
Abstract
The high prevalence of eating difficulties among nursing home residents living with dementia has a significant impact on their health and well-being. While various interventions have been evaluated to reduce eating difficulties and enhance nutritional intake, quantitative evaluation alone may not capture the full impact of the intervention given the trajectory of dementia. Following the implementation of a mealtime intervention, combining Spaced Retrieval with Montessori-based activities, 13 staff members who provided regular direct mealtime support to participating residents living with dementia were interviewed. Using a qualitative descriptive approach, individual semi-structured interviews were conducted. Thematic analysis guided the analysis and interpretation of the interviews. Three overarching themes represented the participants’ views: (1) Mealtime challenges, reflecting physical, cognitive, and behavioural impairments that hindered independent eating; (2) Individualised mealtime support, highlighting the critical role of person-centred strategies tailored to individual unique needs and abilities; and (3) Enhanced outcomes, describing improvements in eating independence, engagement, social interaction, mood, and self-esteem. Staff insights highlighted the importance of individualised, person-centred mealtime support grounded in a reablement approach. The specific challenges experienced by residents living with dementia should be proactively addressed when planning and implementing interventions. This intervention not only promoted eating independence but also enhanced psychosocial well-being, engagement, and mood. This emphasises the broad potential for such interventions to be integrated into daily clinical practice to improve both the quality of care and residents’ well-being and quality of life.
Keywords
Introduction
Internationally, approximately 57 million people are living with dementia, making it a global public health issue (World Health Organization, 2025). As dementia progresses, cognitive and functional abilities diminish, including activities of daily living, such as eating, mobility and toileting (Cipriani et al., 2020). This decline increase the likelihood of people transitioning to nursing home care (Cipriani et al., 2020).
People living with dementia often experience various eating-related difficulties, such as forgetting when to eat and how to use cutlery, difficulty recognising food items, limited attention span during mealtime and poor motor coordination (Fostinelli et al., 2020). These challenges contribute to reduced food intake, malnutrition, and weight loss, ultimately leading to deterioration in overall health, well-being, and quality of life (Perry et al., 2023). The prevalence of eating difficulties among people living with dementia is particularly high in nursing home settings, where up to 48% of residents experience eating difficulties (Ho et al., 2025). Mealtime independence and the quality of the mealtime experience are critical components of care for nursing home residents living with dementia (Aged Care Quality and Safety Commission, 2025). Being able to eat independently is not only essential for maintaining adequate nutrition but also supports dignity and autonomy, and reflects the individual’s life experience and cultural identity (Wang et al., 2024). Mealtimes offer more than just nutritional intake. They are important social and sensory experiences that evoke positive life memories, foster social engagement, and promote emotional well-being (Wang et al., 2024). Positive mealtime experiences have been associated with improved food intake, reduced agitation, and enhanced quality of life for people with dementia (Fetherstonhaugh et al., 2019). Therefore, promoting eating independence and creating meaningful, enjoyable mealtime experiences are increasingly recognised as core components of a reablement-focused, person-centred approach to dementia care. This approach aims to maintain and maximise an individuals’ remaining functional abilities and wellbeing (Lewis et al., 2021; Metzelthin et al., 2024).
Nursing home staff play a pivotal role in facilitating mealtime independence and creating supportive dining environments for residents living with dementia (Wang et al., 2024). Staff attitudes, behaviours, and approaches to care play a critical role in shaping residents’ mealtime experiences, either fostering self-eating independence or increasing dependence on staff assistance (Ataiza et al., 2022). Staff influence how meals are delivered, how residents are supported, and how mealtimes are experienced. Despite growing awareness of the importance of mealtime care, staff are constrained by barriers such as inadequate training, high workloads, staff shortages, and limited organisational support, which impede their ability to provide optimal mealtime assistance (Ataiza et al., 2022). Addressing these challenges requires a systemic commitment to embedding person-centred mealtime practices into the daily routines of dementia care.
To enhance eating independence and mealtime experiences for residents living with dementia, various strategies have been implemented and evaluated in nursing homes, including environmental and food modifications, staff training, and training for residents (Chang et al., 2023; Fetherstonhaugh et al., 2019). One approach that has gained increasing attention in recent years is the training of residents living with dementia using Spaced Retrieval to enhance procedural memory for eating and Montessori-based activities to promote motor skills relevant to eating (Chang et al., 2023). This approach has demonstrated positive outcomes in improving eating independence, food consumption, nutritional status, and the mental health of residents living with dementia (Lin et al., 2010, 2011; Wu et al., 2014; Wu & Lin, 2013). However, previous studies were primarily conducted in Asian cultural contexts and focused solely on eating with a spoon (Lin et al., 2010, 2011; Wu et al., 2014; Wu & Lin, 2013). Building on this evidence, the current study implemented a combined Spaced Retrieval and Montessori-based activities (SPREMON) intervention adapted to Western-style eating etiquette in the Australian nursing home setting (Yan, Drury, et al., 2025; Yan, Traynor, Alananzeh, et al., 2025a). This intervention drew on the conceptual framework of reablement to guide the way in which it sought to promote and optimise functional capacity and wellbeing (Lewis et al., 2021; Metzelthin et al., 2024). Quantitative measures of the impact of mealtime interventions provide an objective assessment of outcomes, such as nutritional intake, body weight, and eating difficulties. However, in residents living with dementia, the meaningful interpretation of quantitative findings is challenged by variable declines in cognitive and physical function. Therefore, qualitative investigations provide important additional insights into an intervention’s impact that cannot be captured in a quantitative evaluation alone. Given the essential role of staff in facilitating and sustaining such interventions and the need to explore qualitative perspectives, this paper examines staff experiences of the SPREMON intervention’s impact on residents living with dementia. Such insights offer critical qualitative insights into the intervention’s feasibility, acceptability, impact, and potential for broader implementation.
Methods
Design
This qualitative descriptive study is part of a larger mixed methods Doctoral project that co-designed and implemented a mealtime intervention, which combined Spaced Retrieval with Montessori-based activities for nursing home residents living with dementia (Yan, Traynor, Halcomb, et al., 2025b). The details of the intervention design and delivery have been reported elsewhere (Yan, Traynor, Alananzeh, et al., 2025a; Yan, Traynor, Halcomb, et al., 2025b).
This paper reports the findings from qualitative descriptive interviews conducted with staff following the intervention delivery. These interviews sought to explore staff experiences of providing mealtime care, their perceptions of the intervention, and its impact on residents living with dementia. A qualitative descriptive approach was chosen given its flexible, theory-neutral stance, which enables researchers to remain grounded in the data, making it ideal for studies requiring clear, straightforward descriptions of events or experiences (Doyle et al., 2020). The Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist was used to guide reporting (Tong et al., 2007).
Sample and Setting
The study was conducted in three nursing homes within the same organisation in a regional area of New South Wales, Australia. The nursing home manager appointed a designated champion to assist the researcher with participant recruitment. In this study, the champion purposively identified eligible staff. Potential participants were identified if they were employed full- or part-time by participating nursing homes for at least three months, worked with residents living with dementia and provided direct mealtime care services to residents who received the SPREMON intervention. This included both care staff (assistants in nursing (AIN)) and catering staff. The champion verbally informed potential participants about the study and provided copies of the participant information sheet, consent form, and demographic data sheet. Once the staff agreed to participate, the PhD candidate (ZY) contacted them individually to arrange an interview at a mutually convenient time. The consent form and demographic information sheet were returned to the PhD candidate (ZY) before the interview.
Braun and Clarke (2016) advocate a context-sensitive approach to sample size determination, suggesting that appropriate sample sizes can vary, depending on the study’s purpose, data richness, research question, and analytic framework. In this study, the sample size was constrained by the number of staff providing direct mealtime care for residents who received the full intervention (n = 8) (Yan, Drury, et al., 2025). This approach is consistent with qualitative scholarship, which recognises that saturation is not always appropriate or achievable in small, context-specific studies with a defined sampling frame (Braun & Clarke, 2013; Malterud et al., 2016). Instead, analytical adequacy was assessed through the coherence, depth, and recurrence of patterns within the data.
Data Collection
A semi-structured interview schedule was adapted from a previous study, which explored the implementation of a physical exercise program (Brett et al., 2018). The interview included three main open-ended questions: (1) Can you describe how you assisted residents with dementia during mealtimes? (2) Can you describe any changes you have noticed in eating behaviours or abilities after the completion of the SPREMON program? (3) Can you describe any changes in engagement and moods, or other behaviours in residents with dementia following the SPREMON program? Consistent with a semi-structured interview format, these questions were followed by probes and prompts to explore the responses. The PhD candidate (ZY) was aware that their experiences and involvement in the study could influence the data collection. Therefore, they consciously sought to ask open-ended questions and avoided prompts that may be perceived as leading during the interviews.
Interviews were conducted one week after the completion of the seven-week SPREMON intervention. This allowed participants time to observe any changes resulting from both the intervention and the period immediately following it. While this was a relatively short interval after study completion, it reflected changes that had occurred both during and after the intervention period and was chosen to fit within the study’s resources and to avoid staff and resident attrition. The interviews took place in private, quiet meeting rooms within the participating facilities to ensure confidentiality and minimise interruptions. The PhD candidate (ZY), a female registered nurse with experience in aged and dementia care and who had delivered the intervention, conducted interviews. Interviews were audio-recorded to facilitate verbatim transcription.
Data Analysis
Data were imported into Microsoft Word and analysed using the thematic analysis method described by Braun and Clarke (2022). First, all transcripts were read and re-read to gain a thorough understanding of the data. Two investigators (ZY and JZ) then developed initial codes to identify recurring patterns and meaningful segments within the data. This coding process led to the organisation of data. Subsequently, relevant extracts were examined in greater depth to generate overarching themes. The themes were then reviewed by all researchers and refined across the entire dataset to ensure they accurately captured participants’ experiences and aligned with the study aim. Next, each theme was clearly defined and mapped onto the initial categories, with representative quotations selected to illustrate each theme’s core meaning. Finally, the findings were presented alongside analytical commentary to highlight key insights and deepen understanding of the data.
Ethical Considerations
Ethical approval was obtained from the University of Wollongong Human Research Ethics Committee (approval number: 2023/268). Written informed consent was obtained prior to participation. Pseudonyms are used in reporting to maintain confidentiality.
Rigour
Credibility, dependability, confirmability and transferability were used to ensure rigour in this study (Lincoln & Guba, 1985). To enhance credibility, two researchers (ZY and JZ) independently coded a subset of transcripts and resolved discrepancies through discussion to ensure consistent interpretation. Data analysis was conducted by ZY and JZ using the approach described by Braun and Clarke (2022) to ensure the dependability of the findings. To strengthen confirmability, the research team documented analytic decisions and engaged in ongoing reflexive discussions throughout the analysis process. These discussions explicitly explored how the PhD candidates’ background and involvement in the intervention may have impacted their interpretations of the data. Detailed descriptions of the setting, participants, and intervention were provided to help readers evaluate the transferability of the findings.
Findings
Participant Characteristics
Participant Demographics
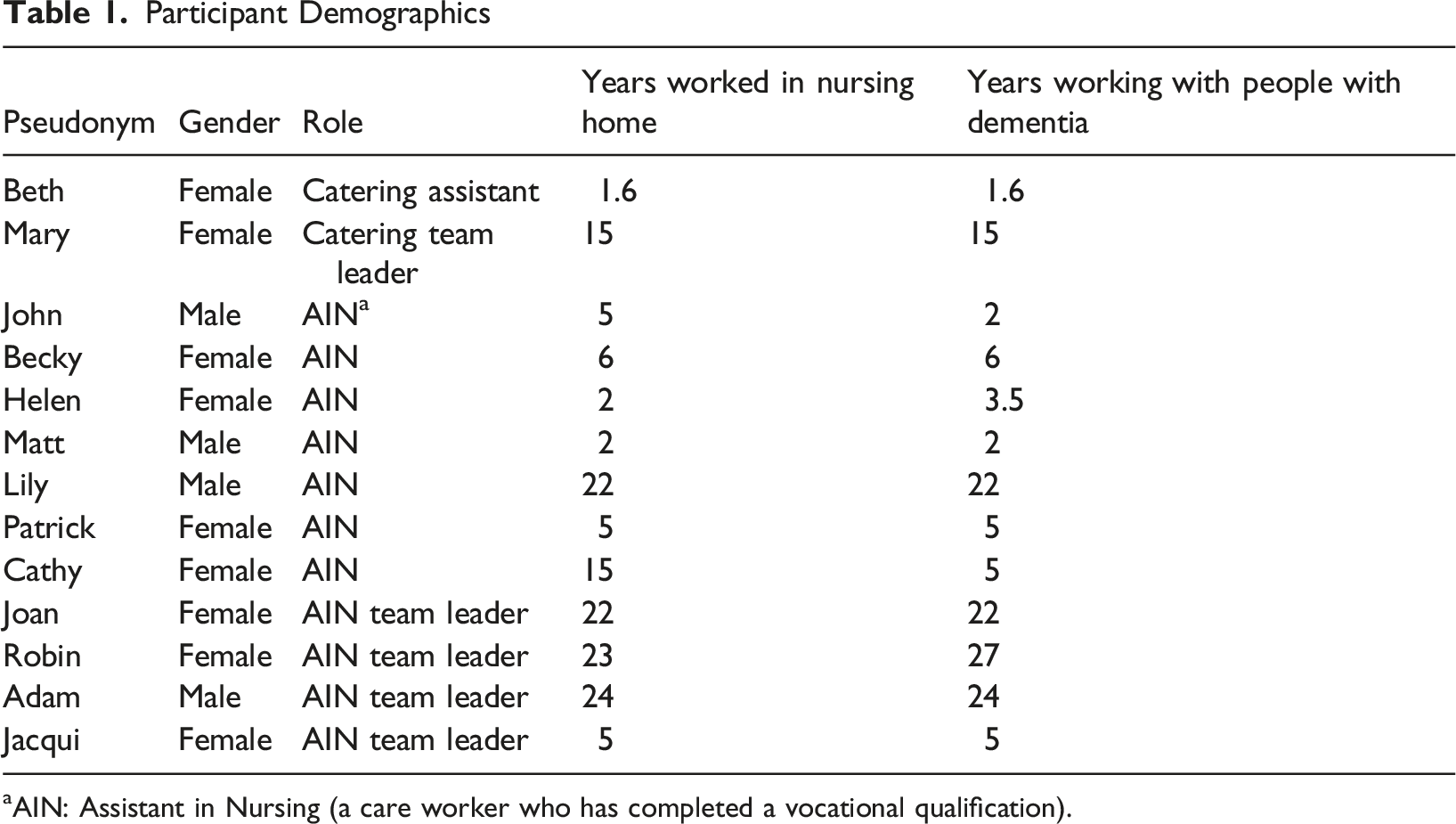
aAIN: Assistant in Nursing (a care worker who has completed a vocational qualification).
Themes
Three themes were established from data analysis: (1) mealtime challenges; (2) individualised mealtime support; and (3) enhanced outcomes.
Mealtime Challenges
Participants reported that the residents they cared for experienced physical, sensory, cognitive and behavioural issues that impacted their self-eating abilities and engagement in the intervention. Physical health issues such as arthritis and associated pain, lethargy, poor dexterity, and sensory impairments significantly impacted eating independence. “Because of the arthritis in her hand, she wasn't holding the cup very well.” (Joan) “She starts off pretty good. Towards the middle, towards the end, either she gets too tired, or she just can’t be bothered to feed herself.” (Jacqui)
Additionally, participants described how cognitive decline significantly affected residents’ independence in eating. Irritability, confusion and disorientation during mealtimes were described as impacting the use of cutlery and resulting in behaviours not conducive to nutritional independence. “She’s more confused now. Her cognitive decline is impacting upon her ability to gauge what utensils and how to use them.” (Adam) “She would get a bit confused, and … just play with the food instead of eating it.” (Becky) “She always cranky and sometimes moody, depending on how she feels on that day.” (Mary) “But with some of the residents who are a bit noisy…she gets angry and irritated a bit, she normally tells the other residents to like, be quiet, or like, sometimes some swear words at them.” (Helen)
Even with repeated eating procedural memory training delivered within the intervention, many residents were described as having limited capacity for focused attention during mealtimes and were readily distracted by people and the environment around them. “She gets distracted very quickly. She plays with the nails, she stretches, and then you have to remind her that your toast is in front.” (Adam) “She does lose a little bit of focus and zoom out sometimes.” (Beth)
These findings demonstrated that physical, sensory, cognitive, and behavioural challenges can significantly hinder eating independence in residents with dementia and should be considered when developing mealtime interventions.
Individualised Mealtime Support
Despite mealtime challenges, person-centred mealtime care was ensured by ongoing individualised support and encouragement from staff. Participants described how verbal encouragement during mealtimes was an important aspect of support. Joan explained that verbal encouragement “made them feel that they could still do something”. Matt stated that encouragement “gives them, like, a bit of sense of achievement… makes them feel like they’re not useless”. Such encouragement validated the individuals’ engagement with meals and promoted efforts at future meals. “But if you see if they like eat the whole meal, we just encourage them: ‘Good job’, ‘well done’ ‘You should be proud of yourself’… Something like that. Then that gives them a nice smile, so then it encourages them to eat more for the next meal.” (Matt) “Yes, after they are finishing their meal, we are thanking them and saying that you have really done well, and ensuring they have finished their drink and dessert too.” (John)
Key to providing effective mealtime support was staff knowledge of the individual with dementia and their determination to create a positive mealtime experience for this cohort. Robin stated, “we know which resident needs a little bit of assistance”. With in-depth personal knowledge, participants described how they gauged individual needs and make informed judgments about when to assist during mealtimes. “We set her up with the plate in front of her, with the cutlery that's available for her dexterity, so it sets it up for independent eating.” (Patrick) “We just give her some props. Verbal prompts. Putting the food in front of her. Handing her the fork. Might have to cut up some of the food into a bite size. And then she can actually feed herself with a little bit encouragement.” (Lily)
As part of providing individualised mealtime care, staff were conscious of the need to account for the individuals’ sensory deficits, physical limitations, and varying stages of dementia during mealtimes. “You do have to, you know, be quite loud and speak right into her ear, otherwise she won't hear.” (Beth) “She will need help cutting the meat and stuff because of a limitation of her arms.” (Matt) “We set her up with the cutlery that’s available for her dexterity. So, it sets it up for independent eating. We do provide the cutlery with the wider handles.” (Patrick)
These findings highlight that an in-depth understanding of individual residents’ preferences, abilities and limitations is essential to support independence.
Enhanced Outcomes
Participants described improved mealtime experiences and observed various changes in the residents with dementia following the intervention. Participants observed some residents having become more focused and engaged in eating. Patrick explained how one person was “paying more attention to what’s in the bowl, like her meal, like how many vegetables she’s eating. Whereas before, …she was just sitting there with her mouth open,.. now she’s sort of looking in more, a little bit engaging.”
Many other participants highlighted improved self-eating abilities, as demonstrated by greater confidence using cutlery, consuming more food, being less likely to pick at or play with their food, and making greater efforts to eat independently. “She seems a bit more confident with the cutlery like she’ll instantly… like pick up the knife and fork and go to and cut.” (Becky) “She eats better without so much prompting or less encouragement just to set the meal up for and she can start.” (Adam) “She has come leaps and bounds since doing your program the way that she's eating now, compared to the way that she was before. She's much more consistent. Yes, she's not picking and playing with the food. She's actually utilising her cutlery more. She's picking up her cup. She's taking regular mouthfuls of water.” (Jacqui) “Prior to this training, she wouldn't even make an attempt. She would just leave the spoon there, and waiting for staff to come along and start feeding her. But because of this training, she's starting to do it on her own before staff get there, and some of the time, she's pretty much fed her meal the whole way through.” (Patrick)
However, the intervention outcomes extended beyond nutrition and the eating process. Participants observed increased social interaction and engagement following the intervention and described residents with dementia leaving their rooms more often, increasing interactions with peers, and participating in more activities. “She's just coming out of her room more often.. there were long periods of time where she wasn't coming to the dining room, but now she's really trying to come to the dining room more often.” (Patrick) “Since the Montessori program, we’ve done with her, She's a bit more social. Yeah, that's going walking around, meeting people, seeing people.” (Cathy) “And because she's been involved in activities with you, we found that she's actually been more social with other people, so the other residents and her are actually have conversations now, whereas prior to that, she was very quiet. Now, she's more than happy to be vocal……So it's built confidence in her, which is great.” (Jacqui)
Participants also expressed how the intervention promoted residents’ self-esteem, mental health, and cognitive function. “It's really helped her self-esteem and her mental capacity. I think, which is really great!” (Cathy) “They feel in control. Yeah, they feel very fulfilled that they've done something.” (Robin) “And then when they come for lunch, they just eat a lot of more of the food, because they they’re so happy on what they accomplish, but they reckon they can accomplish eating their meal as well. And we're very happy that you’re doing this program.” (Matt)
Discussion
This study has provided unique insight into staff experiences of caring for residents living with dementia who participated in a mealtime intervention. The findings offer insights into the impacts staff observed on residents’ eating behaviours, emotional well-being, and autonomy following the intervention. These findings add greater depth and breadth to the quantitative findings on the intervention’s impact (Yan, Drury, et al., 2025). Staff feedback plays a vital role in assessing intervention feasibility, acceptability, and sustainability in everyday care practice, especially in the context of dementia care, where personalised support is critical (Steinskog et al., 2021). By highlighting staff perspectives, this study provides evidence on changes in resident behaviour, the value staff placed on resident outcomes, and future considerations for refining the intervention for real-world practice and shaping caregiving approaches during mealtimes. It also demonstrates the need for staff to be sufficiently trained to recognise issues affecting functional capacity, to understand how Spaced Retrieval and Montessori-based activities can be integrated into daily care and address complex health needs.
Participants’ experiences highlighted that physical, cognitive and sensory issues can negatively impact the independent self-eating abilities of residents living with dementia. Previous research has also identified a range of factors that influence eating independence and contribute to increased dependence on carers, including physical function (e.g., grip strength), performance in activities of daily living (e.g., feeding), mental health conditions (e.g., depression), and the level of cognitive impairment (Chang et al., 2017; Jung et al., 2021; Liu et al., 2024). Notably, comorbidities and physical function were the two key determinants that affected independent eating among this population (Jung et al., 2021). These findings suggest that managing physical and sensory limitations, such as arthritis or vision impairments, may help maximise individuals’ functional capacity. By doing so, we may optimise the functional capacity of residents living with dementia and also enhance their engagement with and adherence to intervention activities. Participants reflected that while the intervention facilitated improvements, residents with physical, cognitive and sensory issues still required tailored support strategies. While this intervention did not incorporate formal functional assessments, future interventions should consider how such assessments and clear care planning can help ensure that care staff are supported to optimise functional outcomes. Additionally, this finding highlights the need for staff training and clearer policies for assessing the functional status of nursing home residents and implementing interventions to promote functional independence and dignity.
This study demonstrated that care staff had individualised knowledge of residents living with dementia that they applied to their care to meet individual needs. Knowing residents well lays the foundation for building therapeutic relationships between staff and residents (Keady & Nolan, 2020). This personalised understanding empowers staff to tailor mealtime support by considering each resident’s preferences, cognitive abilities, and physical limitations. This finding is consistent with Liu et al. (2022) who reported that staff who adopted person-centred mealtime support strategies significantly improved food intake and mealtime behaviours. The impact of staff knowledge highlights the important role of staff in tailoring intervention implementation to suit individual needs. These findings underscore the vital role of staff knowledge in facilitating knowledge translation and ensuring the successful implementation of evidence-based practices.
Participants in this study described improved eating abilities and increased self-feeding initiation among residents living with dementia following the implementation of the SPREMON intervention. These enhancements included more effective use of cutlery and cups, increased attention and engagement during meals, and greater independence in initiating eating. Such findings add a valuable qualitative dimension to quantitative improvements in eating behaviours that must be considered when evaluating the intervention. Previous studies, conducted within an Asian cultural setting, have reported statistically significant improvements in eating abilities and nutritional status following either Spaced Retrieval or Montessori-based activities individually (Lin et al., 2010, 2011) or their combined use (Wu et al., 2014). However, the current study offers a deeper insight into how eating abilities were enhanced. By demonstrating the positive changes in eating behaviours, this study has provided a deeper insight into the impacts of the SPREMON intervention that would not be evident from quantitative evaluation alone. Given the challenges inherent in interpreting quantitative outcomes in dementia, particularly the downward trajectory of the condition, qualitative insights are essential for capturing the intervention’s true impact on participants (Beattie et al., 2025). However, the modest sample size of residents living with dementia who received the complete intervention (Yan, Drury, et al., 2025), makes it difficult to draw conclusions about the differences in response between participants.
In this study, participants described that the outcomes of the SPREMON intervention extended beyond simply improvements in eating abilities and self-feeding initiation. The intervention was also perceived to positively influence engagement, mood (affect), mental health, and other aspects of well-being. These findings are consistent with previous studies reporting a reduction in depressive symptoms (Wu & Lin, 2013) and significant improvements in positive mood and activity engagement following the intervention (Giroux et al., 2010). The rich qualitative data revealed that residents appeared more confident, happier, and more satisfied with their lives. Participation in activities fostered self-esteem, a sense of control, and personal fulfilment. Social engagement was identified as a fundamental human need, essential for maintaining social connections, reducing loneliness, and supporting both mental and social well-being for residents with dementia (Bethell et al., 2021). These findings reinforce the value of nursing homes providing person-centred care, such as tailored, purposeful, and meaningful activities, that improve both functional abilities (eating) and broader aspects of holistic wellbeing as part of routine care (Bethell et al., 2021). Integrating psychosocial components into routine care is therefore crucial for delivering person-centred dementia care, recognising that meaningful engagement is not only beneficial but also an essential human need. This was achieved by intentionally integrating structured, purposeful, and meaningful activities into everyday care routines, enabling residents living with dementia to remain socially connected, engaged, and valued in the community.
Limitations
This study has some limitations. Firstly, it focused exclusively on staff experiences, without exploring the perspectives of residents with dementia and their family members. This focus was chosen, given that staff play a critical role in delivering daily care, observing and reporting on changes in residents’ behaviours, abilities, and other aspects throughout the intervention. Secondly, many residents with dementia experience communication difficulties due to cognitive impairments that limit their ability to articulate their thoughts, feelings, or experiences of an intervention. As such, staff serve as valuable informants who can provide insights into the intervention’s impact. Furthermore, because the intervention was delivered in a single organisation across multiple sites, staff views may differ across organisations. Additionally, as the staff were aware that the intervention had been delivered by the researchers in their facility, this may have led to some positive reporting bias. The relatively small sample of residents living with dementia who completed the study also limits the ability to assess impact across the participant group (Yan, Drury, et al., 2025). However, examples provided by participants referred to a cross-section of residents involved in the study. Finally, interviews were undertaken in a relatively short time frame following intervention completion. While this was undertaken to fit in the study resources and reduce participant attrition, it would not capture longer-term outcomes or the sustained intervention effect. Future studies are encouraged to be larger-scale, multi-facility studies that explore short, medium, and longer-term outcomes, thereby enhancing generalisability and allowing further examination of contextual factors influencing implementation and outcomes.
Conclusion
Maintaining mealtime independence and creating positive mealtime experiences are critical for residents living with dementia. Staff participants provided valuable insights into how the SPREMON intervention affected not only eating behaviours but also engagement, mood, and mental and psychological health. These findings underscore the broad potential benefits of Spaced Retrieval and Montessori-based activities for people living with dementia and highlight implications for practice and education. Future research is recommended to assess the intervention’s effectiveness with larger sample sizes and across more diverse care settings. Additionally, including the perspectives of multiple stakeholders, such as people with dementia and their families, can provide deeper insight. However, this intervention offers a potential strategy that can be implemented by nursing homes to support residents with dementia to thrive in the nursing home setting.
Footnotes
Acknowledgements
We sincerely appreciate Warrigal Nursing Home and the staff and residents who were involved in this research project. Special thanks to Mr. Shiva Gopalan for his guidance as my industry supervisor and to Professor Victoria Traynor for her mentorship during the early stages of this project.
Ethical Considerations
Ethical approval was obtained from the University of Wollongong Human Research Ethics Committee (approval number: 2023/268).
Consent to Participate
Written informed consent was obtained from all participants. To protect confidentiality, pseudonyms were used in all transcripts and reports.
Author Contributions
Zhoumei Yan, Joel Zugai, Peta Drury, Ibrahim Alananzeh, and Elizabeth Halcomb contributed to the methodology, software, validation, formal analysis, resources, data curation, manuscript review and editing. Zhoumei Yan, Peta Drury, and Ibrahim Alananzeh contributed to the conceptualisation of the study. Elizabeth Halcomb, Peta Drury, Ibrahim Alananzeh and Joel Zugai provided supervision for the project. Zhoumei Yan, Joel Zugai and Elizabeth Halcomb drafted the original manuscript. Zhoumei Yan conducted the data collection and led the manuscript development. All authors approved the final version of the paper.
Funding
This research was conducted as part of a Doctoral project supported by the Commonwealth through an Australian Government Research Training Program Scholarship [![]() ] awarded to Zhoumei Yan. Zhoumei Yan also received a stipend from the China Scholarship Council. Apart from the PhD scholarship, no other external financial support was received for this research.
] awarded to Zhoumei Yan. Zhoumei Yan also received a stipend from the China Scholarship Council. Apart from the PhD scholarship, no other external financial support was received for this research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Generative AI Use
Generative AI was used solely for grammar and spelling checks in the preparation of this manuscript.