
Abstract
Non-pharmacological therapies have demonstrated efficacy in alleviating dementia-related symptoms in residential aged care settings; however, their uptake remains limited. This systematic review aimed to identify the barriers and facilitators influencing the implementation of non-pharmacological therapies for people with dementia in residential aged care, with the goal of informing future research, practice and policy development. A systematic search was conducted across seven databases (PubMed, MEDLINE, PsycINFO, EMBASE, CINAHL, Cochrane Central Register of Controlled Trials, ProQuest) from January 2000 to March 2025. Studies were eligible for inclusion if they were published in English, involved participants aged 65 years and older with dementia residing in aged care facilities, and reported on implementation challenges or enablers related to non-pharmacological interventions. Three independent reviewers conducted screening, data extraction, and quality appraisal, with discrepancies resolved through consensus. The Mixed Methods Appraisal Tool was used to assess study quality. Data were synthesised using the Theoretical Domains Framework. Fifty-eight studies met inclusion criteria, representing 11 types of non-pharmacological therapies. The majority were qualitative in design (36/58; 62.1%). Music therapy (20/58; 34.5%) and recreation therapy (16/58; 27.6%) were the most studied. Key barriers and facilitators included staff availability (48/58; 82.8%), education and training (49/58; 84.5%), resource availability and cost (34/58; 58.6%), program usability (38/58; 65.5%), and organisational policy structures (34/58; 58.6%). There was no clear pattern in the type of barriers or facilitators reported by therapy type. Improving staff capacity, increasing access to training, ensuring resource availability, and designing flexible and user-friendly programs are critical to enhancing the successful adoption of non-pharmacological therapies in aged care. Addressing these factors may contribute to more sustainable and effective dementia care practices.
Introduction
Dementia is a progressive, neurodegenerative syndrome marked by a gradual deterioration of cognitive capacities, increasingly impairing an individual’s ability to communicate, comprehend, and effectively convey their needs (Cerejeira et al., 2012; Gustafson, 1996). As dementia advances, the individual’s capacity to articulate internal states becomes increasingly compromised, often manifesting in a spectrum of changed behaviours encompassing affective, psychological, and behavioural disturbances (Cerejeira et al., 2012; Health, 2013; Samtani et al., 2023). Changed behaviours in people living with dementia are best understood through a person-centred and strengths-based lens and reflects the ongoing interaction between the individual’s cognitive abilities, capacity to communicate internal experiences, and the environmental and social context in which care is provided (Au-Yeung et al., 2024; Molony et al., 2018; Power, 2015). Through this lens, changed behaviours are not solely viewed as disease symptoms. Rather, experiences such as agitation, withdrawal, apathy, sleep disturbance, and emotional distress are often viewed as meaningful responses to unmet needs, environmental stressors, changes in routine, or barriers to self-expression (Au-Yeung et al., 2024; Power, 2015). Regardless of their origin, changed behaviours profoundly affect both the individual and those providing care, exacerbating caregiver burden, inflating healthcare expenditure, and diminishing overall quality of life (Cerejeira et al., 2012; Health, 2013). While the severity and prevalence of changed behaviours vary according to disease progression, the inability to adequately respond to them at home is commonly experienced (Health, 2013; Steele et al., 1990). In Australia alone, as of 2019–2020, an estimated 244,000 individuals live in residential aged care settings (Welfare, 2024).
To guide evidence-based intervention in residential aged care settings, national dementia care guidelines in Australia advocate for the prioritisation of non-pharmacological interventions as the first-line approach to reduce environmental stressors and dementia-related behavioural and psychological changes associated with dementia (Deudon et al., 2009; Dyer et al., 2018). Non-pharmacological interventions are defined as structured interventions that do not involve pharmacological agents but are designed to enhance the psychosocial, physical, and environmental contexts to better meet the needs of individuals with dementia (Douglas et al., 2004). These interventions commonly include sensory stimulation, reminiscence, therapeutic use of music, art, or dance, among others (Deudon et al., 2009; Dyer et al., 2018). They also include rehabilitation and reablement approaches provided by allied health professionals, such as physiotherapy, occupational therapy, and tailored exercise programs, each aiming to support or restore physical function, independence, and quality of life in residential aged care settings (Poulos et al., 2017). Numerous studies and clinical guidelines indicate that such interventions, delivered by multidisciplinary teams, address not only behavioural and psychological changes associated with dementia but also have an important role in maintaining functional capacity, promoting wellbeing, and reducing reliance on pharmacological treatments (Berg-Weger & Stewart, 2017; Poulos et al., 2017; Foong et al., 2022). For example, music therapy has demonstrated measurable benefits for cognition and mood (Moreno-Morales et al., 2020), while physical rehabilitative efforts led by allied health professionals are recognised as essential for enabling independence and supporting daily living (Poulos et al., 2017). However, despite their established efficacy and their centrality in current clinical guidelines, the implementation of non-pharmacological interventions in residential aged care remains inconsistent and underutilised.
This incongruity between best practice recommendations and real-world implementation is particularly concerning given evidence of inappropriate reliance on pharmacotherapy. Current guidelines stipulate that pharmacological measures should be reserved for severe cases where individuals pose an imminent risk to themselves or others (Deudon et al., 2009; Dyer et al., 2018), yet in practice, psychotropic medications are frequently overprescribed. Indeed, an Australian Senate inquiry reported that only one in five individuals prescribed antipsychotic medications in residential aged care had a clear clinical indication for such treatment (Cerejeira et al., 2012; Committee, 2014).
Multiple systematic reviews have affirmed the efficacy of non-pharmacological interventions in mitigating the symptoms associated with dementia, particularly when interventions are individualised and embedded within multicomponent programs tailored to resident preferences (Burgener et al., 2008; J. Cohen-Mansfield et al., 2012; Deudon et al., 2009; Dyer et al., 2018). Nevertheless, the implementation of non-pharmacological interventions is impeded by the complex operational frameworks of aged care services, where systemic constraints, such as staffing limitations, regulatory requirements and institutional routines, can hinder the successful adoption of new care models (Bourbonnais et al., 2020).
Applying an implementation science perspective in dementia care is essential, particularly given the persistent gap between research evidence supporting non-pharmacological interventions and their limited routine use in residential aged care settings. Implementation science is an emerging field focused on understanding and addressing the multi-level factors that influence the uptake, adoption, and sustainability of evidence-based healthcare interventions. Systematic reviews that examine barriers and facilitators to implementation, rather than efficacy alone, are needed to support practice change and knowledge transfer, and to ensure that evidence-based interventions achieve real-world impact (Bauer et al., 2015).
In this systematic review, we adopted the Theoretical Domains Framework, a widely used synthesis tool in implementation science, which provides an integrated lens to identify and categorise determinants of implementation across cognitive, affective, social, and environmental domains (Atkins et al., 2017). By using the framework to guide data extraction, analysis, and synthesis, we aimed to build a systematic understanding of the practical barriers and enablers influencing the implementation of non-pharmacological interventions in dementia care. This approach supports the translation of research evidence into routine practice by identifying actionable targets for intervention development, staff education, and organisational change.
This systematic review was designed to comprehensively characterise non-pharmacological interventions for dementia in residential aged care, and to evaluate key implementation outcomes including barriers, facilitators, acceptability, feasibility, and sustainability. Although our review included elements typical of scoping reviews (such as broad mapping of intervention and implementation characteristics), we employed systematic review procedures: a registered protocol, formal eligibility and appraisal, and structured synthesis using the theoretical domains framework. We made this choice to ensure transparency, rigour, and applicability of outcomes for aged care stakeholders requiring both breadth and methodological robustness. Our approach aligns with recent calls (e.g., Munn et al., 2018) to broaden systematic reviews in health services research to better inform future research, practice, and policy development by reporting on intervention types, modalities, targets, program components, and context alongside implementation challenges. In doing so, this review contributes to the broader imperative of promoting person-centred, non-pharmacological approaches that uphold the dignity and wellbeing of individuals living with dementia in residential aged care settings.
Methods
Search Strategy
A systematic search of electronic databases was conducted in December 2022 across PubMed, MEDLINE, PsycINFO, EMBASE, CINAHL, Cochrane Central Register of Controlled Trials and ProQuest. The search was limited to English articles only. Government reports and other grey literature were searched using Google Scholar. Guided by a clinical librarian, the search strategy incorporated MeSH search terms and is included in Appendix A. These search terms were connected with the appropriate Boolean operators (e.g., AND, OR). An updated search was conducted in March 2025.
Eligibility Criteria
This review focused on primary research which assessed the barriers and facilitators to non-pharmacological intervention implementation in residential aged care settings for individuals with dementia. Peer reviewed articles published from 1 January 2000 to 20 March 2025 were included to ensure relevance and up to date evidence. Articles were included if they involved participants who were: (1) self or medically diagnosed with dementia or fit the criteria for dementia, (2) individuals who received the intervention were aged over 65 years old or staff participants aged over 18 years old, (3) living in residential aged care settings and (4) undertaking or delivering non-pharmacological therapies. Non-pharmacological therapies were defined as any sort of intervention not directly involving the use or delivery of medication and attempting to optimise an individual’s need or management of dementia-related symptoms (Douglas et al., 2004). These included agitation, irritability, depression, delusions, sleep and appetite changes and apathy. Publications which did not assess the barriers and facilitators to the implementation of an intervention were excluded. Publications which consisted of evaluations of decision tools (e.g., decision trees) for interventions were also excluded. Literature reviews, study protocols, theoretical papers, conceptual papers, and position papers were also excluded from the review.
Study Selection
One researcher (EG) screened titles and abstracts for duplicates in Endnote and eligibility in Rayyan, with an additional reviewer (JS) randomly reviewing 10% of the initial articles. Subsequently, two researchers (EG and JS) independently evaluated each article for full text inclusion. Any disagreements were resolved through discussion or by involving a third reviewer (MA).
Data Extraction
Three reviewers (EG, JS, SS) independently extracted relevant data from publications using a created standardised table including details on study design, participant demographics, non-pharmacological intervention type, organisation characteristics, resident characteristics and factors identified (e.g., barriers and facilitators). Data extraction was recorded in Word. Included studies were grouped based on the type of intervention and the targeted management goal of each intervention.
Quality Assessment
Two reviewers (EG, HA) independently assessed the quality of full text inclusion articles using the Mixed Methods Analysis tool (MMAT) (Hong et al., 2018), which is a comprehensive framework for evaluating and screening research studies, allowing for the inclusion of both quantitative and qualitative papers. Any disagreements were resolved through a third reviewer (JS).
Data Synthesis
Data were synthesised using the Theoretical Domains Framework as a basis for evaluation of barriers and facilitators to the implementation process (Atkins et al., 2017). This framework is a comprehensive and widely used framework in healthcare research, particularly in implementation science (Atkins et al., 2017). Factors which could influence the implementation process were coded according to the framework relevant domains and further adjusted systematically dependent on data extraction (e.g., staff related factors, education, resourcing, policy and procedures, flexibility, mindset/attitudes, usability, and accessibility). These elements were systematically coded to identify barriers and facilitators affecting both staff and individuals with dementia. Definitions for each barrier and facilitator were established based on the literature (Léegaré & Zhang, 2013) and expert consensus in the team. Data extraction involved initial categorisation of barriers and facilitators from the included studies followed by a subsequent synthesis process within the research team to analyse and interpret the extracted data. For qualitative studies, frequency in which factors are reported according to each domain was recorded. For quantitative studies, the significance of any associations between a factor and a measure of implementation by the domain was reported. For acceptability scoring, if studies used validated scales, we reported the rating according to the scale thresholds (eg, >70% agreement classified as high) according to prior literature (Siette et al., 2023). For qualitative studies, feasibility and acceptability ratings were based on how participants described the appropriateness and practicality of the intervention. The overall “high acceptability” classification reflected participants’ willingness and ability to use the intervention within the study context. Barriers and facilitators were also coded for differences between staff and residents. Two authors independently coded the data (EG, HA) from the studies and compared for inconsistencies and were resolved by a third member on the research team (JS) if any were apparent.
Results
Study Selection
The search identified a total of 4,066 potentially relevant studies across all databases. After screening of titles and abstracts, 181 papers were identified for full-text review and of those, 58 papers met the selection criteria. The PRISMA flow diagram for the study selection process and reasons for exclusion are illustrated in Figure 1. PRIMSA flow diagram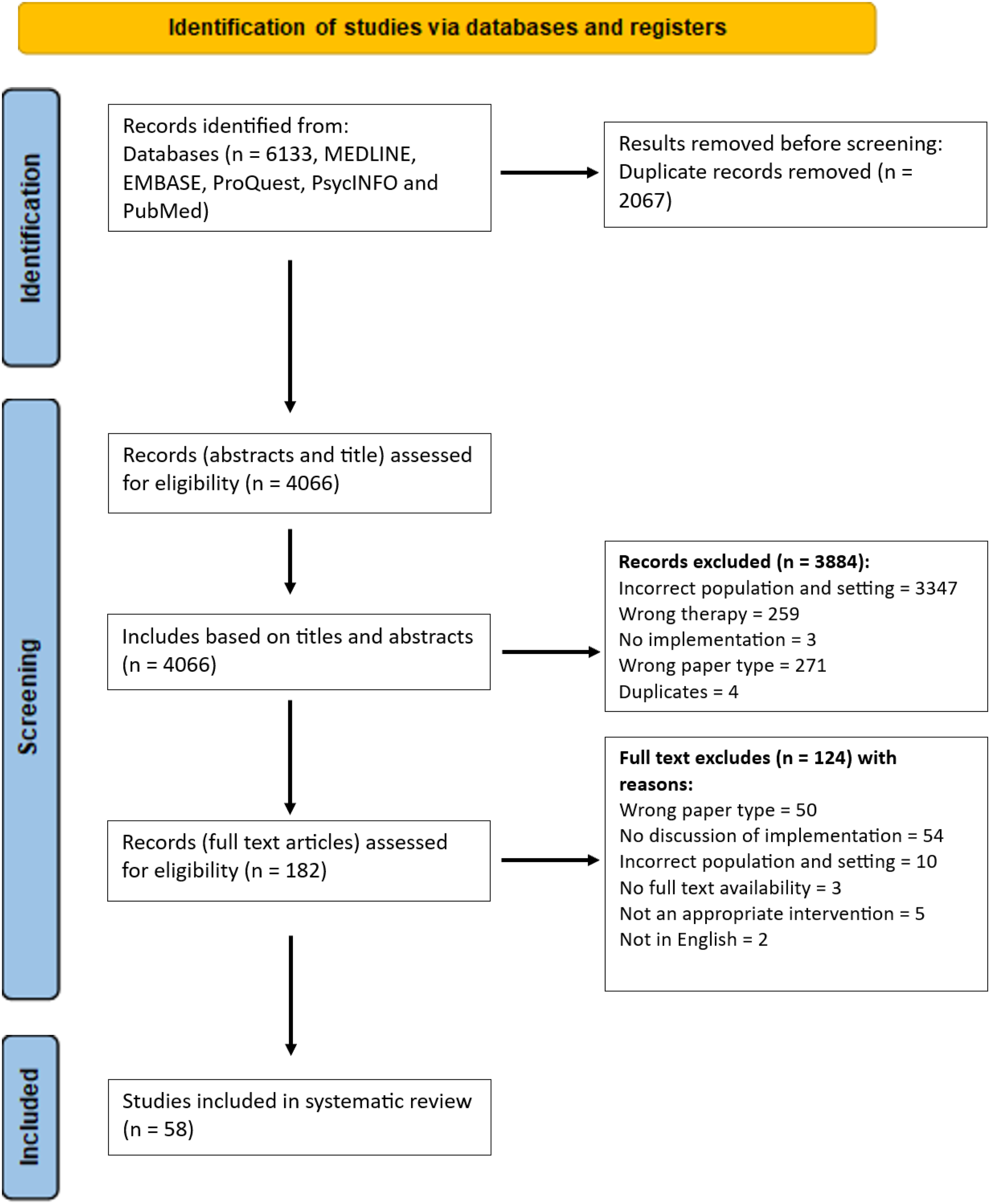
Study Characteristics
Characteristics of Included Studies (n = 58)
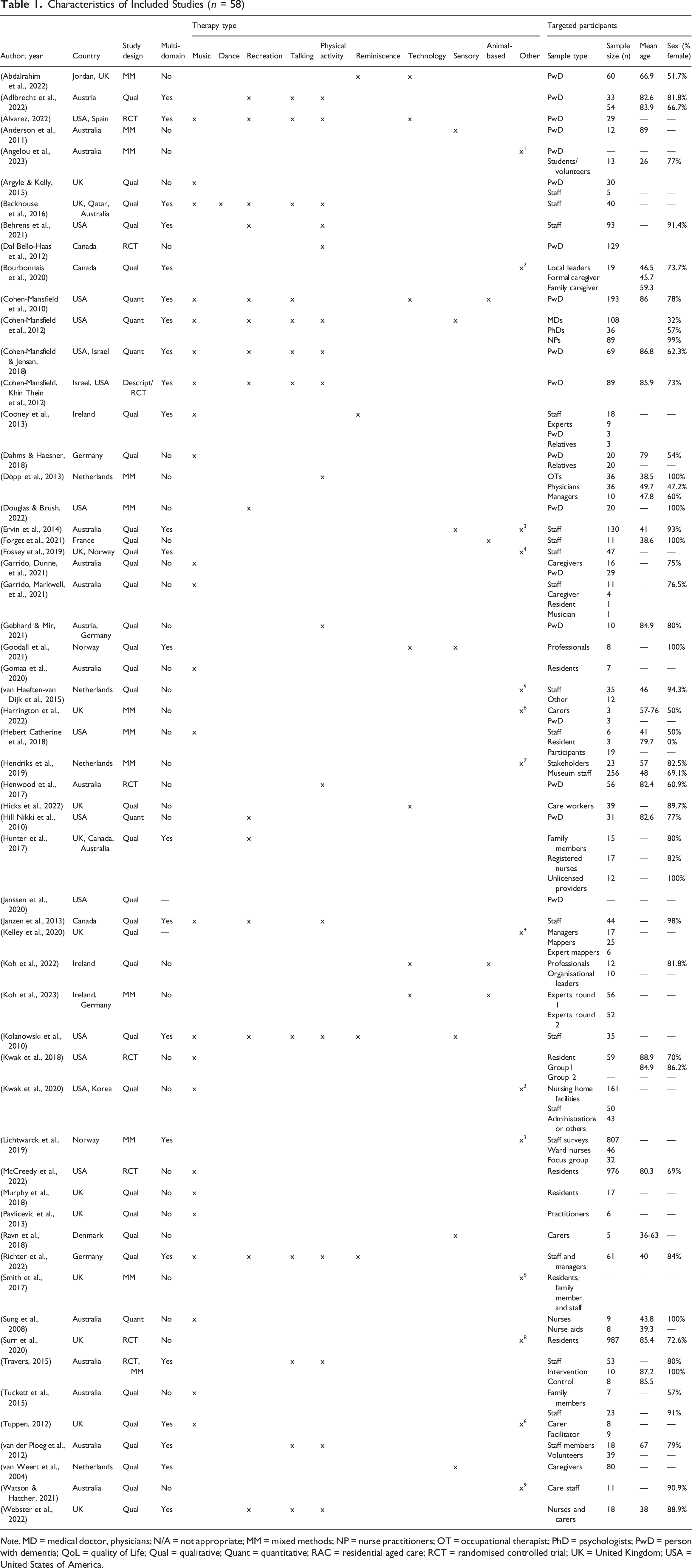
Note. MD = medical doctor, physicians; N/A = not appropriate; MM = mixed methods; NP = nurse practitioners; OT = occupational therapist; PhD = psychologists; PwD = person with dementia; QoL = quality of Life; Qual = qualitative; Quant = quantitative; RAC = residential aged care; RCT = randomised controlled trial; UK = United Kingdom; USA = United States of America.
Studies were primarily conducted in the USA (14/58; 24.1%), UK (14/58; 24.1%) and Australia (14/58; 24.1%). Other countries include Canada (4/58; 6.9%), Germany (4/58; 6.9%) and the Netherlands (4/58; 6.9%).
Included articles had a variety of participants, including residents with dementia, their families or primary caregivers, and care home staff or volunteers, or a combination. The most common study cohort, the primary group of participants, was staff members (27/58; 46.6%), this included studies that evaluated education or training-focused interventions for staff, as well as studies in which staff provided data through interviews, surveys, or focus groups regarding the implementation and outcomes of the non-pharmacological interventions.
Interventions
Summary of Program Characteristics
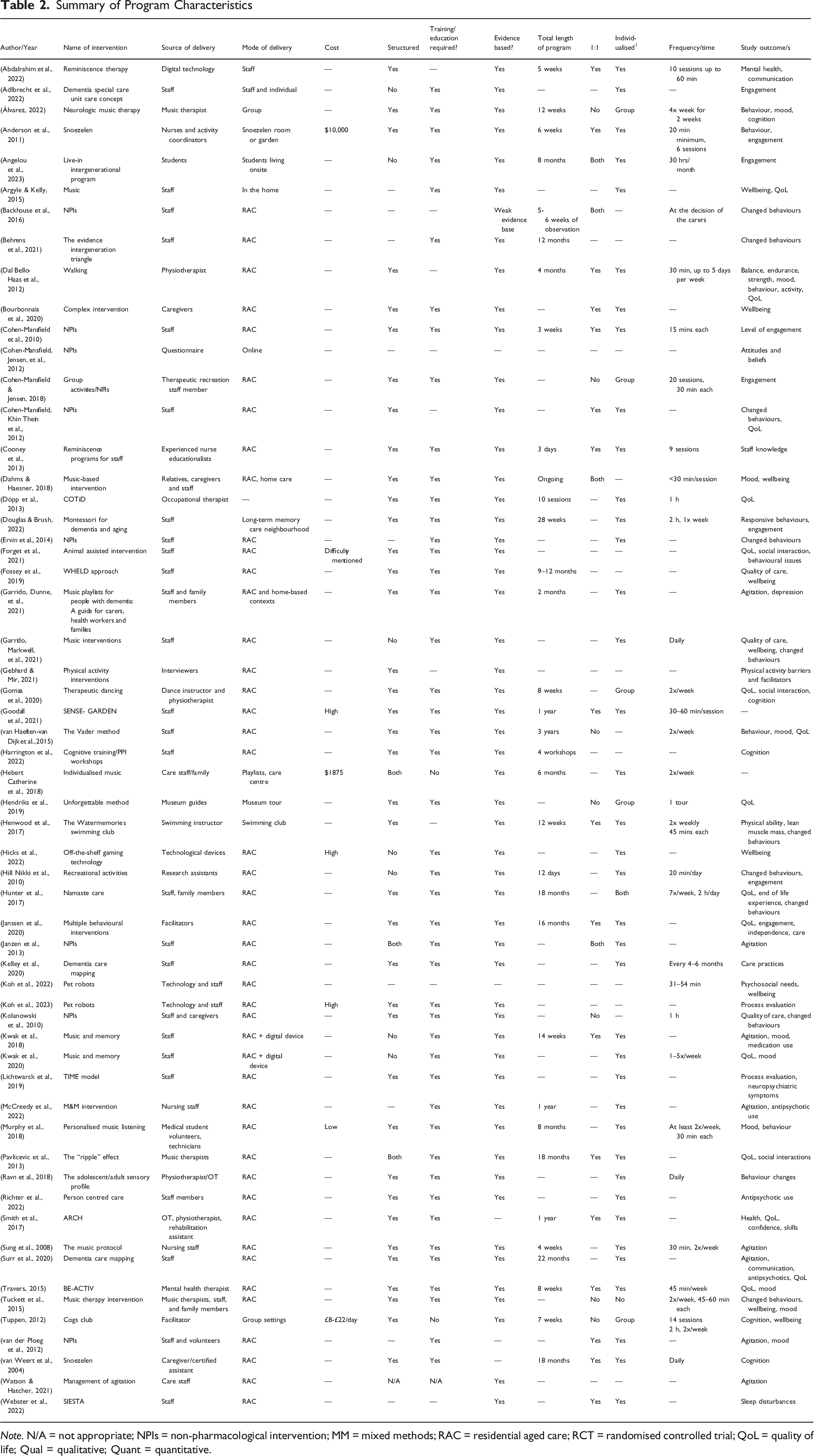
Note. N/A = not appropriate; NPIs = non-pharmacological intervention; MM = mixed methods; RAC = residential aged care; RCT = randomised controlled trial; QoL = quality of life; Qual = qualitative; Quant = quantitative.
In general, most interventions were structured with set programs and procedures, and individualised (40/58; 69.0%), while 31.6% were conducted on a one-to-one basis. Structured interventions with set programs and procedures include interventions with a set timetable for individuals or group therapies. The majority (52/58; 89.7%) of these programs were evidence-based. Additionally, 79.3% of interventions required prior training or education for delivery and use. Over 41% of studies (24/58) did not report on intervention duration. Of those that did report, interventions ranged from 3 days to ongoing.
The primary focus of these non-pharmacological interventions was to target changed behaviours and agitation. Additional outcomes addressed included cognition, engagement, sleep patterns, quality of life, mood, and behavioural changes.
Acceptability and Feasibility
Perceived Acceptability and Feasibility and Reported Fidelity of the Program
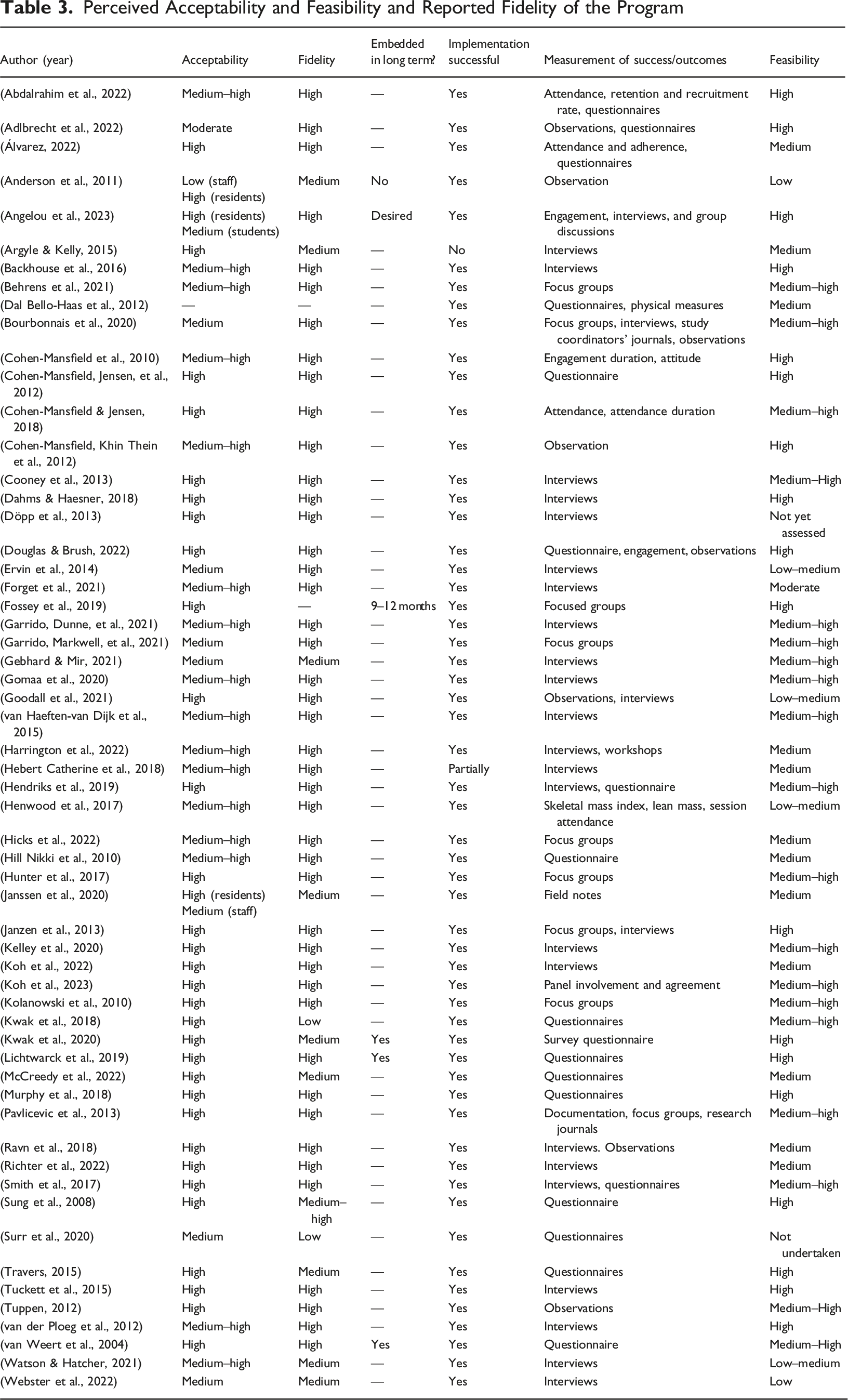
In terms of feasibility, the majority of interventions (53/58; 91.4%) were rated as moderately to highly feasible. Only a small subset of studies (5/58; 8.6%) identified challenges related to feasibility, citing barriers such as limited resources, logistical complexity and difficulties in participant engagement. Facilitators of feasibility included sufficient resource allocation, logistical efficiency, adaptability of interventions to diverse settings, and potential for scalability. However, long-term sustainability was infrequently addressed; only five studies (8.6%) reported ongoing use beyond six months post-implementation, and few provided further evaluation of acceptability or feasibility over time.
Barriers and Facilitators
Identified Barriers and Facilitators to Program Implementation
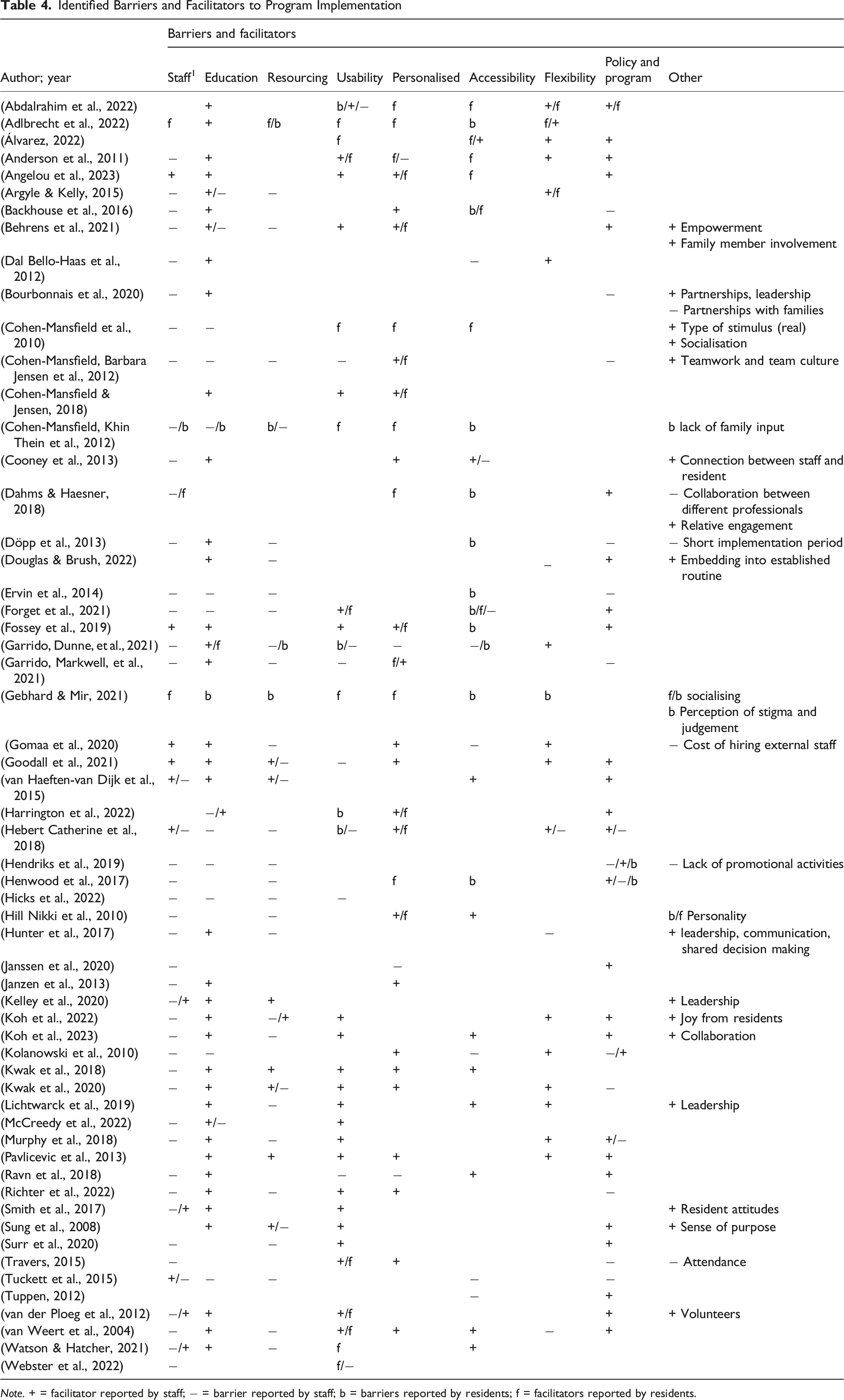
Note. + = facilitator reported by staff; − = barrier reported by staff; b = barriers reported by residents; f = facilitators reported by residents.
Education and training emerged as a central theme, identified in 49 studies (84.5%) as either a facilitator or barrier. Of these, 77.6% highlighted education (particularly regarding the structure, use, and expected outcomes of interventions) as a facilitator for both staff and residents. Studies such as (Behrens et al., 2021; Cooney et al., 2013; Gomaa et al., 2020), specifically described the role of ongoing staff development in promoting engagement and easing implementation.
Usability was reported in 38 studies (66.7%), with the majority (30/38; 78.9%) describing it as a facilitator. Facilitators under this theme included intuitive program design, clear guidance, and ease of recruitment and participation for both staff and individuals with dementia (e.g., (Pavlicevic et al., 2013)). Conversely, accessibility, especially for residents, was noted as a barrier in over half the studies (30/58; 51.7%). Accessibility challenges included physical or cognitive limitations, technological barriers, and environmental constraints (e.g., (Forget et al., 2021; Gebhard & Mir, 2021)). Of the studies reporting accessibility barriers, 27.6% cited impacts on staff, while 37.9% noted reduced resident participation.
Personalisation of interventions (e.g., one-to-one delivery or tailoring to individual needs) was another key facilitator, noted in 27 of 31 relevant articles (87.1%). Personalisation was associated with enhanced engagement among both staff (70.1%) and residents (66.7%). However, interventions incorporating personalised elements were also more frequently associated with staff-related barriers, likely due to increased demands on time and resources (e.g., (Janzen et al., 2013; Kolanowski et al., 2010)).
Flexibility in implementation (i.e., allowing for adaptation to individual and contextual needs) was discussed in 20 studies (34.5%). Most (16/20; 80%) identified flexibility as a facilitator, aiding integration into existing workflows and promoting sustainability. In contrast, lack of flexibility was cited as a barrier in the remaining four studies, often related to rigid program structures or incompatibility with care routines.
Policy and program-level considerations were mentioned in 34 studies. While a minority (8/34; 23.5%) identified these as barriers, often due to misalignment between policies and frontline care demands, the majority (76.5%) highlighted them as facilitators. Examples included alignment of programs with staff capabilities, supportive leadership, and integration with existing care schedules (e.g., (Fossey et al., 2019; Gomaa et al., 2020).
Positive staff and resident attitudes, though less frequently discussed (8 studies), were consistently described as facilitators (87.5%), contributing to higher engagement and smoother implementation (e.g., (Koh et al., 2022; Smith et al., 2017). Emotional factors such as sense of purpose, empowerment, and joy derived from resident participation further stressed the humanistic value of these interventions.
Music therapy appeared to be associated with a slightly higher number of facilitators per study compared to other intervention types (mean: 3.5 vs. 3.3), although overall, no significant differences were observed in the frequency of facilitators or barriers between intervention modalities. Interventions delivered by external professionals rather than internal staff were less likely to report staff-related barriers, while those requiring resources beyond what was already available in facilities more commonly encountered resourcing challenges and particularly so for external programs. Interventions emphasising personalisation also tended to report more staff-related barriers, which may suggest a trade-off between individualisation and implementation burden.
Quality Assessment
MMAT Critical Appraisal Scores. Studies Classified as Either “Medium” (Meeting 3-4/5 Criteria), or “High” (Meeting 5/5 Criteria)
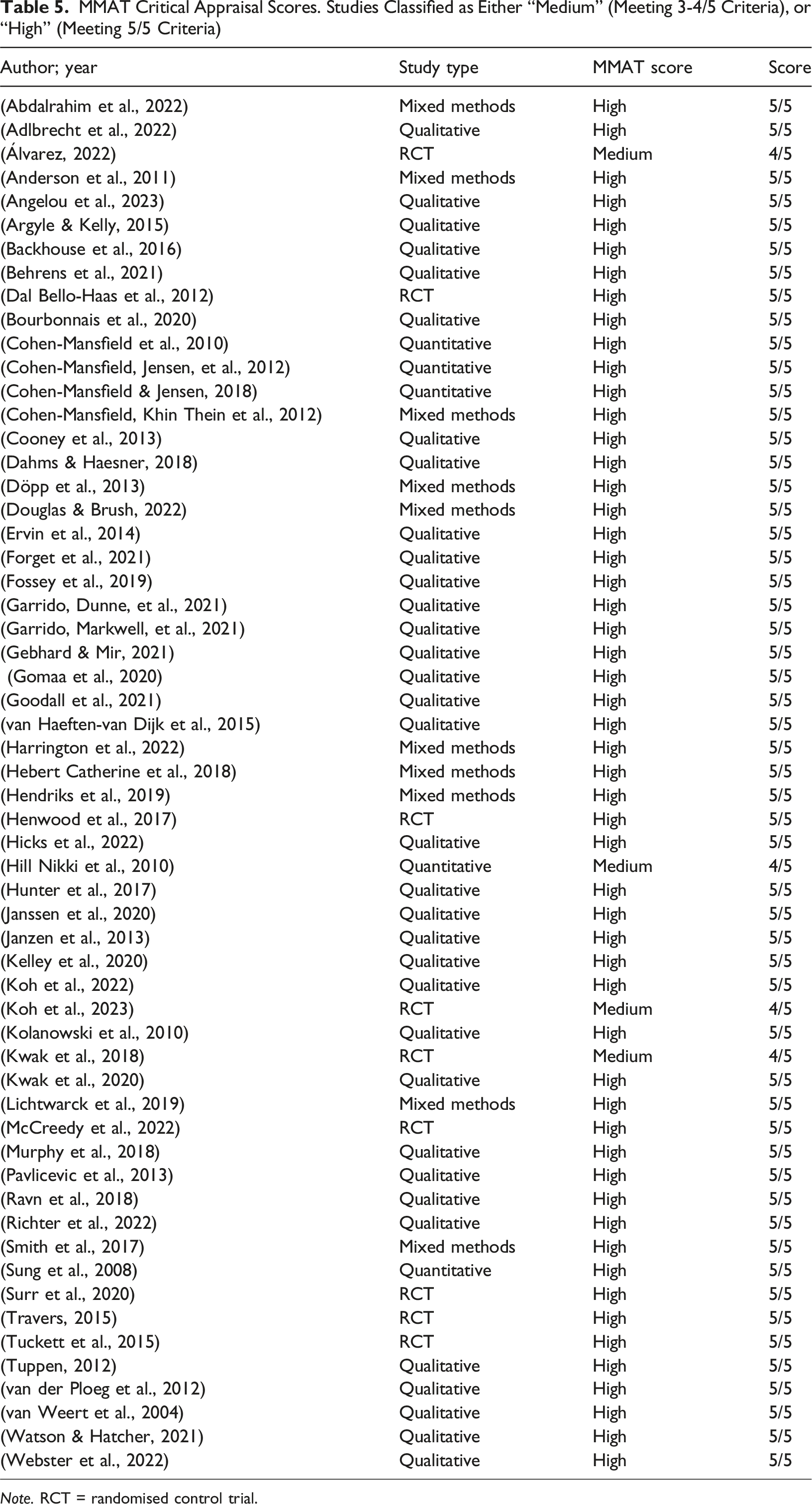
Note. RCT = randomised control trial.
Discussion
This review synthesises evidence on the barriers and facilitators influencing the implementation of non-pharmacological interventions for individuals with dementia in residential aged care settings. The objective was to support a deeper understanding of implementation challenges and inform strategies to enhance the sustainability and integration of non-pharmacological interventions in routine care. Our findings were categorised into key domains: staff-related factors (including workforce capacity, time constraints, and professional roles), education and training, resource availability, accessibility and usability of interventions, program flexibility, and policy or systemic considerations.
The barriers found to be the most prevalent included staff-related factors, lack of training and education, as well as inappropriate resource allocation and in-accessibility for individuals with dementia. By contrast, the most common facilitators included education for staff, carers and participants, flexibility with the use and timing of the intervention, as well as policy and program considerations such as aligning the program with staff capabilities, needs and timetables for smoother implementation and uptake.
Among the most pervasive impediments were those pertaining to the workforce. Time scarcity, staff availability, and a perceived misalignment between professional roles and the delivery of non-pharmacological interventions constituted recurrent themes, reflecting both operational and cultural barriers within care environments. These findings corroborate prior literature indicating that structural under-resourcing in aged care frequently results in an overreliance on pharmacological interventions to manage behaviour symposiums, despite guideline-based preferences for person-centred, non-pharmacological approaches (Cabrera et al., 2015; Deobald, 2024; Md Hussin et al., 2023; Windle et al., 2023). Moreover, the low prevalence of facilities that meet the minimum staffing standards for optimal care (3.8%) (Sutton et al., 2022) exemplifies a systemic incongruity between regulatory expectations and operational capacity. The chronicity of these deficits suggests that interventions that necessitate substantial staff time or specialised competencies may face persistent implementation friction. Accordingly, the use of adjunctive personnel, such as trained volunteers, family carers, or allied health professionals, may serve as a pragmatic buffer and mitigate some of the temporal and skill-related constraints borne by residential care staff (Gitlin et al., 2020; Kong et al., 2022; Peters et al., 2021; Sutton et al., 2022).
A robust finding across our synthesis was the salience of education and training as critical enablers for implementation. Staff who were equipped with structured, intervention-specific training not only demonstrated higher levels of acceptability and engagement but were also more likely to perceive non-pharmacological interventions as legitimate components of therapeutic care. These results resonate with previous evidence suggesting that educational initiatives can enhance both the attitudinal and practical uptake of non-pharmacological interventions among care providers (Ayeno et al., 2024; Bauer et al., 2018; Bennett et al., 2021; Gitlin et al., 2020; Kong et al., 2022; Parajuli et al., 2021; Wong et al., 2024).
Yet, the pedagogical void in many facilities, where non-pharmacological interventions delivery is guided more by trial-and-error than by structured, evidence-based protocols (Yous et al., 2020), suggests an urgent need for curriculum development tailored to dementia-specific care competencies. Furthermore, fostering dementia literacy among family carers and residents may augment shared decision-making and bolster the overall sustainability of non-pharmacological interventions (Ayeno et al., 2024; Bauer et al., 2018).
The implementation of non-pharmacological interventions is also circumscribed by resource-related exigencies. Financial outlays associated with program delivery, infrastructure adaptation, and intervention-specific materials were frequently cited as obstacles. These findings align with prior evaluations indicating that non-pharmacological interventions with minimal or no cost to residents and facilities exhibit higher rates of adoption and continuity (Eaglestone et al., 2023; Knapp et al., 2013; Steinbeisser et al., 2020). This observation invites a broader reconsideration of how cost-effectiveness is assessed in dementia care. Standard economic evaluations may inadequately capture the downstream benefits of non-pharmacological interventions including improved quality of life, reduced medication burden, and delayed institutionalisation which necessitates more longitudinal cost-benefit frameworks.
The finding that personalised non-pharmacological interventions enhance engagement for both people with dementia and care staff aligns with a well-established body of research reflecting the value of tailoring care to individual preferences, histories, and abilities. Person-centred care frameworks, such as those proposed by (Kitwood & Kitwood, 1997), emphasise that personalisation fosters dignity, agency, and meaningful engagement in dementia care. A systematic review similarly highlights that individually tailored interventions, such as music, reminiscence, or activity programs, can improve affective states and reduce behavioural symptoms (Möhler et al., 2020). However, our review also found that personalised interventions were more frequently associated with staff-related barriers, particularly time constraints and workload pressures. This reflects broader implementation challenges. For example, personalisation, while desirable and effective, requires system-level changes to be feasible at scale. Investing in staff training (Eggenberger et al., 2013), and adequate staffing ratios (Chenoweth et al., 2009) are therefore potential enablers. Without such systemic support, personalised non-pharmacological interventions delivery risks becoming another demand placed on already stretched staff. In policy terms, this speaks to the need for integrating personalisation into workforce planning and intervention design, ensuring that interventions are not only evidence-based but also practically deliverable in everyday care settings.
Positive attitudes in both caregivers and care recipients, while noted in fewer studies, may also play a role in determining the uptake of non-pharmacological interventions. The literature suggests that when staff perceive personalised interventions as impactful, they are more likely to invest their delivery, despite structural or resource limitations (Chenoweth et al., 2009). Similarly, when residents experience joy and meaningful connection during activities, they are more likely to participate consistently, which reinforces staff motivation and reinforces a positive feedback loop (Han et al., 2016). This suggests the need for a shared vision and collective action among staff in the implementation of non-pharmacological interventions. Normalisation Process Theory offers a valuable conceptual framework for understanding processes around intervention implementation, highlighting four core mechanisms: coherence (making sense of the intervention), cognitive participation (commitment to the process), collective action (the work required to enact the intervention), and reflexive monitoring (evaluation and adaptation over time) (May et al., 2009). Successful non-pharmacological interventions implementation not only requires staff education, but also alignment around purpose that supports coherence, and mechanisms for collective action that embed interventions into day-to-day routines (May et al., 2009). Our review suggests that supporting all elements of normalisation process theory, throughout initial adoption and ongoing practice, remains a key challenge and priority for future implementation efforts in dementia care.
Additional factors like procedural simplicity, adaptability, and the ease of integrating the non-pharmacological interventions into existing workflows were perceived to be more amenable to uptake. Flexibility in timing, modality, and staff responsibilities was consistently associated with increased feasibility, particularly in under-resourced settings (Bühler et al., 2023; Cabrera et al., 2015; Ross et al., 2023). The heterogeneous needs and capabilities of individuals with dementia further emphasise the necessity for non-pharmacological interventions that can be customised and modified across varying stages of cognitive decline. Designing interventions with intrinsic adaptability that are not only in content but also in delivery mechanisms are important for long-term integration. Indeed, our review found that interventions that align with staff routines, minimise additional workload and accommodate resident preferences are more likely to be sustained. Research has identified that the implementation environment is inextricably linked to broader organisational and policy architectures (Bullock et al., 2021). Evidence suggests that when interventions are harmonised with existing policy directives, staffing schedules, and care models, they are more likely to be embedded into routine practice (Aarons et al., 2014; Braithwaite et al., 2018; Brownson et al., 2022). Conversely, incongruence between intervention design and institutional structure may stymie even well-intentioned initiatives (Blankenship et al., 2006; Morrison et al., 2012). There is thus pressing need for implementation frameworks that account for contextual contingencies and facilitate the alignment of program delivery with organisational capacity.
Overall, findings from our review support the need for systematic implementation support to facilitate the sustainable implementation of non-pharmacological interventions in residential aged care (Andrews et al., 2024). There is increasing evidence that the use of implementation frameworks and toolkits; such as the Towards Organisational Culture Change resource, can equip organisations to systematically address context-specific barriers and facilitators to build staff capacity, and sustain change with minimal external facilitation (Etherton-Beer et al., 2021). Approaches grounded in participatory action research and co-design further strengthen implementation efforts by fostering collaboration, ownership, and responsiveness to the needs of both staff and residents (Etherton-Beer et al., 2021). Embedding non-pharmacological interventions within these frameworks maximises the likelihood of meaningful and sustained practice change.
Strengths and Limitations
This systematic review’s strengths include its comprehensive, reproducible search strategy, application of rigorous methodological processes using multiple reviewers, and the use of an established theoretical framework to categorise implementation determinants. Additionally, its focus on barriers and facilitators to the implementation of non-pharmacological interventions across diverse settings and intervention types ensures that findings are highly applicable and provide actionable insights for policy and practice. While the aim of this review is to synthesise barriers and facilitators to the implementation of discrete non-pharmacological interventions for people with dementia, it is important to also recognise broader models of care, which integrate these interventions into a philosophy or system, in residential aged care settings. Montessori-based activities, for example, can be delivered as individual, structured interventions and as an overarching model of care characterised by system-level changes, staff training, environmental modification, and continuous assessment. Emerging evidence suggests that the latter is associated with more substantial reductions in behavioural and psychological symptoms of dementia, improved staff knowledge and confidence, and enhanced resident and family satisfaction (Berg-Weger & Stewart, 2017). Similarly, the ABLE model, a composite person-centred approach integrating Montessori principles, has demonstrated significant improvements in resident agitation, engagement in meaningful activities, and a marked reduction in anti-psychotic use following implementation at the organisational level (Roberts et al., 2015). Although beyond the scope of this review, multi-component models could be more effective in preventing changed behaviours in dementia care contexts.
While our search terms such as “residential” and “aged care” are in alignment with Australian and international nomenclature, we recognise that they are not exhaustive. As such, some relevant studies may have been missed, particularly those indexed or titled using other terminology for residential aged care. Further, the disproportionate representation of music therapy within the included studies may have introduced thematic bias in identifying barriers and facilitators, however this may also indicate that non-music programs are desired in these settings. Also, cross-jurisdictional comparisons were limited, constraining the ability to examine how national policy environments and care models influence implementation dynamics. Finally, heterogeneity in study design and reporting limited the ability to conduct meta-analytical assessments.
Future Research and Implications to Policy and Practice
Future inquiry should adopt longitudinal and comparative approaches to elucidate how specific non-pharmacological interventions are implemented across diverse organisational and policy contexts. Research is also needed to establish standardised implementation protocols and fidelity measures, and to identify core components that enhance scalability. Developing and validating comprehensive implementation toolkits, potentially co-designed with stakeholders, may facilitate the integration of non-pharmacological interventions at both service and system levels. Furthermore, governmental support in formulating evidence-based guidelines, akin to the processes used by the Belgian Centre for Evidence-Based Medicine, could provide a structured pathway for widespread dissemination and uptake (Wang et al., 2022).
Conclusion
The successful implementation of non-pharmacological interventions for individuals with dementia in residential aged care is contingent upon a confluence of interrelated factors spanning workforce capacity, training infrastructure, resource availability, intervention design, and systemic policy alignment. This review highlights that while the therapeutic potential of non-pharmacological interventions is increasingly recognised, their integration into routine care remains fraught with structural, operational, and epistemic barriers. Addressing these challenges requires a multi-level implementation strategy underpinned by robust education and workforce development, adaptable and resource-conscious intervention models, and institutional policies that support sustained engagement. Future efforts must prioritise the co-design of context-sensitive implementation frameworks and evidence-informed guidelines to ensure that non-pharmacological interventions can be not only introduced, but sustained, within the complex realities of aged care environments. Only through such integrated approaches can we advance equitable, person-centred dementia care across settings.
Supplemental Material
Supplemental Material - Barriers and Facilitators to Implementing Non-Pharmacological Dementia Therapies in Residential Aged Care: A Systematic Review
Supplemental Material for Barriers and Facilitators to Implementing Non-Pharmacological Dementia Therapies in Residential Aged Care: A Systematic Review by Elesha Gebran, Mark Antoniou, Suraj Samtani, Ruth Brookman, Joyce Siette in Dementia
Footnotes
Acknowledgements
The authors would like to acknowledge the assistance of Ms Hanan Abubasheer with the critical appraisal of some articles. We would also like to acknowledge Dr Paul Strutt for earlier reviews and feedback on subsections of the manuscript.
Consent to Participate
There are no human participants in this article and informed consent is not required.
Author Contributions
EG: Methodology, validation, formal analysis, investigation, data curation, writing – original draft, writing – review and editing. MA: Methodology, validation, formal analysis, investigation, writing – original draft, writing – review and editing, supervision. SS: validation, formal analysis, investigation, data curation, writing – review and editing. RB: writing – review and editing. JS: Conceptualisation, methodology, validation, formal analysis, investigation, resources, writing – original draft, writing – review and editing, supervision, project administration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
PROSPERO Registration ID
CRD42022369239.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.