
Abstract
Behavioural interventions, such as those provided by allied health professionals and psychologists, help manage symptoms of people living with dementia. Access to such interventions depends on individual factors (e.g., support, travel) and service availability. One way to improve access and availability is via synchronous telehealth. However, there may be challenges implementing telehealth interventions. A systematic review was conducted to explore barriers and facilitators to implementing synchronous telehealth interventions for people living with dementia. The review protocol was registered on PROSPERO (CRD42024508098). Five databases were systematically searched in February 2024. Implementation determinants were extracted and analysed deductively using the Theoretical Domains Framework (TDF) and COM-B behaviour change model. Determinants that did not correspond with the TDF or COM-B were described inductively using content analysis. Determinants were further analysed as to whether they pertained to the intervention, or to the technology used to deliver it. 25 papers were included in the review, including group, dyadic and individual interventions from 14 countries including those from the Global South. Key implementation determinants corresponded to the TDF domains Environmental Context & Resources and Knowledge. Two inductively created domains were developed: Creativity & Safety. Most implementation barriers were to do with technology. These were often clear problems with potentially straightforward, linear, implementation solutions related to the COM-B concepts of Capability and Opportunity. Most implementation facilitators involved the telehealth intervention itself. These were often complex issues, with potentially complex and non-linear implementation strategies, most often related to the concept of Motivation. Reporting quality was variable in the literature. Use of implementation and behaviour change frameworks may enhance reporting, reproducibility, and improve implementation of behavioural telehealth interventions for people with dementia. Using the TDF and COM-B can help clinicians and policymakers to identify and prioritise implementation determinants, delineate potential implementation strategies, and guide decision making to improve practice.
Background
Dementia describes a group of neurodegenerative conditions which progressively and differentially impact multiple neurocognitive domains including memory, motor function, behaviour and language (World Health Organisation, 2025). In 2021, approximately 57 million people worldwide were estimated to be living with dementia, with 10 million new cases diagnosed annually. Over 60% of these cases are predicted to come from low- and middle-income countries (World Health Organisation, 2025). By 2050, the total number of people living with dementia is set to reach over 152 million (Alzheimer’s Disease International, 2019). With recent pharmaceutical advances in dementia treatment (e.g., Hardy & Mummery, 2023; Mummery et al., 2023), non-pharmacological behavioural interventions for dementia symptom management - such as those provided through speech and language therapy, physiotherapy, occupational therapy, psychology, care and caregiver support - are also showing positive impacts for people with dementia and their care partners (Livingston et al., 2024; Morello et al., 2017; Woods et al., 2023). However, access to such interventions is impacted by individual circumstances including travel constraints and availability of a support network (Gulline et al., 2025). Service availability is also variable across healthcare providers, settings, and geographical location, particularly for rarer dementias (Giebel et al., 2025; Hockley et al., 2025; Sullivan et al., 2025). These determinants directly contribute to health inequalities (Giebel et al., 2024).
One way to increase the reach and availability of behavioural interventions for dementia is via synchronous telehealth, i.e., delivered synchronously online via videoconferencing or telephone. Telehealth may increase access to behavioural interventions, enabling more people living with dementia, their families and friends, to engage with and benefit from them. This may be particularly relevant for those unable to attend clinic-based sessions, such as people in the later stages of dementia. Telehealth also enables care partners with work or caring commitments to attend or support sessions (e.g., Volkmer, Walton, et al., 2023). As such, telehealth delivery may influence both the implementation and uptake of interventions.
The COVID-19 pandemic necessitated a rapid and substantial expansion of telehealth usage (Omboni et al., 2022; Shaver, 2022). While adoption and attitudes during this period may not be typical, the pandemic has likely permanently reshaped the role and perception of telehealth.
As telehealth becomes more widespread, identifying determinants that support implementation and sustainability is essential (Thomas et al., 2024).
Implementation Science, Complexity, and Telehealth in Dementia
Implementation science is “the study of methods and strategies to promote the adoption and integration of proven clinical treatments, practices, organisational, and/or management interventions into routine practice.” (Neuman et al., 2020, p. 434). While effectiveness research focusses on how interventions work, implementation science focusses on ways to enable the “spread and adoption”, integration and sustainability of evidence-based interventions in real-world settings (Glasgow et al., 2012, p. 1275).
Delays in translating health research into clinical practice result in reduced patient access to evidence-based interventions and wasted research and development effort (Morris et al., 2011). Over half of clinical innovations never make it into general clinical usage (Bauer & Kirchner, 2020). Furthermore, interventions which are poorly implemented in everyday practice may not produce the same health benefits seen in research trials, leading to poor clinical outcomes (Neuman et al., 2020). Considering the pace of technological advance, implementation of telehealth interventions may be particularly problematic. To address the research-practice gap, the Medical Research Council (MRC) framework for evaluating complex interventions emphasises that implementation should be considered early and throughout intervention development to increase the chance of their timely, widespread and sustained adoption. Implementation questions should be addressed at each stage of intervention development and evaluation (Skivington et al., 2021). Implementation processes are therefore iterative. Implementation questions extend beyond assessing effectiveness to examine how interventions may be implemented across dynamic and evolving settings and contexts (Raine et al., 2016). Implementation processes must therefore be both non-linear and consider complexity (Murdoch et al., 2023). This may be especially relevant in dementia (where symptoms evolve over time and interact with individuals’ lives and overall quality of life), telehealth (evolving technology and use within organisations), and behavioural interventions (changing therapeutic protocols and relationships over time).
Using theoretical frameworks to systematically identify implementation determinants (i.e., barriers and facilitators) can lead to more effective implementation strategies, and better understanding of implementation outcomes (Eccles et al., 2005; Haynes & Loblay, 2024). Implementation outcomes are indicators of the success and quality of implementation efforts, defined by constructs including acceptability, adoption, appropriateness, feasibility, fidelity, cost, and sustainability (Proctor et al., 2011). The Theoretical Domains Framework (TDF) (Cane et al., 2012) is a comprehensive, integrative, meta-theoretical framework which helps to identify behaviour change factors across fourteen domains and thereby investigate implementation determinants and strategies (ways to leverage facilitators and overcome barriers to improve outcomes) (Atkins et al., 2017; Phillips et al., 2015). The TDF has been informative in understanding behaviour change and implementation in healthcare interventions (Cane et al., 2012; Cowdell & Dyson, 2019; Schaffer & Henry, 2023).
However, limitations of the of the TDF have been described including lack of domain specificity (Atkins et al., 2017), insufficient specification of how domains may interact (Cowdell & Dyson, 2019; Lipworth et al., 2013; McGowan et al., 2020), and difficulty accounting for context, such as socio-cultural factors impacting behaviour and implementation (Mather et al., 2022). Thus, the framework has been enhanced using various methods. For instance, researchers have applied the TDF using a deductive approach (i.e., aligning data within the TDF domains) alongside inductive reasoning. This enables categorisation of content that does not neatly fit within the existing TDF domains, ensuring that important but unexpected themes are not overlooked. As an example, the TDF has been combined with content analysis (Elo & Kyngäs, 2008; Hsieh & Shannon, 2005) by Shrubsole and colleagues (2023) to identify and then synthesise determinants to speech and language therapists implementing communication partner training (Shrubsole et al., 2023). The TDF has also been used alongside reflexive thematic analysis (Braun & Clarke, 2006) to better account for the impact of socio-cultural factors on complex healthcare interventions (e.g., Nguyen-Hoang et al., 2024; Petersen et al., 2023).
To overcome difficulties identifying how TDF domains may combine, the TDF has been integrated with complementary frameworks such as the COM-B model. This model is structured into three domains (Capability, Opportunity, and Motivation) that have been proposed as pivotal in changing behaviour (Michie et al., 2011, 2014). The COM-B has been used alongside the TDF in healthcare implementation systematic reviews (e.g., Atkins et al., 2020; Mather et al., 2022; Shrubsole et al., 2023) and telehealth implementation research (e.g., MacPherson & Kapadia, 2023).
Existing Reviews of Telehealth Dementia Interventions
Previous reviews have examined aspects of telehealth in dementia care but with notable gaps. Some have only investigated specific conditions such as Alzheimer’s or Parkinson’s disease (e.g., Adams et al., 2020; Yi et al., 2021) or narrowly focussed on assessment and services over specific interventions (Yi et al., 2021). While other reviews have more broadly considered intervention implementation and all dementia types (e.g., Liang & Aranda, 2023; Ye et al., 2025) findings have been listed in terms of barriers and facilitators, an overly reductive approach that has been criticised for potentially missing crucial interactions between implementation determinants (Haynes & Loblay, 2024). Nevertheless, common issues across these reviews include limited sample diversity, persistent digital access barriers, and an emphasis on social and personal benefits of using telehealth with people with dementia.
Existing reviews therefore either lack a focus on implementation using a theoretical framework (Liang & Aranda, 2023; Ye et al., 2025) or address specific neurodegenerative conditions (Adams et al., 2020; Yi et al., 2021). This study aims to fill this gap and answer the research question: What are the barriers and facilitators to implementing behavioural telehealth interventions for people living with dementia, of any type, with or without their care partners?
Methods
The protocol for this systematic review was pre-registered and published on PROSPERO on the 31st January 2024 under registration number CRD42024508098. The protocol follows the PRISMA-P (Moher et al., 2015) and PRISMA E&E (Liberati et al., 2009) transparent reporting of systematic reviews recommendations.
Search Strategy
On the 1st February 2024, systematic searches were undertaken in five databases: MEDLINE, Embase, PsycINFO (accessed through Ovid) and CINAHL Plus and Scopus; predicted to encompass the dementia intervention literature from medicine, nursing, allied therapies, and psychology.
The search strategy was refined in consultation with research librarians at University College London (co-authors EC and BW). Consequently, the broad terms ‘virtual’ and ‘remote’ were not used to reduce the risk of retrieving papers focusing on non-therapy interventions, e.g., virtual training environments for professionals. The search was limited to articles published since 1st January 2018 because preliminary searches identified an acceleration of dementia telehealth intervention papers published from 2018 onward, including a surge in telehealth use necessitated by the COVID-19 pandemic. Including intervention delivered during the COVID-19 period was predicted to provide evidence on intervention adaptations under pressure, as well as potential lasting shifts in telehealth practice.
The search strategy included the following concepts to search article titles, abstracts and keywords: dementia (and associated terms) AND telehealth (and associated terms) AND intervention (and associated terms). See Figure 1 for the full search strategy. Full search strategy
Study Selection
Selection Criteria
National Institute of Health Research and Care Excellence (NICE) guidance on ‘Dementia: assessment, management and support for people living with dementia and their carers’ (NICE, 2018) frames dementia intervention as rehabilitation. To align with this, the operational definition of intervention used for article inclusion was taken from the World Health Organisation definition of rehabilitation, specifically “a set of interventions designed to optimize functioning and reduce disability in individuals with health conditions in interaction with their environment” (World Health Organisation, 2024). To broaden inclusion, intervention studies were not required to be implementation studies. They could include research studies which were not implemented within real-world practice and did not have to have specific implementation outcomes. Implementation determinants are defined as barriers or facilitators which could potentially influence implementation outcomes, extracted from researcher and participant reports within the studies.
Quality assurance
RT assessed the quality of papers using the Mixed Methods Appraisal Tool (MMAT) (Hong et al., 2018). The MMAT is a reliable quality assessment instrument, which enables the assessment of qualitative, quantitative and mixed methods study designs within the one tool (Crowe & Sheppard, 2011). Qualitative and quantitative papers are scored on a scale of 0–5. Mixed-methods papers are scored out of 15 by adding qualitative and quantitative scores to a mixed-methods component which is also scored out of 5. No papers were eliminated following quality assessment. There was no rating cut-off for eliminating a paper. Ratings were included to inform the reader of the quality of the studies, and to help describe and understand them.
Data extraction
Summary of Extracted Data
Data Analysis
Deductive thematic analysis was used to group identified implementation determinants according to behaviour change domains from the TDF (Cane et al., 2012) which were then subsumed within the COM-B model (Michie et al., 2014) using framework analysis (Ritchie & Lewis, 2003). Concepts which did not align with domains in the TDF, but which repeatedly appeared in the retrieved literature, were coded inductively using content analysis and informed the development of new domains (Elo & Kyngäs, 2008; Hsieh & Shannon, 2005). The inductive coding process involved: open coding - recording an identified determinant that could not be neatly aligned with the TDF categorization - grouping the codes to identify recurring patterns abstraction - grouping categorised data into higher order themes
The frequency of deductive and inductive domains was analysed using descriptive statistics and interpreted using narrative synthesis. This process was informed by the system used by Shrubsole et al. (2023). Steps included: Summarise how often a TDF domain (and corresponding COM-B component) or inductive domain appeared Code determinants as to whether they pertained to the intervention, the technology, or a mixture of the two (i.e., it was not possible to disassociate the two concepts) Group similar determinants together as exemplar categories of implementation determinants within domains
Results
The search identified 2,796 articles. Following duplicate removal, 1,297 article titles/abstracts were screened for eligibility. Having excluded 1,251 articles, 46 full texts were retrieved and screened for inclusion. This resulted in the exclusion of a further 23 articles. The references of the remaining 23 articles were then checked against the inclusion and exclusion criteria by RT. This resulted in the in the addition of a further two articles. Thus, a total of 25 articles were included in the review. The PRISMA flow diagram (see Figure 2) provides details of reasons for exclusion. PRISMA flow diagram for selection of studies documenting barriers and facilitators to telehealth implementation in dementia
Quality Assurance
The quality of the literature was high. All qualitative papers scored the maximum 5/5. All quantitative papers scored 3/5 or above (five scoring 5/5, six scoring 4/5, and three scoring 3/5). The four mixed-methods studies ranged in quality from 9/15 to 15/15 (Average = 12/15). See supplemental file 1 for details of the quality assessments.
Study Characteristics
Study Characteristics
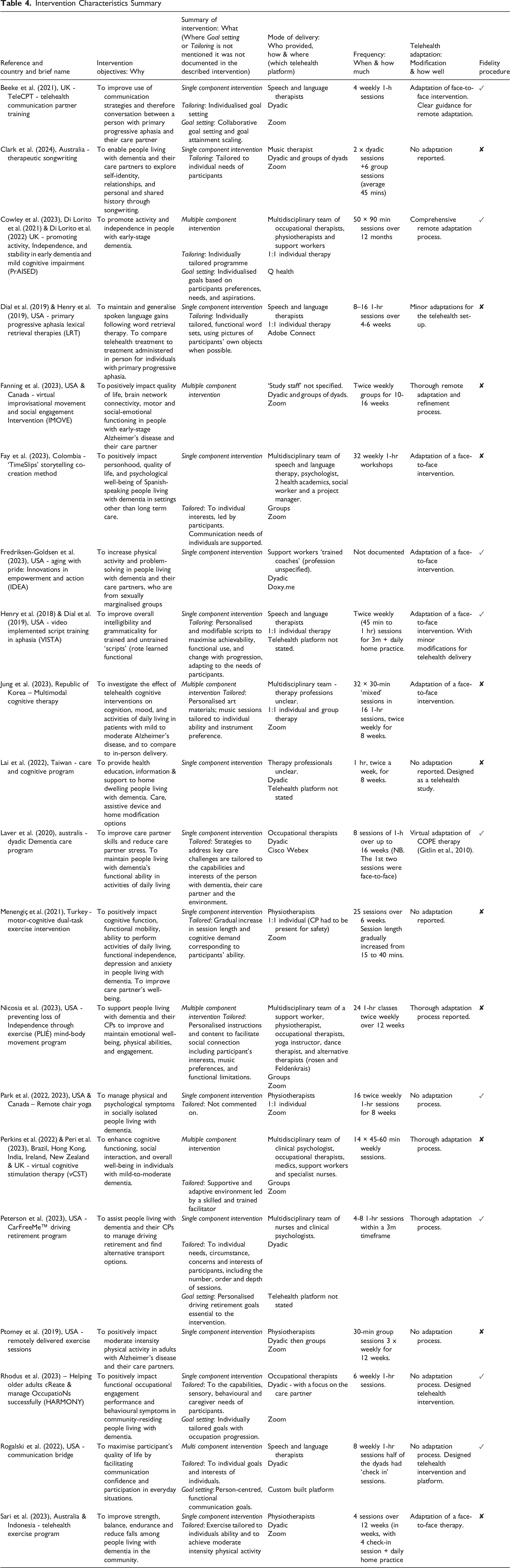
Studies are presented in alphabetical order by first author. See Table 4 for details of the interventions.
Implementation Frameworks:
aBowen’s Feasibility Framework (Bowen et al., 2009).
Consolidated Framework for Implementation Research (CFIR) (Damschroder et al., 2009).
cFramework for Reporting Adaptations and Modifications-Expanded model (FRAME, Stirman et al., 2019).
dTechnology Adoption Model (TAM) (Davis, 1989).
eUnified Theory of Acceptance and Use of Technology (UTAUT) (Venkatesh et al., 2003).
Intervention Characteristics Summary
Six studies used frameworks to inform implementation, or help describe feasibility, adaptation and acceptance (Fredriksen-Goldsen et al., 2023; Lai et al., 2022; Park et al., 2022, ; Perkins et al., 2022; Sari et al., 2023).
All 25 studies reported positive implementation outcomes in terms of feasibility, acceptability or adoption. One study (Lai et al., 2022) reported possible negative adoption outcomes due to increased care partner support burden during the telehealth intervention. Views on implementation were reported based on the opinions of researchers (included in 14 studies), people living with dementia (in seven studies), care partners (nine studies) and therapists (eight studies).
No papers provided health economic data, or details of implementation costs. Despite this, seven studies (28%) made assumptions about cost savings of telehealth over in-person intervention delivery. These included time and money savings related to cancellations and session scheduling (Fredriksen-Goldsen et al., 2023), travel (Beeke et al., 2021; Menengiç et al., 2021), perceived efficiency (Di Lorito et al., 2021; Ptomey et al., 2019) and emotional cost savings such as reduced participant stress (Lai et al., 2022; Perkins et al., 2022).
The inclusion criteria in 17 studies (68%) resulted in digital exclusion (e.g., participants had to have their own equipment, internet connection, or prior technological skill). Of the eight papers without this inclusion criteria, three studies provided equipment or training (Fanning et al., 2023; Fredriksen-Goldsen et al., 2023; Laver et al., 2020), with five studies providing no documented solution to support technology use (Henry et al., 2018, 2019; Jung et al., 2023; Peterson et al., 2023; Rogalski et al., 2022).
Ten studies (40%) described interventions which were necessitated by the COVID-19 pandemic, i.e., they were not designed as telehealth studies from the outset, but were adapted due to the pandemic (Beeke et al., 2021; Cowley et al., 2023; Di Lorito et al., 2021, 2022; Fanning et al., 2023; Fay et al., 2023; Fredriksen-Goldsen et al., 2023; Peri et al., 2023; Perkins et al., 2022; Sari et al., 2023).
Intervention Characteristics
The 25 retrieved studies described 20 interventions. These are summarised in Table 4 according to the characteristics from the template for intervention description and replication (TIDieR) checklist (Hoffman et al., 2014). Supplemental file 2 provides a complete summary of intervention components.
Why (Intervention Objectives), What (Intervention Type) and Who (Intervention Provider)
The 20 interventions represented a range of intervention types and providers. Six studies investigated multiple-component interventions (e.g., physical therapy combined with cognitive therapy), five of which were delivered by multi-disciplinary teams (MDTs) (Cowley et al., 2023; Di Lorito et al., 2021, 2022, Jung et al., 2023; Nicosia et al., 2023; Perkins et al., 2022; Peri et al., 2023). The remaining multi-component intervention was delivered by speech and language therapists, which included condition education and support alongside a variety of communication therapy approaches (Rogalski et al., 2022). The remaining fourteen studies investigated single component interventions (e.g., communication, or physical therapy focused alone).
In summary, five interventions were predominantly communication therapies delivered by speech and language therapists (Beeke et al., 2021; Dial et al., 2019; Henry et al., 2018, 2019; Rogalski et al., 2022), five were physical therapies delivered by physiotherapists (Menengiç et al., 2021; Park et al., 2022, 2023; Ptomey et al., 2019; Sari et al., 2023), two focussed on care and environment optimisation delivered by occupational therapists (Laver et al., 2020; Rhodus et al., 2023), and one described a collaborative songwriting intervention delivered by music therapists (Clark et al., 2024). Five interventions were delivered by MDTs, which included allied health professionals, psychologists and complementary therapists (e.g., yoga and Feldenkrais instructors). Of these, two were cognitive rehabilitation therapies (multimodal cognitive therapy in Jung et al., 2023; cognitive stimulation therapy in Perkins et al., 2022; Peri et al., 2023), and three were a mixture of cognitive, physical, complimentary and communication therapies (Cowley et al., 2023; Di Lorito et al., 2021, 2022; Nicosia et al., 2023). In the remaining three interventions it was unclear who delivered the intervention. These were a cognitive behavioural intervention (Fredriksen-Goldsen et al., 2023), a health education intervention (Lai et al., 2022) and an improvisational movement and social engagement intervention. (Fanning et al., 2023). Of all 20 reported interventions a quarter (n = 5) documented personalised goal setting processes (Beeke et al., 2021; Cowley et al., 2023; Di Lorito et al., 2021, 2022; Peterson et al., 2023; Rhodus et al., 2023; Rogalski et al., 2022)
How (Delivery Mode and Configuration) and Where (Telehealth Platform)
Six interventions (30%) were one-to-one between a therapist and a person with dementia (Cowley et al., 2023, Dial et al., 2019, Di Lorito et al., 2021, 2022; Henry et al., 2018, 2019; Jung et al., 2023; Menengiç et al., 2021; Park et al., 2022). Nine and the majority of interventions (45%) were dyadic, i.e., the person with dementia and their care partner engaged together with a therapist (Beeke et al., 2021; Fredriksen-Goldsen et al., 2023; Lai et al., 2022; Laver et al., 2020; Peterson et al., 2023; Ptomey et al., 2019; Rhodus et al., 2023; Rogalski et al., 2022; Sari et al., 2023; Sari et al., 2023, 2023). The remaining five interventions (25%) were group interventions (Fay et al., 2023; Nicosia et al., 2023; Peri et al., 2023; Perkins et al., 2022) including two groups of dyads (Clarke et al., 2024; Fanning et al., 2023).
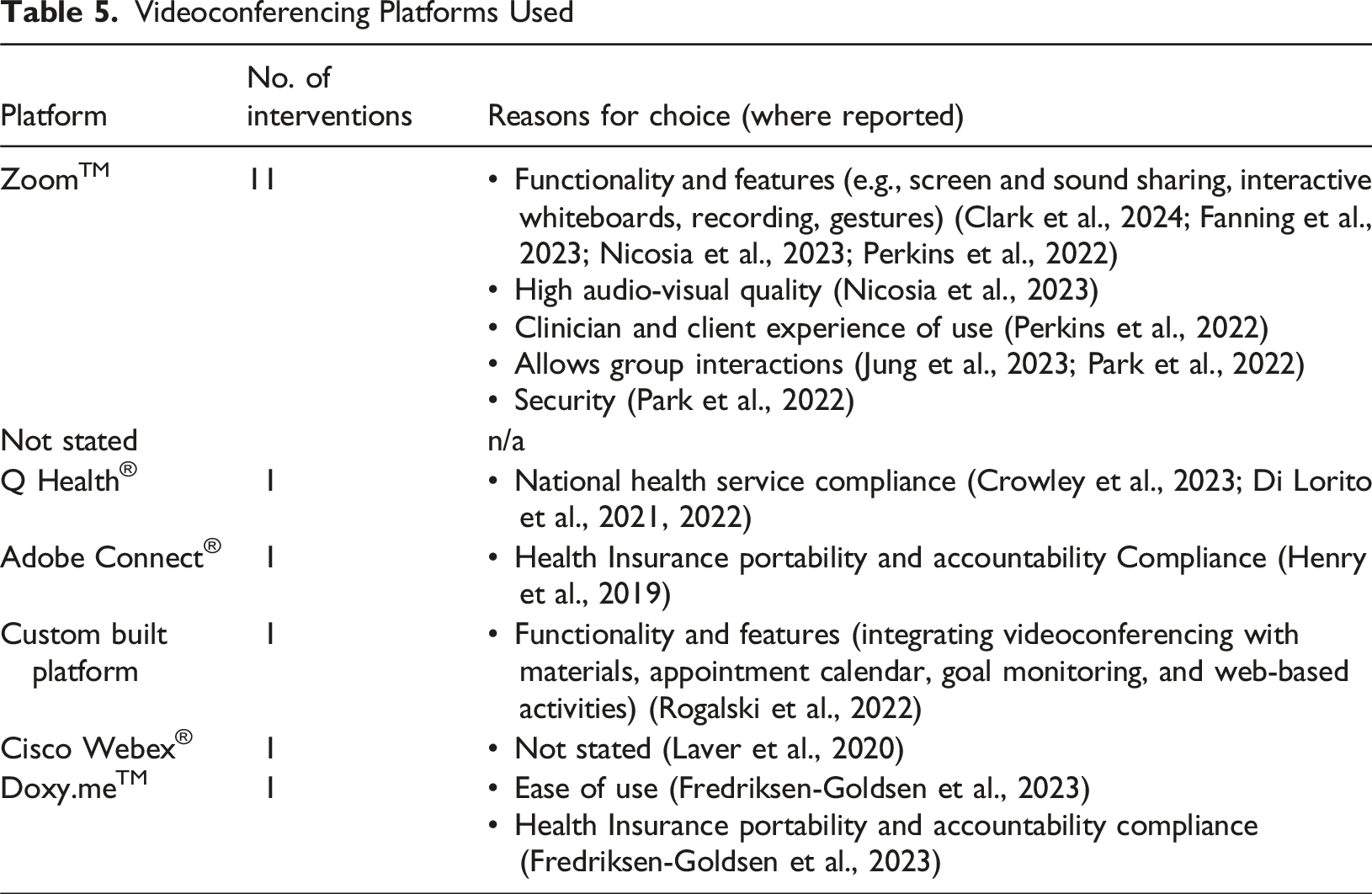
Videoconferencing Platforms Used
When and How Much (Duration, Number of Sessions)
There was a wide range of intervention durations and intensities reported, from four one-hour sessions delivered once-weekly (Beeke et al., 2021), to 50 ninety-minute sessions over twelve months (Di Lorito et al., 2021).
Modifications and How Well (Adaptations and Fidelity)
Seven interventions (35%) were designed and trialled as telehealth interventions from the outset. The remaining thirteen interventions described telehealth adaptations of a face-to-face intervention (65%). Of these, seven were adapted for online due to the COVID-19 pandemic, while six were planned adaptations. Eight interventions (40%) reported fidelity procedures, with only one paper (Henry et al., 2018) specifically reporting fidelity outcomes.
Implementation Barriers and Facilitators
TDF Domains
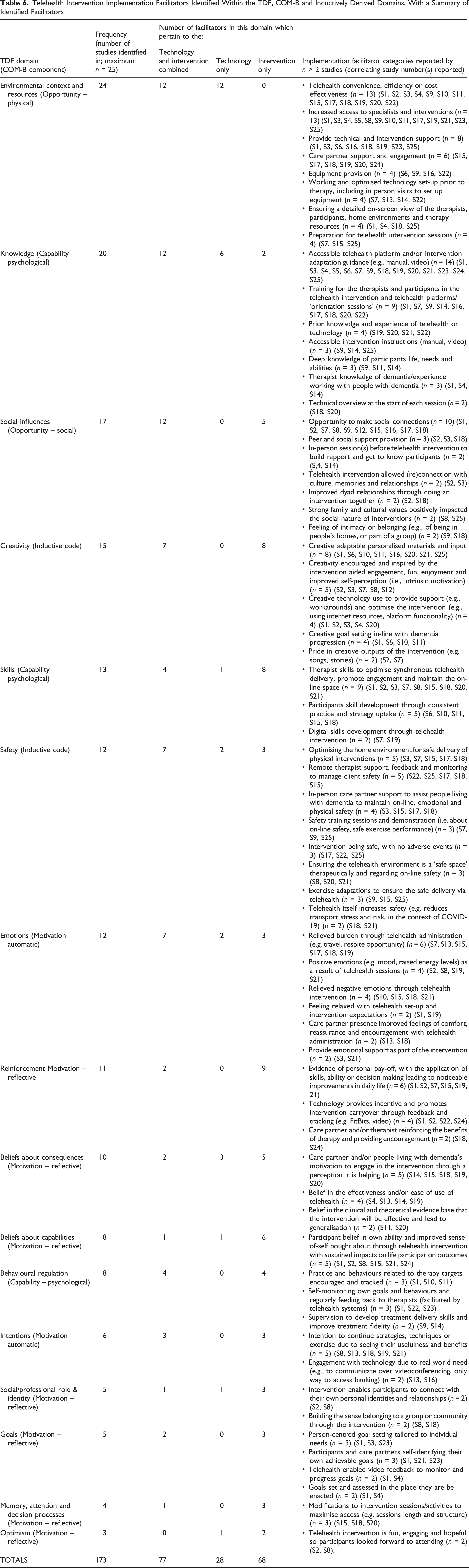
Implementation determinants were deductively categorised into the 14 TDF domains. Two further domains ‘Creativity’ and ‘Safety’ were inductively identified in the content analysis. These domains included determinants related to: Creativity: Creative telehealth adaptation such as therapist creativity to overcome technological or contextual barriers in the remote delivery of an intervention, creative use of technology to enhance an intervention, creative goal setting and personalised materials in-line with individual needs and dementia progression, and pride from creative output of interventions. Safety: Participant physical, psychological or digital safety to engage in a telehealth intervention without a therapist present in-person; feelings of a ‘safe space’ engendered by a group or therapeutic alliance.
Frequently identified determinants of creativity and safety often fell outside TDF domains, prompting the two new inductive domains to capture these nuances.
Telehealth Intervention Implementation Facilitators Identified Within the TDF, COM-B and Inductively Derived Domains, With a Summary of Identified Facilitators
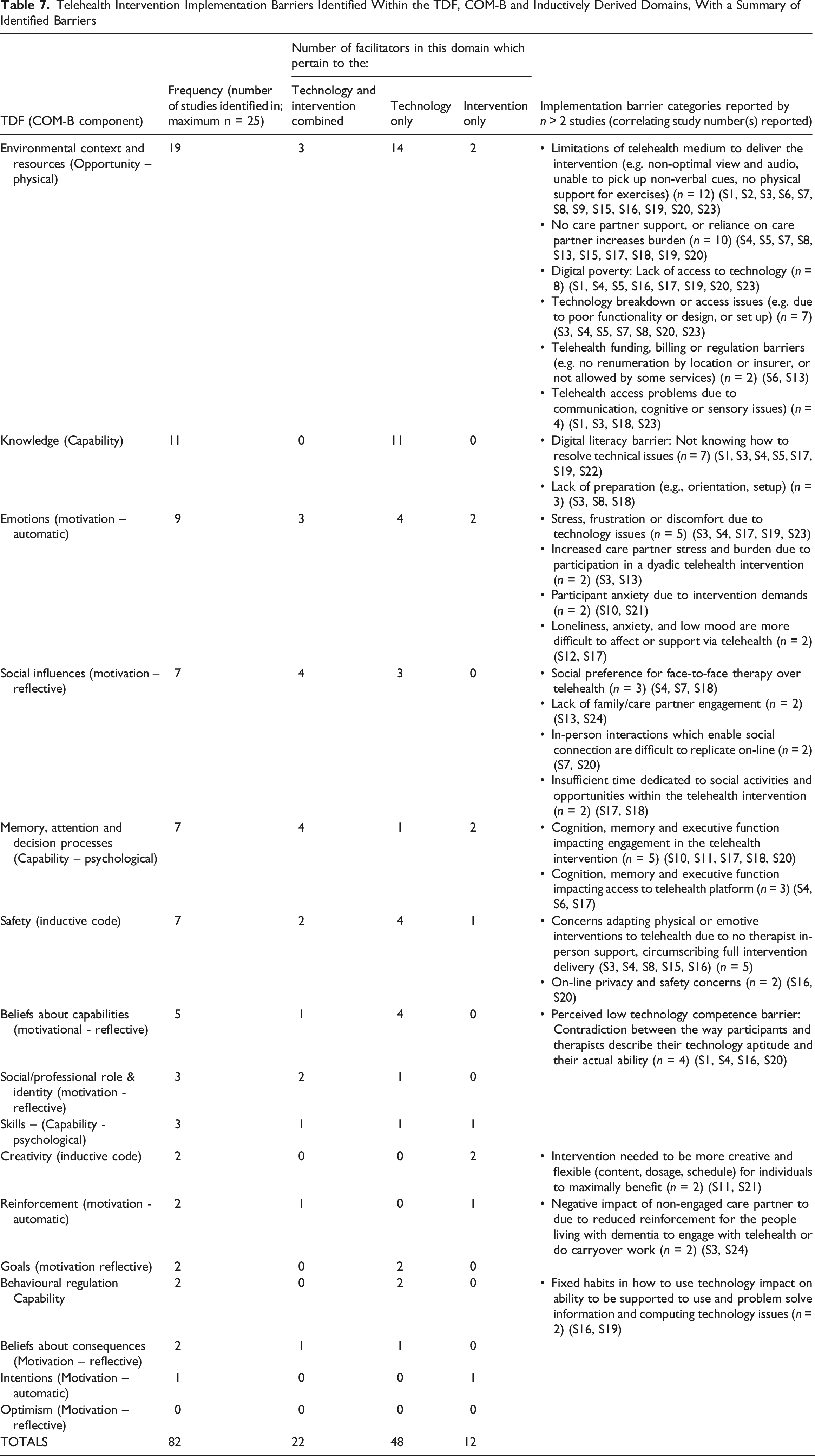
Telehealth Intervention Implementation Barriers Identified Within the TDF, COM-B and Inductively Derived Domains, With a Summary of Identified Barriers
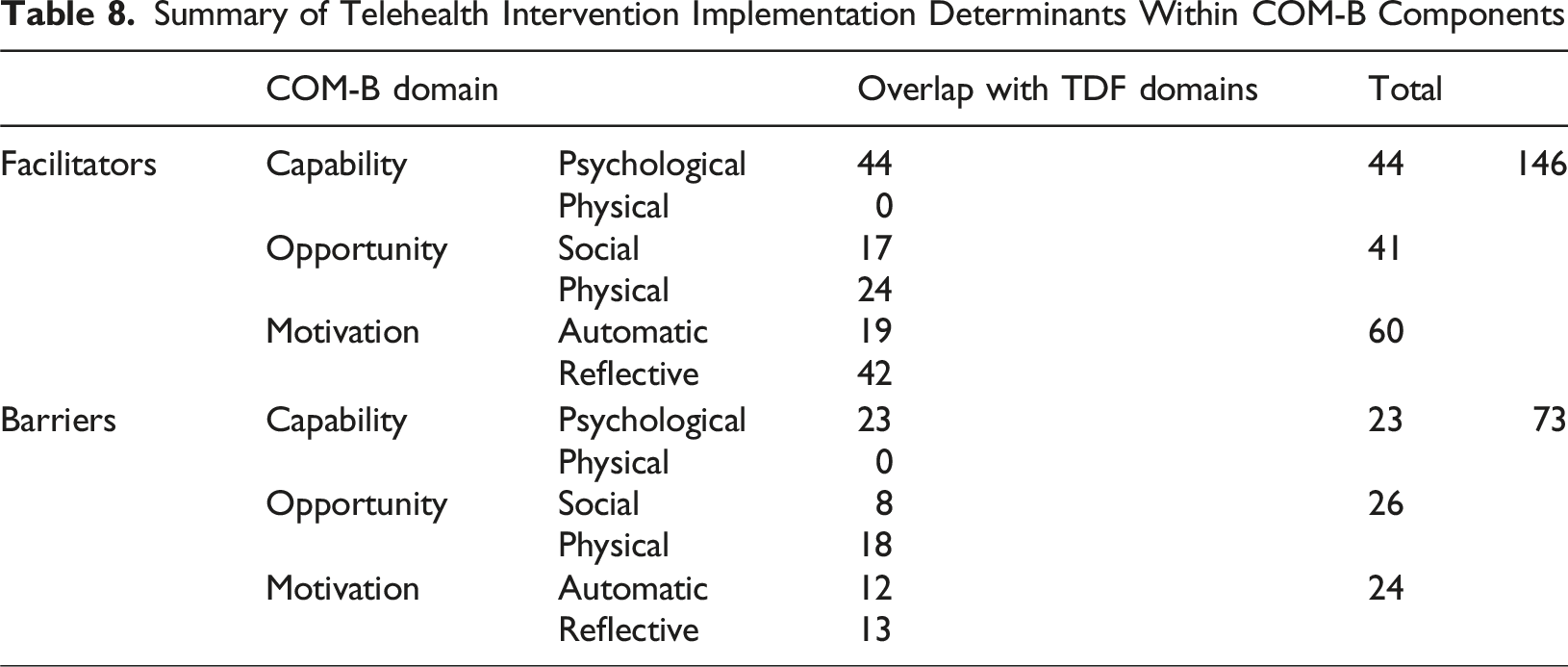
COM-B Concepts
Summary of Telehealth Intervention Implementation Determinants Within COM-B Components
Discussion
This systematic review identified 25 peer reviewed studies which investigated barriers and facilitators to implementing synchronous telehealth interventions with people with dementia. Despite categorising determinants using the TDF and COM-B theoretical frameworks, two additional domains ‘Safety’ and ‘Creativity’ were identified. The data were further categorised as either barriers or facilitators to implementation and classified based on whether they pertained solely to the intervention, the technology, or both.
Inconsistent Reporting
Studies in this review did not consistently report all aspects of telehealth interventions or their implementation. Key details were often missing, possibly because only 24% used a framework to guide implementation or adaptation. These omissions included details of videoconferencing platforms and their adaptations, information on clinicians delivering the intervention, the dementia type studied and implementation costs. Such gaps hinder comparisons, replication, and implementation efforts. Provision to address digital exclusion was rarely documented, despite recommendations to tackle digital access barriers (Ye et al., 2025).
40%) of the studies in the review reported fidelity procedures. This compares favourably to evidence of fidelity reporting in the aphasia (21%; Brogan et al., 2019) and dementia (22.5%; Hwang et al., 2024) behavioural intervention literature, only one paper actually reported fidelity outcomes, key to implementation (Proctor et al., 2011). Inconsistent reporting and inadequate specification have been shown to compromise the replicability and efficacy of complex interventions and their implementation (Hoffman et al., 2014; Lewis et al., 2018; Michie et al., 2009; Proctor et al., 2023; Stirman et al., 2019). Including details of telehealth platform used, how it was adapted to facilitate the intervention, costs, and who delivered and benefitted from the intervention, can facilitate future implementation efforts across contexts (Miller et al., 2021).
Care Partner Role
Care partner involvement and support were identified as important facilitators to telehealth intervention implementation, while their lack of such involvement and support acted as a corresponding barrier. Care partners were important in maintaining safety, helping overcome technological barriers and to providing motivational support. Care partner engagement was a particularly important implementation determinant linked to clinical and functional outcomes in Rogalski et al.’s (2022) multi-component speech and language therapy telehealth intervention. Care partner involvement has also been identified as an important implementation determinant in quality of life interventions in dementia (Hockley et al., 2023; Wyman et al., 2022). A crucial implementation strategy may therefore be to encourage and support care partner input. Dyadic interventions may be particularly amenable to telehealth interventions, and to those living with dementia, hence the high representation of dyadic interventions in this review.
Technology Facilitators
Ease of use of the telehealth platform is an important determinant in implementation. Zoom was the most frequently used platform. This is perhaps unsurprising considering its ease of use compared to other videoconferencing software, and widespread usage in telehealth (Hersh et al., 2024; Hilari et al., 2024). This review found common determinants emphasising optimal human-computer interaction (HCI) design and access, echoing a prior telehealth review (Scott Kruse et al., 2018). HCI design is the process of creating user-friendly digital systems that are efficient and accessible by focusing on how people interact with the technology. Unfortunately, platforms used by health care organisations can have poor HCI design and access (e.g. Di Lorito et al., 2021). Therefore, engaging information governance managers to support preferred platforms may be a key implementation strategy (e.g. Peri et al., 2023).
Creative and Social Facilitators
The importance of replicating social aspects of face-to-face interventions via telehealth was reflected by the prominence of the Social influences domain as a facilitator, the third most frequently identified facilitator domain. Commonly identified determinants included incorporating social opportunities into intervention schedules (e.g., Park et al., 2023), incorporating local cultural elements into interventions (e.g., Fay et al., 2023), and meeting face-to-face before embarking on remote therapy (Di Lorito et al., 2021; Laver et al., 2020). The importance of peer and social support is well documented for people with dementia and their care partners (Carter et al., 2020; Willis et al., 2016), including providing such support via telehealth (Dam et al., 2016), especially those with rare dementias (Harding, 2023; Sullivan et al., 2022). Social factors may be overstated in studies during COVID-19, when telehealth offered rare social contact. Still, digital platforms have been shown to help people with dementia manage pandemic stresses through connection and self-actualisation (Talbot & Briggs, 2022). Social facilitators have also been reported outside the pandemic context, for example in telehealth peer-support groups for care partners of individuals with primary progressive aphasia (Schaffer & Henry, 2023), and in previous systematic reviews of telehealth in dementia (Liang & Aranda, 2023; Ye et al., 2025). Ensuring that social and peer support opportunities prevalent in in-person interventions are not lost in telehealth delivery may be important to implementation and sustainability.
Creativity was repeatedly identified (n = 15 studies) in this review as a facilitator domain. Creativity was often related to the Skills (the 4th most frequently identified domain) of therapists to adapt materials and interventions for on-line use, make the most of opportunities provided by technology and overcome telehealth access barriers. The Royal College of Speech and Language Therapists surveyed members on changes to service delivery made during the COVID-19 pandemic and found adoption of telehealth was one of the most common, with over half of therapists reporting this provided opportunities for innovative, creative practice (61%) and skills development (54.4%) (RCSLT, 2020). Creativity also encompassed determinants related to the adaptability of interventions for telehealth delivery. Given that ten studies employed telehealth only in response to the COVID-19 pandemic, the prominence of Creativity may be overrepresented in studies from this period. Whenever Creativity was identified as a facilitator, so was the Goal domain, implying a connection. However, patient centred goal setting was only documented in five interventions. This is likely related to the strict therapy protocols seen in several interventions, which required repetitive practice but with the absence of personally relevant goals (e.g., Ptomey et al., 2019; Sari et al., 2023). A consideration for future implementation studies of telehealth dementia interventions should be the inclusion and adaptability of goal-setting procedures, so that goals can be modified in line with progression and remain relevant and useful to people’s changing lives, thus improving motivation.
Clinician Views
The views of clinicians themselves are underrepresented in the studies in this review. For example, eight of 25 studies included clinicians’ views; however, even fewer studies identified their views within the domains of Social/professional role and identity (n = 2) or clinicians’ Beliefs about [the] consequences of telehealth interventions (n = 5). Although Motivation component domains were the most frequently identified TDF domains overall, their significance in the implementation of telehealth interventions for dementia may still be underestimated in this review, as determinants relevant to therapists might be missing. Previous reviews investigating clinician determinants of intervention implementation have found that Motivation domains are the least frequently identified (e.g., Mather et al., 2022; Shrubsole et al., 2023). Ultimately, it is clinicians who deliver interventions and who make decisions key to their implementation and sustainability, notwithstanding setting and contextual factors. Future research should therefore probe individual clinician’s Motivation TDF domains more deeply, particularly considering their potential interaction with frequently identified TDF domains, which may be crucial to implementation and intervention success.
Managing Complexity in Implementation
Most barriers identified related to technology and sit within Opportunity and Capability COM-B components. These determinants could often be classified as clear benefitting from relatively straightforward implementation strategies to address them (e.g., providing equipment, providing training and support on how to use that equipment) with potentially predictable, linear outcomes. It may therefore be sensible to address these barriers first, before testing the feasibility of a telehealth intervention, to better ensure implementation outcomes are not impacting intervention outcomes. Notably, as four of the included telehealth interventions were implemented in the Global South, no papers addressed possible contextual determinants of underdeveloped digital infrastructure. This may be related to the high proportion of studies which already had inclusion criteria which resulted in digital exclusion, i.e., people in digital poverty could not access these therapies, or they were not implemented in under resourced areas. Broadening inclusion and augmenting sample diversity have been recommended in previous dementia telehealth reviews and would give a more rounded picture of telehealth implementation determinants (Liang & Aranda, 2023; Ye et al., 2025).
Conversely, telehealth intervention facilitators were mostly to do with the intervention itself and mainly sit within the Motivation COM-B component. These could be conceptualised as complex determinants, requiring more complex implementation strategies. For example, therapy engagement can be promoted by dynamically and creatively modifying therapeutic input to align with changing individual goals, circumstances, and relationships in line with dementia progression (e.g., Cowley et al., 2023; Rhodus et al., 2023). This aligns with the main themes of person-centredness and complexity, highlighted by the international expert consensus of the principles and philosophies for working with people with primary progressive aphasia (Volkmer, Cartwright, et al., 2023). It also aligns with the MRC guidance on developing complex interventions, which views interventions as dynamic and evolving within settings (Skivington et al., 2021). Complex implementation strategies, therefore, often lead to non-linear and less predictable outcomes, such as those addressing motivation. Moreover, the distinction between intervention components that promote motivation and motivational implementation strategies is not always clear. This distinction should be explicit when describing and testing interventions as well as when preparing for implementation
Understanding the type of problem increases the likelihood of identifying potential solutions. In healthcare management and implementation, policymakers and service providers have been criticised for mischaracterising complex problems, leading to inappropriate solutions that overlook the complexity, while concurrently overlooking clear problems that could more straightforwardly be addressed (Cottam, 2018; Glouberman & Zimmerman, 2002; Haynes & Loblay, 2024). Identifying potential barriers and enablers within settings and contexts by developing strategic and tailored implementation strategies is key to preparing for implementation. If clear implementation strategies have already been put in place it may impact complex determinants. For example, Knowledge and Resource domains may interact with the Social/professional role and identity domain. Social/professional role and identity contains determinants including therapists professional identity being challenged through not looking competent using technology, a determinant also identified in previous telehealth implementation literature (Oudbier et al., 2024). Prioritising technology provision (Resource) and training (Knowledge) may then impact downstream motivational determinants.
Many of the determinants identified in this review may not be unique to dementia interventions and appear broadly applicable across telehealth contexts and with other conditions. This highlights a paucity of determinants in the Memory, Attention, and Decision-Making domain, where more dementia-specific barriers might reasonably be expected. Finally, the limited use of implementation frameworks in designing and describing this set of telehealth interventions may contribute to a blurred boundary between determinants, potential implementation strategies and actual intervention components themselves. Greater use of implementation frameworks, and hybrid implementation–intervention designs, may help to better delineate this fuzzy boundary (Curran et al., 2012, 2022; Landes et al., 2019).
Strengths and Limitations
Environmental context and resource and Knowledge domains are commonly related to technology provision and use and have consistently been identified as determinants of telehealth intervention implementation (Borges do Nascimento et al., 2023; Oudbier et al., 2024). These domains are also predominately identified in TDF informed systematic reviews of interventions in healthcare (e.g., Mather et al., 2022; Shrubsole et al., 2023). Whilst it is possible that there is bias in the domains that the TDF foregrounds when used to analyse interventions, it also provides confidence in the current study’s methodology. This study made provision for potential bias by using the COM-B model in conjunction with the TDF.
No papers were excluded from the current study based on language. In reality, the search terms were in English, rendering it unlikely any non-English papers would be found. Indeed, only one paper not written in English was found (Yang et al., 2022) but the paper was screened out at the abstract/title stage as it was a meta-analysis. To improve equality, diversity and inclusion of studies in future systematic reviews, including search terms in languages other than English should be considered.
Restricting the review to papers published since 2018 may introduce bias, as most studies would have been conducted after the COVID-19 pandemic when there was a major shift in telehealth implementation. However, telehealth implementation changes are likely to be enduring, raising questions about the lasting relevance of some pre-pandemic implementation factors. Conversely, including a large number of pre-2018 papers would risk incorporating studies based on outmoded technology while overlooking factors related to videoconferencing, now a ubiquitous technology.
Only one researcher (RT) completed the quality assessment and inductive data coding. However, screening and data extraction was otherwise rigorously undertaken by multiple researchers providing strength and rigour.
Conclusion
This study highlights the importance of systematic reporting of telehealth interventions in dementia to reduce barriers to implementation. The use of theory enabled understanding of implementation determinants and how they may interact, and informed potential implementation strategy prioritisation. Most implementation barriers in telehealth dementia interventions were to do with technology. These barriers were often clear problems, relating to Capability and Opportunity. Most implementation facilitators were to do with the telehealth interventions themselves, relating to Motivation. Leveraging these facilitators is complex, requiring complex implementation strategies. Effectively managing complexity and unpredictability must be a key implementation goal for policymakers and clinicians when providing telehealth interventions for people with dementia.
Supplemental Material
Supplemental Material - Barriers and Facilitators to Implementing Synchronous Telehealth Interventions for People With Dementia - A Systematic Review
Supplemental Material for Barriers and Facilitators to Implementing Synchronous Telehealth Interventions for People With Dementia - A Systematic Review by Richard Talbot, Charlotte Harris, Esther Cable, Breege Whiten, Jason D. Warren, Rosemary Varley, Anna Volkmer in Dementia
Supplemental Material
Supplemental Material - Barriers and Facilitators to Implementing Synchronous Telehealth Interventions for People With Dementia - A Systematic Review
Supplemental Material for Barriers and Facilitators to Implementing Synchronous Telehealth Interventions for People With Dementia - A Systematic Review by Richard Talbot, Charlotte Harris, Esther Cable, Breege Whiten, Jason D. Warren, Rosemary Varley, Anna Volkmer in Dementia
Supplemental Material
Supplemental Material - Barriers and Facilitators to Implementing Synchronous Telehealth Interventions for People With Dementia - A Systematic Review
Supplemental Material for Barriers and Facilitators to Implementing Synchronous Telehealth Interventions for People With Dementia - A Systematic Review by Richard Talbot, Charlotte Harris, Esther Cable, Breege Whiten, Jason D. Warren, Rosemary Varley, Anna Volkmer in Dementia
Footnotes
Ethical Considerations
As a systematic review of previously published research, with no primary data collection or direct involvement of human participants, ethical approval and informed consent were not required. All data included in this review were obtained from publicly accessible sources. All original research retrieved adhered to ethical guidelines.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AV and RT are funded by AV’s National Institute for Health Research (NIHR) Advanced Fellowship (NIHR302240), CH is supported by the Alzheimer’s Society (AS-PhD-19a-006), RV is supported by a Leverhulme Research Fellowship (RF-2023-690\10), JDW has received funding support from the Alzheimer’s Society, Alzheimer’s Research UK, the Royal National Institute for Deaf People (Discovery Grant G105_WARREN), the NIHR University College London Hospitals Biomedical Research Centre, and The National Brain Appeal (Frontotemporal Dementia Research Studentship in Memory of David Blechner).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are openly available in the open science framework repository at https://osf.io/gkzjv/ DOI: 10.17605/OSF.IO/GKZJV (Talbot, 2025).
Supplemental Material
Supplemental material for this article is available online