complex phenomenon among people living with dementia, particularly those who live alone and have no informal caregivers. It is shaped by a combination of personal, cultural, environmental, and systemic factors, and addressing it requires a nuanced, person-centred approach.
One of the first barriers to engagement lies in the acceptance of diagnosis, which limits willingness to approach support services. As one participant explained, ‘I think it is not very common for a person who lives alone and doesn’t have support to go to the GP [General Practitioner] and say – I feel like I have a memory problem’ (P01; Dementia Adviser). This hesitancy is often rooted in stigma, as ‘dementia has been associated with someone who is mad, someone who is losing their mind’ (P01; Dementia Adviser). Such perceptions contribute to concealment of symptoms and delayed help-seeking behaviour.
Gender and cultural norms also play a significant role in shaping resistance to support. Traditional masculine ideals, particularly among older generations, emphasise autonomy and stoicism. As one professional noted, ‘men have been living all their lives with the pressure of being independent and being strong and self-sufficient, making it really hard for that person to say – “OK now I’m ready for help”’ (P01; Dementia Adviser). Similarly, autonomy and self-reliance are deeply embedded in those who have lived independently throughout their lives. Accepting help, especially with personal care, can feel profoundly difficult. One nurse observed, ‘it is not easy when the person living with dementia has always been super independent… now, all of a sudden, they need to accept that some youngster needs to come in and help them take a bath’ (P05; Admiral Nurse). These perceptions also reflect broader Western cultural values of individualism and self-reliance, where dependency is often internalised as failure: ‘you can also see yourself as a failure if you’re not independent’ (P12; Social Care Worker).
Narratives around social welfare may further inhibit engagement. Social services can be perceived in a negative connotation, with fears of ‘the state doing something to you and removing things from you’ (P12; Social Care Worker), such as institutionalisation or loss of property. These anxieties reinforce mistrust and avoidance of formal support.
Environmental and logistical factors also create barriers. Access to services often depends on transport availability, which is a recurrent challenge for those living alone. As one adviser explained, navigating alone can be overwhelming: ‘…transport is a big one, finding the place and getting back home. One of my clients could not remember what time or where to get off the bus’ (P03; Dementia Adviser). Transport support is often tied to social care packages, as ‘support often comes with that’ (P06; Dementia Programme Lead). For those without such packages, assistance is limited to: ‘a case-by-case basis, with occasional use of taxis or informal lift shares’ (P10; Project Manager).
Professionals suggested strategies to address these barriers. Gender and cultural influences highlight the need for culturally sensitive, gender-aware approaches that challenge dominant narratives of independence. One worker advocated reframing independence toward interdependence: ‘we all are interdependent on others, a subtle but significant shift in care philosophy’ (P12; Social Care Worker). On the motivational side, professionals emphasised exploring hidden barriers. One prescriber recounted how a client refused home visits, and only through dialogue was it discovered that the distress stemmed from ‘having somebody stand over them (client) when they were still sleeping, which was quite distressing’ (P21; Social Prescriber). Adjusting the care plan accordingly improved engagement.
Maintaining a balance of power with clients in decision-making is also critical. Professionals emphasised collaborative development of care plans: ‘Instead of going ‘I’m here to tell you what’s going to happen,’ it’s actually listening to what they’ve got to say’ (P07; Social Care Worker). Building trust is equally vital, achieved through consistent support and personalised interactions. As one care lead explained, ‘relationship is at the heart of everything because it enables better communication and it enables trust’ (P16; Dementia Care Lead). Regular contact fosters familiarity and engagement: ‘What helps them to engage in services is that consistency of having a point of contact, a face that is familiar to them’ (P09; Social Care Worker).
System-level constraints, however, often undermine these efforts. Limited resources and repeated exposure to distressing situations can desensitise professionals, leaving them ‘hardened to it… they just don’t have any more empathy to give’ (P14; Clinical Research Practitioner). Without systems and processes reducing the risk of erosion of empathy, relational care can diminish and reinforce disengagement.
In conclusion, disengagement from support among people with dementia who live alone and lack informal caregivers arises from cultural values, personal fears, and practical obstacles. Addressing these challenges requires flexibility, empathy, and a commitment to understanding each individual’s uniqueness. By adopting culturally sensitive, gender-aware approaches and reframing independence as interdependence, professionals can promote sustained, compassionate engagement.
Supporting the Clients: From Risk-Aversion to Risk-Management
Some distinct challenges also present when developing and implementing support plans for the client who lives alone and unsupported. Risk and safety for this group are multidimensional issues that extend beyond physical harm to encompass psychological, emotional, and social domains. This layered understanding of vulnerability challenges reductive safety assessments and calls for holistic approaches that consider isolation, unmet emotional needs, and behavioural risks.
Environmental assessments are critical for identifying physical risk. As one professional noted, while her patient stated that she did not need home support ‘the house was absolutely cluttered, and this person was at a high risk of falls’ (P05; Admiral Nurse). In-person assessment prompted immediate referral for social care services and occupational therapy. Functional evaluations, such as asking individuals to demonstrate meal preparation, can reveal cognitive limitations that may not be evident through verbal reporting alone.
Cognitive impairment and not having informal support at home also increases susceptibility to exploitation. One participant recounted a case where a woman ‘forgot who I was and what I was there for’ (P09; Social Care Worker), which made her think how vulnerable to exploitation from strangers this client was. In fact, neighbours had previously reported that the person had been scammed by someone posing as a service provider. Another example around the risk of exploitation was reported when referring to clients’ needs for intimacy and emotional connection. A client’s pursuit of sexual companionship in their home highlighted the need for nuanced understanding of risks associated to relational needs in later life, the importance of challenging conventional ideas on age and sexual intimacy and adopting non-ageist, inclusive, person-centred approaches to addressing clients’ needs and associated risks.
Because of these unique risks, there might be a tendency on the part of professional to become risk-averse when developing support plans for these clients and to implement overreactive interventions. A professional reported that in one case she had dealt with a client’s aggressive behaviour. This had led to prescription of sedatives. The professional, however, wondered whether the decision had been made too arbitrarily, in the absence of informal caregivers. She wondered, knowing the client only superficially, ‘who am I to decide whether the client is agitated or not, whether they need sedation or not?’ (P12; Social Care Worker). This highlights the risks involved in interpreting and responding to behavioural symptoms with this particular population when there are no informal caregivers to provide information.
Another example involved an occupational therapist recommending: ‘we should really have that cooker removed, because she’s got dementia’ (P14; Clinical Research Practitioner), despite there being no evidence of misuse or tangible risk for the client. The professional reported challenging this suggestion, advocating for ‘a more dynamic’ approach that balanced autonomy with safety. Similarly, decisions on suitable accommodation frequently defaulted to residential care when individuals lacked advocates. ‘They’re not safe to go home’ becomes the prevailing narrative, excluding the person from decision-making’ (P16; Dementia Care Lead), as reported by one professional. A more flexible stance was proposed, shifting to a framework of ‘risk management as opposed to risk elimination,’ recognising that ‘anybody can fall in their own home… if we put mitigations in place, that person could manage’ (P16; Dementia Care Lead).
Collectively, these insights call for nuanced, person-centred risk assessments that prioritise dignity, context, and collaborative decision-making over blanket risk-averse safety protocols.
Preventing the Revolving Door: Strategies for Continuity of Care
Ensuring continuity of care for individuals with complex needs, particularly those with dementia who live alone with no informal caregivers requires a proactive, person-centred, and collaborative approach across health and social care systems. First contact with social services, once clients have been referred by community support services (e.g., social prescribers), is particularly vulnerable to failure when rushed or inadequately resourced. A classic example of this tangible risk was reported by one professional: ‘The person states – “No, I don’t need support. I’m managing fine”. Therefore, adult social care closes that referral’ (P17; Social Prescriber). This creates a misperception that the person is being supported, as ‘the GP… thinks adult social care is looking after that person, but that person isn’t looked after by anyone really’ (P17; Social Prescriber).
Even when a client is successfully taken on, service provision for individuals with dementia generally is characterised by fragmentation, time constraints, and inconsistent quality—resulting in what one professional described as a ‘complete potluck’ (P14; Clinical Research Practitioner). Outcomes, for instance, are highly dependent on the individual professional involved. When professionals are ‘really passionate about being an advocate’ (P14; Clinical Research Practitioner) and possess a nuanced understanding of dementia, the impact can be helpful. Flexibility and responsiveness are typical of this type of professional who sometimes go the extra mile and provide support that goes beyond their remit, acknowledging that ‘doing it myself, at least it’s done’ (P18; Social Prescriber). Maintaining involvement beyond discharge/referral is a classic example of out-of-remit activities dictated by personal commitment: ‘I check myself how it is going on even though I referred, finding ways to follow up even after I’ve referred them’ (P01; Dementia Adviser).
Short-term models of operation create particular challenges for those with dementia who live alone and unsupported, who, due to cognitive impairments and lack of any support post-discharge, despite initial improvements, fall back within system gaps. Clients with dementia may report coping well during reviews of social care packages only to deteriorate shortly after discontinuation of care, ending up back in the initial referring agency. This sets in motion a cycle of decline, and clients tend to end up ‘re-engaging with service periodically, often following recurring incidents’ (P11; Occupational Therapist). Cyclical patterns of identification of need, referral to and short-term use of services and return to the initial step with unmet needs is typical in this population group. Part of the reason for this is premature withdrawal of social support. But part of the problem has also to do with fragmented information exchange and effective communication across care transitions. This would require strategies such as making extensive/detailed notetaking on the part of the professional discharging the client to be handed over to the professional taking over; and for the professional taking over, to hold initial joint visits with the professional who has supported the client until then.
Ideally, long-term engagement is identified as a critical factor in effective support. There are examples of teams that are committed to ‘stay with that person all the way,’ contrasting with most services that ‘do what they need to do, and they move on, but the person’s still there’ (P18; Social Prescriber). This insight underscores the need for sustained, person-centred care models that prioritise consistency, adaptability, and long-term support over rigid service boundaries.
Discussion
This study aimed to address a critical gap in research and service provision for people with dementia who live alone and lack informal caregivers. Specifically, it examined the barriers professionals encounter when supporting this population and identified strategies that have proved useful for them. These strategies were organised chronologically along the dementia care pathway—from identification through post-discharge continuation of care, to provide a practical framework for professionals working with this vulnerable group.
The foremost challenge is the identification of clients living with dementia in the lack of their active self-referral, or informal caregivers facilitating the process. Practical and motivational barriers often prevent these clients from seeking help, meaning they are typically identified only following serious incidents (James & Clark, 2025), a process often triggered by neighbours or the police. Such late identification reduces the effectiveness of interventions and imposes significant costs on both individuals and services (Power et al., 2023). Remaining “hidden” for extended periods prevents timely implementation of care packages that could enable safe, longer independent living. Participants emphasised that without addressing this key barrier, discussions about barriers and strategies in subsequent stages of the dementia pathway has no purpose.
In terms of potential strategies, unfortunately, participants recognised that approaches such as welfare calls to at-risk demographics, embedding dementia screening in chronic disease reviews, informal disclosures to non-clinical staff, or rapid response hotlines still rely on clients’ ability and willingness to engage, which can often be absent. However, participants highlighted the potential of proactive community outreach, which can have high impact at relatively low costs. One such example is the Com-PROACT project, which trained community volunteers integrated within local areas and services (Primary Care Network teams) to conduct door-to-door welfare checks (Nair et al., 2025). This model proved particularly effective in reaching individuals at the intersection of dementia and marginalised identities, such as ethnic minority or LGBTQ+, who may be reluctant to engage with statutory services (Alam et al., 2021).
Once identified, individuals without informal caregivers face additional barriers at every stage of the care pathway. Literature has consistently highlighted the crucial role of informal caregivers in arranging appointments, providing accurate background information, facilitating communication and engagement with support services (Dalgarno et al., 2021; Di Lorito et al., 2025; Lampinen et al., 2025; Sunjaya et al., 2025; Zuber et al., 2024). In their absence, clients must navigate these processes alone, often resulting in missed appointments, incomplete information, resistance to support, and disengagement.
Professionals reported that these challenges necessitate the presence of a “key supporter”—a service representative who assumes the responsibility of helping clients to navigate services. However, this role is not formally conceived of in the current service provision, leading to overlap across services and reliance on individual professionals’ commitment (in the best-case scenario) or to a lack of consistent support (in the worst). While many professionals go beyond their remit to provide this support, such ad hoc arrangements create great inequity in service provision (Miele et al., 2022). Further, relying on a single professional may lead to overdependency, “separation anxiety” at discharge, resistance to new providers, and as a result, falling back again into system gaps. A recurring cycle of time-bound support, discharge, loss of contact, and re-entry into services at worsened stages was observed.
As a result, another key finding of the study was a need to shift from a paradigm of time-bound support toward continuity of care. Ideally, services would accompany clients consistently across the pathway (Saragosa et al., 2025). Considering resource constraints, however, participants recognised the value of improved information sharing, joint visits during transitions, and regular follow-up between referrer and clients, as well as between services. These practices could mitigate risks associated with fragmented care and ensure smoother transitions.
Risk management emerged as another distinct challenge. In households with informal caregivers, professionals can rely on a system of checks and balances that allows calculated exposure to risk, yielding benefits such as autonomy and wellbeing (Lindeza et al., 2020). In contrast, when clients live alone, professionals reported a tendency toward risk aversion, driven by the severity of incidents prompting referral and the perception of sole responsibility. Promoting independence, however, requires a shift from risk aversion to risk management, acknowledging that complete elimination of risk is impossible, and can in fact be harmful (Marnfeldt & Wilber, 2025). One example was that of a client who wanted intimacy and let strangers into their home for these purposes. The professional acknowledged that this was an important need to be addressed, and that the risks that the client would be exposed to in letting strangers into the house could not and should not be eliminated. However, some mitigating measures could be deployed to ensure their safety (e.g., follow-up calls from professional, securing belongings).
This study was characterised by certain strengths and limitations. It addressed the gap in research reporting professional perspectives of supporting people with dementia who live alone and without informal caregivers. By interviewing a diverse sample of professionals across roles, responsibilities, locations, genders, and ethnicities, the study generated practical recommendations applicable to a range of professionals. Input from an advisory group, including two people with lived experience of dementia, strengthened the relevance of findings through Patient and Public Involvement (PPI)-informed validation.
The study also had several limitations. All participants in the sample were from England, which limited the generalisability and transferability of findings to other healthcare systems and configurations. Further, the study did not include participants living with dementia. Recruitment challenges, common with this group, were compounded by the difficulty of identifying those among them who live alone, have no informal caregivers, and have experience of receiving support. In line with principles of research inclusion, future studies should therefore plan and deploy strategies to facilitate inclusion and representation of the voices of people with dementia living alone to ensure that research reflects the perspectives of those who will ultimately be affected by it.
Conclusion
This study found that professionals face unique challenges when supporting people with dementia who live alone and lack informal caregivers across the care pathway. Identification remains the most critical step, with late referrals following crises undermining intervention effectiveness. Community outreach models, such as Com-PROACT, offer promising solutions for earlier engagement, particularly among marginalised groups.
Beyond identification, the absence of informal caregivers creates additional obstacles, necessitating the presence of a consistent “key supporter” and highlighting the importance of continuity of care. Risk management must shift from avoidance to balanced strategies that promote autonomy while mitigating harm.
By addressing these challenges, services can move toward more equitable and effective support for this vulnerable population. The findings underscore the need for systemic changes that prioritise continuity, long-term engagement, and person-centred risk management, as essential conditions in sustaining independent living for people with dementia who live alone.
Footnotes
Ethical Considerations
The study obtained sponsorship from UCL, and HRA (Health Research Authority)/IRAS (Integrated Research Application System) ethical approval from the Social Care Research Ethics Committee (Ref: 24/IEC08/0033).
Consent to Participate
Written informed consent from all participants was required/gathered before taking part in the qualitative interviews.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This presentation features independent research funded by the National Institute for Health Research Applied Research Collaboration North Thames (NIHR ARC North Thames). The views expressed are those of the authors and not necessarily those of the National Institute for Health Research or the Department of Health and Social Care.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on request.