
Abstract
Dementia is a growing public health concern in sub-Saharan Africa (SSA), driven mostly by an ageing population and increasing life expectancy. Evidence has shown that physical activity is an effective, non-pharmacological intervention to improve health outcomes for people living with dementia, but the extent to which it has been utilized among older adults with dementia in SSA remains unclear. This scoping review aimed to map and describe physical activity interventions targeting older adults with dementia or cognitive impairments in SSA using JBI guidelines. We systematically searched seven electronic databases (PubMed, Scopus, Embase, CINAHL, PsycINFO, SPORTDiscus and African Journal Online). We also searched Google Scholar, and other gray literature sources. A total of three studies were found, all three were interventional studies. Intervention characteristics were described using the FITT-VP framework (Frequency, Intensity, Time, Type, Volume, and Progression) and compared to international recommendations for physical activity. Outcomes and diagnostic tools were also described, alongside considerations of cultural tailoring. Findings indicate that despite a low volume of studies, interventions implemented largely aligned with international physical activity recommendations for older adults living with chronic health conditions. Improvements were reported in cognitive function, functional ability, and societal participation. However, there was limited use of culturally tailored diagnostic and outcome assessment tools, and interventions. The last eligible study was published in 2021, highlighting a stagnation in research despite the increasing prevalence of dementia in SSA. Potential reasons include underdevelopment of dementia research, diagnostic challenges, and poor indexing of African research in academic databases. Nevertheless, this review showed that physical activity is a promising strategy to address the growing gap in dementia care in SSA. Future research should focus on developing physical activity interventions co-designed with the local communities and adapted to the sociocultural contexts.
Introduction
Dementia is a growing global health challenge which affects mostly older adults, but also puts a significant pressure on healthcare systems, families, and caregivers (Aranda et al., 2021). The World Health Organisation (WHO) estimates that there are currently over 55 million people living with dementia, and this number is projected to increase to 139 million by 2050 due to the global ageing population (WHO, 2023). Dementia is associated with progressive decline in cognitive and physical function, loss of independence, increased caregiver burden, and rising healthcare costs (Aranda et al., 2021).
Sub-Saharan Africa (SSA) is experiencing a demographic transition, with a rapidly increasing ageing population and a corresponding rise in the prevalence of dementia and cognitive impairments (Akinyemi et al., 2022; Alemayehu et al., 2025). The increasing prevalence of dementia in SSA is also attributed to increasing life expectancy and non-communicable diseases (Alemayehu et al., 2025), and improving diagnostic capacity (Paddick et al., 2013). The determination of the current prevalence of dementia in SSA has been extremely challenging with estimates ranging from 2.3% to over 20% (Alemayehu et al., 2025). The disparity in the reported prevalence rates were mostly due to poor identification, methodological differences, and generally limited access to health care services in the region (Alemayehu et al., 2025; Paddick et al., 2013). Despite the limitations of the current estimates, projections suggest the prevalence rate will triple by 2050 (The Lancet Public Health, 2021). Yet, dementia care remains underdeveloped in many SSA countries, with limited specialized services and a continued heavy reliance on informal care by family members (Akinyemi et al., 2022; Alemayehu et al., 2025; WHO, 2017).
A major barrier to effective dementia care in SSA is the widespread underdiagnosis of the condition, particularly in rural and underserved areas (Akinyemi et al., 2022; Paddick et al., 2013). This has been attributed to low awareness, cultural perceptions of ageing, lack of trained personnel, and the limited availability of culturally appropriate diagnostic tools (Alemayehu et al., 2025). Additionally, there is no clear consensus on the most suitable diagnostic criteria for dementia in African populations, further complicating efforts to accurately estimate and address its burden (Paddick et al., 2013). Against this backdrop, physical activity is emerging as a promising, non-pharmacological strategy for improving cognitive function, preserving independence, and enhancing the quality of life in people living with dementia (de Almeida et al., 2020; McArthur et al., 2024).
Growing evidence from systematic reviews and meta-analyses supports the benefits of physical activity for people living with dementia or cognitive impairment, including small-to-moderate improvements in global cognition, activities of daily living, quality of life, and behavioural and psychological symptoms, although effects vary by intervention type, duration, and intensity (Do et al., 2020; McArthur et al., 2024; Mendes et al., 2023; Xiao et al., 2024; Zhou et al., 2022). Across these reviews, multicomponent exercise interventions, particularly those that combine aerobic and resistance training appear most likely to yield clinically meaningful, though still modest, benefits (Borges-Machado et al., 2021; Law et al., 2020; Liu et al., 2025; McArthur et al., 2024; Venegas-Sanabria et al., 2022; Xiao et al., 2024).
As a low-cost and adaptable intervention, physical activity is especially appealing in resource-constrained settings like those in SSA, where formal health and social care services are limited (Naidoo et al., 2024). Moreover, the WHO recommends that for substantial health benefits, older adults living with chronic health conditions should engage in at least 150–300 minutes of moderate intensity aerobic physical activity or at least 75–150 minutes of vigorous intensity aerobic physical or an equivalent combination of both moderate and vigorous intensity aerobic physical activity throughout the week (WHO, 2024a). Despite the physical activity guidelines for older adults, adherence remains low in sub-Saharan Africa. For example, the WHO estimates suggest that approximately one-quarter of adults aged 60 years and older in the African Region are insufficiently active, with prevalence increasing with age (Bull et al., 2024). Consistent with this, regional reviews report high levels of physical inactivity among older adults in sub-Saharan Africa (Naidoo et al., 2024).
However, many reviews in SSA have indicated that the success of physical activity interventions in SSA is highly dependent on their contextual relevance (Akinyemi et al., 2022; Alemayehu et al., 2025; Guerchet et al., 2017). These studies suggest that interventions that are tailored to the cultural, social, and economic realities of target populations are more likely to be accepted and sustained (Akinyemi et al., 2022; Naidoo et al., 2024). This can include using locally meaningful activities (e.g., dancing or group walking) that ensure accessibility and incorporate social or community-based approaches (Naidoo et al., 2024).
Despite a growing body of international research supporting the benefits of physical activity for people with dementia, evidence from SSA remains scarce (Alemayehu et al., 2025). A recent scoping review of physical activity interventions implemented for older people in SSA showed that when combined with lifestyle education, structured physical activity programs reduces non-communicable diseases among the population (Naidoo et al., 2024). However, the extent to which physical activity interventions have been developed, implemented, and evaluated for older adults with dementia or cognitive impairments in SSA has not been reviewed. In this review, cognitive impairment is defined as age-related cognitive decline or clinically defined conditions such as mild cognitive impairment or dementia and does not include lifelong developmental cognitive impairment or cognitive deficits secondary to acute brain injury, stroke, or other neurological conditions.
This scoping review aims to map and describe physical activity interventions among older adults with dementia or cognitive impairment in SSA. Specifically, this review will be guided by the following questions: (a) What physical activity interventions have been implemented and evaluated for older adults with dementia or cognitive impairment in sub-Saharan Africa? (b) What are the key characteristics of these interventions, including frequency, intensity, time, type, volume, and progression? (c) What outcomes have been assessed to evaluate the effects of these interventions? And (d) To what extent do these interventions align with current physical activity recommendations for older adults, and were cultural tailoring strategies reported?
Methods
This scoping review was conducted following the JBI methods for scoping reviews (Peters et al., 2024) and is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis extension for scoping Reviews (Tricco et al., 2018). The protocol for this review has been published elsewhere (Ibekaku et al., 2025).
Inclusion Criteria
Participants
We included studies involving people with a diagnosis of dementia and or older adults (≥65 years) with cognitive impairment residing in SSA.
Concept
The review focused on reports of physical activity interventions for older adults with dementia or cognitive impairment. We adopted the WHO definition of physical activity, including structured and unstructured bodily movements that result in energy expenditure, such as walking, aerobic training, resistance training, and functional exercises (WHO, 2024b).
Context
Studies were included if they were conducted in SSA countries, regardless of setting (community, residential care, clinical, or institutional). SSA is a region of the African continent that lies south of the Sahara, consisting of 48 of the 54 countries within the African continent (Britannica, 2025).
Types of Sources
We considered both quantitative and qualitative empirical studies, as well as mixed-methods studies. Reviews, editorials, commentaries, and opinion pieces were excluded, but their references were screened for potentially relevant studies.
Search Strategy
A comprehensive three-step search strategy was employed. First, an initial limited search of MEDLINE and CINAHL was undertaken to identify relevant keywords and indexing terms. This informed a broader search across multiple databases: PubMed, CINAHL, PsycINFO, SPORTDiscus (all via EBSCOhost); Scopus and Embase via Elsevier and African Journals Online. Additional sources searched for gray literature were Google Scholar (the first 20 pages) and the Database of African Theses and Dissertations-Research. We did not restrict the search by date or language, or language of publication and the search strategy was peer-reviewed by a health sciences librarian at Dalhousie University. The final search was conducted in April 2025. Key search terms included dementia/cognitive impairment, physical activity/exercise, and sub-Saharan Africa, combined using Boolean operators and adapted across databases. The full PubMed search strategy was published as part of the review protocol (Ibekaku et al., 2025) and is reproduced in Supplemental File I. This strategy was adapted for use in the other databases by modifying controlled vocabulary and syntax as appropriate.
Study Selection
All records retrieved were imported into Covidence for screening and a pilot screening was completed with all five reviewers jointly reviewing selected articles from the reference lists during a Team’s meeting. Titles and abstracts as well as full text screenings were completed by five reviewers (MCI, NN, CPO, JMFY, and SM) with each article reviewed independently by two reviewers. Discrepancies were resolved in both stages of the screening by a third reviewer.
Data Extraction
A data extraction form was developed from a template in Covidence and was pilot tested by the review team. Extracted data included: study details (author, year, country), study design, characteristics of participants, type and description of physical activity intervention (frequency, intensity, time, type, volume, and progression), outcome measures, results, and any information related to cultural tailoring of the interventions. Two reviewers independently extracted data, with disagreements resolved through discussion.
Data Analysis and Synthesis
The data were summarized using descriptive statistics and narrative synthesis. Physical activity interventions were analyzed using the FITT-VP framework (Frequency, Intensity, Time, Type, Volume, and Progression) (Baptista et al., 2024). The FITT-VP framework is a structured approach to describing and evaluating exercise interventions. It specifies the Frequency (how often sessions occur), Intensity (the level of effort required), Time (duration of each session), Type (form of activity, e.g., aerobic, strength), Volume (total amount of exercise), and Progression (how the program is increased over time) (Bushman, 2018). We also examined the extent to which the interventions were culturally tailored to the local sociocultural and economic context. Sociocultural context was not used as an inclusion or exclusion criterion during study screening. Instead, data related to cultural tailoring and contextual relevance (e.g., use of locally meaningful activities, community-based delivery, or adaptations to social norms and resource constraints) were extracted during data charting and synthesized narratively.
Results
We retrieved 5,281 studies from the database searches. After removing duplicates, 4,471 citations underwent title and abstract screening, resulting in 42 full-text articles assessed for eligibility. Of these, 39 studies were excluded for the following reasons: wrong setting (studies conducted outside sub-Saharan African, (n = 13)), wrong study type (e.g., protocols, reviews, or observational studies without an intervention, (n = 12)), wrong intervention (non-pharmacological interventions that did not include physical activity or exercise, such as cognitive stimulation therapy alone, (n = 4)), wrong population (studies involving participants without dementia or population with cognitive impairments that are younger than 65 years, including studies focused on HIV-associated neurocognitive disorders or stroke survivors, (n = 7)), and abstract-only publications, ((n = 3). Figure 1 presents the PRISMA flow diagram of the study selection process. PRISMA flow diagram of the study selection process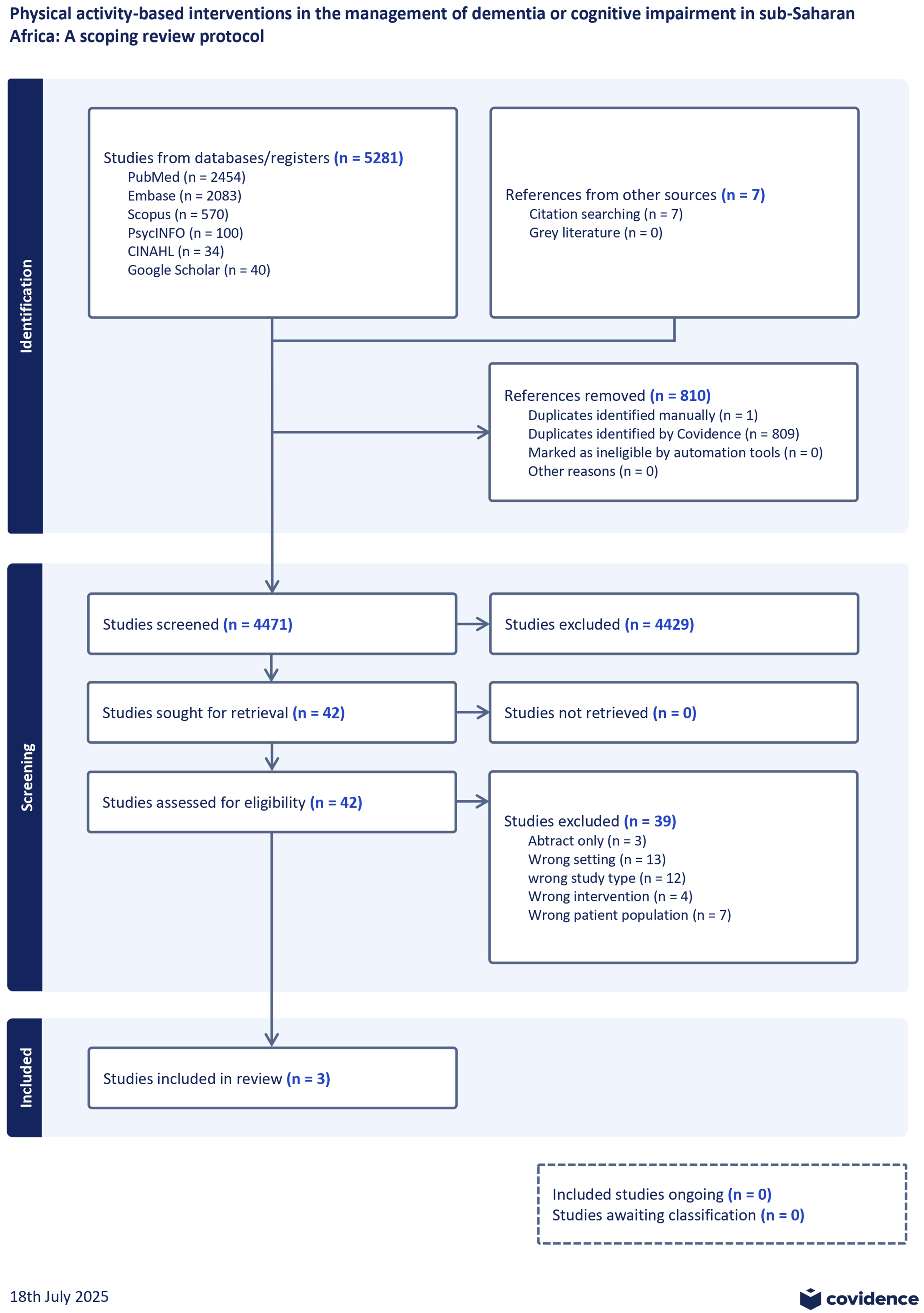
Characteristics of Included Studies and Study Population
Three studies were included in this review and were published between 2020 and 2021. These included two randomised controlled trials (Gbiri & Amusa, 2020; Shaw et al., 2021) and a pre-post intervention study with a qualitative component for caregivers (John et al., 2021). Two studies were conducted in Nigeria (Gbiri & Amusa, 2020; John et al., 2021), one in South Africa (Shaw et al., 2021). The studies were conducted in residential care facilities (John et al., 2021; Shaw et al., 2021) and a tertiary hospital (Gbiri & Amusa, 2020).
Descriptive Summary of Included Studies
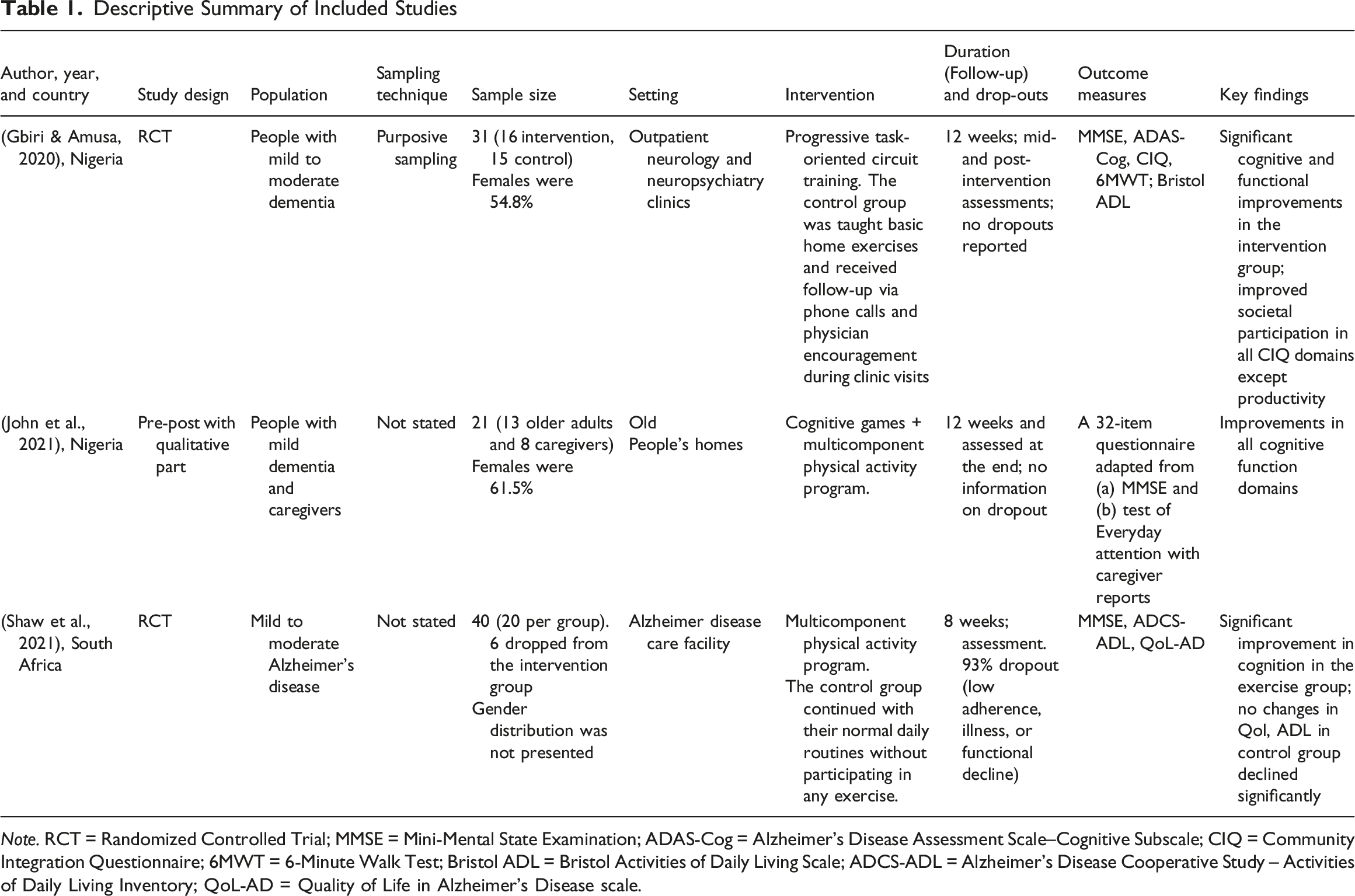
Note. RCT = Randomized Controlled Trial; MMSE = Mini-Mental State Examination; ADAS-Cog = Alzheimer’s Disease Assessment Scale–Cognitive Subscale; CIQ = Community Integration Questionnaire; 6MWT = 6-Minute Walk Test; Bristol ADL = Bristol Activities of Daily Living Scale; ADCS-ADL = Alzheimer’s Disease Cooperative Study – Activities of Daily Living Inventory; QoL-AD = Quality of Life in Alzheimer’s Disease scale.
Dementia was determined differently across the studies. Mild to moderate Alzheimer’s disease was diagnosed based on National Institute of Neurological and Communication Disorders and Stroke and the Alzheimer disease and related disorders association criteria (Shaw et al., 2021), Community Screening Interview for Dementia and the Five-Word Test (John et al., 2021), However, Gbiri and Amusa (2020) did not report any diagnostic criteria.
Types of Physical Activity-Based Interventions
FITT-VP for Intervention Studies
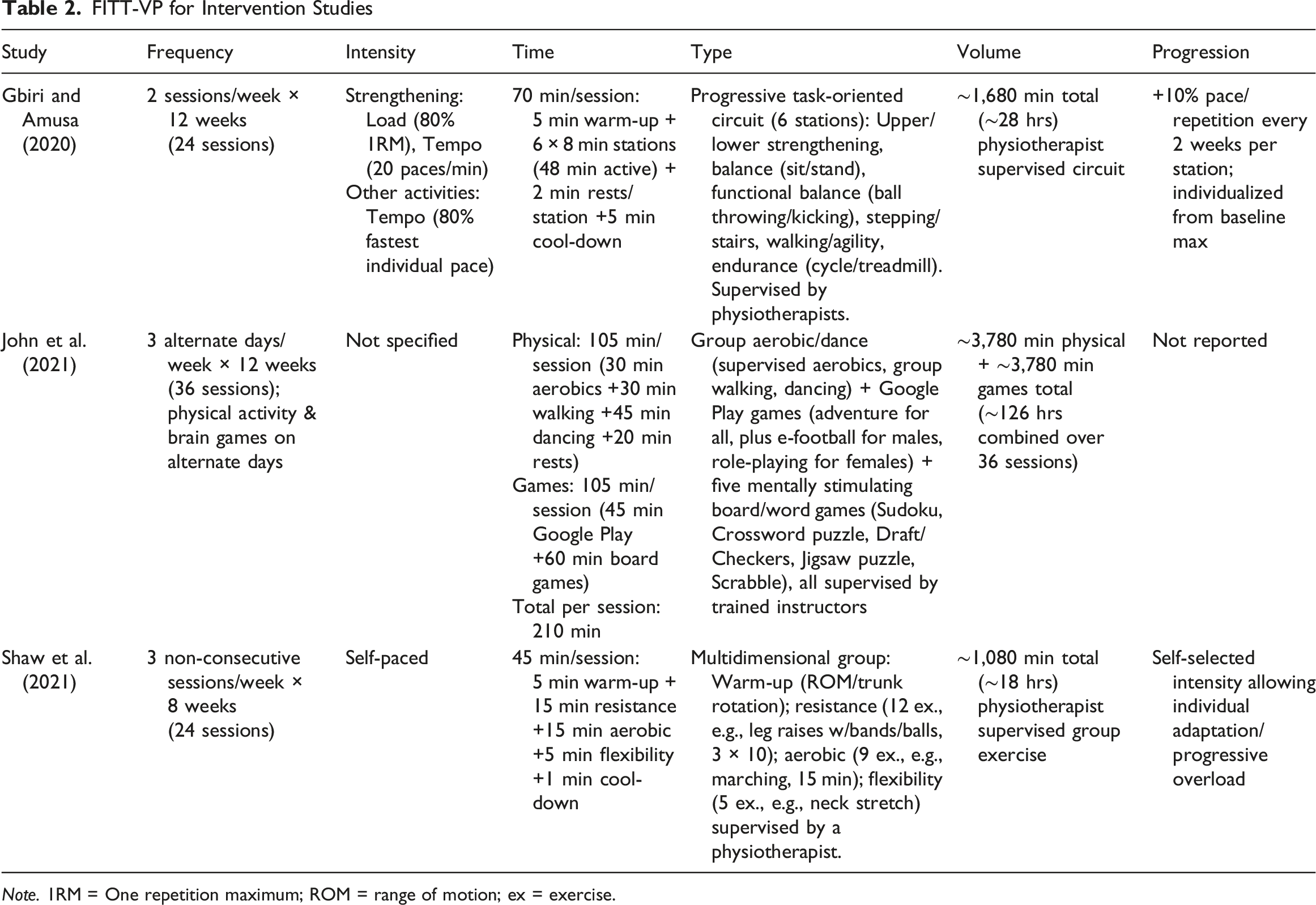
Note. 1RM = One repetition maximum; ROM = range of motion; ex = exercise.
FITT-VP Characteristics of Included Interventions
Using the FITT-VP principles, we summarized the exercise interventions across all included studies in Table 2. The programs included different exercise types, including aerobic, strengthening, balance, and flexibility exercises, and the duration of each session ranged from 45 minutes to over 100 minutes. Hence, their duration generally met or exceeded the WHO’s recommendation of at least 150–300 minutes of moderate-intensity physical activity per week for older adults with chronic health conditions. Notably, one study also integrated an additional 105 minutes of cognitive stimulation through digital and board games on alternate days, hence, participants were engaged six days per week over 12 weeks. All sessions were supervised by physiotherapists or trained instructors. To gradually increase the total volume of exercise received by participants, the studies used varying strategies to progress the prescribed physical activity. Gbiri and Amusa (2020) progressed the exercises by 10% every two weeks while Shaw et al. (2021) progressed the prescriptions based on participants’ tolerance.
Cultural Tailoring of Interventions
Socioeconomic and cultural factors were not major considerations across the included studies. John et al. (2021) described their intervention as low-cost and considered gender differences in the selection of cognitive games, but this was not extended to physical activity. Gbiri and Amusa (2020) involved informal caregivers in the study, including assisting with comprehension and adherence.
Discussion
This scoping review aimed to map and describe studies that have utilized or described the use of physical activity among older adults with dementia or cognitive impairments in SSA countries. Only a small number of relevant studies were identified, with the most recent published in 2021, highlighting a persistent gap in research and practice in this area.
Physical activity interventions included in this review largely aligned with current evidence-based recommendations for older adults with chronic health conditions based on the FITT-VP principles (Naidoo et al., 2024; WHO, 2020). However, the exercise intensity and progression criteria were objectively described in only one of the studies (Gbiri & Amusa, 2020). Specifically for older adults with chronic health conditions in SSA, Naidoo et al. (2024) recommended that physical activity interventions should span at least over 12 weeks, include at least three 1-h sessions per week, and combine both aerobic and resistance training at moderate intensity and progressed over time. They also emphasized incorporating task-oriented and enjoyable activities to enhance adherence and cognitive stimulation (Naidoo et al., 2024). While two of the three intervention studies did not include task-oriented activities, and one of the study lasting for only eight weeks (Shaw et al., 2021), the studies were largely consistent with the recommendations. Hence, these physical activity programs could potentially improve health outcomes for older adults with dementia.
Some outcomes and outcome measures commonly used in physical activity interventions for people with dementia (de Almeida et al., 2020; McArthur et al., 2024). The diagnosis of Mild Cognitive Impairment and dementia was confirmed using different diagnostic criteria and with one of the studies describing no specific means of assessing who had dementia (Gbiri & Amusa, 2020). This is interesting as many studies have attributed an extremely low prevalence of dementia in SSA especially in rural areas to lack of diagnostic capacity including lack of culturally adapted screening tools (Akinyemi et al., 2022; Guerchet et al., 2017) and lack of consensus on which diagnostic criteria is best suited to SSA (Paddick et al., 2013). This shows that without consistent and culturally tailored diagnostic approaches, both the accurate identification of dementia and the evaluation of intervention effectiveness in SSA will remain limited, underscoring the urgent need for standardized and contextually adapted diagnostic tools.
Similarly, the Alzheimer’s Disease International (2021) reported that while 75% of all cases of dementia cases are undiagnosed globally, the number of undiagnosed cases in low-and-middle income countries are up to 90% (Alzheimer’s Disease International, 2021). Other outcomes such as cognitive function, functional outcomes, and quality of life were measured using different tools including an adapted version of the mini mental status exam (John et al., 2021). According to Akinyemi et al. (2022), cognitive diagnostic tools that are culturally tailored, with excellent psychometric properties, and that are capable of minimizing biases linked to variations in language and levels of education, are needed for deployment across SSA. For example, the Community Screening Instrument for Dementia and the Intervention for Dementia in Elderly Africans Cognitive Screen have been validated in Nigeria and Tanzania, with high accuracy even among populations with low literacy (Gray et al., 2016; Paddick et al., 2015). Similarly, functional assessment tools like activities of daily living, have also shown strong psychometric properties among SSA population (Akinyemi et al., 2022), which should provide a more holistic and context-tailored evaluation of dementia. Despite these advances, their limited use in intervention studies including those in this review suggests a continued gap in dementia research in SSA.
Physical activity represents a promising and cost-effective approach to supporting people with dementia, particularly in many SSA countries where access to formal health and social care services is limited (Li et al., 2023). Low-cost physical activity programs provide an opportunity for accessible and scalable interventions that are not only effective but also align with cultural norms and local values (Naidoo et al., 2024). However, the pace of research development in this area has been slow and appears to be stagnating, with no new studies published since 2021. This slow progress is concerning given the increasing burden of dementia in SSA and the growing evidence supporting physical activity as a non-pharmacological intervention. There is an urgent need for renewed attention and investment in this area as findings from other regions cannot simply be transplanted to SSA because differences in culture, health systems, socioeconomic conditions, and daily activity patterns may affect both the feasibility and effectiveness of physical activity interventions (Akinyemi et al., 2022; Naidoo et al., 2024). While the limited volume of published studies may partly reflect the broader underdevelopment of this research area, it is also important to consider that research from SSA is often poorly indexed in major bibliographic databases such as Web of Science and Scopus (Asubiaro, 2023; Mills & Asubiaro, 2024). Although our search strategy included regional databases like African Journal Online, and other open sources such as Google Scholar, and gray literature sources to help mitigate this limitation, these searches did not yield many additional studies. This suggests that, beyond indexing challenges, there may be a genuine gap in the development and dissemination of physical activity interventions for people with dementia in SSA. Future studies should prioritize co-designed, community-embedded physical activity programs that are feasible, culturally tailored, and evaluated using validated cognitive and functional outcome tools appropriate for SSA contexts.
Strengths and Limitations
This scoping review has several strengths. First, it is the first study to specifically review physical activity programs for the management of dementia in SSA and, as such, draws attention to the urgent need for more research in this area. Secondly, we consulted an experienced health sciences librarian who helped develop a comprehensive and rigorous search strategy, and we also thoroughly reviewed sources of grey literature, including thesis databases, to ensure we captured all relevant articles.
The limitations of this review should also be acknowledged. Although we did not restrict by language, we searched only English-language databases, which may have led to the exclusion of articles published in other languages, particularly French, which is an official language in many SSA countries. Additionally, despite the broad and inclusive search, only a small number of studies met the inclusion criteria, limiting the generalizability of the findings. Another limitation is that research from SSA is often poorly indexed in major databases which may have contributed to the small number of studies identified. Finally, the possibility of publication bias cannot be ruled out, especially in regions where studies with null results may be less likely to be published or disseminated.
Conclusion
This scoping review shows that while physical activity interventions for dementia in SSA align with international recommendations, research in this area is scarce, and limited by diagnostic and outcome measures that might not be culturally tailored. Given the rising dementia burden and limited access to formal care in the region, there is an urgent need for culturally tailored, community-based, and scalable programs in SSA.
Supplemental Material
Supplemental Material - Physical Activity Interventions for Older Adults With Dementia or Cognitive Impairment in Sub-Saharan Africa: A Scoping Review
Supplemental Material for Physical Activity Interventions for Older Adults With Dementia or Cognitive Impairment in Sub-Saharan Africa: A Scoping Review by Michael C. Ibekaku, Nazanin Nasiri, Chukwuebuka P. Onyekere, Jasmine M. Friedrich Yap, Sydney MacNinch, Lawrence Adebusoye, Lori E. Weeks, Parisa Ghanouni, Caitlin McArthur in Dementia
Footnotes
Acknowledgement
The authors would like to thank Shelley McKibbon, Health Sciences Librarian at Dalhousie University, for their invaluable support in developing the search strategy for this review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data for this scoping review consist of published studies retrieved from electronic databases and grey literature sources. No primary data were collected. A detailed search strategy, including search strings for each database, is provided in Supplemental File I. The full reference list of included studies is available in the main manuscript. Raw data extraction forms are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.