
Abstract
Introduction
Dementia is a progressive neurodegenerative condition that usually occurs in people aged 65 years and above, becoming a leading contributor to the burden of disease and disability worldwide, including in Australia (Australian Institute of Health and Welfare, 2023; Wakefield, 2020; World Health Organization, 2023). Individuals living with dementia gradually experience not only cognitive and physical impairments but also changes in behaviours, losing the ability to live independently and ultimately becoming wholly reliant on informal and formal caregivers (Australian Institute of Health and Welfare, 2023; Wakefield, 2020; World Health Organization, 2020). Usually, family members and close friends become their primary caregivers (i.e., informal caregivers) until they require advanced care in a formal care setting (Rathnayake et al., 2019; Wakefield, 2020; World Health Organization, 2023). As dementia advances and individuals living with dementia increasingly require assistance with both physical and psychosocial needs, informal caregivers (hereafter caregivers) often experience high levels of stress and burden (van den Kieboom et al., 2020; World Health Organization, 2023). Respite services are therefore essential, providing caregivers with critical relief from the ongoing demands of round-the-clock care (McCabe et al., 2016; Vandepitte et al., 2016).
Despite the preference for home-style respite for the individuals living with dementia and their caregivers, respite services remain predominantly offered in residential aged care (RAC) facilities (Harkin et al., 2020). Institutional respite, such as RAC, dominates because it is more visible, systematised, aligned with existing policies and administrative structures, and provides the trained staff and continuous monitoring needed to support people living with dementia safely (Leocadie et al., 2018; Whear et al., 2014). However, for community-dwelling people living with dementia, access to flexible, person-centred care remains limited. There is a need to broaden the range and diversity of respite care options, fostering a more person-and family-centred approach to caregiving (Ho et al., 2021; World Health Organization, 2018). Person- and family-centred care prioritises the preferences, life circumstances and clinical needs of both individuals living with dementia and their families. It actively involves them in care decisions and empowers them with the knowledge, skills and access to support services needed to optimise quality of life (QoL) (Epstein & Street, 2011; Marulappa et al., 2022). Integrating green environments in respite can enhance well-being by leveraging nature’s therapeutic benefits to promote relaxation and QoL for individuals living with dementia and their caregivers (De Bruin et al., 2020; Ng et al., 2024). Public health experts, therefore, advocate integrating green environments into person-centred dementia care, including respite services (Haubenhofer et al., 2010; Marulappa et al., 2022).
Health-promoting interventions that utilise both living and non-living elements of nature in their treatments are known as green care (Haubenhofer et al., 2010). Having contact with nature and spending time in natural environments can provide a sense of self-worth and autonomy that is often lost following a dementia diagnosis (Cook, 2022; Mmako et al., 2020). Green Care activities, such as sensory gardens and horticulture, are linked to improved mood, sleep, and well-being, along with reduced disruptive behaviours and reliance on psychotropic medications (Barrett et al., 2019; De Boer et al., 2017). Furthermore, compared to traditional RAC respite care, green care-based respite is associated with significantly higher levels of well-being among individuals living with dementia (Haubenhofer et al., 2010; Mmako et al., 2020).
For caregivers, green care offers all the usual benefits of respite care, such as time to rest, maintain social connections and work. Additionally, green care offers the extra benefit of reassurance that the caregiver’s loved one is enjoying their time away, easing the guilt of handing the responsibility of caring for their loved one to someone else (De Bruin et al., 2021). Green care activities may require physical effort, but activities can be tailored to the individual’s physical ability. Further, these activities are more engaging than in traditional dementia care settings (De Bruin et al., 2020), providing opportunities to experience meaningfulness, social connection, autonomy, and structure that mirrors daily living (De Bruin et al., 2020; Mmako et al., 2020). Caregivers interviewed in one study indicated that using green care respite could delay their decision to place their loved one into full-time care (Taranrød et al., 2021). However, there is limited evidence regarding the ability of green care respite to delay entry for a person living with dementia to permanent residential care.
The GreenConnect Dementia Respite Project (GreenConnect Dementia Respite Project, 2024) is a three-year (2023-2026) innovative Australian-first pilot project aimed at improving the QoL of individuals living with dementia, reducing the burden of caregiving for caregivers, and improving well-being and respite experiences for people living with dementia and caregivers. Following grant success for the project concept, the GreenConnect Dementia Respite Project implementation was co-designed with key stakeholders, including dementia caregivers, people living with dementia and formal respite care providers to design the GreenConnect Dementia Respite Program. Co-design is a recognised best practice approach for developing successful and sustainable public health interventions through meaningful collaboration with key stakeholders, including end-users, who are integral to the project’s success (Boyd et al., 2012). Previous research has shown that co-designing complex interventions with people living with dementia, caregivers, health professionals and other relevant stakeholders enhances both efficacy and value (Brijnath et al., 2023; Gaffy et al., 2022; Lord et al., 2022; Tsekleves et al., 2020). Involving people living with dementia in the co-design phase is recognised as a best intervention practice (Lord et al., 2022). Studies also revealed that the fluctuating nature of dementia symptoms -which can vary day to day - may affect an individual’s ability to participate consistently in co-design activities. Hence, ensuring their active and meaningful engagement can be challenging (Suijkerbuijk et al., 2019). To overcome these challenges, inviting both person living with dementia and their caregivers to engage together, known as the dyadic approach, has proven to be an effective solution. As caregivers play a vital role in interpreting and advocating for the needs of the person they support, this approach facilitates effective communication, enhances understanding and promotes more inclusive decision-making (Cerino et al., 2025). Finally, designing public health interventions for people with dementia and their caregivers requires flexible but active and meaningful engagement through open communication and shared decision-making to ensure the end-users’ voices are heard and valued (Lord et al., 2022).
Project Overview
The GreenConnect Dementia Respite Project is a pilot initiative showcasing an innovative, co-designed respite program for individuals with early-stage dementia and their caregivers. The project is a collaborative effort led by a consortium comprising a grassroots community dementia care organisation, three aged care and respite service providers, and an academic institution. The consortium group provides overall governance of the project, with key representatives from each organisation meeting regularly to oversee and monitor progress toward the project’s short- and long-term objectives.
Rooted in nature-based immersion, the GreenConnect Dementia Respite Project draws on green care principles and their demonstrable benefits for social, physical and mental health (Haubenhofer et al., 2010). GreenConnect was designed to support varying levels of engagement, accommodating the diverse abilities, functional capacities and personal preferences of individuals living with early-stage dementia. The activities of this program are coordinated from three of the project consortium members’ sites in the Loddon-Mallee region: Heathcote Health in Bendigo (at the southern end of the Loddon-Mallee region), Princes Court, and Rural Care Australia in Mildura and Merbein (the north-west of Loddon-Mallee) (Figure 1) (Heathcote Dementia Alliance, 2024). Map of Loddon Mallee region, Victoria, Australia. (Source: https://www.rdv.vic.gov.au/victorias-regions/loddon-mallee)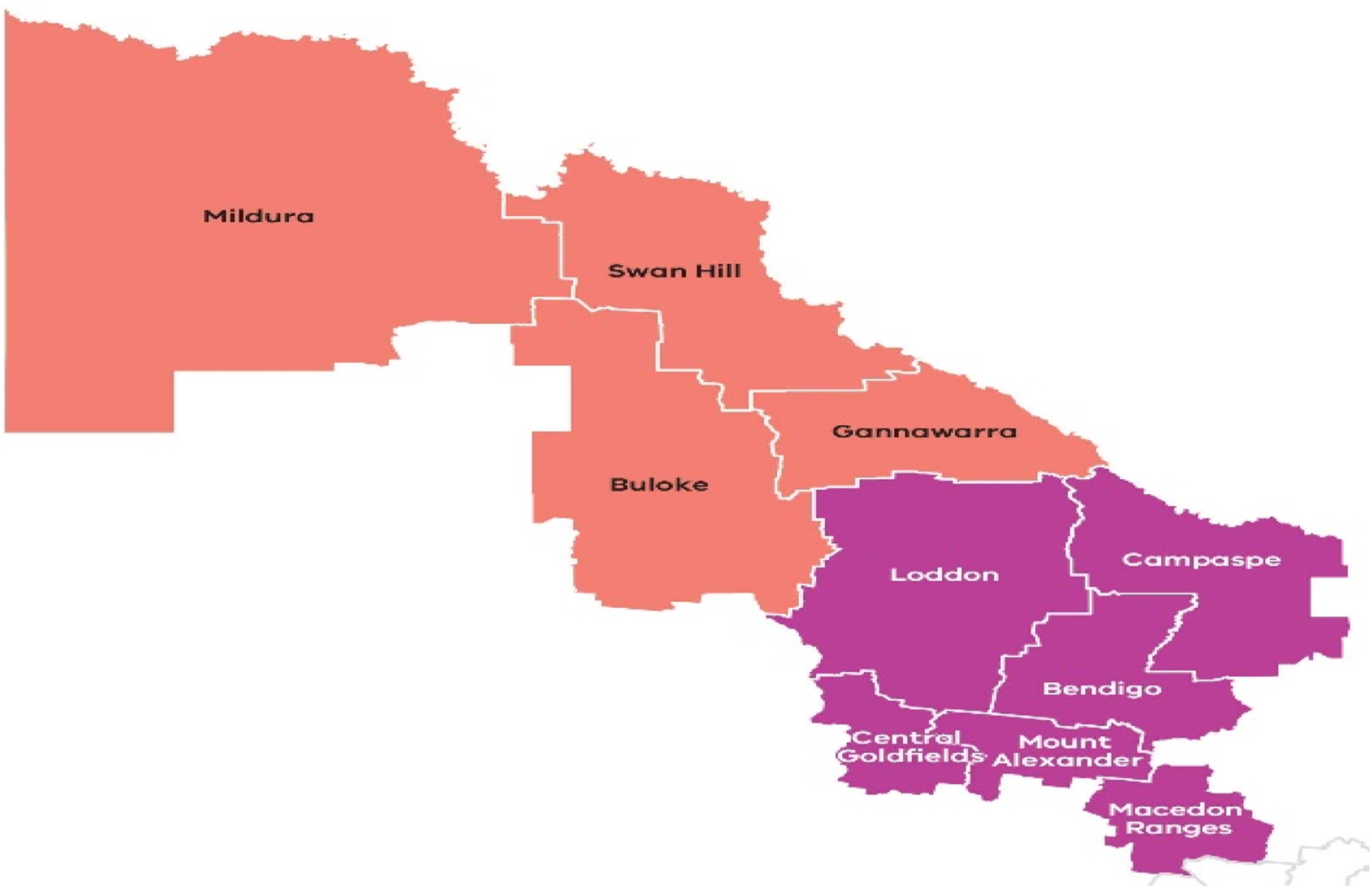
The Loddon-Mallee region is home to approximately 6% of the total population of Victoria (334,911 people in 2024), making it the largest region in Victoria, Australia (Bendigo Health, 2024). Nearly one-quarter of the total population (22%) in this region is aged 65 and older, with nearly 1% diagnosed with dementia (Bendigo Health, 2024). Recent statistics revealed that the number of people aged ≥65 and people with a dementia diagnosis is increasing (Bendigo Health, 2024). The region is characterised by its diverse and vibrant communities, including First Nations people and people from ethnically, culturally, and linguistically diverse backgrounds. Many residents encounter significant socio-economic disparities due to lower levels of education and income, as well as higher unemployment rates, particularly in remote areas. Furthermore, the rate of health risk factors – such as smoking, alcohol consumption, obesity and unhealthy diet – is higher in this region (Bendigo Health, 2024). These factors are expected to drive a rise in chronic diseases, including dementia, in the coming years (Joshi & Tampi, 2024; World Health Organization, 2023). Yet, service provision for older adults needing support remains limited in this region (Bendigo Health, 2023). Implementing the GreenConnect Dementia Respite Program in the Loddon-Mallee region is therefore timely, addressing critical service gaps in regional Victoria and contributing to the evidence base for dementia care in aged care services.
This paper describes the co-design process to inform the implementation of the GreenConnect Dementia Respite Project, aimed at ensuring the project was grounded in lived experiences and tailored to end-users’ needs. Findings of the co-design study were generated through active engagement of diverse key stakeholders, including dementia caregivers and people living with dementia. The findings shaped the core elements of the project’s model of care and informed its implementation and evaluation strategies. The outcomes of program implementation and evaluation will be reported elsewhere following the program completion in 2026. Figure 2 shows the Projects’ timeline. The study was approved by the La Trobe University Human Research Ethics Committee (HEC23341). All participants or their proxies provided written informed consent. The GreenConnect Dementia Respite Project timline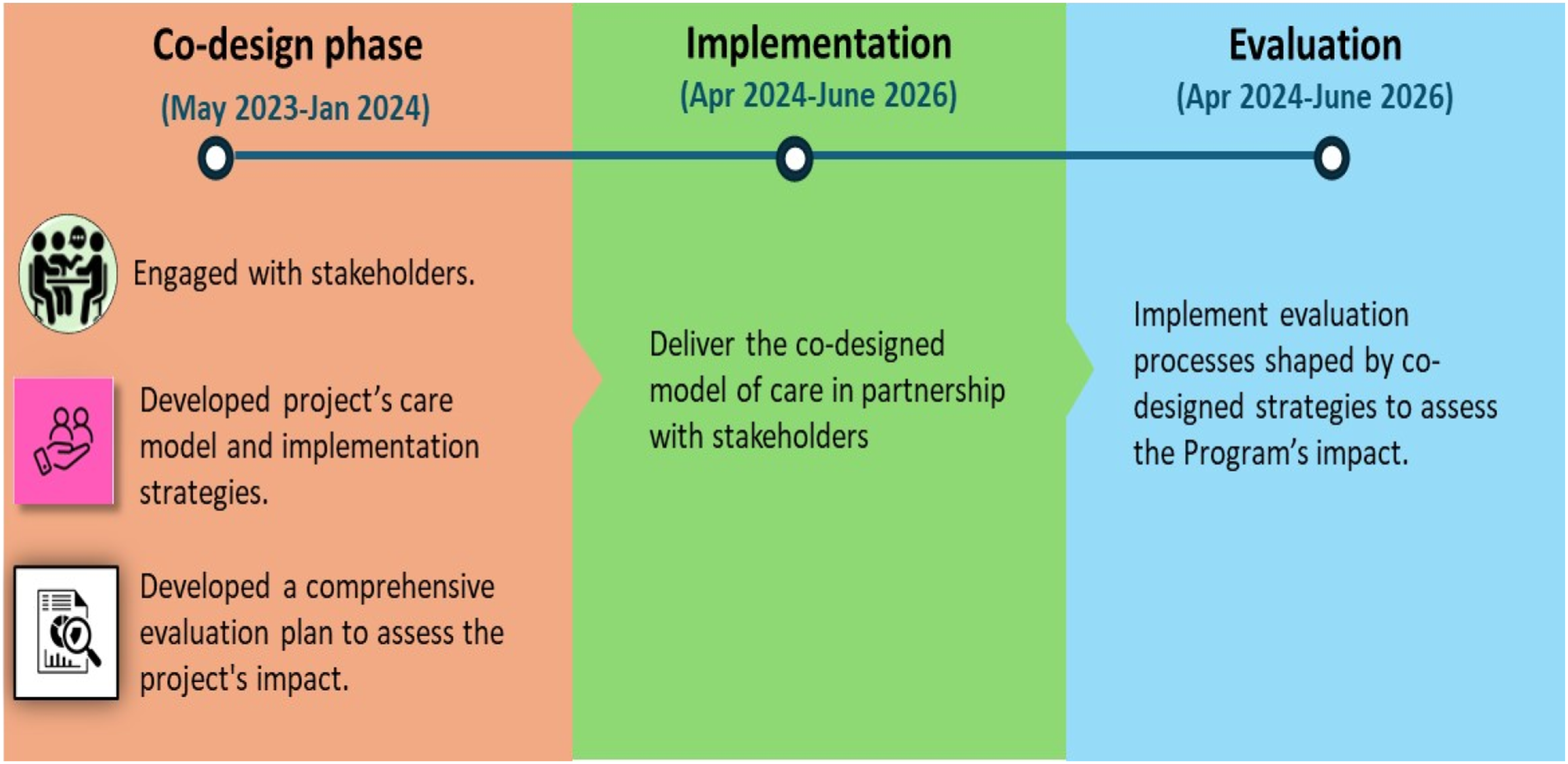
Methods
Development of the GreenConnect Dementia Respite Project employed a co-design approach that was guided by participatory action research and the socio-ecological framework (a multifaceted interplay between individual, interpersonal, community, and societal factors) (Slattery et al., 2020; Wang et al., 2019). The co-design phase, or the pre-implementation phase of the project, focused on designing the GreenConnect Dementia Respite Project, its model and implementation for people living with dementia and their informal (someone who was caring for their partner, parents, or friends) and formal caregivers (Oliver et al., 2004; Slattery et al., 2020).
Data Sources
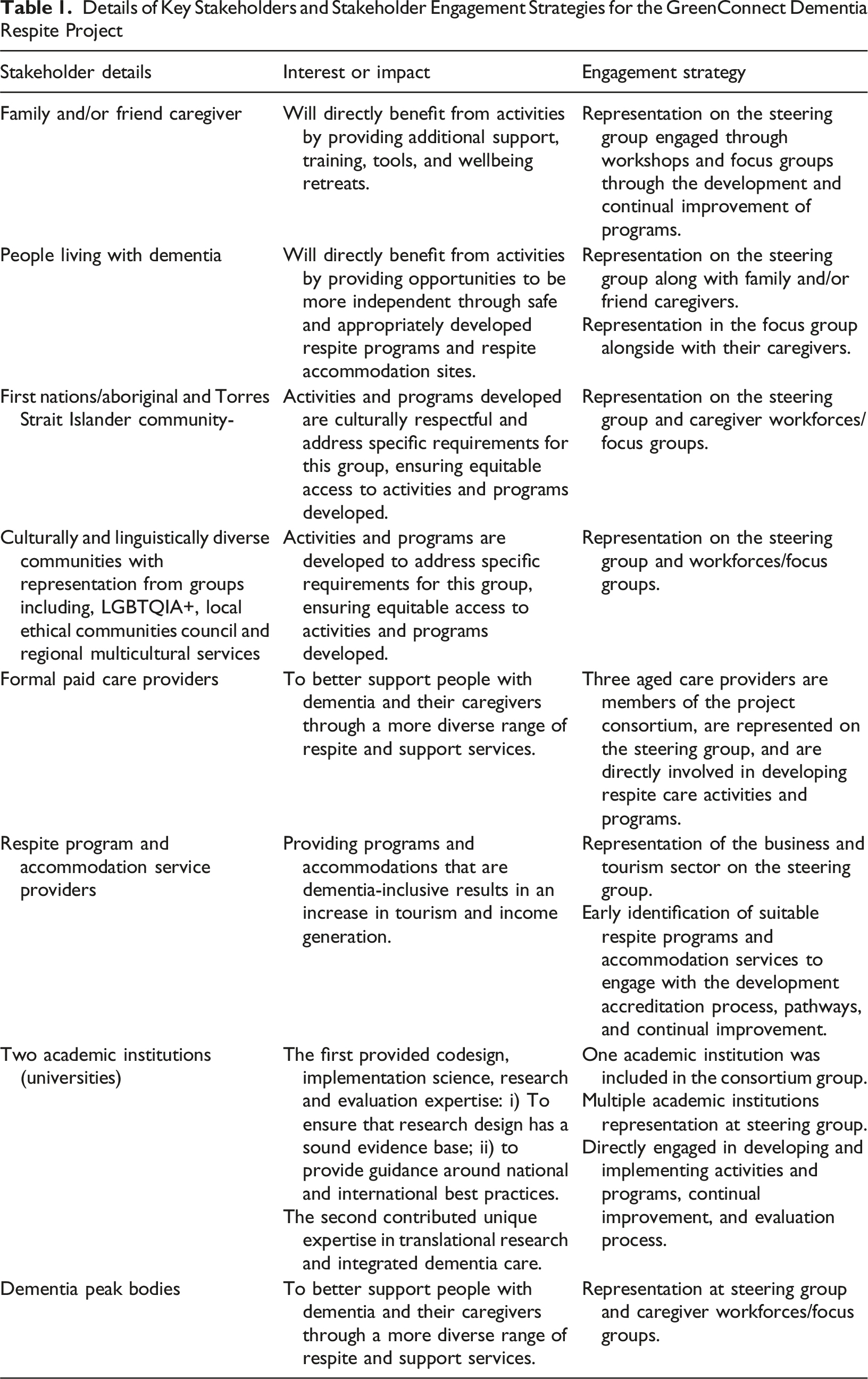
Details of Key Stakeholders and Stakeholder Engagement Strategies for the GreenConnect Dementia Respite Project
Participant Recruitment Procedures
Community participant recruitment for the co-design was supported by project consortium members, who identified potential eligible individuals through their networks within the project catchment area. In collaboration with the grassroots consortium member, the project team distributed flyers inviting expressions of interest for two activities, i.e., i) consultation workshop with dementia care professionals and ii) focus groups for caregivers of people living with dementia together with those they cared for. The adoption of dyadic participation – engaging both dementia caregivers and care recipients together-was deemed practical for the purpose of the co-design activities (Lord et al., 2022; Suijkerbuijk et al., 2019). Interested individuals were then provided with a participant information pack, including a plain language summary of the project and a consent form, prior to attending the co-design workshops and focus groups.
An additional workshop participant group was made up of the GreenConnect Dementia Respite Project steering group. The steering group comprised consortium partners and other key stakeholders (see Table 1). Members included representatives from academic dementia research, people living with dementia, caregivers, dementia service providers, the Australian Indigenous community, a national dementia peak body, LGBTQIA+ community, dementia advocacy and support groups, and aged and respite care providers.
Data Collection Procedures
Focus Groups With Joint Informal Caregivers and People Living With Dementia
Two face-to-face focus groups with caregivers and people living with dementia were held in Bendigo and Mildura. We invited both people living with dementia and their caregivers to participate together (i.e., dyadic participation). Dyadic participation in focus groups is recognised as an effective method, particularly for dementia care-focused interventions. Because it enables participants to build on their shared understanding and experiences (Cerino et al., 2025; Wammes et al., 2021). Plus, it mirrored the difficulty of separating the caregiver and the person they care for. The focus groups explored the challenges and potential improvements of existing respite care services for people living with dementia and their caregivers. Despite attempts to be inclusive of dyad participation, only two dyads participated in the focus groups, and the remaining caregivers participated individually without the person they care for. Our initial inclusion criteria focused on inviting current caregivers of people living with dementia. However, several former caregivers also expressed their interest in taking part in the study during the participants’ recruitment process. Given their comprehensive experience across the full trajectory of dementia care, the insights of former caregivers were considered a value add to the co-design. Hence, we decided to include former caregivers whose caregiving responsibilities ended within 12 months, due to the death of the person living with dementia.
Both focus groups were conducted in readily accessible locations at each study site to maximise participants’ convenience. Two participants brought their loved ones with an early stage of dementia. The research team was mindful of maintaining a comfortable environment for them and asked their caregivers if additional assistance was needed. Also, with their caregivers’ assistance, the people living with dementia were invited to contribute to the discussion. However, both chose to remain silent during the focus groups and sat comfortably with the group. Their caregivers actively participated in the discussions. The duration of each focus group was nearly an hour. Two authors (TMR and SA) facilitated the focus groups and took turns taking notes. All participants (caregivers of a person living with dementia) at the focus groups were reimbursed with $150 gift vouchers for their participation.
Consultation Workshop
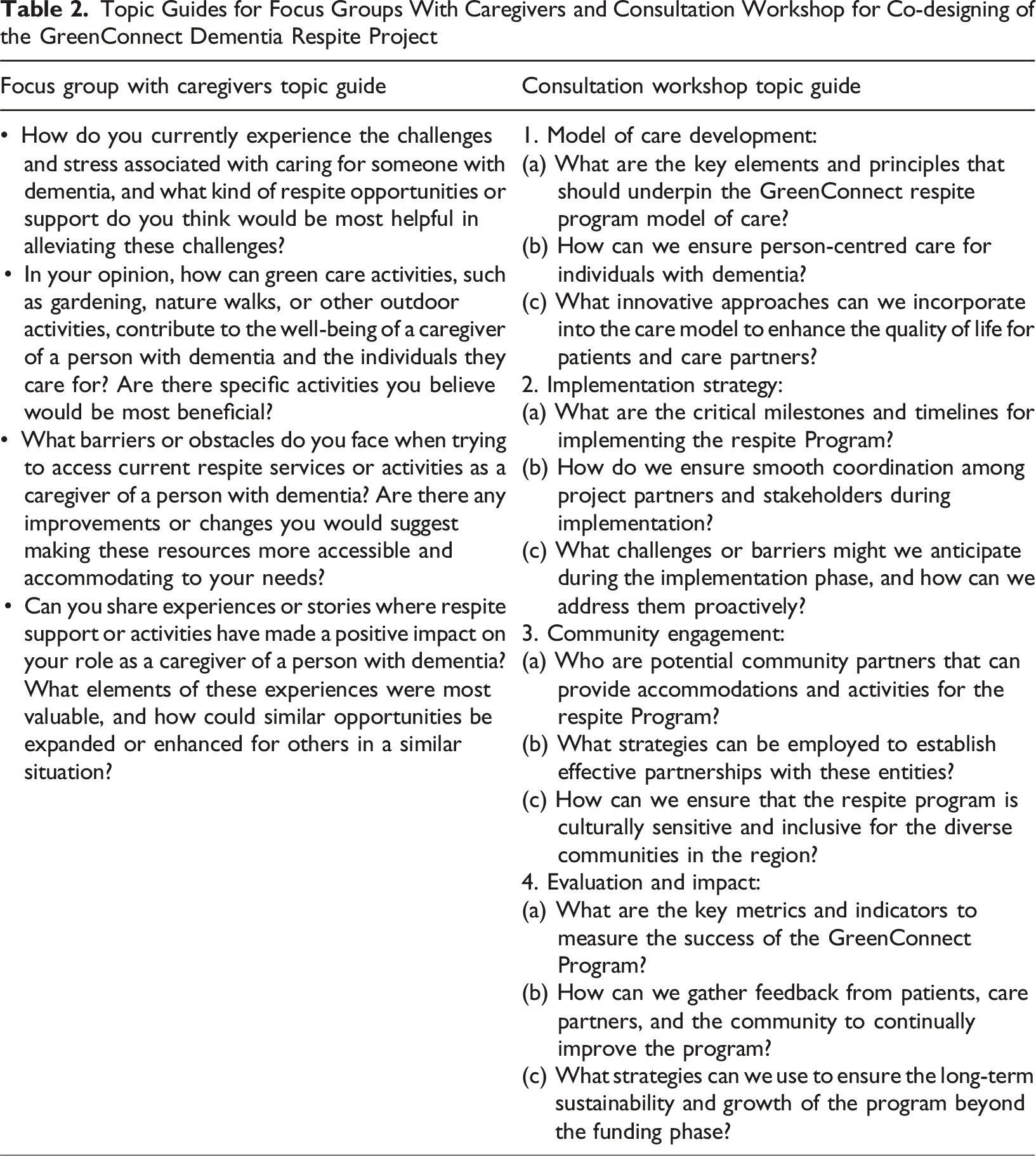
Topic Guides for Focus Groups With Caregivers and Consultation Workshop for Co-designing of the GreenConnect Dementia Respite Project
Focus groups were audio-recorded, ensuring accurate capture of discussions. Recordings were transcribed verbatim. To further enrich data triangulation, research team members’ notes were supplemented to the subsequent transcriptions and analysis of the focus groups and consultation workshop.
Data Collection Instruments
Two separate pre-developed topic guides were used during the consultation workshop and focus groups for data collection (Table 2). All discussions were conducted in English.
Data Analysis
Audio recordings of the discussions were transcribed verbatim by a trained transcriber. Two authors (TMR and SA) reviewed the transcripts to ensure accuracy. During discussions, members of the research team took notes of the discussions, which were collated and analysed manually using thematic analysis (Braun & Clarke, 2006) underpinned by the socio-ecological framework (Bronfenbrenner, 1977; McLeroy et al., 1988).
Co-Design Study Team
The co-design study was carried out by a multidisciplinary research team comprising professionals from various fields, including medicine, psychology, physiotherapy, public health, anthropology, and project management. In addition, five coauthors have substantial experience working directly with communities focused on aged care and dementia care. All team members have extensive experience in co-designing public health interventions.
Results
A total of 35 participants participated in the co-design study (n = 23 participated in the consultation workshop and n = 12 in two focus groups). Of the 23 participants in the consultation workshop, 18 participants attended in person (i.e., face-to-face) and 5 joined online.
Focus group participants were mainly female, had English-speaking backgrounds and were informal caregivers (n = 10/12); primarily supporting their partners (n = 9) and a parent (n = 1). Most of them (n = 8/12) were current caregivers of a person living with dementia, and two (n = 2/12) were former caregivers. Two informal caregivers participated together with their loved ones who had dementia. There was a low response (n = 2 individuals out of approximately 10 professional dementia care organisations invited). Consequently, the two formal caregivers participated in the second focus group rather than a separate formal (professional) caregiver focus group.
Thematic Analysis Findings
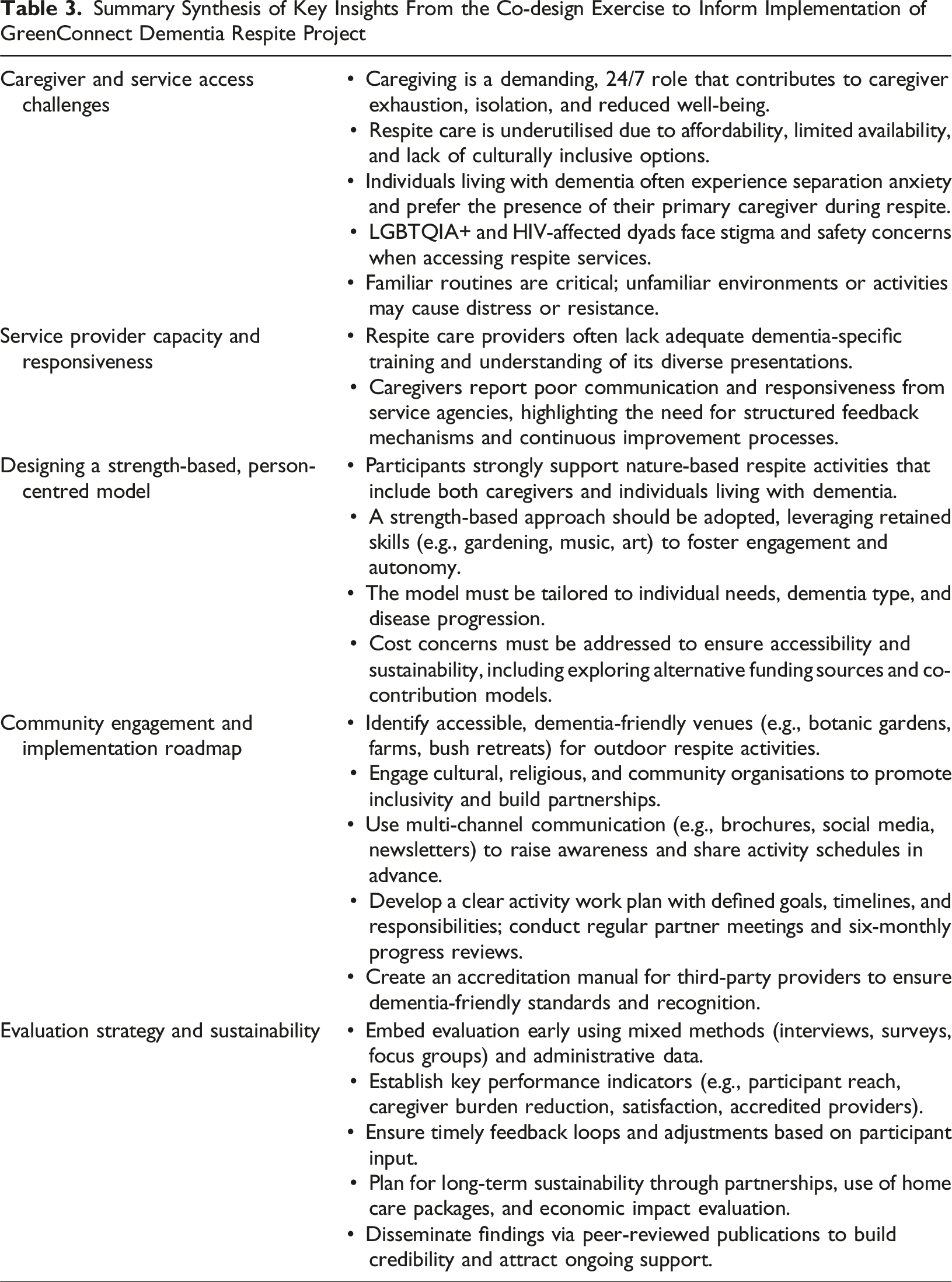
Some key priorities identified through the co-design process included: a) caregivers’ perspectives on challenges associated with caring for a person living with dementia and accessing respite care services; b) co-developing a model of care for the GreenConnect Dementia Respite Project; c) developing the implementation roadmap and engaging with community entities; and d) designing a clear evaluation strategy.
Caregivers’ Perspectives on Challenges Associated With Caring for the Person Living With Dementia and Accessing Respite Care Services
Participants highlighted significant challenges faced by informal caregivers, including stress, social isolation, and a lack of culturally inclusive respite options. All focus group (denoted with FG in the supporting quotes) participants mentioned that caring for a person living with dementia was a demanding 24/7 job, making it difficult to take time off. They described the relentless nature of the caring responsibilities as “exhausting” coupled with the separation anxiety faced by individuals living with dementia whenever they found themselves alone without their primary caregiver. “You know, the other thing, too, is that a lot of people with a (dementia) diagnosis, when their loved one (caregiver) is not there, they become extremely anxious, and they need them to be there”. [FG1, Mildura]
Most focus group participants played a dual role as both caregiver and spouse, making it extremely difficult to dissociate from the individual living with dementia. “I get really frustrated being a caregiver too, but it's a different frustration. … I've taken annual leave for three weeks, but I'm still caring for [partner’s name]. But it is exhausting”. [FG1, Mildura]
Individuals living with dementia often experience social isolation, and spouse caregivers were especially vulnerable. As their caregiving responsibilities take priority, caregivers’ social connections gradually shrink, leaving them with limited opportunities for interaction and support. They stopped doing things they “love to do”. The isolation increased the caregivers’ risk of stress and declining health and well-being. “…because dementia itself limits you. Yes. You cut off so many things in your life and you're living in a box ... My world moves around my husband’s routine … I have lost contact with my friend circle”. [FG2, Bendigo]
All caregiver participants reported using respite services, though most accessing them only once monthly due to affordability constraints. The cost constraints extended to respite activities that were most enjoyed by the individuals being cared for. “He loves farms, he loves playing with dogs …, but it was expensive… how often can I afford this?” [FG2, Bendigo]
Experiences with existing respite varied. Several caregivers expressed dissatisfaction due to high costs. Participants raised concerns that if the services under the proposed model became too costly, accessibility would be limited, ultimately jeopardising the Project’s long-term sustainability and impact. Despite these concerns, consultation workshop participants suggested that the Project should proceed with development and implementation after a comprehensive cost analysis is conducted, alternative funding sources are explored, and sustainability measures and growth projections are established.
Another criticism of current respite was limited activities, lack of diversity and culturally inclusive options. They indicated that unlike self-funded retirees, most elderly dyads relied on pensions and home care packages, which fell short of meeting respite needs. Furthermore, caregivers of individuals in the LGBTQIA+ community and/or living with HIV alongside dementia reported that accessing respite was limited by stigma. Many feared disclosures of their loved one’s sexual orientation or medical condition, raising safety concerns. This sentiment was echoed by the consultation workshop participants, including several with first-hand experience in formal dementia care. “LGBT(QIA+) people and their caregivers still love doing everything … no matter where they go for accommodation, or no matter what activity they do together, there still has to be that safety, where the personal relationship that these people have doesn't necessarily rely on disclosure to the outside world, about their sexuality, about their HIV status”. [FG2, Bendigo]
Other challenges to accessing respite services were that individuals living with dementia rely on familiar routines and disruptions can cause distress, depending on the type and progression of dementia. Those in the early stages of dementia may consent to outdoor respite activities without their caregiver, but most, regardless of disease progression, still preferred their primary caregiver’s presence. Consequently, this contributed to limiting caregivers’ social connections and increasing isolation.
Most participants expressed dissatisfaction with respite care providers’ limited knowledge of dementia and lack of experience in supporting individuals with the condition. All participants believed and suggested that comprehensive dementia training would equip respite care providers with the knowledge and skills needed for effective care. “[Respite] care workers should have more training in dementia and all the facets of it. Yeah, that would help… because a lot of workers that I found … that we have, …. they just think it's all [dementia] one thing! They don't understand that there are several different variations”. [FG1, Mildura]
Caregivers felt providers often lacked empathy for the unique challenges faced by people living with dementia and their caregivers. Despite repeated attempts to voice concerns through various channels (e.g., email, phone, formal complaints), many received no acknowledgment or experienced delayed responses from the agencies. Participants stressed the importance of establishing better communication strategies and a structured mechanism for delivering constructive feedback to agencies and respite care providers. “… you've heard of continuous improvement… You can't have continuous improvement unless people complain because you don't know what needs to be improved!” [FG1, Mildura]
Co-developing a Model of Care for the GreenConnect Dementia Respite Project
Given that existing respite care services are primarily indoor-based with minimal involvement of the caregivers, focus group participants expressed excitement about a nature-based respite activities plan for them and the individuals they care for. Participants stressed the importance of the proposed nature-based respite to incorporate a diverse range of activities in outdoor settings to cater to the unique needs and preferences of caregivers and individuals living with dementia. “Oh God, wouldn't it be wonderful if people [individual living with dementia and their caregiver] could go out to the botanical gardens!” [FG1, Mildura]
In addition to diverse activity offerings, focus group participants emphasised the importance of a strength-based approach; one that recognises and draws on the unique talents of individuals living with dementia to foster engagement and positive experiences. Despite cognitive decline, participants noted that long-term memories can still be accessed, enabling meaningful participation. They believed this approach could enhance purpose and agency for those with dementia while also alleviating caregiver burden. “… there are still some strengths there. And you know, people have got skills that maybe they haven't lost, like art or something else. I think they still really respond when someone says, ‘We need you to help with this’. I know that I see Mom shine dramatically if she feels that she's got a role. She's important or doing something like that. And I'm sure there's a little something in each person, sometimes incredibly diminished, but if we can find that.” [FG2, Bendigo]
In line with the model’s emphasis on openness and transparency, co-design participants highlighted the importance of maintaining regular, timely, and clear communication with all key stakeholders, particularly end-users (i.e., people living with dementia and their caregivers), throughout the project. This would enable participants to raise safety concerns, identify areas for improvement, and ensure that project activities remain aligned with their needs and expectations. Several participants stressed the importance of establishing effective and transparent feedback mechanisms, such as satisfaction surveys, interviews, performance reviews, and accessible online portals. They further recommended encouraging ongoing participant feedback on any changes made in response to earlier input. Such transparent communication not only fosters trust between the project team and its stakeholders but also ensures that the individual and cultural values of dyads are respected and upheld.
Developing an Implementation Roadmap and Engaging With the Community
Given the project’s focus on nature-based respite care, accommodation and activities, participants emphasised the need to identify suitable community locations for green care respite. They highlighted several potential venues, such as vineyards, bush retreats, farm stays and botanic gardens with sensory-based designs, which should be easily accessible to ensure safe mobility.
To promote cultural inclusivity, participants recommended engaging various cultural and religious groups. They also stressed the importance of collaborating with local aged care agencies, existing partners, and community organisations. Effective communication channels, including newsletters and word of mouth, were suggested to strengthen partnerships. Furthermore, participants recommended a multifaceted strategy to enhance project awareness. This included printed (e.g., brochures) and online resources, i.e., a website and dedicated social media pages (Facebook and LinkedIn) to inform potential participants, existing respite care providers and the broader community about Project objectives, expectations, and activities. Additionally, participants proposed sharing activity calendars and schedules in advance, allowing dyads ample time to plan and prepare for participation. “…if you do have enough notice of when a particular weekend away or a three-day retreat is in four months’ time, you can really lock it in… I think I know there’s one thing that’s going to be here… we know it’s in the middle of March. So, I’m not planning anything else at that time!” [FG2, Bendigo]
Consultation workshop participants emphasised the need for a well-defined activity work plan to serve as a roadmap for project execution, ensuring all partners are aligned on goals, timelines, and responsibilities. They recommended scheduling regular meetings with project partners to review progress, assess evolving needs, conduct risk assessments, develop mitigation strategies, and implement necessary adjustments. Regular updates to stakeholders were seen as essential for maintaining transparency and accountability. Participants proposed a six-monthly review report to track critical milestones, timelines, progress, client engagement, experiences, feedback, and key metrics. They also noted the importance of aligning the project with the timeframe set by aged care standards.
Additionally, participants suggested developing an accreditation manual for third-party providers, such as GreenConnect respite accommodation and activity businesses. The manual would help them prepare for accreditation, ensuring recognition as GreenConnect dementia-friendly partners or businesses. This was seen as fostering a supportive environment where partners and stakeholders could openly share concerns and collaboratively seek solutions.
Given potential for dropouts and withdrawals from the Project among older adults and individuals living with dementia, participants proposed possible solutions to address this threat to implementation: for example, respecting individual preferences; developing contingency plans to modify activities or reschedule sessions if need arise (such as bad weather conditions to run outdoor activities); adopting realistic and flexible timelines for each stage; providing additional support to staff so the service providers can complete tasks effectively; and organising information sessions for potential respite providers.
Designing a Clear Evaluation Strategy
Participants’ responses underscored the importance of embedding evaluation early into the proposed project. They posited that achieving this would require a mixed method design and the use of a variety of appropriate data collection tools (e.g. interviews, focus groups, and surveys) for quality administrative data that would foster analysis of effects and impacts. Furthermore, participants advised that the Project should provide comprehensive dementia training to its staff and service providers to equip them with the required skill set to deliver consistent and quality person-centred care that aligns with the evaluation strategy. Alongside this would be establishing key performance indicators to help measure project success that align with the Project objectives.
Some exemplar metrics included measuring reach by tracking the number of participants and accredited businesses, while also gathering participant feedback and reviews across online project platforms to evaluate impact. Feedback from individuals living with dementia and their caregivers should capture key outcomes such as reduced caregiver burden, improved QoL, and overall satisfaction. Participants also emphasised the need for timely adjustments based on feedback.
Additionally, the workshop participants discussed the ways to ensure sustainability and growth of the Project beyond funding ends and proposed a combination of strategic initiatives for implementation, which included partnerships with government agencies and local businesses to provide affordable options for outdoor activities. For example, they mentioned funding through home care packages (HCPs) for the dyads to continue activities and respite care. The HCPs are Australian government-funded programs to provide coordinated care and support for elders (aged 65 and older) to enable them to live in the home longer (MyAged Care, 2025). They suggested developing a sustainable fee structure for activities that require the target population to make a minimum financial co-contribution so that they can continue participating in their preferred activities. They also recommended undertaking economic impact evaluations of these initiatives and disseminating findings through peer-reviewed publications to build credibility and attract continued support from stakeholders. Figure 3 depicts potential socio-ecological factors that may influence the GreenConnect Dementia Respite Program implementation. Schematic diagram of potential socio-ecological factors identified in the co-design study that can influence the GreenConnect Dementia Respite Program
Summary Synthesis of Key Insights From the Co-design Exercise to Inform Implementation of GreenConnect Dementia Respite Project
Discussion
This study presents, to the best of our knowledge, the first dementia-focused respite program in rural Victoria, Australia, grounded in green care principles. The GreenConnect Dementia Respite Project set out to actively engage relevant key stakeholders in the program co-design phase through a consultation workshop and two focus groups. By actively involving different key stakeholders (N = 35 caregivers of people living with dementia, health professionals, nurses, social workers, academics, dementia advocacy groups and peak bodies, members of the Indigenous community and the LGBTQIA+ community and other professionals) in the discussions, we sought to determine our key stakeholders’ perspectives on the factors that could influence the implementation of innovative, dementia-friendly respite founded on green care principles. Our co-design study revealed four key findings: caregivers’ perspectives on the challenges of dementia care and accessing respite; the collaborative development of a clear and practical implementation strategy; the co-design of the project’s model of care; and designing implementation strategies. Across all discussions, participants consistently emphasised the importance of a person-centred, culturally inclusive approach that places people living with dementia and their caregivers at the heart of the program.
The co-design approach allowed informal caregivers to voice the complex emotional and physical challenges they encounter while caring for loved ones with a dementia diagnosis. While caregiving is commonly driven by love, duty, reciprocity, or satisfaction (Engel et al., 2022), this co-design engagement highlighted deeper insights into the evolving challenges of dementia caregiving as the condition progresses. Caregiver participants identified key challenges in dementia care, including social isolation, limited access to affordable person- and family-centred services, and a shortage of trained respite providers with dementia expertise, echoing findings from previous studies (Azevedo et al., 2021; Thompson et al., 2024). All caregivers in our study accessed respite services at least monthly and expressed a desire for more frequent use. However, limited availability, particularly of dementia-focused respite options in rural and remote areas, remains a significant barrier. While respite is a vital support for people living with dementia and their caregivers (Hao & Ruggiano, 2020; O’Shea et al., 2019; Temple & Dow, 2018), the lack of tailored services highlights a gap in meeting their unique needs. Limited understanding of dementia among the service providers, combined with higher costs associated with respite services, often results in unsatisfactory care for the dyads. Consequently, caregivers and individuals living with dementia dyads residing in rural areas face more challenges accessing the support they need (Temple & Dow, 2018; Wakefield, 2020). These shortcomings adversely impact the QoL of both individuals living with dementia and their caregivers who require immediate assistance (Hao & Ruggiano, 2020; Neville et al., 2015; Ramachandran et al., 2023; Temple & Dow, 2018). Healthcare professionals and experts in dementia care at the consultation workshop agreeing to those concerns suggests an urgent call to action and more funding for the development and implementation of tailored, effective dementia-focused respite care options (Macleod et al., 2017; McCabe et al., 2016).
The enthusiastic response to the GreenConnect Dementia Respite Program from the co-design participants also highlights the urgent need for innovative dementia focused respite services. The proposed dementia-friendly Program’s activities are set to occur outside RAC settings. Both caregivers and individuals living with dementia can participate together in the Program activities, along with other dyads in similar situations, to encourage social interaction and connection (Azevedo et al., 2021; Evans et al., 2019; Haubenhofer et al., 2010). Given its unique nature, all suggestions related to the Program’s model of care and implementation strategies emerged from the co-design discussions, including establishing partnerships with local communities and entities (Brewin, 2018; De Bruin et al., 2009) and conducting risk assessments of activities, locations and suitability for the target population to ensure the safety and well-being of the participants are timely and relevant (Dementia Australia, 2025), which we believe will ensure the successful implementation of the program.
As expected, the co-design process highlighted diverse views and expectations with practical recommendations regarding the outdoor-based activities. For example, a recommendation to employ a strength-based approach. Traditional interventions for people diagnosed with dementia have often relied on deficit-based models that emphasise limitations in daily functioning, which contradict the principles of person-centred care and risk disempowering those affected (D'Cunha et al., 2020; Warchol, 2006). However, the lived experiences of caregivers highlight that people living with early stages of dementia do not lose their unique skills immediately after the diagnosis and can remain responsive if opportunities are given. This focus on an individual’s strengths was also largely overlooked in many previous interventions, particularly in the context of outdoor-based interventions (Gaffy et al., 2022; Haubenhofer et al., 2010; Lord et al., 2022). During focus groups, several caregivers reported that their loved ones retained long-term memories and skills related to gardening, music, dancing, singing, art and craft, and management or leadership. They suggested that these attributes or interests could be incorporated into outdoor activities to support autonomy and meaningful engagement. While not prescribing specific activities, these insights informed the project’s adoption of strength-based principles in planning activities and outings (Foidel, 2019).
Another key finding of this co-design study was the need for gender-inclusive interventions that address the diverse needs of individuals living with dementia in disadvantaged population groups, particularly those from the LGBTQIA+ community. Promoting diversity, equity, and inclusion helps respond to the unique challenges faced by these groups (Australian Institute of Health and Welfare, 2025; Stites & Velocci, 2024). As such, the project set about to actively engage with disadvantaged groups to promote GreenConnect as inclusive and culturally safe. The ensuing project implementation was flexible, where disadvantaged groups could participate in GreenConnect Project as part of the mainstream groups or as a separate group.
Our key findings also recognised the importance of co-developing the program’s care model and implementation strategies that are contextually relevant and stakeholder driven. A co-design approach produces care solutions that are practical, accessible and emotionally attuned in the lived experiences of people living with dementia and their caregivers, making them more likely to be adopted and meaningfully used (Goeman et al., 2016; Macdonald et al., 2018). One of the critical insights identified by the consultation workshop participants was the potential risk of participant dropout during implementation (Ibsen et al., 2020; Weuve et al., 2015). Their concerns echoed in the findings from previous dementia studies where participant dropout was attributed to several health-, contextual- and design-related factors, including cognitive and physical decline, age, transitioned to residential care, lack of tailored activities, and timeline of the program. These dropouts can lead to biased outcomes and underpowered studies (Ibsen et al., 2020; Weuve et al., 2015). While the GreenConnect Dementia Respite Program was in its design phase, the recommendations for developing contingency plans and adopting flexible timelines to prevent participant dropouts before commencement of Program implementation helped us prepare for unseen events and refine our implementation strategies (Beishuizen et al., 2017). Furthermore, participants played a vital role in confirming the best evaluation approach, a mixed method approach, to assess the Program’s impact, feasibility and sustainability.
A key strength of this program is the early involvement of people affected by dementia, i.e., both caregivers and individuals living with dementia conditions, in its development. We acknowledge that the active engagement of individuals living with dementia was limited during co-design activities because of their cognitive states. However, their perspectives were represented through participation in the Steering Committee and via dyadic participation in the focus groups. Equally important is the participation of diverse stakeholders across the dementia care landscape, which ensured that the co-designed program was inclusive, holistic, practical and centred on the needs of the target population. The inclusion of both current and former caregivers further enriched the study, bringing a wide range of lived experiences to the group discussions.
While the inclusion of both current and former caregivers in the group discussions enriched the co-design process, it also presented some limitations. Former caregivers, drawing on their broader experiences, may unintentionally dominate conversations, potentially overwhelming current caregivers or eliciting difficult emotions, particularly when differing perspectives emerge (Mroz et al., 2023). Our experienced facilitators were attentive to these dynamics, especially variations in emotional readiness and actively worked to ensure balanced and respectful participation from all. Notably, participants expressed appreciation for the opportunity to learn from one another, regardless of their caregiving stage. A further limitation of the study was the absence of male caregivers, meaning that the distinct challenges they face were not captured to inform the model of care and implementation strategies.
Conclusion
This study lays the foundation for the implementation of a novel green care founded project, the GreenConnect Dementia Respite Project, in the Australian rural/regional setting. It underscores the importance of a co-design approach that preceded and informed project implementation. Through meaningful engagement with caregivers, individuals living with dementia and a diverse range of stakeholders, the GreenConnect Dementia Respite Project was shaped to reflect the needs, preferences, and lived experiences of its end users. Early and meaningful engagement with stakeholders helped shape an implementation framework that is both acceptable and potentially sustainable. By centring the voices of people living with dementia and their caregivers, the program is better positioned to achieve its goals.
Footnotes
Acknowledgements
The authors would like to thank all participants for their participation in the study. We would like to acknowledge Marg Rae (current caregiver of a person living with dementia) and Dot (Person living with dementia) for their support during our co-design study. Additionally, as founding members of the project consortium, we extend our gratitude to the former CEO of Rural Care Australia: Darren Midgely for their support.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Australian Government (Grant ID 4-IK7S7DS).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Dan Douglass is the Chief Executive Officer at Heathcote Health. Gerard Jose is the Chief Executive Officer of Rural Care Australia Ltd. Carrie Chappell was the Chief Executive Officer of Princes Court Ltd.